
Abstract
Objective
To systematically review all available English literature on mechanochemical endovenous ablation and to report on the anatomical, technical, and clinical success.
Methods
A systematic literature search was performed in PubMed, EMBASE, and the Cochrane Library on mechanochemical endovenous ablation for the treatment of insufficient great and/or small saphenous vein. Methodological quality of the included studies was evaluated using the MINORS score. The primary outcome measure was anatomical success, defined as closure of the treated vein on follow-up duplex ultrasound imaging. Secondary outcomes were technical and clinical success, and major complications defined as deep venous thrombosis, pulmonary embolisms or paresthesia.
Results
The literature search identified 759 records, of which 13 were included, describing 10 unique cohorts. A total of 1521 veins (1267 great saphenous vein and 254 small saphenous vein) were included, with cohort sizes ranging from 30 to 570 veins. The pooled anatomical success rate after short-term follow up was 92% (95% CI 90–94%) (n = 1314 veins). After 6 and 12 months these numbers were 92% (95% CI 88–95%) (n = 284) and 91% (95% CI 86–94%) (n = 228), respectively. The long-term anatomical success rates at 2 and 3 years were 91% (95% CI 85–95%) (n = 136) and 87% (95% CI 75–94%) (n = 48), respectively. Major complications and especially nerve injury were very rare (≤ 0.2%). All studies were of moderate or good quality using the MINORS scoring scale.
Conclusions
Mechanochemical endovenous ablation using the ClariVein in combination with liquid sclerosant is associated with an anatomical success rate ranging from 87% to 92% and good clinical success. To date, no randomized controlled trials are available studying the anatomical success after mechanochemical ablation, compared to the endothermal ablation. The risk of major complications is very low after the procedure.
Introduction
Chronic venous insufficiency of the lower limbs is a common disorder. Symptoms range from pure cosmetic complaints to hard-to-treat venous ulcers. The gold standard in the treatment of incompetent saphenous veins has drastically changed over the last decade. Surgical high ligation and stripping has been replaced by endovenous thermal techniques, such as endovenous laser ablation (EVLA) and radiofrequency ablation (RFA). These minimally invasive procedures are associated with less hematoma, less pain, superior cosmetics, and earlier resumption of normal activities. They seem to have superior anatomical success rates compared to the traditional surgical stripping of both great and small saphenous veins.1–4 Thermal ablative techniques, however, necessitate tumescent anaesthesia to avoid severe pain and injury to the surrounding tissue. This anaesthetic technique requires multiple punctures along the vein segment to be treated, which prolongs the procedure and adds to patient discomfort during treatment. Despite the use of tumescent anaesthesia, a subset of patients with postoperative pain remains, which can last for several weeks.5,6 To provide an alternative to the thermal ablation techniques various other approaches have been studied, including foam sclerosing, glue and mechanochemical endovenous ablation (MOCA). MOCA was introduced in 2010 and combines mechanical damage to the endothelium caused by a rotating wire and the use of the ClariVein device with simultaneous infusion of a liquid sclerosant, causing fibrosis of the vein. 7
This study systematically reviews all published data on outcomes and major complications using MOCA as a treatment for great and small saphenous vein insufficiency.
Materials and methods
A structured literature search was performed using the guidelines outlined in the Cochrane Handbook for Systematic Interventions (version 5.1.0) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).8,9
Search strategy
Three different biomedical bibliographic databases (PubMed, EMBASE, and the Cochrane Library) were used to perform a systematic search for all English literature. Search terms were all differently spelled text words or abbreviations on (“vein incompetence”, “varicose vein”, “small saphenous vein”, “great saphenous vein”, “venous reflux”) and (“endovenous ablation”, “mechanochemical ablation”, “ClariVein”, “MOCA”) and (“outcome”, “results”, “success rate”, “failure rate”, “complications”, “obliteration”, “occlusion”, “recurrence”, “recanalization”, “reflux”, “pain”, “return to normal activities or work”, “haematoma”, “paresthesia”, “nerve injury”, “wound infection”, “deep vein thrombosis”, “thromboembolism”) in the title, abstract, and medical subject heading (MeSH).
Inclusion and exclusion criteria
All manuscripts that included patients treated with MOCA for saphenous insufficiency (either great saphenous vein (GSV), small saphenous vein (SSV) or both), with the primary outcome measure described, were eligible for inclusion in this review. Exclusion criteria were case reports, studies with ≤ 10 MOCA treated legs, and studies aimed at recurrent saphenous vein insufficiency. Studies describing cohorts that did not solely use MOCA treatments could only be included if the data for patients with MOCA could be specifically extracted from the study results. If more than one study reported the same patient cohort, only the most recent and complete manuscript was included in this review. Studies on the use of MOCA outside the instructions for use were excluded from the analysis. Finally, the same criteria were used to screen all cross-references for potentially relevant studies not identified by the initial literature search.
Patients
Included were patients with great and/or small saphenous vein insufficiency who were treated with MOCA.
Outcome measures
The primary outcome was anatomical success, defined as closure and absence of reflux on duplex ultrasound (DUS) imaging. 10 The primary outcome was evaluated for multiple follow-up periods. Secondary outcomes were initial technical success, clinical success, and major complications.
Data extraction
Two reviewers (D.B. and M.W.) evaluated all publications for inclusion or exclusion in this review based on title, abstract and full text. To systematically extract the data from the manuscripts a predetermined standardized extraction form was used. When studies included patients with multiple treatment modalities, only the data of MOCA treated patients were extracted.
Outcome measures for success were described as “closure”, “occlusion”, “obliteration”, or “ablation.” In some studies failure was described using terms such as “recurrence”, “reflux”, “recanalization”, “patent”, or “open”. To convert these failure rates to anatomical success, the failure percentage was deducted from 100%. Initial technical success, defined as the absence of technical failure, was the ability to complete the procedure as planned. 10 The venous clinical severity score (VCSS) was scored to evaluate the clinical success. Disease specific and generic quality of life (QoL) were studied and presented descriptively.
The following major complications were scored: deep venous thrombosis, pulmonary embolism, and (transient or persisting) paresthesia. Paresthesia was reported differently throughout the studies as (sural) nerve injury, numbness, or paresthesia. Other (minor) complications (e.g. superficial phlebitis, hematoma, superficial infection, and skin staining) were excluded from analyses.
Validity assessment
Two authors (D.B. and M.W.) independently assessed the methodological quality of the articles using the MINORS (methodological index for nonrandomized studies) quality score. 11 Disagreement was resolved by discussion and consensus within the complete groups of authors.
Data analysis
Data were extracted from the studies and pooled into a database. All outcomes were separately described. The number of legs per study at the start of the study was noted. To further specify the included case, the number of GSVs and SSVs were noted for every study.
For follow-up, all available durations of follow-up were used and categorized for pooling. To illustrate the proportion of the patients lost-to-follow-up (LTFU), all anatomical success rates are accompanied by the absolute number of patients per moment of follow up.
To optimize the reliability of the outcomes, only studies with MINORS scoring scales of at least 10 were used for pooled analyses. Rates were pooled using a random-effects model.
The secondary outcomes, technical success and major complications, were calculated for each treatment modality and were corrected for the number of treated legs for each treatment modality (weighted means). Data were analyzed using SPSS 21.0 or comprehensive meta-analysis V3 statistical software.
Results
Literature search
The literature search was performed on 18 October 2016. A total of 759 studies were identified in PubMed (n = 605), EMBASE (n = 152), and Cochrane Library (n = 2). After excluding 92 duplicate studies, we screened 667 articles on title and abstract, leading to the exclusion of 649 studies for the following reasons: not written in English (n = 36), review articles or commentaries (n = 132), study protocol (n = 3), case reports (n = 9), and other technique or study aim (n = 469). We subsequently analyzed 18 full text articles and excluded another 5 articles (Figure 1). One article aiming to describe the pain of MOCA
12
was excluded, because it only reported on an incomplete subset of a larger patient cohort. One was a commentary to one of the included MOCA studies. Another three papers reported on another technique.
Flowchart (in accordance with PRISMA 2009 guidelines).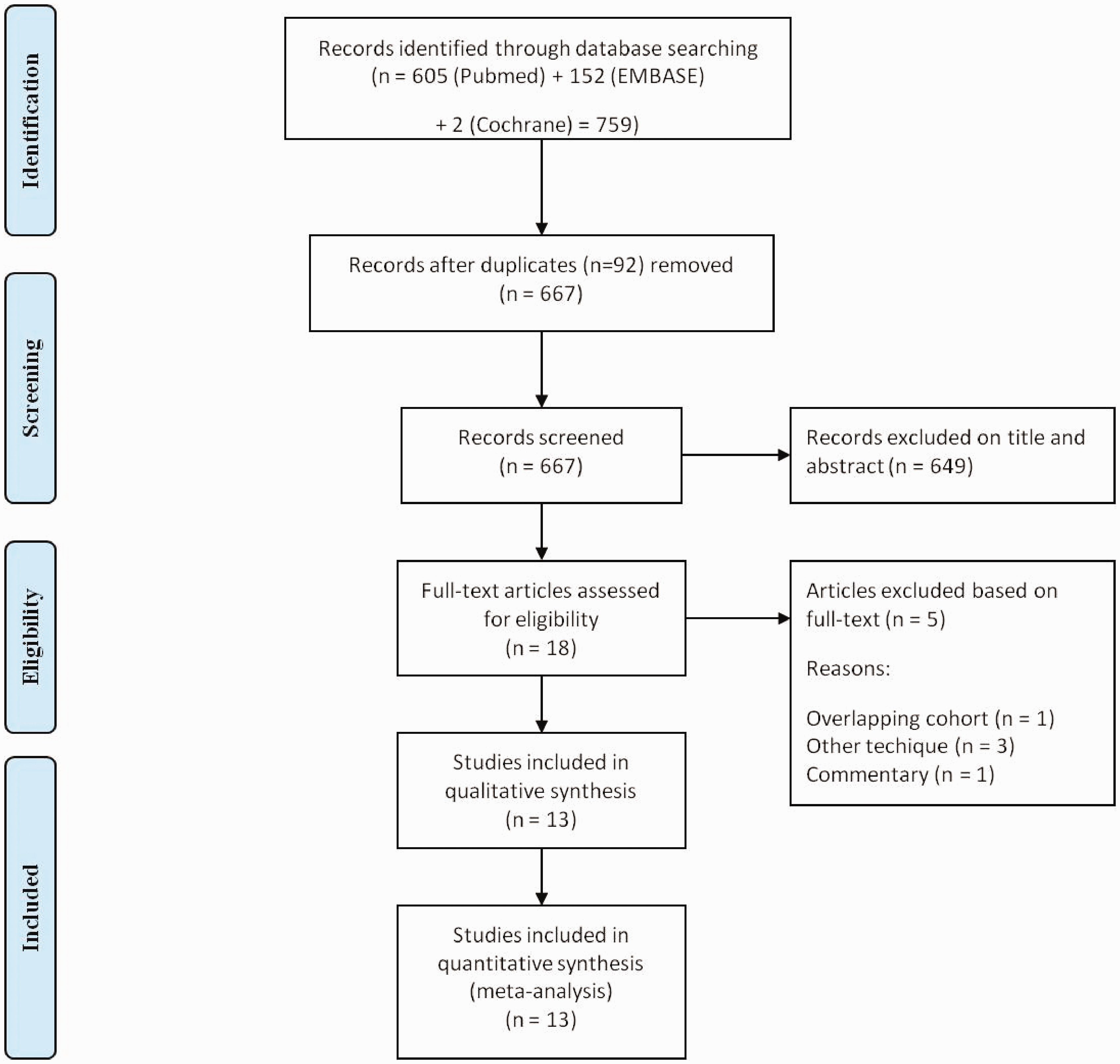
Included studies
Overview of results of MOCA treatment in published clinical studies.
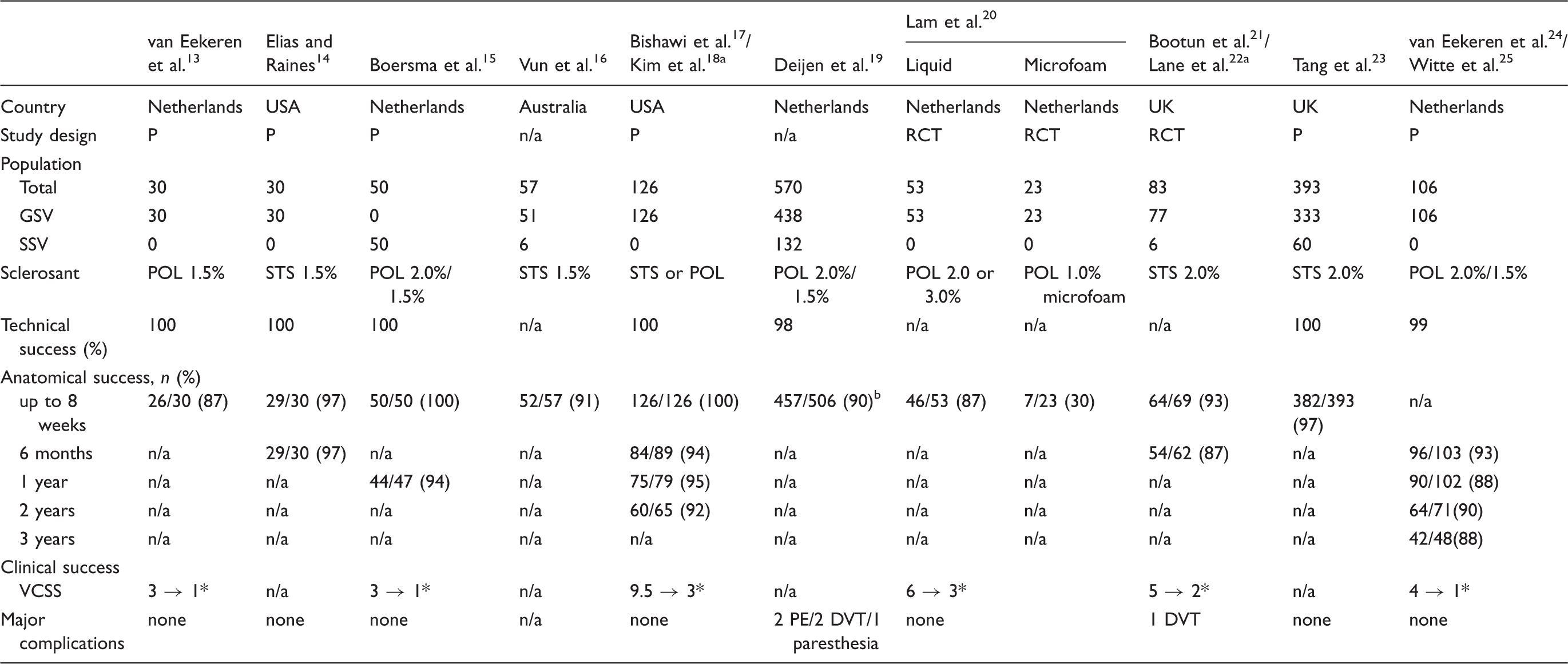
P: prospective cohort; RCT: randomized controlled trial; GSV: great saphenous vein; SSV: short saphenous vein; n/a: not available; VCSS: venous clinical severity score; DVT: deep venous thrombosis; PE: pulmonary embolism.
Two publications on same patient population.
Median follow up of 54 days (range 12–266 days)/anatomical success 92% in GSV/87% in SSV.
Statistically significant.
Pooled data from clinical studies/trials.
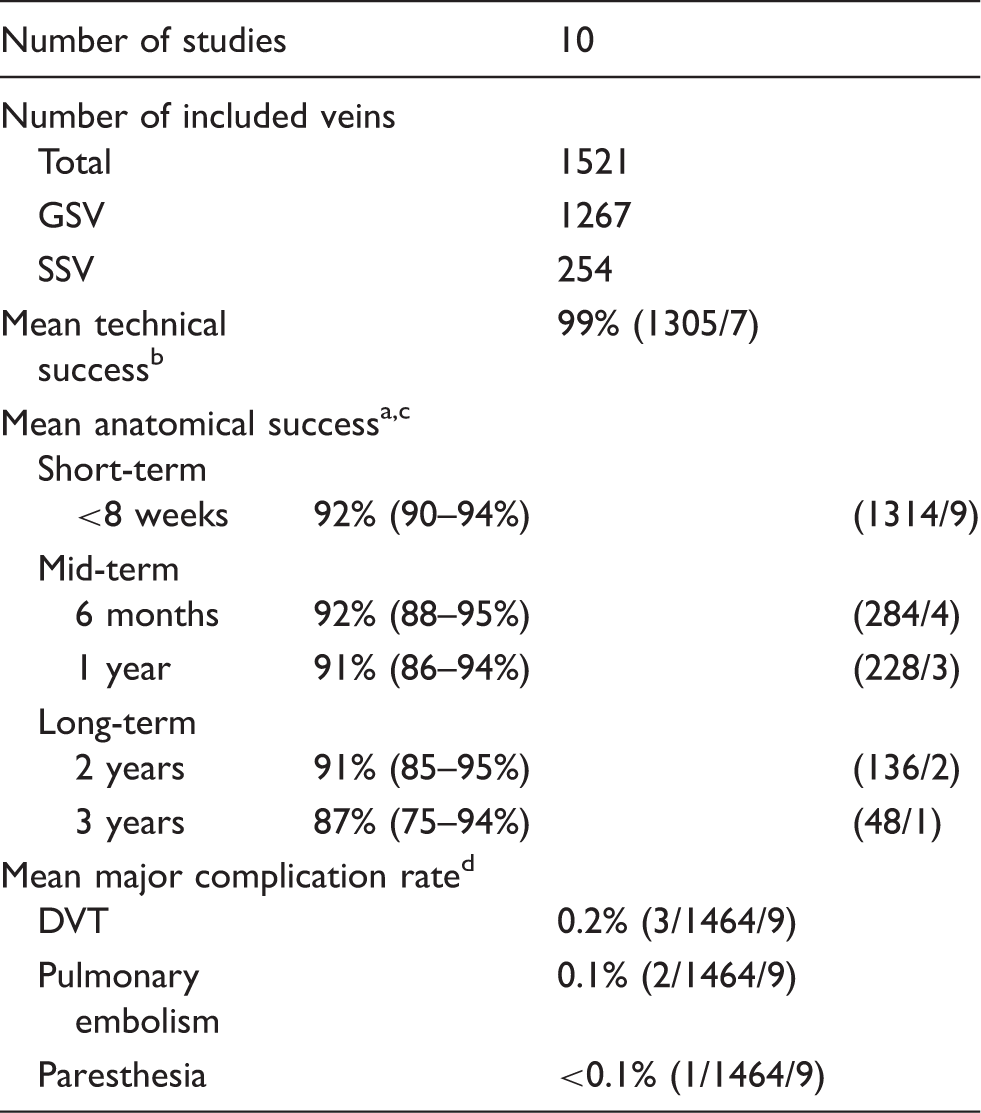
Percentage (95% CI) (number of veins/number of cohorts).
Percentage (number of veins/number of cohorts).
Results from MOCA combined with 1% microfoam were not included.
Percentage (absolute number/number of veins/number of cohorts).
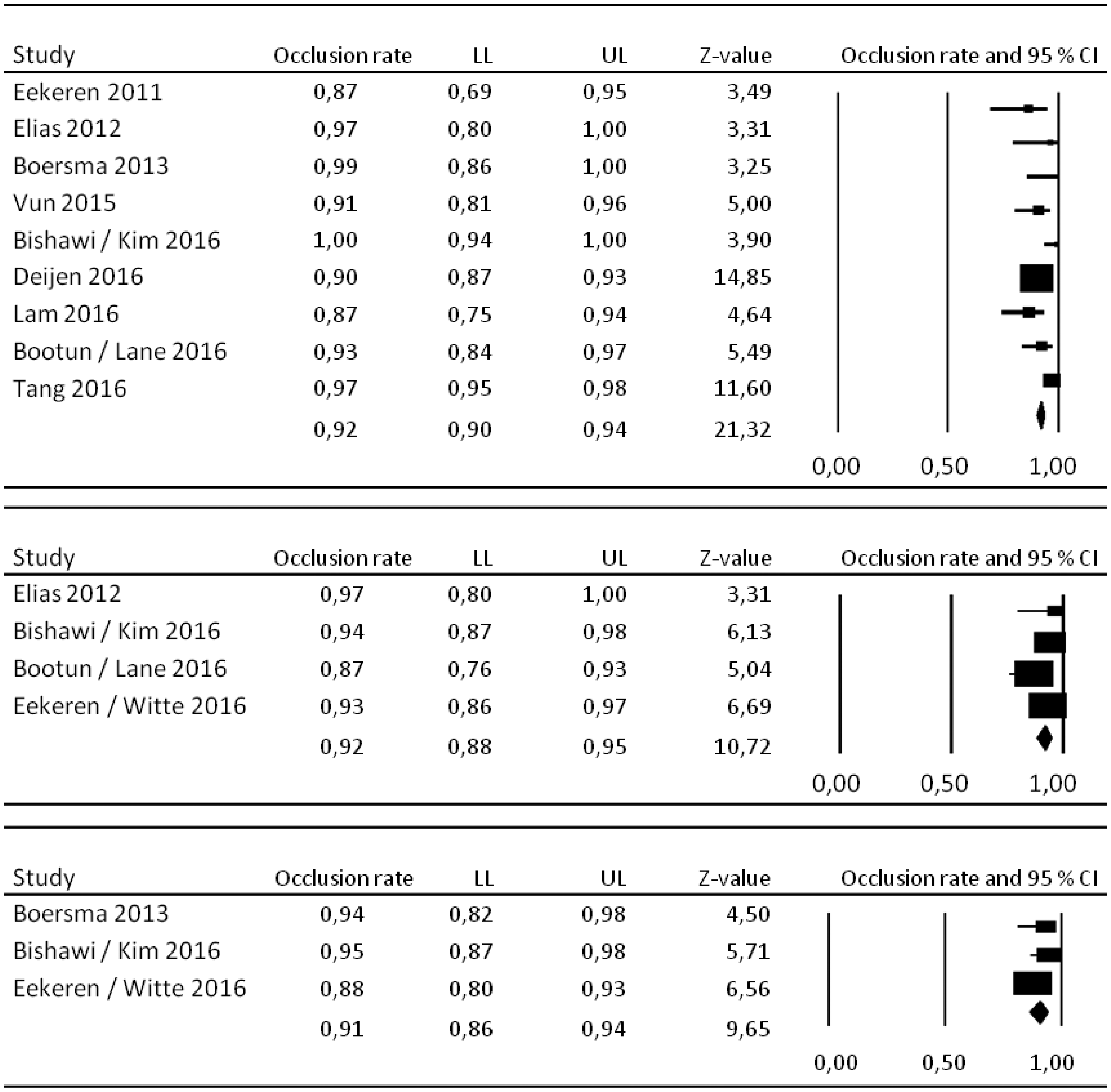
Forest plots for anatomical success rate after <8 weeks, 6 months, and 1 year, respectively.
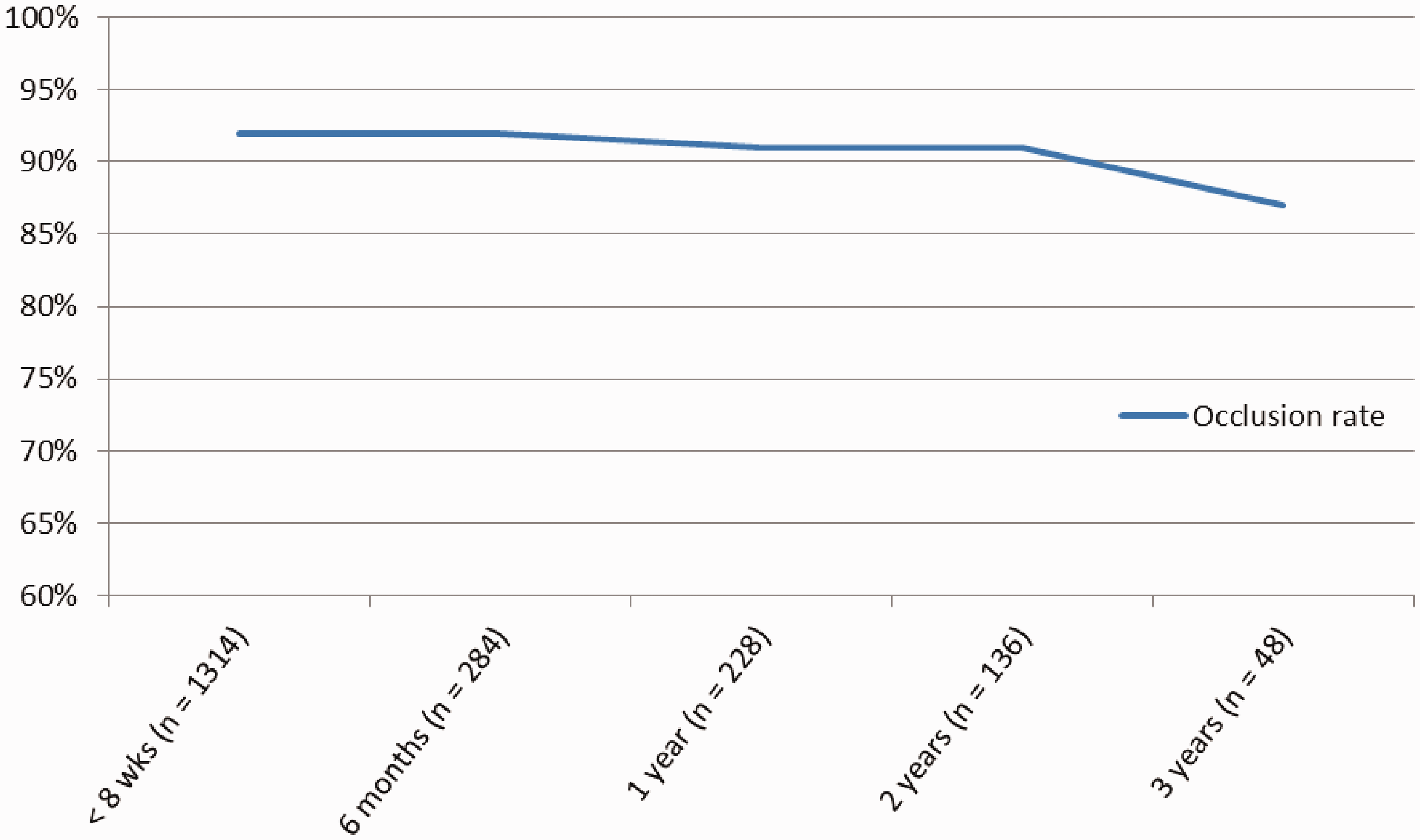
Anatomical success at different timepoints.
Study design of included studies
The majority of studies were prospective cohort studies (n = 8 studies/6 cohorts). Two RCTs were included: one was designed as a pain study comparing MOCA with RFA;21,22 the second was designed as a dose finding study comparing two concentrations of liquid polidocanol and polidocanol microfoam. 20 None of the RCTs was designed or powered to compare the anatomical success of MOCA with endothermal ablation. In two studies, the study design was not described in the publication.16,19
Outcome measures
A total of 1521 veins (1267 GSVs and 254 SSVs) were included. Study sizes ranged from 30 to 570 veins. The primary outcome, anatomical success, was described for all cohorts. The majority of all studies only reported on short- or mid-term anatomical success. As a consequence long-term data were scarce. Furthermore, in the two studies publishing long-term results, around 50% of all patients were LTFU.18,25
The pooled anatomical success rate after follow up < 8 weeks was 92% (95% CI 90–94%) (n = 1314 veins). These rates after 6 months and 1 year were 92% (95% CI 88–95%) (n = 284) and 91% (95% CI 86–94%) (n = 228), respectively. The long-term anatomical success rates at 2 and 3 years were 91% (95% CI 85–95%) (n = 136) and 87% (95% CI 75–94%) (n = 48), respectively (Figure 3).
In the included publications, both liquid polidocanol (concentration ranging from 1.5% to 3.0%) and sodium tertadecyl sulphate (STS or sotradecol in 1.5 or 2.0% concentration) were used. Due to variation in used concentrations and limited long-term data it was not possible to compare the results of different sclerosants and concentrations.
One study included a subgroup of 23 veins treated with MOCA in combination with 1% polidocanol foam. This variation in treatment is outside the instructions for use and certification and is therefore excluded from data pooling. The short-term anatomical success in this group of patients was as low as 30% at 6 weeks follow up.
The pooled initial technical success was 99%, as described in seven cohorts (n = 1305 veins). All studies but one reported on (major) complications, which occurred very rarely. In a total of 1464 veins, only three cases of DVT (0.2%) and two cases of pulmonary embolism (0.1%) were noted. Transient paresthesia was only seen in one case (<0.1%).
Clinical success was reported with both the physician reported VCSS and the patient reported Aberdeen Varicose Vein Questionaire (AVVQ). All eight studies (six cohorts) reporting on VCSS showed a significant decrease after MOCA treatment. Four studies have reported on the AVVQ, a disease-specific QoL score in two cohorts.21,22,24,25 In both cohorts, a significant decrease in AVVQ was measured during the first year following MOCA compared to baseline, which indicated less impairment of QoL, due to the varicose veins. Although AVVQ remains significantly better after 3 years follow up compared to baseline, Witte et al. 25 showed that between 1 and 3 years the initial improvement in AVVQ is followed by subsequent deterioration. The absolute measurements for each cohort are depicted in Table 1. The effect of MOCA on generic QoL scores was limited.
Discussion
This systematic review shows that MOCA in combination with liquid sclerosant is a feasible, safe, and effective treatment for insufficient saphenous veins. Initial technical success was 99%. At short-term follow up, the pooled anatomical success rates were 92%. Mid-term results range from 87% to 96% (pooled 91–92%) and anatomical success rate after 2 to 3 years stabilized at 87% to 91%. These results are in line with short- and mid-term results of endovenous laser and radiofrequency ablation in GSV, ranging from 88% to 93%. 3
This review included studies using MOCA combined with both liquid polidocanol and STS. This is because in some countries only one of the two is registered for this indication. Although in-vitro experiments show that STS might have a potent impact in the vein wall compared to polidocanol, 26 there are no signs that anatomical success in humans differs greatly between the two sclerosants. This review is unable to give more insight in the optimal type of sclerosant, or its concentration, as it is hampered by limited long-term data and multiple variations in treatment protocol regarding type and concentration of sclerosant, even within studies. Nevertheless, the initial SSV study gave circumstantial evidence that increasing the concentration could improve the anatomical success. 15 Currently a RCT, comparing MOCA with 2% or 3% liquid polidocanol with 1% polidocanol microfoam (off label use) is enrolling. As reported above, an interim analysis showed that MOCA with use of foam led to anatomical success of only 30%. Inclusion in the foam arm of the RCT has been seized for these reasons. Until final results of this RCT are published, there will be no definitive answer to this question.
One of the major advantages of MOCA is that it is non-heat-based. This has two clinically relevant advantages compared to endothermal ablation: (1) no necessity for tumescent anesthesia and (2) the abolishment of heat-related complications. The latter is of great importance, especially in ablation of the SSV and below-the-knee GSV, in which the anatomic proximity of both the sural and saphenous nerves poses an additional risk. EVLA and RFA of the SSV is associated with risk for paresthesia of 4.8% and 9.7%, respectively. 4 Pooled data showed that the risk of (transient) paresthesia after MOCA is less than 0.1%. This finding could well be explained by the findings of two animal experimental studies on MOCA. These studies showed that the mechanical injury induced by the ClariVein is limited to the endothelium. In contrast to similar studies in endovenous laser, no perforation or extravenous injury was present in any of the specimens.27–29
In all eight studies (six cohorts) included in this review that described clinical symptoms of varicose disease before and after treatment, a significant decrease in VCSS was measured.13,15,17,18,20–22,24,25 Furthermore, it was repeatedly shown that MOCA treatment led to a significant improvement in HR-QoL (without significant difference compared with RFA).11,21,22,24,25 This significant decrease in VCSS in AVVQ compared to baseline is still seen at 36 months; however, after 2 years a deterioration in clinical scores was described. This might be caused by the recurrent nature of varicose veins.
Supported by the continuously growing number of publications, MOCA should be considered a valid alternative to endothermal ablation. Nevertheless, there are still some important limitations. To date, the long-term data remain limited and around 50% of initially included patients are lost to follow up at 2–3 years after treatment.18,25 Although it is widely accepted that the anatomical success should be assessed with follow up duplex ultrasounds, there is still heterogeneity regarding the exact definition of occlusion; in five cohorts a description of the exact definition used was lacking.13,16,17,21,23 In the remainder, the definition of the anatomical success ranged from occlusion over 85% of total length treated to less than 10 cm recanalization.15,24,25 Furthermore, it should be appreciated that all published data are derived from cohort studies or RCTs not adequately powered for anatomical success. Recently, a protocol for the LAMA trial, a RCT comparing anatomical success and pain after MOCA vs EVLA, has been published (NCT02627846). 30 This trial is currently recruiting participants. Unfortunately, the randomized controlled trials comparing MOCA and RFA in GSV and SSV stopped inclusion prematurely due to reimbursement issues in Netherlands.31,32
Conclusion
Mechanochemical endovenous ablation using the ClariVein in combination with liquid sclerosant is associated with an anatomical success rate ranging from 87% to 92% and good clinical success. To date, no RCTs are available studying the anatomical success after MOCA compared to the endothermal ablation. The risk of major complications is very low after the procedure.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.