
Abstract
Purpose
Lower limb varicose veins have a significant effect upon the quality of life and a considerable socioeconomic impact despite their relatively benign nature. The aim of this study is to compare the effects of various therapeutic strategies among patients with varicose veins to surgical ligation and vein stripping on the basis of quality of life.
Methods
PubMed/Medline and Scopus databases were systemically searched from 1 January 2000 until 23 December 2015 for studies reporting outcome on the quality of life of different treatment techniques for varicose veins. We used Cohen’s d to make the outcomes of the reported scales comparable. Heterogeneity was calculated with the use of the Q statistic and the I2.
Results
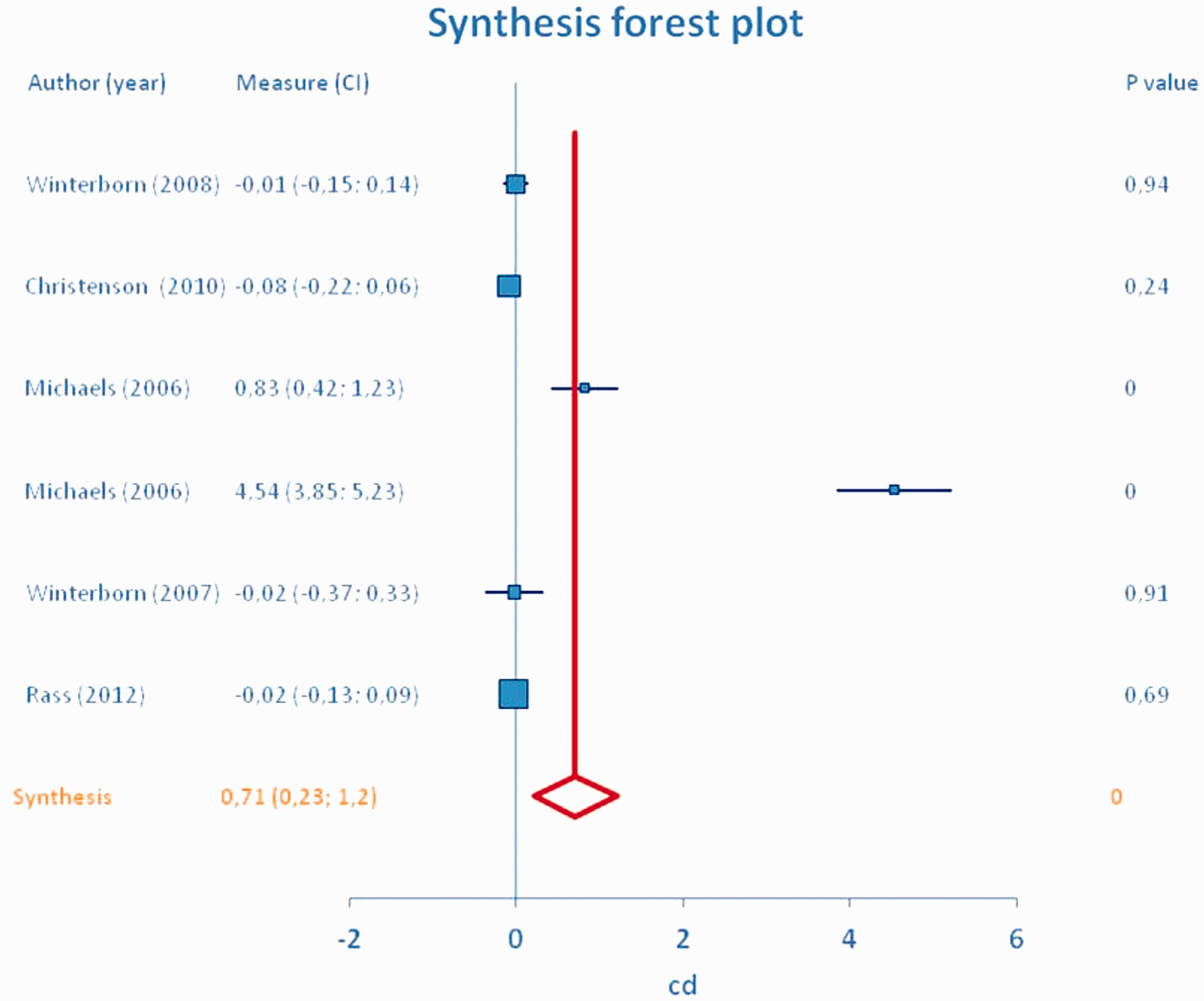
A total of 1047 participants were randomized across all analyzed trials. The number of participants in a single trial ranged from 30 to 308. The majority of participants in any trial were C2 on the CEAP scores. Overall, the quality of evidence was low. For the meta-analysis performed at 12 months postintervention (seven studies, n = 1047 patients) and after random effects meta-analyses due to high heterogeneity, no differences are observed between intervention and surgical ligation and vein stripping. The pooled estimate is −0.001 and the 95% confidence interval is −0.069 to 0.067 with a p = 0.98. In the case of the 24 months, postintervention analysis (six studies, n = 840 patients) the inference is almost identical. The effect of various interventional modes of treatment compared to surgical ligation and vein stripping is negligible in terms of clinical outcomes and quality of life so that surgical ligation and vein stripping versus the other interventional procedures were equally effective approaches to treat great saphenous vein incompetence in terms of quality of life measurements.
Conclusion
The procedures were at least equally efficient in treating patients with varicose vein disease in terms of quality of life assessment tools at 12 and 24 months compared to surgical ligation and vein stripping.
Keywords
Introduction
Lower limb varicose veins represent a common clinical problem of the superficial venous system. They have a significant effect upon the quality of life (QoL) and a considerable socioeconomic impact in terms of health care expenditure and lost working days despite their relatively benign nature. 1 Their clinical manifestation ranges from asymptomatic varicose veins to leg ulceration.2–7 In the United Kingdom, varicose veins affect nearly 40% of the adult population, of which 80% involve the great saphenous vein (GSV) alone, 10% the small saphenous vein alone, and 10% both. Furthermore, approximately 80,000 varicose vein procedures are performed annually in the UK.8,9 Standard surgical ligation and vein stripping (SL-VeS), of the great and small saphenous vein combined with saphenofemoral or saphenopopliteal disconnection, respectively, and phlebectomies has been considered the gold standard interventional treatment for varicose veins for more than 100 years. In recent years, alternative treatments, such as endovenous thermal ablation of the saphenous vein using laser (EVLA) or radiofrequency (RFA) as the heat generator, and ultrasound-guided foam sclerotherapy (UGFS), have gained popularity.10,11 Perceived advantages of the new techniques over traditional surgery include reduced periprocedural pain, faster recovery time, fewer complications, improved health-related quality of life (HRQoL) scores, and reduced need for general anesthesia.12–15
Research has primarily focused on beneficial clinical effects of minimally invasive techniques for varicose vein treatment. The NICE 16 guidelines recommend EVLA or RFA as first-line treatment and the Society for Vascular Surgery 17 and the American Venous Forum recommend EVLA, RFA, or UGFS as alternative treatments to conventional surgery. 18
Besides numerous reported outcomes in clinical effectiveness of treatment strategies in patients with varicose veins,19–21 critical questions regarding QoL remain unanswered. QoL has been defined as “the functional effect of an illness and its consequent therapy upon a patient, as perceived by the patient.” 22 The CEAP 23 classification (Clinical–Etiology–Anatomy–Pathophysiology) has been shown to be associated with severity of clinical symptoms of chronic venous disorders (CVD) and patient-reported QoL.24,25 HRQoL along with the development of various disease-specific measuring tools is now considered an important outcome parameter in studies investigating effects of treatments for varicose veins. 26 Besides the improvement in clinical status, the improving QoL in patients receiving these treatments has become an important treatment goal. Methods used to measure QoL may be generic, covering a wide range of health dimensions, or disease specific. Generic tools allow comparison across a population of patients with different diseases, whereas disease-specific tools are considered to be more sensitive at detecting minor changes in patient health status introduced by specific diseases.
This systematic review and meta-analysis was driven by the need to assess the effects of different therapeutic strategies among patients with CVD on the basis of QoL using various QoL scoring systems.
Methods
Aim of review
We sought to systematically review the current publications examining the impact of different interventional or conservative methods for the treatment of patients with lower limb varicose veins on their QoL. In particular, we sought to analyze the effectiveness of minimally invasive techniques compared with SL-VeS in patients with varicose veins in terms of QoL by comparing trials using a variety of generic and disease-specific questionnaires. The efficacy of each measurement tool was defined within each specific questionnaire. This review did not require any ethical approval since it was based on published studies and not individual participant data.
Search strategy
A computer-assisted systematic literature search of English language articles was carried out using the PubMed/Medline and SCOPUS databases to identify relevant publications which investigated patients with lower limb varicose veins and who received one of the following interventions: EVLA, RFA, foam sclerotherapy (FS), cryostripping (CS), perforate invagination stripping (PIS), subfascial endoscopic perforator surgery (SEPS), invagination stripping (IS), flush saphenofemoral ligation (FSL), or conservative management (C) compared to standard SL-VeS. The study potentially included randomized clinical trials (RCTs), systemic reviews, or meta-analyses. Trials not comparing different modes of treatment and articles studying patients with venous ulcerations were excluded. Search was limited to reports between January 2000 and December 2015. We used combinations of the keywords: varicose veins, interventions, QoL, surgical stripping, interventional methods. Further articles were identified through references of analyzed manuscripts. All publications retrieved after the initial screening (title, abstract, full-text reading) analyzing the QoL of patients after having received either the intervention or the conservative treatment, and any publications needing clarification were peer reviewed by two independent reviewers and in case of any inconsistencies in the participation or rejection of an article a third reviewer was left to judge its relevancy to the present study.
Data extraction
From the selected studies, we extracted the following data onto standardized data forms: (a) study characteristics such as first author, year of publication, study design, compared treatment modalities, CEAP score, number of patients, and/or limbs and follow-up period; (b) retrievable studies to be potentially eligible required the description of therapeutic strategies among patients with CVD on the basis of QoL using various QoL scoring systems. Outcome variables used were QoL measurements.
Questionnaires used in the studies
The QoL tools reported were Chronic Venous Insufficiency Quality of Life Questionnaire (CIVIQ 1 and CIVIQ 2), 27 Short-form 36, 28 Euro-Qol (EQ)-5D™ (3L version), 29 Aberdeen Varicose Vein Questionnaire, 30 SF-6D, SF-12, Venous Clinical Severity Score (VCSS), 31 VEINS-QoL/Sym, 32 Specific Quality of Life, Homburg Varicose Vein Severity Score (HVVSS), 33 and Outcome Response-Venous. The most frequently used tools were the Aberdeen Varicose Vein Symptom Severity Score (AVVSS), the EQ-5D™, and the HVVSS. AVVSS and EQ-5D™ instruments rate the patient’s QoL on a numerical scale, and differences in scores can be used to evaluate the effectiveness of therapies. The AVVSS score is a validated instrument to measure disease-specific QoL in patients with varicose veins. It produces a score from 0 (no venous symptoms) to 100 (worst venous symptoms).30,34 EQ-5D™ is composed of five items covering five domains (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each of which is rated at three levels (no problems (level 1), some problems (level 2), severe problems (level 3)), yielding 243 potential combinations of health states excluding death. Each health state is associated with a utility score by means of an additive function derived from the Dutch general population.29,35 Furthermore, EQ-5D™ consists of a visual analog scale on which patients can rate their health state from worst possible (0) to best possible (100). HVVSS includes varicose vein-associated symptoms (pain, heaviness, swelling, and itching), severity of varicose veins, chronic venous insufficiency findings (varicose veins, edema, pigmentation, dermatitis, active ulceration), and semiquantitative venous refilling time assessed by digital photoplethysmography.
Statistics
Thirty-five different RCTs were initially included in the review. After data abstraction we used Cohen’s d to make the outcomes of the reported scales comparable. Results from seven published RCTs were combined in a collaborative meta-analysis of 1047 patients performed at 12 months postintervention. For the meta-analysis performed at 24 months postintervention, results of six studies (n = 840 patients) were used.
The estimates were log transformed before conducting the analyses. After data extraction, the difference between intervention and SL-VeS in terms of QoL was assessed using the Cohen’s d for each study as well as the intervention applied and the scales used. The reason for using Cohen’s d was because the variance between the two groups is homogenous and the size of the sample does not play a part in the calculation. In contrast, we excluded Pearson r correlation because it is sensitive to data distribution as outliers can make values misleading. Heterogeneity across the selected studies was evaluated using the standard Cochran Q statistic, I2, t2, as well as Funnel plots. Calculations of heterogeneity statistics (Q statistic = 351.8, I2 = 98.3%, t2 = 0.53) showed that a random effects model should be applied to evaluate the difference between intervention and SL-VeS.
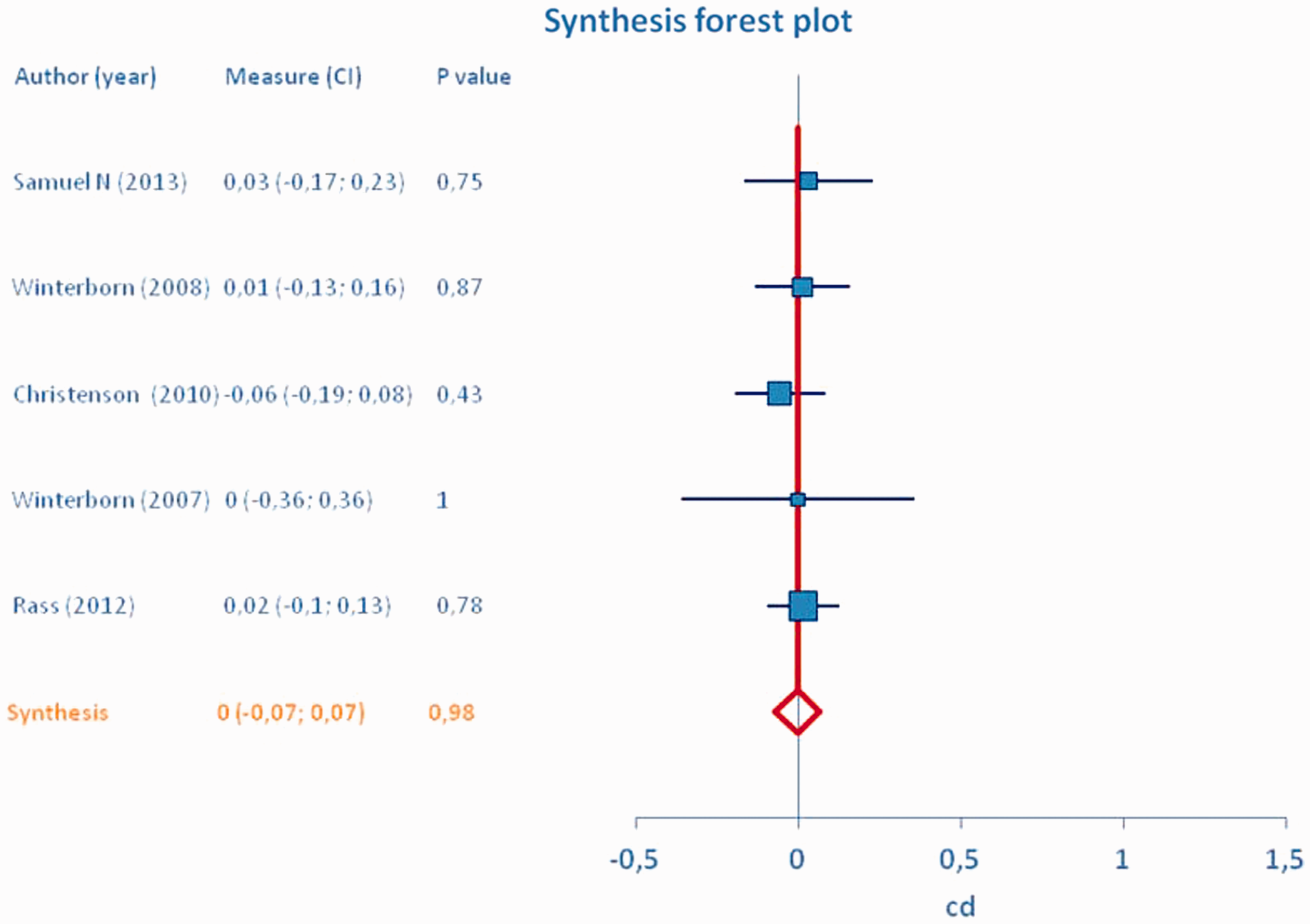
Studies were assigned weights using the inverse variance method. Sensitivity analyses were conducted to assess the impact of each study’s exclusion on the pooled estimates. Results were pooled at two different time points, at 12 months postintervention and at 24 months. Results are graphically displayed using synthesis forest plots in which the estimated reported scales values (with CI) for each trial and their average are marked along the length of a vertical line which represents “no difference in QoL measurements.” Analysis was carried out with the use of MIX 2.0 pro (Version 2.0.1.4).
Results
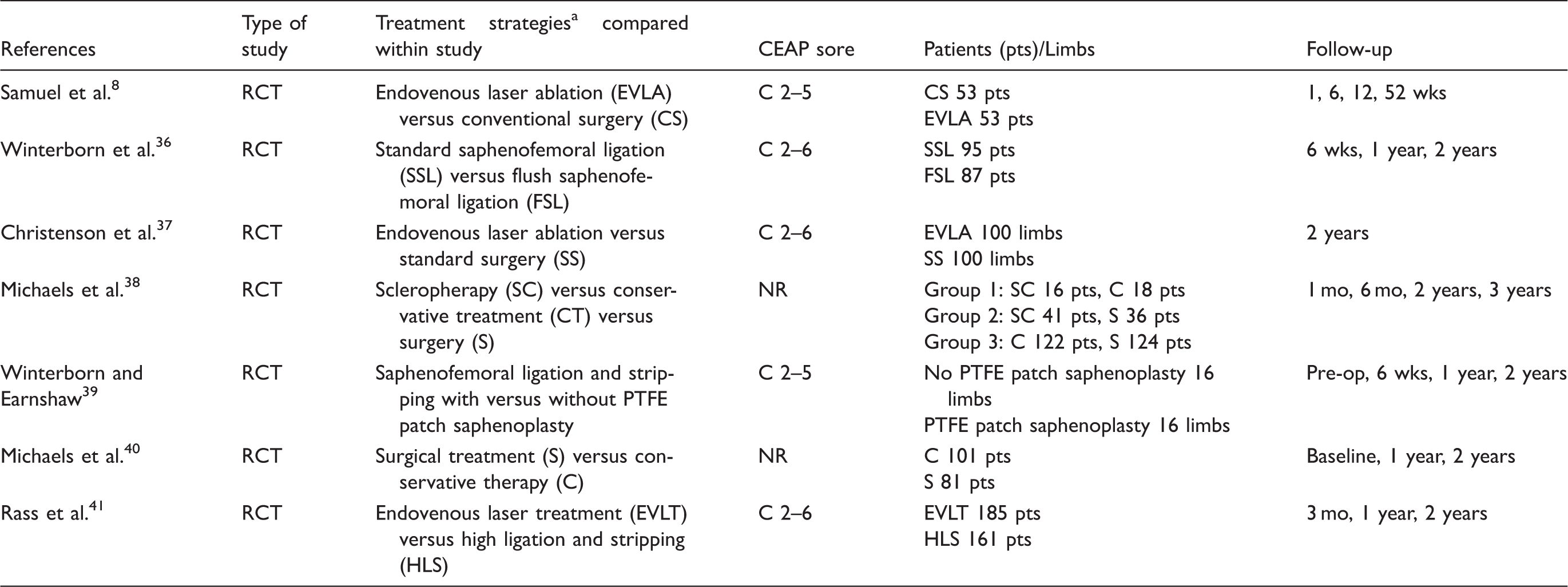
Study identification and selection flowchart is shown in Figure 1. The electronic database search and searching of bibliographic reference list identified 1642 articles of which 35 different RCTs were assessed for eligibility. Results presented concerned comparisons of several interventions. In 26 of these, reported comparisons concerned different intervention versus SL-VeS. Interventions reported across all included studies were RFA, EVLA, UGFS, FS, CS, PIS, SEPS, IS, FSL, and C. The detailed characteristics of the final seven trials providing appropriate data for statistical analysis are summarized in Table 1.8,36–41 A total of 1047 participants were randomized across all trials. The number of participants in a single trial ranged from 30
39
to 308.
41
The majority of participants in any trial were C2 on the CEAP score except for two trials38,40 where the CEAP scoring was not reported.
PRISMA flow diagram of the systematic article selection process. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Characteristics of literature included in the review. PTFE: polytetrafluoroethylene; mo: months; RCT: randomized clinical trial; wks: weeks. Abbreviations as reported in review studies.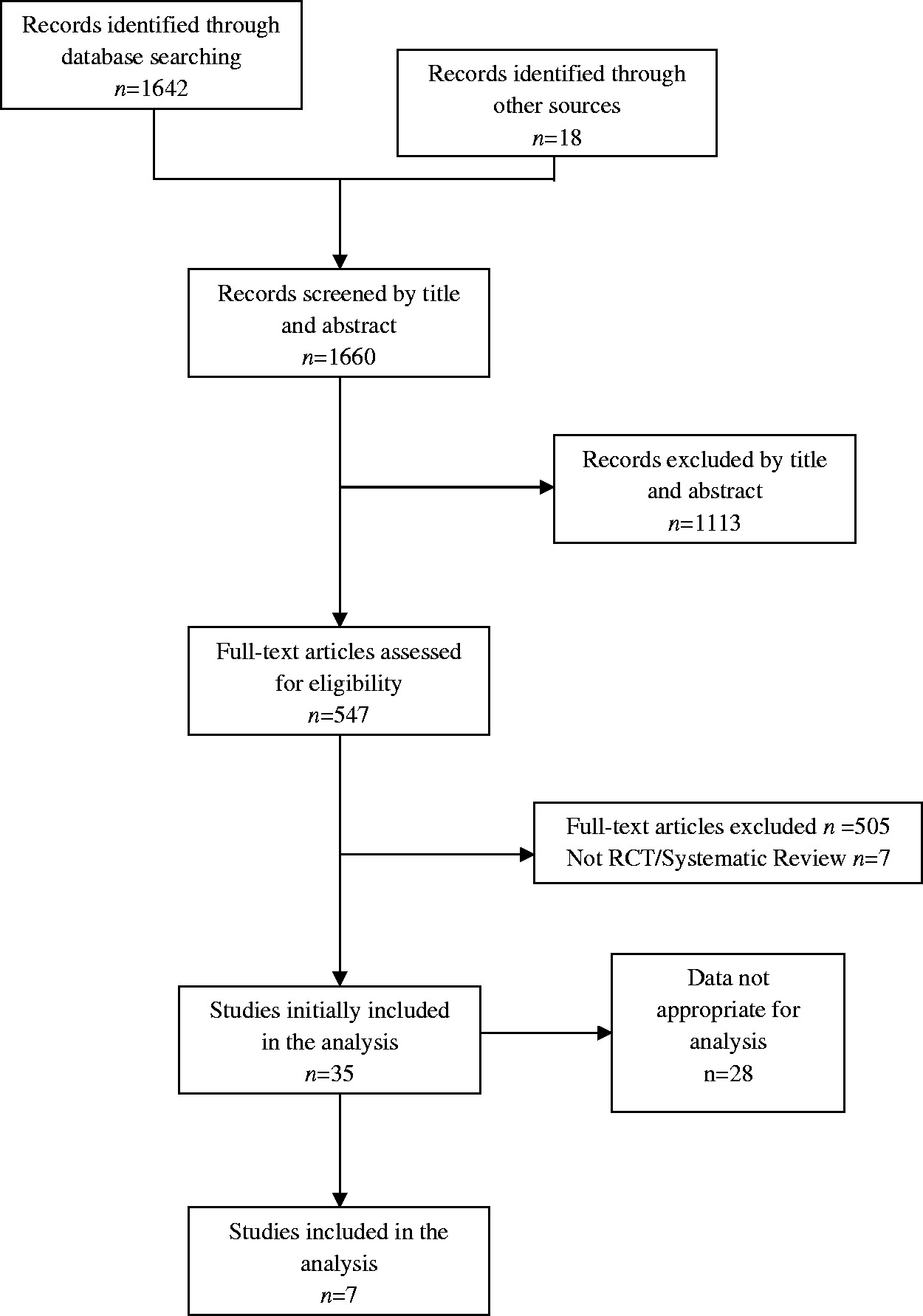
Data provided by each study for the meta-analysis 12 months postintervention.
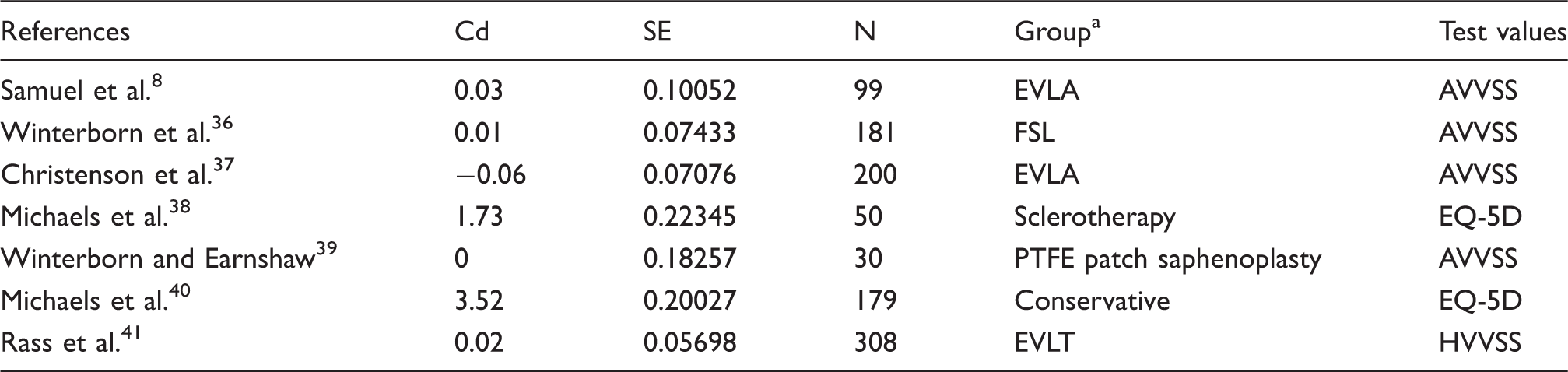
AVVSS: Aberdeen Varicose Vein Symptom Severity Score; Cd: Cohen’s d; EVLA: endovenous laser ablation; EVLA: endovenous laser ablation; EVLT: endovenous laser treatment; FSL: flush saphenofemoral ligation; HVVSS: Homburg Varicose Vein Severity Score; N: number of participants in the study; PTFE: polytetrafluoroethylene; SE: standard error.
Abbreviations as reported in review studies.
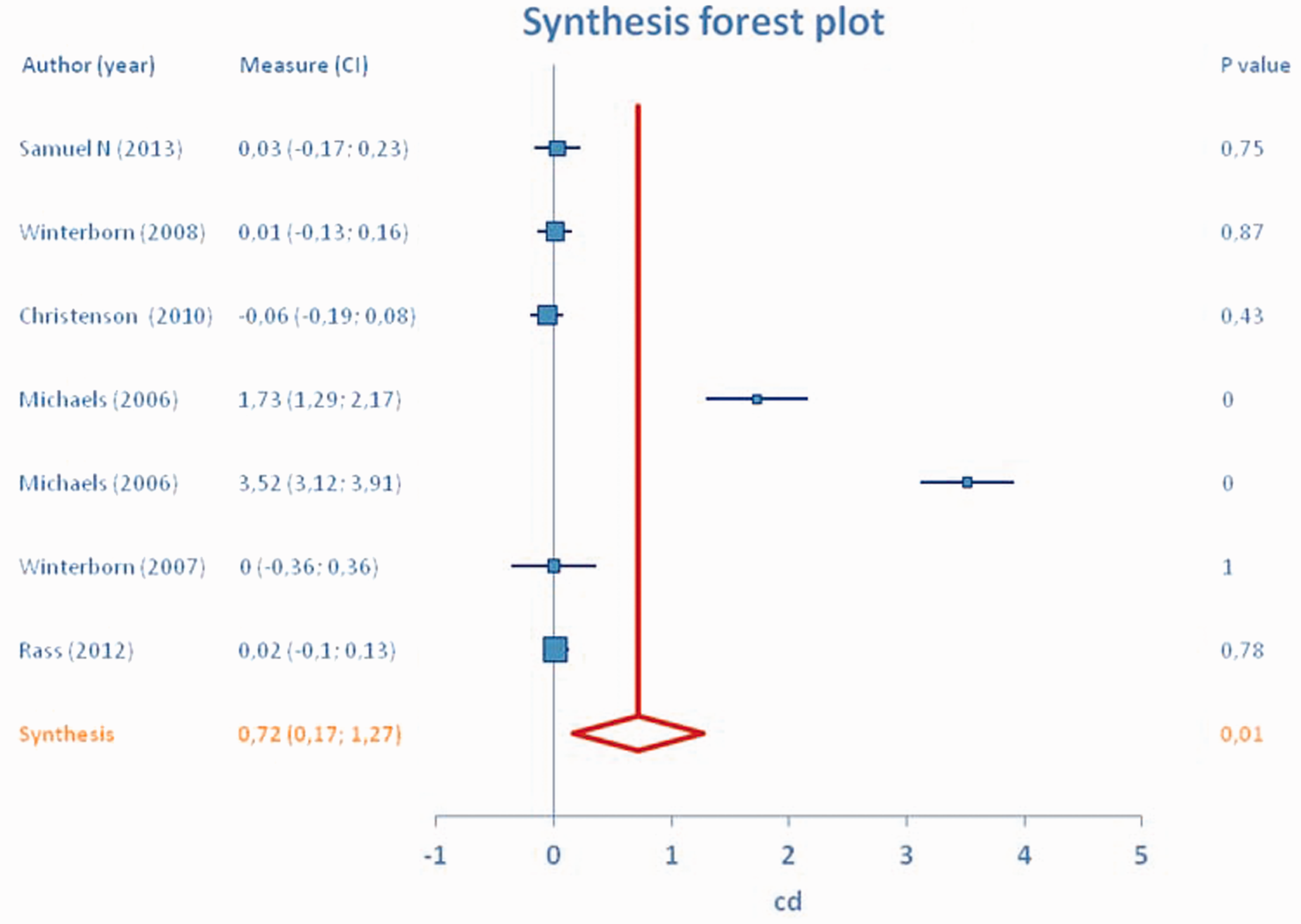
Synthesis forest plot for the 12-month postintervention meta-analysis. SL-VeS versus any intervention. SL-VeS: standard surgical ligation and vein stripping.
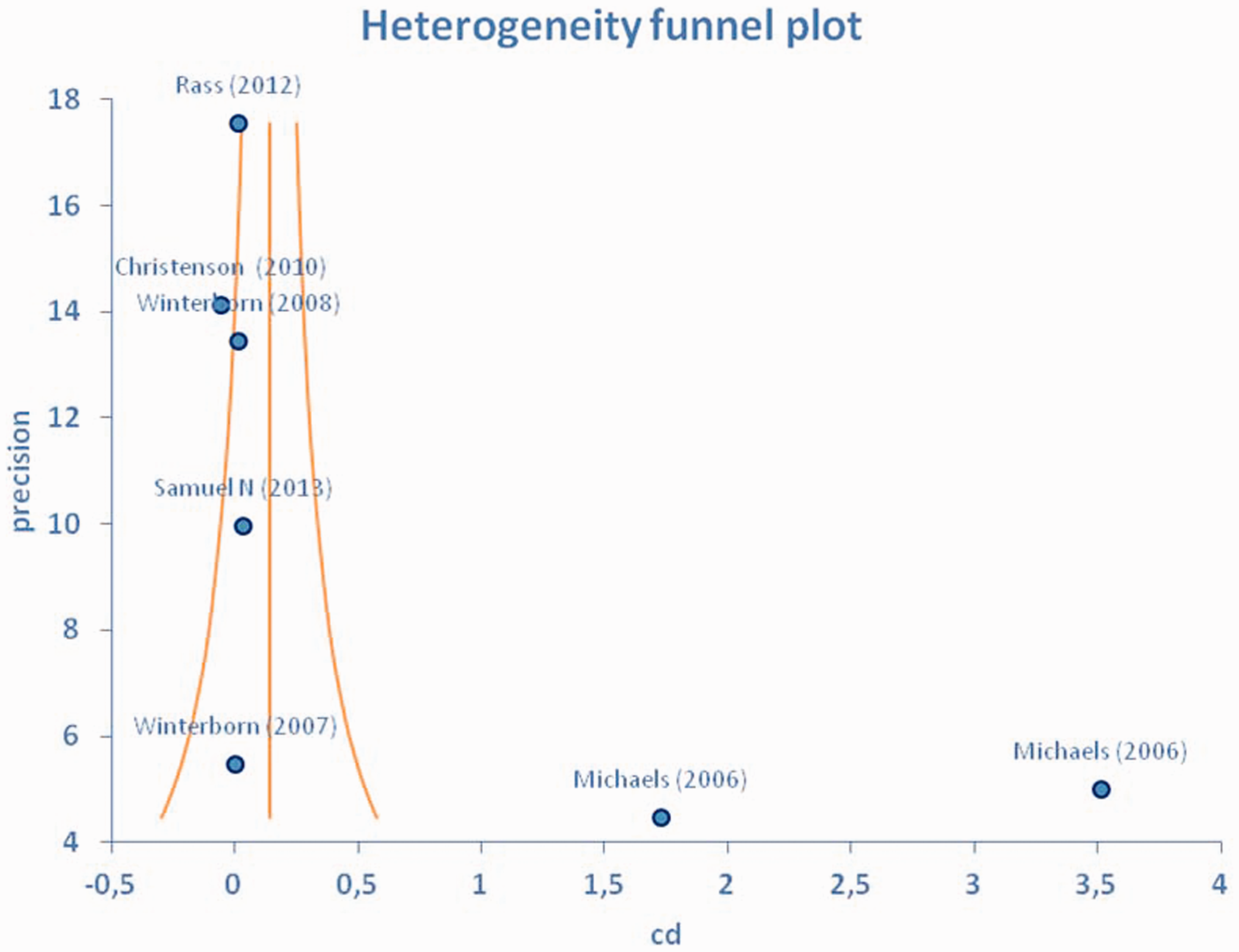
Heterogeneity funnel plot. SL-VeS versus any intervention. SL-VeS: standard surgical ligation and vein stripping.
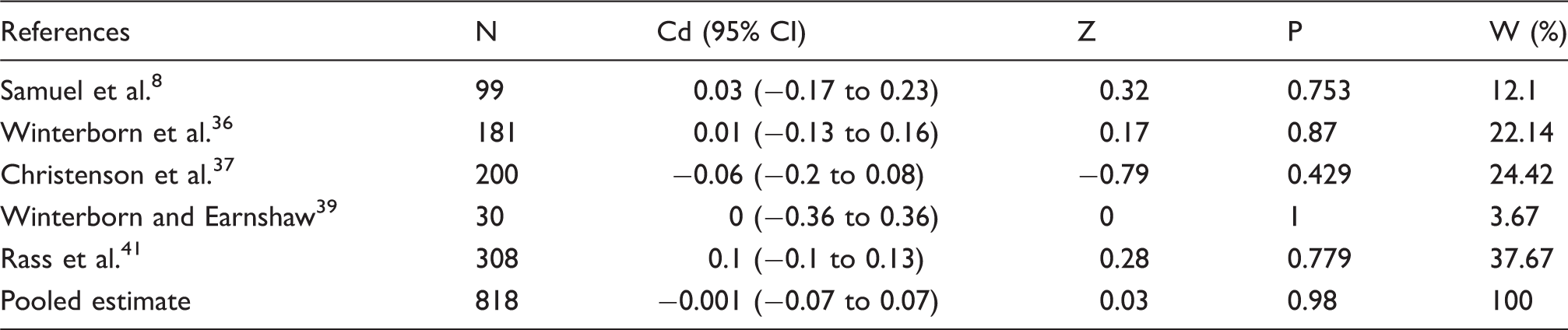
Cd: Cohen’s d; CI: confidence interval; N: number of participants in the study; P: P value; W: weight; Z: Z test value.
Data provided by each study for the meta-analysis 24 months postintervention.
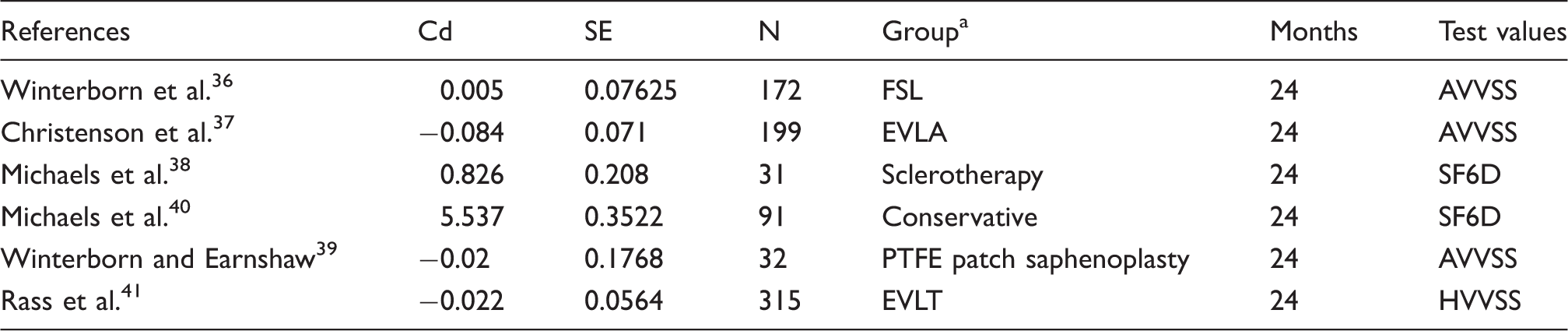
AVVSS: Aberdeen Varicose Vein Severity Score; Cd: Cohen’s d; EVLA: endovenous laser ablation; EVLT: endovenous laser treatment; FSL: flush saphenofemoral ligation; HVVSS: Homburg Varicose Vein Severity Score; PTFE: polytetrafluoroethylene; N: number of participants in the study; SE: standard error.
Abbreviations as reported in review studies.
Synthesis forest plot for the 24-month postintervention meta-analysis. SL-VeS versus any intervention. SL-VeS: standard surgical ligation and vein stripping.
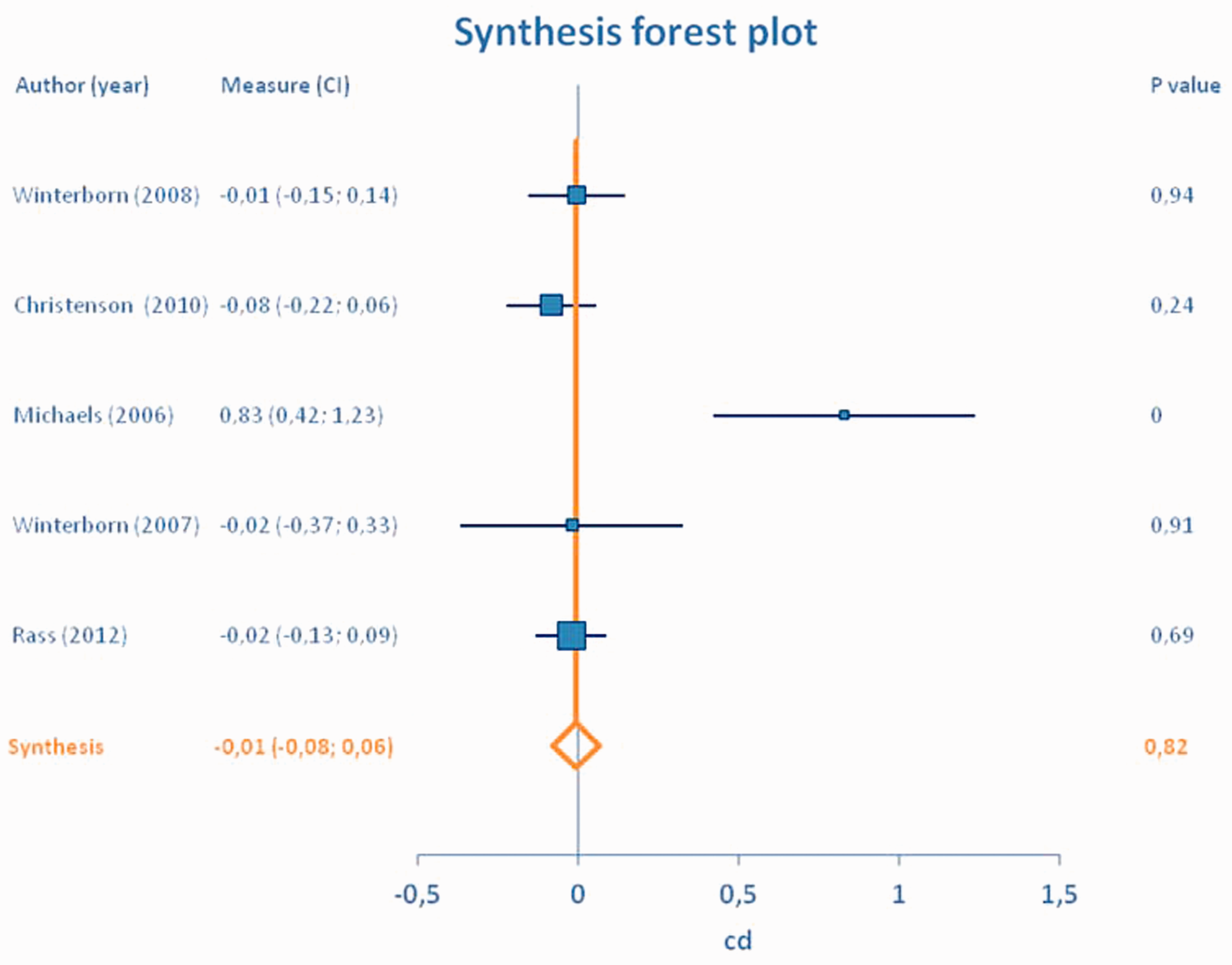
The effect of the reported treatment strategies compared to SL-VeS is negligible in terms of clinical outcomes and QoL measurement. Therefore, SL-VeS versus these interventional procedures were equally effective and safe approaches to treat GSV incompetence in terms of QoL measurements both at 12 and 24 months postintervention.
Discussion
Venous disease has received relatively little attention in the public arena and in vascular training programs, despite the fact that it is more prevalent in the United States than coronary artery disease, peripheral arterial disease, congestive heart failure, and stroke combined. 42 Recently, growing awareness and improvements in tools and techniques have piqued interest in venous disease. CVD has a significant impact on health care resources. Millions of people seek medical attention annually for varicose veins because of their cosmetic appearance or associated symptoms. Although often underestimated, the cosmetic consequences may impose an adverse effect on an individual’s QoL. An even greater socioeconomic impact is seen with more advanced venous disease. 2 Venous ulceration has dramatic consequences that impair an individual’s ability to engage in social and occupational activities, reduces QoL, and imposes financial constraints. 16 Furthermore, varicose vein recurrence is associated with a significantly worse QoL than is found among patients with primary varicose veins. 43 For all these reasons, QoL is considered to be an important secondary endpoint in several clinical trials investigating new treatment strategies for CVDs. Ultimately, the key question to answer is whether newer techniques provide besides better cosmetic results, also greater improvement in QoL score. Many papers disregard QoL outcomes and put too much emphasis on technical outcomes such as reflux and incompetent vein segments. We have attempted to do a true pooling, comparing various QoL outcomes for traditional stripping with newer endovenous techniques.
This study demonstrates that SL-VeS versus other interventional procedures are equally effective and safe approaches in terms of QoL measurements to treat GSV incompetence, both at 12 and 24 months postintervention, meaning that each strategy offers a clinically effective result alternative to traditional stripping. Venous symptoms adversely affecting QoL parameters may be more common than previously suspected and severity may not correlate to the size or type of refluxing veins. 44 The ideal treatment for varicose veins should be relatively noninvasive, repeatable if necessary, relatively safe, and free of significant complications. The fact that there has been no previous meta-analysis comparing surgery with other techniques for the treatment of varicose veins strictly in terms of QoL suggests that changes in QoL and symptomatic follow-up of these patients are much more difficult to measure than simple technical recurrence of the disease. However, QoL is an important outcome measure after surgical interventions for varicose veins. Several studies provide evidence of QoL improvement after varicose vein surgery in the great majority of patients. 45 Disease-specific QoL instruments are increasingly utilized in clinical trials as patient-reported outcome measures. 2
In our meta-analysis, there were no statistically significant differences between the various stripping techniques at either 12 or 24 months postoperative intervals. Our study included AVVSS and EQ-5D™ as health-related assessment tools and we found improvement in all domains which reached statistical significance in most of them confirming that all interventional methods proved equally effective. Due to this narrow difference in QoL between the techniques, other issues important to patients such as the less invasive nature of the procedure and the accomplishment of a better cosmetic result may be important in the choice of the procedure. Furthermore, one could take into account the cost-effectiveness not solely of the procedure itself but also the time to return to work or to the usual daily activities.18,37 In the same meta-analysis, 18 evidence showed that there is little to choose between the minimally invasive techniques in terms of efficacy or cost and each technique offers a good alternative to standard stripping, although minimally invasive treatments are marginally more cost effective compared to surgery in terms of quality-adjusted life year.
In a meta-analysis that evaluated 12,320 patients from 64 studies who had undergone treatment of truncal veins with RFA, EVLA, FS, or surgery, the results over 32 months were more sobering for sclerotherapy than for RFA and EVLA. The success rates, defined as vessel obliteration or complete removal, were 84% for RFA, 94% for ELA, 78% for surgery, and 77% for FS. 46 On the other hand, in terms of QoL considering these different techniques, our study showed that these treatments were equally effective in dealing with varicose veins in terms of QoL measurements, with no difference in time to resume normal activity or return to work. No difference was observed in the VCSS or in the Aberdeen score between the groups at 12 and 24 months of follow up. However, the possibility that the QoL in patients with CVD may depend also on other factors (e.g. obesity with long-term weight reduction hardly achieved, gender) that cannot be modified by venous therapeutic interventions should not be overlooked.
Possible indications for ligation and stripping of the GSV not favoring endovenous techniques are tortuosity of axial veins, GSV dilatation, or aneurysmal venous segments greater than 2.5–3 cm or large aneurysmal venous segment along the course of the GSV, economic consideration, and physician choice. Chronic thrombophlebitis, excessive tortuosity, and acute superficial thrombosis represent also relative contraindications to endovenous techniques However, ligation and stripping has decreased in popularity as a technique for treating GSV reflux because of the less invasive nature of endovenous techniques.
Although surgery remains the most commonly performed procedure for varicose veins, despite the high rates of recurrence, 47 the recently published guidelines of the Society for Vascular Surgery, of the American Venous Forum, 17 as well from NICE16,48 clearly state that EVLA, RFA, and FS are effective alternatives to surgery, conclusions that also match our present study.
Study limitations
In this analysis we have compared disease specific with generic questionnaires instead of running a separate analysis on both types. However, a major problem in comparing the validity of QoL questionnaires is the lack of a gold standard. In general, one approach to measure QoL is the use of generic health questionnaires which measure physical, social, and emotional dimensions of health. Another approach for assessing QoL is the use of disease-specific questionnaires. Since little is known about the comparative validity between generic and disease-specific questionnaires in patients with CVD, at least to date, the authors did not find any benefit of a separate analysis.
Another possible limitation of this study is the use of some physician-reported scores (e.g. VCSS) compared with patient-reported scores. However, we believe that by combining a patient-reported outcome with a clinical severity score should give a more sensitive outcome for treatment results.
Finally, there are no available data on QoL measurement in the perioperative period since the scope of our study was to assess the effectiveness of the reported treatment strategies in terms of QoL in the mid- and long-term period (12 and 24 months follow-up, respectively).
Conclusions
Venous reflux causes a myriad of symptoms and a wide range of therapeutic modalities exist that offer statistically proven symptom improvement. The purpose of this study was to evaluate the efficacy of various interventional methods for treating patients with varicose veins compared to standard SL-VeS in terms of various QoL measurement assessment tools. The procedures were at least equally efficient in treating patients with varicose vein disease in terms of QoL assessment tools at 12 and 24 months compared to standard stripping. Thus, the physical component of health is similar in treated venous disease. However, the results from available studies seem to suggest that a very large trial would be necessary to demonstrate a significant difference, if it exists, between the various methods.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.