
Abstract
Objectives
Compare the efficacy and safety of fibrin gel to 8% papain gel for wound dressing of venous ulcers.
Method
Patients with chronic venous ulcers were randomly assigned to one in three groups: Group 1—fibrin gel; Group 2—8% papain gel; Group 3—carbopol gel (control). Patients were seen every 15 days during 2 months, verifying reduction of the ulcer area, local infection, exudation, and epithelization. All serious or nonserious adverse events were recorded.
Results
Fifty-five patients (total of 63 ulcers) were randomly distributed in three groups (G1 = 21; G2 = 19; G3 = 23). No patient was excluded or discontinued treatment throughout the study. The areas of the ulcers were similarly reduced in all groups (14.3%, 21.1%, and 30.4% in groups 1, 2, and 3, respectively), and all had significant reduction in exudation and contamination.
Conclusion
The data demonstrate that neither fibrin gel nor papain gel were able to improve the process of ulcer-healing, as compared to control.
Introduction
The healing process encompasses a sequence of molecular and cellular events that interact in order to restore the wounded tissue.1,2 In chronic venous ulcers (CVU), however, this process is compromised by the extended inflammatory phase, 3 which contributes to the initiation of remodeling defects in the extracellular matrix and epithelium, and leads to molecular and cellular alterations in the microenvironment, and to tissue hypoxia. These defects predispose to increased tissue fibrosis, and to the accumulation of metalloproteinase, collagenase, and elastase, which prematurely degrade collagen and diminish growth factors, fibronectin and remodeling of the extracellular matrix. 4
Recently, there has been renewed interest in the mechanisms involving the wound bed preparation 5 and reduction of the necrotic load.6,7 Processes involved in the removal of senescent cells, devitalized tissues and non-viable granulation tissue, as well as in the reduction of biofilms, control of bacterial load and exudates, have been widely studied. 8
Enzymatic agents may play an important role in the preparation of the wound bed. 5 There are two types of enzymatic debridement: a) using exogenous proteinases (i.e., papain, collagenase), which are able to chemically degrade devitalized tissues; b) autolytic debridement that occurs due to endogenous proteinases. The latter may be achieved by the use of occlusive dressings that keep a humid environment in the ulcer wound bed, 9 thus activating phagocytic cells and endogenous proteolytic enzymes. This process can also be stimulated by the use of a fibrin gel. 10 The components of the fibrin clot are many: fibronectin, thrombospondin, vitronectin, glycosaminoglycan, plasminogen, plasminogen activator, thrombin, fibroblast growth factor, insulin-like growth factor binding protein 3, vascular endothelial growth factor, transforming growth factor-beta, and platelet-derived growth factor. These components contribute to debridement, angiogenesis, collagen synthesis, and re-epithelization. 10
The use of papain for the treatment of venous ulcers has been common practice in Latin America for over 20 years. However, all previous studies with such product in CVU have poor level of evidence, since they are based only in case reports or small series.9,11–13 We were unable to find any previous randomized study comparing papain or fibrin gel with controls.
The objective of the present study was to compare the action of fibrin gel or 8% papain gel with carbopol as control in CVU, through a randomized clinical trial.
Methods
This is a prospective randomized double-blind controlled trial. Patients were consecutively enrolled from the Services of Dermatology, and Vascular Surgery of our University Hospital from July 2008 to August 2011. This study was approved by the local Institutional Review Board (protocol number 515/08).
Inclusion criteria were: age 18 years and above, CVU with a minimum area of 5 cm2, wound bed with devitalized tissues like necrotic tissues, no use of venotonic drugs or active topic agents for at least 2 weeks before the study, and having signed the Informed Consent.
Exclusion criteria were: severely infected ulcers, ulcer of arterial and/or mixed etiology with ABI (ankle brachial index) less than 0.9, or chronic ulcers of other etiology. Pregnant and breastfeeding patients were also excluded. Patients who had ulcers that presented clinical signs of infection during the follow-up interval would be discontinued from the study. When the following symptoms were present the ulcer was considered infected: pain, erythema, edema and increase in local temperature, with or without systemic hyperthermia, and poor general condition. Ulcers were considered to have critical colonization when no good granulation tissue was present and the wound bed was friable, of purplish, yellowish, or greenish (colonization by Pseudomonas) tinge. 14
Randomization protocol was based on numbers randomly generated by software. Fifty-five opaque sealed envelopes numbered in ascending order were prepared, containing the randomized treatment. The pharmacist of the Cellular Engineering Laboratory prepared all the products, which were numbered and similar in appearance and presentation. The pharmacist kept the envelopes and the randomization list. The investigators were unblinded only by the end of the study.
Patients were randomly distributed in three groups: Group 1—fibrin gel; Group 2—8% papain gel, and Group 3—carbopol gel (which was the carrier-vehicle used in the other products). Patients from all three groups received compressive elastic bandages (Surepress®) and instructions on how to use them.
The protocols for the production of fibrin gel, 8% papain gel and carbopol gel followed the standard procedures of the Cellular Engineering Laboratory. Fibrin gel was prepared using a pool of five cryoprecipitate units (cryo) prepared in SOPs conditions for blood banks, with the addition of 100 IU/ml of human thrombin cryoprecipitate purified by ethanol precipitation, 6% (w/v) vitamin A and E (alpha tocopherol), and 5% calcium gluconate. After preparation of the Carbopol Ultrex® gel, the protein components were slowly added under continuous agitation in the emulsifier, in order to obtain a homogeneous gel of pearly color and sui generis odor. Papain gel was made with 8% commercial papain (All Chemistry®) diluted in Carbopol gel (All Chemistry®).
During the baseline visit, the patients received an explanation about the content and procedures of the study. The ulcers were photographed and the areas were evaluated by the ImageJ® software. 15 Punch biopsies from the ulcer edges were collected by the dermatologist at baseline and in the last visit, and were sent to the pathologist, who was blinded to the groups.
Demographic data, baseline measurements, and anthropometric data, body mass index, physical examination (pedal and popliteal pulse evaluation, perfusion, and limb temperature), ankle brachial index, evaluation of the wound bed (tissue characteristics, presence of exudate, signs of critical colonization, wound edge evaluation), initial pain related to the ulcer, were all recorded.
The patients signed the informed consent and received a copy of it. They were instructed on how to apply, transport, and preserve their respective topic agent, as well as on how and when to change dressings (cleaning around the ulcer and flushing the wound bed with warm 0.9% saline), and the use of elastic bandage. The treatment kit contained: the treatment gel in a Styrofoam box with reusable ice brick, one compression bandage (Surepress®), a handout with information about the gel and bandage changes, and the schedule for a follow-up visit. The treatment agents (gel) were packed inside disposable toothpaste tubes in sufficient amounts for 15 days.
Primary outcomes included: reduction of the wound area (cm2), evaluation of the characteristics of the bed wound (presence of vitalized or devitalized tissues), signs of critical colonization, presence of exudate. Secondary outcomes were: a) angiogenesis count analyzed via immunohistochemistry; b) complete healing; and c) local adverse events. It was considered complete healing when cutaneous integrity was re-established. Visits were scheduled for every 15 days in order to assess primary and secondary outcomes.
The reduction of the ulcer areas (cm2) was evaluated by the analysis of digital photographs (Kodak digital camera in automatic mode with 800 × 200 pixels) from D0, D15, D30, D45, D60 by ImageJ® software. Each ulcer was measured five times and its average size was used. 16
The principal investigator (PI) and two other specialized health professionals not involved in the study evaluated the characteristics of the tissue of the wound bed, as well as signs of critical colonization. Each examiner received a protocol guide about every tissue to be observed, together with a spreadsheet to record the results.
The PI was the only one to observe and analyze the presence of exudate (yes/no). Slides from the ulcer biopsies were marked by anti-CD34 monoclonal antibody for immunohistochemistry, photographed in a Nikon Coolscope II microscope under a 4 × magnification, and presented as BMP pictures of 512 pixels. All the images were analyzed using ImageJ® 1.46 software. The quantifications of pixel percentage were calculated as equivalent to the immunohistochemistry mark of each image after automatic segmentation of the histogram.
The safety data were compiled by the PI and subsequently checked by the dermatologist. Non-serious events were: little to mild pain during the use of the topic agent, skin maceration around the ulcer, and/or presence of a satellite ulcer. Serious events were: infected ulcer and increase in ulcer area.
The sample size was estimated in 17 patients per group, presuming 80% ulcer healing for Group 2 and 40% for Group 1, with significance level of 5% and 80% test power.
Chi-square test was used for qualitative variables analysis. Mixed linear model was used to assess groups, time periods, and interaction between groups. Kappa coefficient was used to study examiners' agreements considering the debridement data (ulcer wound bed tissue characteristics, critical signs of colonization, and wound edge characteristics). Significance level was set at p < 0.05.
Results
Fifty-five patients were included, five of them presenting multiple ulcers, providing a total of 63 ulcers. No patient was excluded or discontinued treatment during the study. They were randomly distributed into: Group 1—fibrin gel: N = 21; Group 2—papain gel: N = 19; and Group 3—carbopol gel: N = 23.
Demographic data of groups.
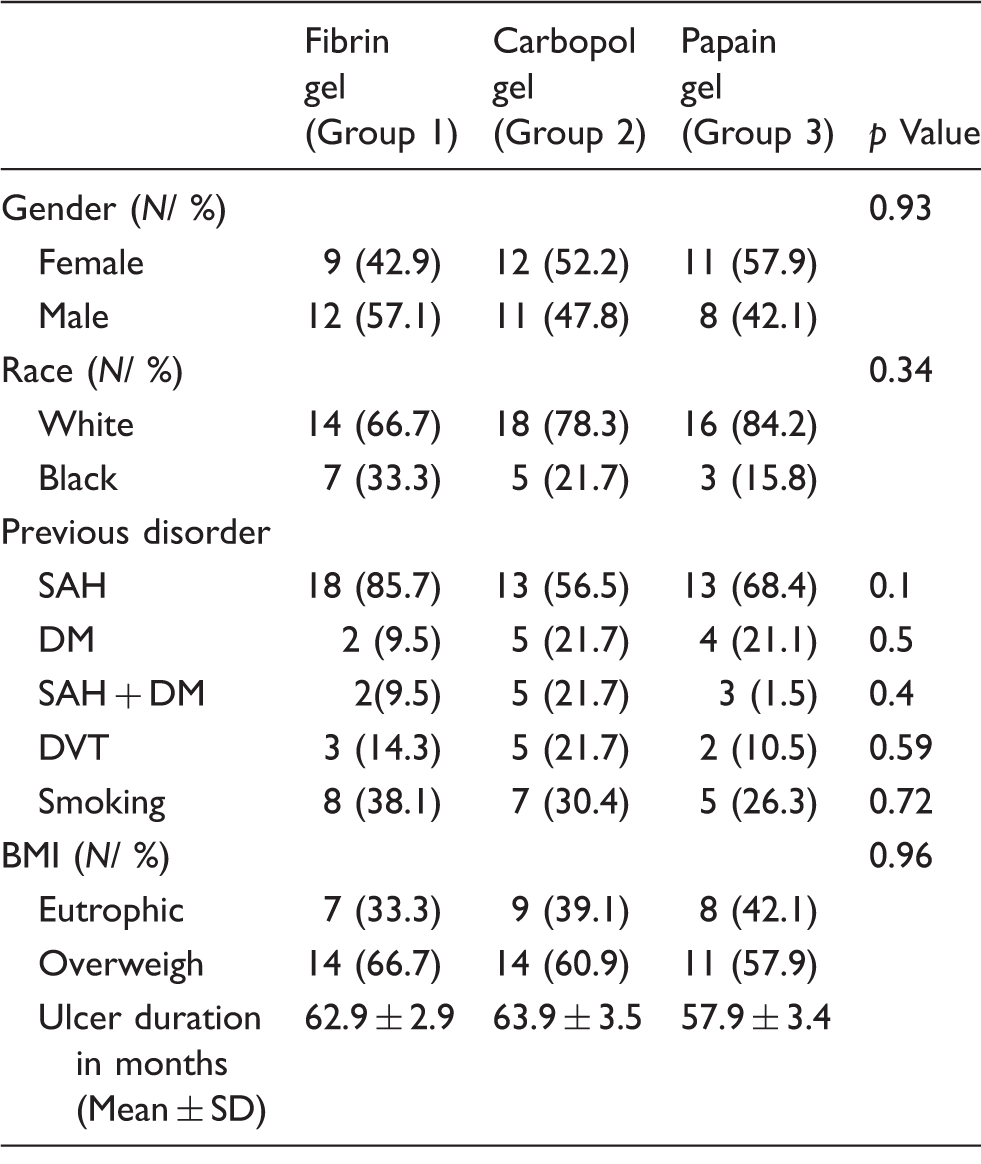
Note: SAH: systemic arterial hypertension; DM: diabetes mellitus; DVT: deep venous thrombosis; BMI: body mass index; M: media; SD: standard deviation.
Ulcer area was similar between groups at baseline (D0) (p = 0.38). Throughout the study, there was a similar reduction in the area inside each group (p = 0.14), and between groups (p = 0.62) (Figure 1).
Distribution of ulcer area (cm2) in the groups and along time. There was consensus among the examiners on the characteristics of the ulcer wound beds (Kappa = 1.00). In all groups there was presence of devitalized tissue at baseline (D0) and similar reduction of devitalized tissues, critical colonization signs, and presence of exudate in the wound bed along time. Edge epithelization increased in all groups at D60, with no statistical difference (p > 0.05).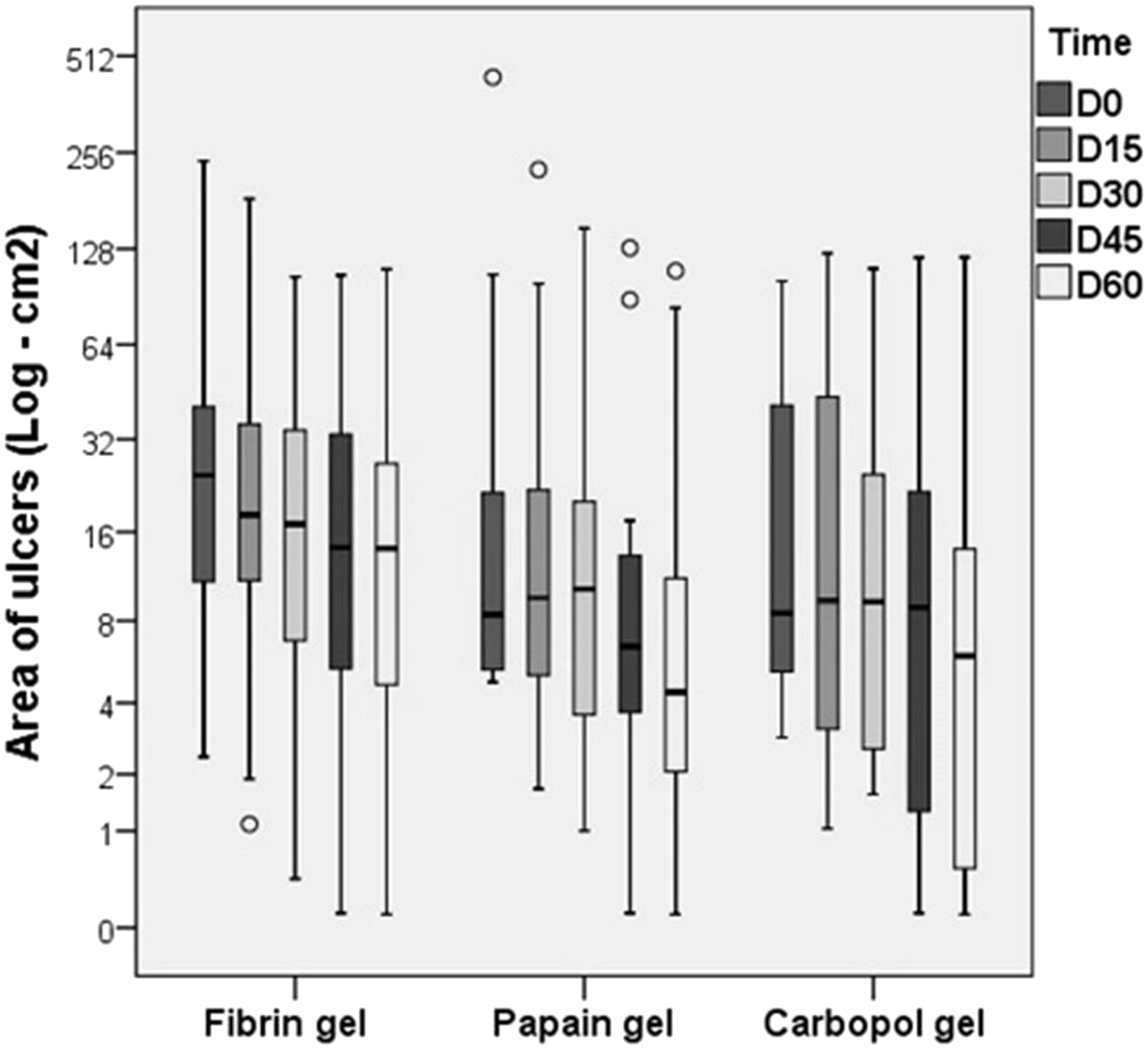
There was agreement among the examiners on the characteristics of the ulcer wound bed (Kappa = 1.00). Devitalized tissue at baseline (D0), reduction of devitalized tissues, critical colonization signs, presence of exudate in the wound bed along time were all similar in all groups. Edge epithelization increased similarly in all groups at D60 (p > 0.05).
Biopsies were collected at the final visit only in 16 patients of Group 1, 14 of Group 2, and 9 of Group 3. Some patients refused to have the last biopsy, some ulcers had healed, and some presented area <0.5 cm2. This sample loss was homogeneous (p = 0.17).
Angiogenesis was similar in all groups (p = 0.46). The mixed linear model found increase in the percentage of pixels related to vessels in the more vascularized areas from D0 to D60 (Figure 2).
Pixel percentage related to the presence of blood vessels in vascularized areas at D0 and D60.
Rates of complete ulcer healing per study group.
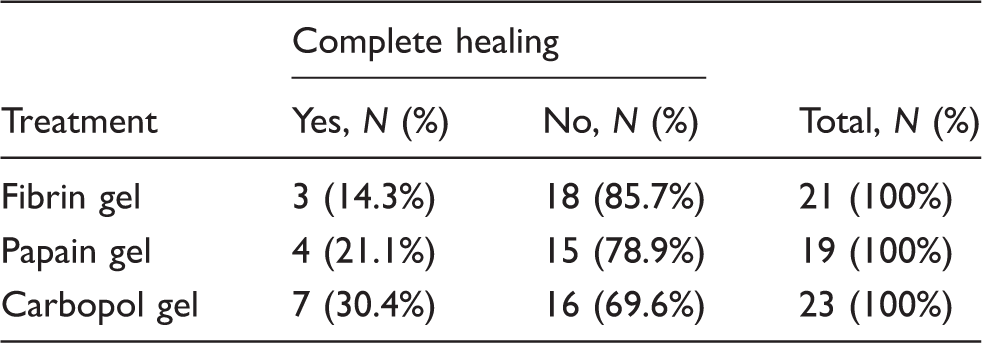
p = 0.43.
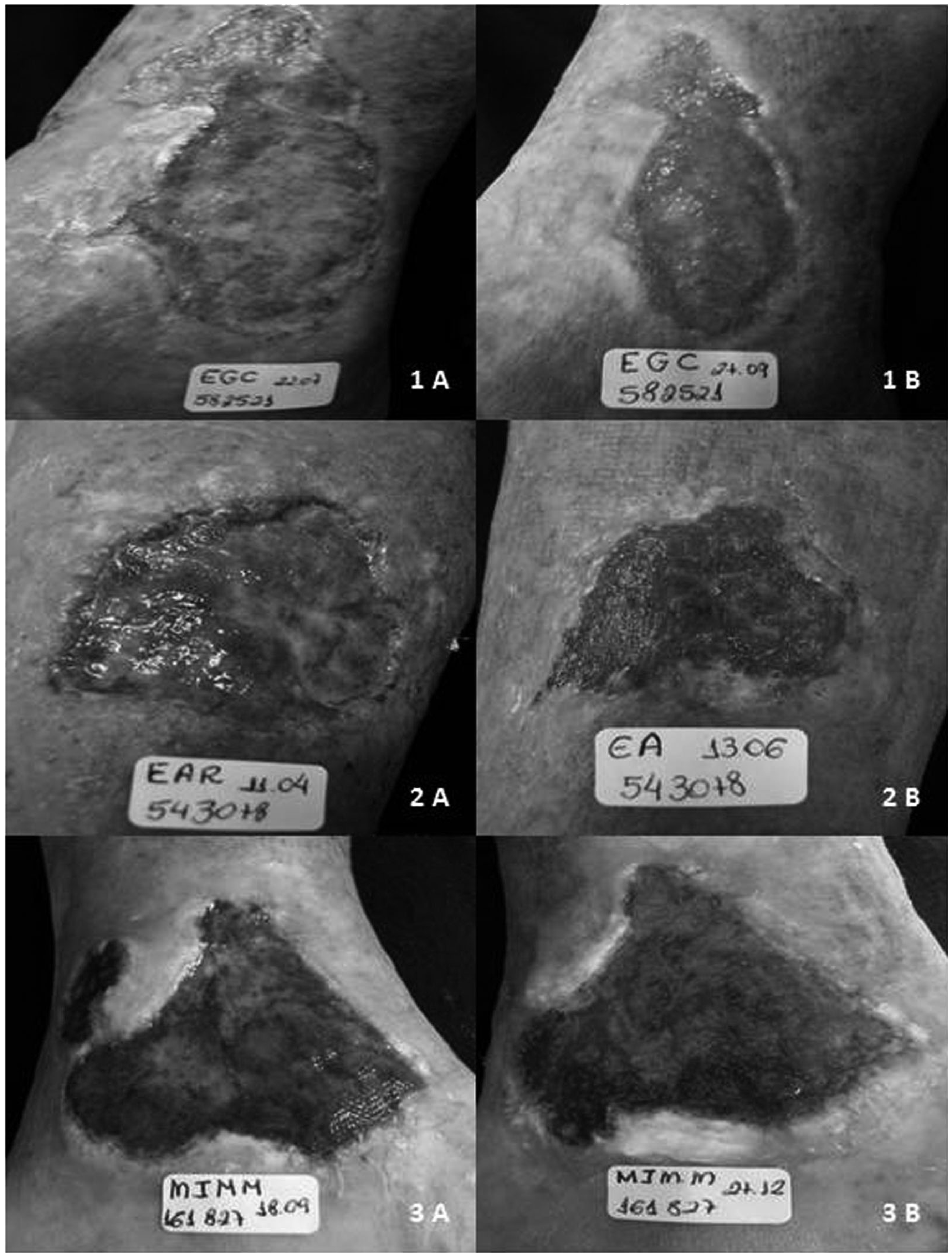
Examples of ulcer aspects before treatment (a) and 60 days after treatment initiation (b). 1: Group 1—Fibrin gel; 2: Group 2—8% Papain gel; 3: Group 3—Carbopol gel (carrier-vehicle used in the other products).
Figure 4 depicts the patients' compliance to elastic compression. Regular use was associated to reduction of ulcer areas.
Evolution of ulcer area (cm2) considering clinical care: use of elastic bandage, hygiene, medication.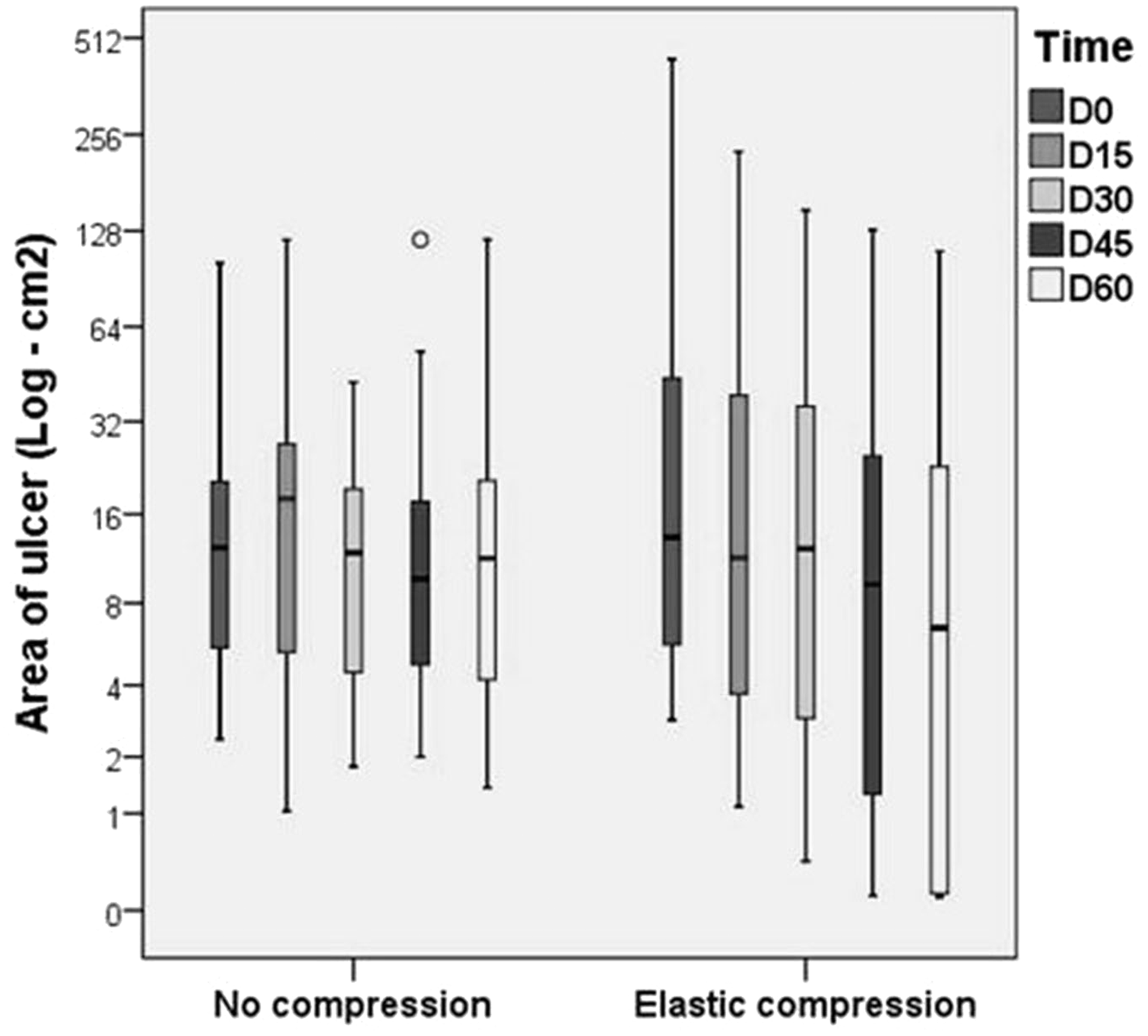
Nonserious adverse events were: pain in two patients, one of Group 1 and one of Group 2, (10.5% for each group); a satellite ulcer in one patient of Group 1 (4.8%); increase in ulcer area in one patient of Group 3 (control) (4.3%). Serious adverse events were: infection in three patients, one of each group (1, 2, and 3, respectively).
Discussion
Open venous ulcer is the most advanced stage of chronic venous disorder, with clinical classification CEAP 6. 17 The prevalence of females and males found in this study was similar to previous studies from our institution.18,19 The proportion between genders was of 1.4 females:1 male. Even though the prevalence for male and female patients is not established for venous ulcers, some studies show a two- to three-fold prevalence of female patients.20,21
Most of the patients were Caucasian. It is controversial whether skin color influences in the development of venous ulcer. According to the 2011 demographic census, 22 white patients were majority (47.33%) in Brazil.
In the present study, systemic arterial hypertension, Diabetes mellitus, and obesity did not interfere in the healing process. This is in accordance with the literature results23,24 in which these factors did not predispose to recurrences or have influence upon the size and duration of active ulcers. The deleterious effects of smoking over the healing process are still controversial due to the lack of clinical studies correlating the amount of nicotine necessary to interfere in the healing process.3,9,25–27 In our study, smoking did not have influence.
The duration of active ulcers and the size of the wound bed are predictive factors for ulcer healing. 28 The average duration of active ulcers in this study was 61.2 months, which is close to the findings of Abbade et al. 18 (64 months), and Silva et al. 29 (60 months). The long duration of active ulcers as well as the large wound beds found in our population are probably related to the patients' difficulty to find appropriate treatment or failure of previous treatments conducted elsewhere.
In order to improve the treatment response and minimize the effects of venous hypertension, compression bandages were employed in our protocol. Compression therapy is in fact the key treatment for venous ulcer. 30 As depicted in Figure 4, adherence to elastic compression was an important factor for the process of ulcer healing. Compression therapy presents effects on macro and microcirculation. 30 In the macrocirculation it increases return in the deep venous system, therefore diminishing the pathological reflux during ambulation, and increasing the ejected volume during the contraction of the calf muscles. The compression applied to the limb increases tissue pressure favoring reabsorption of edema, and improves lymph drainage. Additionally, it acts in the microcirculation diminishing the exit of fluid and macromolecules from capillaries and venules to the interstitium, and can stimulate fibrinolytic activity. 31 The reduction in ulcer area in all groups was probably related to the summed effects of compression and routine wound care established for all patients.
Chronic ulcers have an unfavorable colonization of the microenvironment by aerobic and/or anaerobic bacteria, as well as fungi. 32 Removal of devitalized tissue is important to accelerate wound healing. 6 Our results demonstrate that in all groups there were similar outcomes regarding debridement and reduction of bacterial load, corroborated by concomitant reduction in exudates, mainly after D45.
The epithelization of the edges was evident and similar in all three groups by D45. There was no statistical significance in the present study to support that one treatment was better than the others. Once balance is established in the wound bed, fibroblasts, endothelial cells, and keratinocytes synthesize growth factors that trigger cell migration and proliferation, as well as the synthesis of components of the extracellular matrix and angiogenesis. The ulcer wound bed is then totally filled with granulation tissue; blood flow will be re-established by angiogenesis, and the lymph network will be restored.3,7 During the period of our study, angiogenesis increased in all groups.
The adverse effects observed were few and included pain, infection, and the presence of a satellite ulcer. Proteolytic enzymes can trigger an inflammatory response by breaking viable components from the ulcer wound bed. Some authors have considered this inflammatory response as a predisposing factor for pain. 33 One patient from Group 1 and one from Group 2 had ulcer infection. All the remaining patients also had mild pain that could be explained by individual reaction to the dressing components. The satellite ulcer was probably consequence of elastic compression misusage.
Although various previous studies report good clinical results with papain in venous ulcers, the results in our study reflect the impression of our clinical experience. In spite of the efforts with the new medication, it did not improve the CVU healing process when compared to the other gel or to the control group that used only wound bed cleaning, carbopol, and elastic compression.
Conclusions
Regarding clinical efficacy: fibrin gel and papain gel did not differ from control in healing CVU. Elastic compression was independently associated to faster area reduction. Angiogenesis was observed in all three groups. Adverse effects were nonsignificant for all three treatments.
Ethical approval
This study was conducted according to the principles of the Declaration of Helsinki, ISO14155 and the guidelines for Good Clinical Practices. The Institutional Review Board of the Botucatu Medical School, Universidade Estadual Paulista, São Paulo State, Brazil, approved this study, which was registered under the protocol number CEP 515/08. All subjects signed a written informed consent before enrollment. Subjects could leave the trial at their own discretion, with no constraint or penalty.
Footnotes
Acknowledgements
We would like to thank Boston Medical Device for their kind donation of the high-compression bandages (Surepress®).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was undertaken for educational purposes and clinical care of patients with chronic venous ulcers, funded by the Botucatu Medical School and with the support from Boston Medical Device that donated the high compression elastic bands used by all patients (Surepress®).