
Abstract
Chronic Venous Disease is estimated at 83.6% of the global population. Patients experience pain, discomfort and severe complications with few effective therapies being available. Current strategies for the treatment of malfunctioning venous valves are invasive with a high recurrence rate. A prosthetic venous valve replacement is imminent, possibly providing better outcomes and improved general quality of life. In this review, prosthetic venous valves history is presented and assesses the advantages and disadvantages of developed venous valves. Articles that discussed potential designs of prosthetic venous valves were examined. A systematic search produced thirty-five papers fitting the inclusion criteria. Our understanding of the ideal abilities required in prosthetic valves has evolved. Developed valves are reported for regurgitation, migration and leakage. Issues have been resolved, but we are still away from the ideal valve. Improvements within the last eight years provided information on the importance of sinuses and prosthetic to venous wall-size mismatch.
Keywords
Introduction
Valves located in the venous system hold an essential role in the regulation of the flow pattern of the blood and are known to be passive flow regulators that react to the pressure change. 1 When the valves in the extremities shut, they prevent reflux and provide a one-way route for the blood to the heart. 1 These valves hold the same function as the valves in the heart that prevent regurgitation. 2 However, mechanisms may differ; but the goal is the same. In the heart, incompetent valves force the heart to work harder against the regurgitation force; eventually leading to heart failure. 3 In the lower extremities, incompetent valves allow gravity to force blood down, causing a pooling effect at the distal portion of the vein resulting in oedema. 3
Additionally, incompetent valves can cause stasis which gives rise to the risk of clot formation, varicose veins and in the advanced cases, a risk of venous ulcers; which are repetitive non-healing ulcers that put the patient at high risk of infection. 3 For decades, valve issues revolved around leakage, migration, thrombosis and more. In this review, the majority of issues are discussed with the ideal valve being addressed.
Methods
Reviews addressing venous valve implants were evaluated as well as articles which focus on emerging or potential designs of implantable venous valves. Prosthetic venous valve, valve sinus, and chronic venous disease management were used as keywords. The databases searched were PubMed, Science Direct and Google Scholar. Seven hundred and forty-five records were identified in this way. Twenty-eight more records were identified through books on venous disorders and the venous system. After removal of duplicated records, seven hundred and thirty-one records were left for screening.
The exclusion criteria used were vascular thrombosis of any type, management other than the jugular and lower limb venous system and year of publication before 2012. That decreased the number of records to seventy-eight. These records where then assessed for eligibility and were excluded if a stent was the focus of the record, if the solution proposed was not for a deep venous valve, or if the solution proposed was not an implantable venous valve. As a result, the records were decreased to thirty-five, which were used for purposed of this review. The below PRISMA diagram indicates the procedure used (Figure 1).
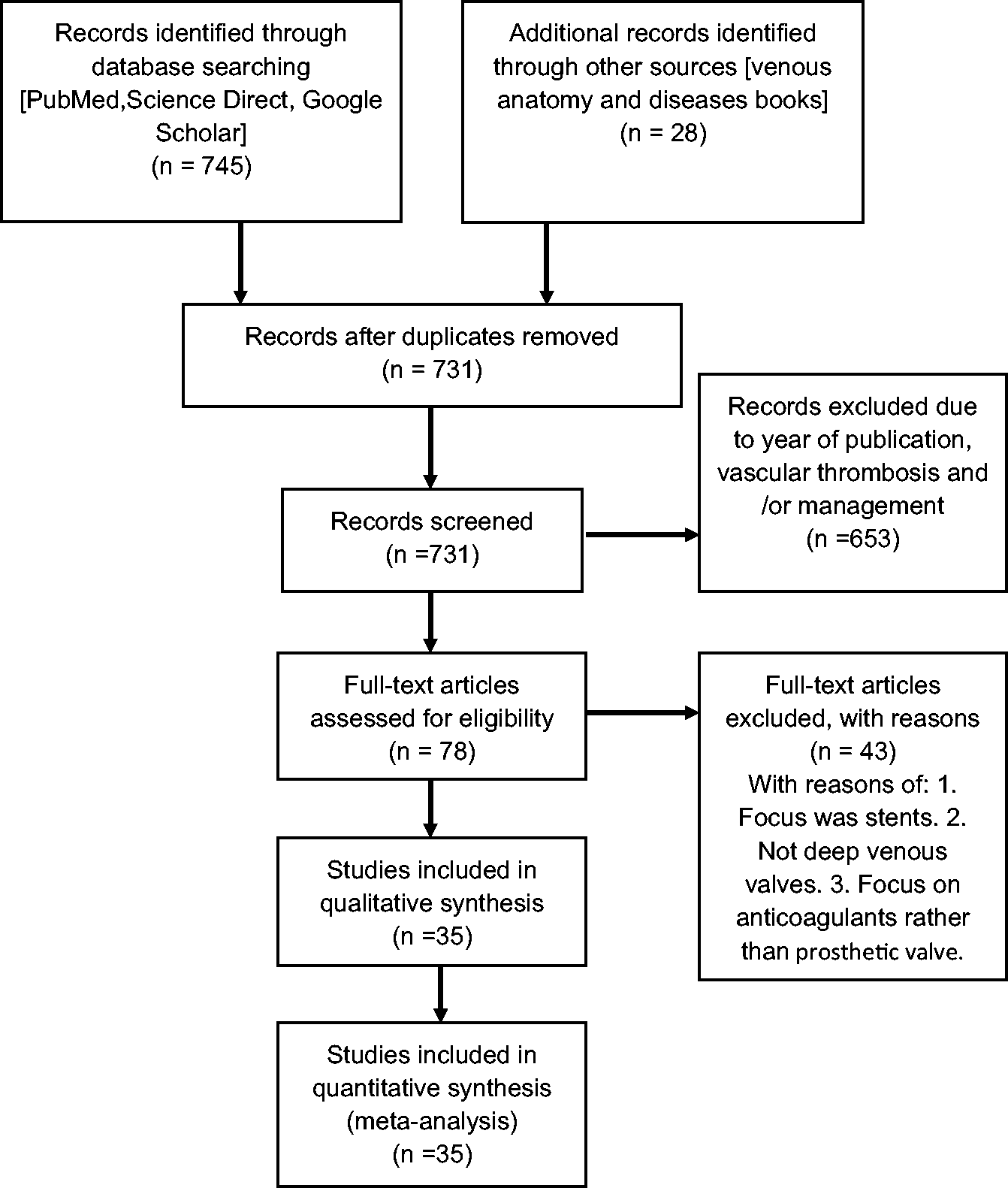
Manuscript PRISMA flow diagram.
Previous and current treatments for Chronic Venous Disease
CVD is a significant field in healthcare to target resources. Currently, therapy for CVD can be categorised into two sections; Conservative and interventional. 2 Conservative measures are aimed at reducing the symptoms, slow progression and improve quality of life. 2 These measures are mostly activity-related. One method involves raising one's legs to remove gravity's work on moving blood to the distal areas. 2 Two trials that were aimed at identifying whether exercise played any role in CVD were carried out. A randomised controlled study of CVD patients (50% with pre-existing DVT and 30% with deep venous post-thrombotic changes in doppler ultrasound) showed improvement in the hemodynamics of the venous flow after six months of exercise aimed at increasing the strength of calf muscles. 4 The second trial involved two medical centres in which patients with post-thrombotic syndrome (PTS) showed improvement in the severity of the disease and quality of life. 5 The medical centres focused on leg strengthening, leg stretching and aerobic workouts for six months. 2 The use of compression socks in the prevention of the PTS in patients who suffered DVTs has been deemed ineffective. 6
Due to current treatment options not providing the highest yield of benefits to the patients, a look into the need for prosthetic venous valves as an alternative treatment method was undertaken by a group of researchers. 7 Since the mid-1900's several designs, have been tested. The current review focuses on the main valve designs from 1960 to 2012. Recent discoveries in the years 2012 to 2020 will also be discussed. To date, valve designs have included single, double or triple cusp leaflets. 8 The materials chosen included allografts, xenografts or synthetic material which were attached to either a frame or a carrier. 8 Most of these have not been pursued further as they performed poorly in animal studies. 8 A long history of attempts at constructing biological and artificial venous valves exist. 2 The main factors to take into consideration when designing a valve include size, hemodynamic properties, type of prosthetic material and the method of installation. 2 The prosthetic material is usually placed on a stent or frame to allow surgical placement or percutaneous installation on a venous wall. 2 Most valves demonstrate good competency in a short period; however, factors such as thrombosis or/and hyperplasia limit longevity. 9
A short recap on the history of prosthetic venous valves
In terms of allografts; fresh allograft venous valve transplantations between dogs, with no rejection concerns, have been attempted. 10 McLachlin et al. tested 14 fresh allografts with 24 hours of full systemic anticoagulation in dogs. 10 7% of the 14 transplants were patent, and after a research period of 4 weeks, none were competent. Another experiment in which Gerlock et al. 9 reported that the valves were still functional after 6 to 8 months in the 1985 transplantation attempt of Bioprosthetic trileaflet cardiac valves made of glutaraldehyde-fixed pericardium along with a Dacron graft, into the inferior vena cava of 4 dogs. 9 Also, in 1985, Hill et al. attempted to transplant xenograft and artificial bicuspid tissue valves made of Pellethane polymer or tanned human umbilical vein into the jugular veins of 20 dogs. 11 Despite an anticoagulant regime, umbilical veins occluded after 48 hours, and all veins were thrombosed after eight days. 11 Kaya et al. in 1988, transplanted glutaraldehyde-preserved venous valves in dogs, with a distal arteriovenous fistula that was continuously functional for support. 12 Despite anticoagulation treatment which included heparinisation, all valves performed poorly after seven weeks.
Bicuspid valves with centrally hinged hemidiscs made of platinum or pyrolytic carbon-covered titanium were implanted in dogs in 1995 by Taheri and Schultz 13 Growth of neointimal hyperplasia rendered the valves useless within two years. 13 Human lyophilised saphenous veins containing a valve were tested by Reeves et al. in 1997 to determine viability for venous allograft transplant. 14
For evaluation, veins were lyophilised in vacuumed bottles and reconstructed in saline solution. All valves withstood the pressure of 350 mmHg, while one developed a leak under 140 mmHg pressures and above. Assessment of leaks was carried out by attaching the proximal end of each vein as well as a syringe to a pressure transducer and physiologic monitor (Figure 2). 14 The pressure was able to be monitored as it was applied retrograde through the vein against a closed valve. The veins distal portion is placed in water, allowing for any air escape to be evaluated across the closed valve to assess for any indications of a leak. Valve closure times ranged from 0.2–0.62 seconds and had a mean of 0.31 +− 0.03.
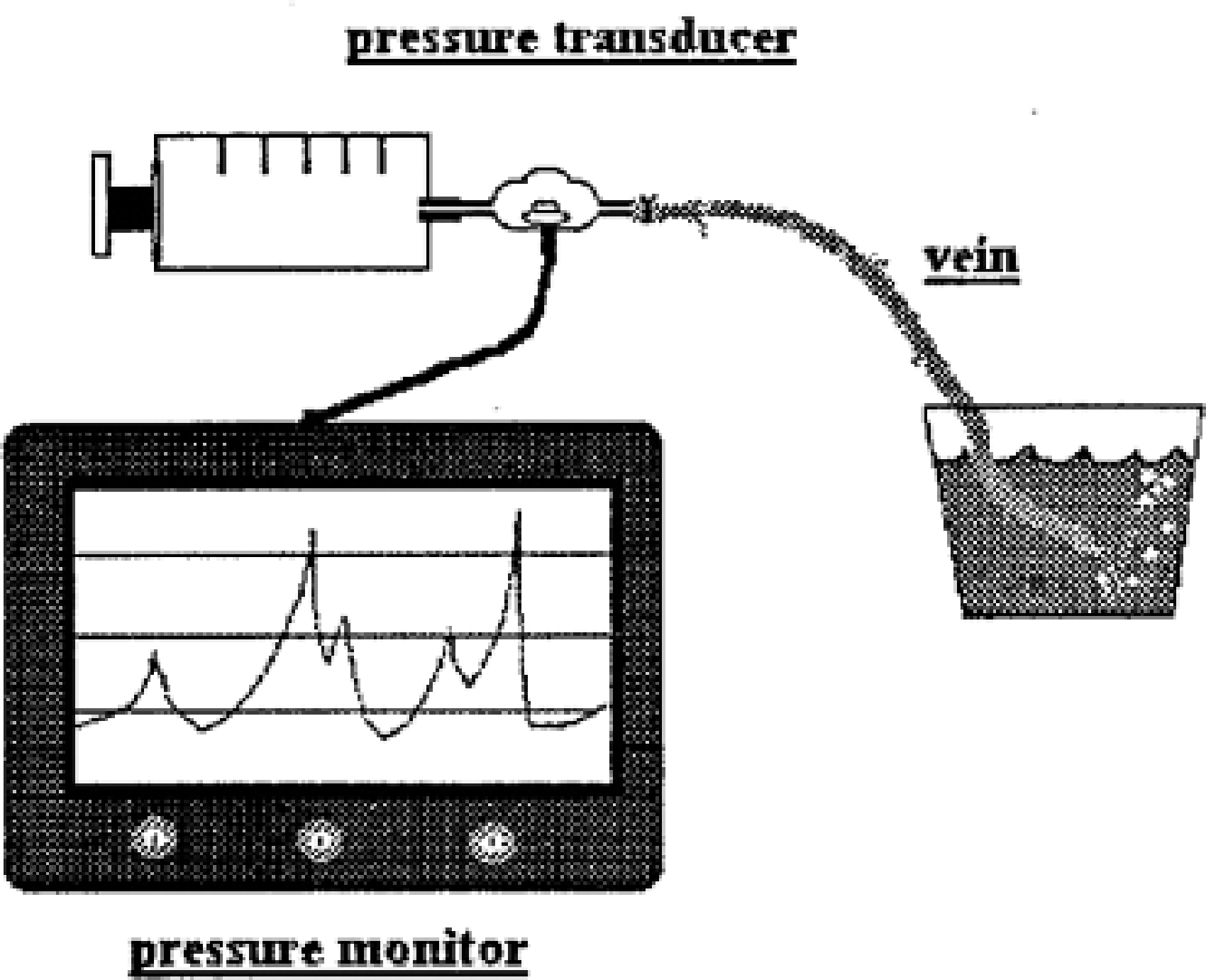
Maximum pressure testing. A valve leak is demonstrated by escaping air. With permission from Elsevier. 14
Teebken et al. 15 in 2003 attempted to develop a graft that possesses immunologically tolerated tissue-engineered venous valves that will be placed into the native vessel with hopes of restoring normal valve function. Twenty-four tissue-engineered grafts were grown using decellularised allogenic ovine veins as donor matrix, which would then proceed to be replaced by the recipients' myofibroblasts and endothelial cells. The venous valves were implanted into the external jugular vein. No anticoagulation therapy was mentioned, and after 12 weeks, all the tissue-engineered grafts were competent except for two. 15 The patent tissue-engineered valves were able to be distinguished from the control autograft valves with minor inflammatory reactions (Figure 3). 15
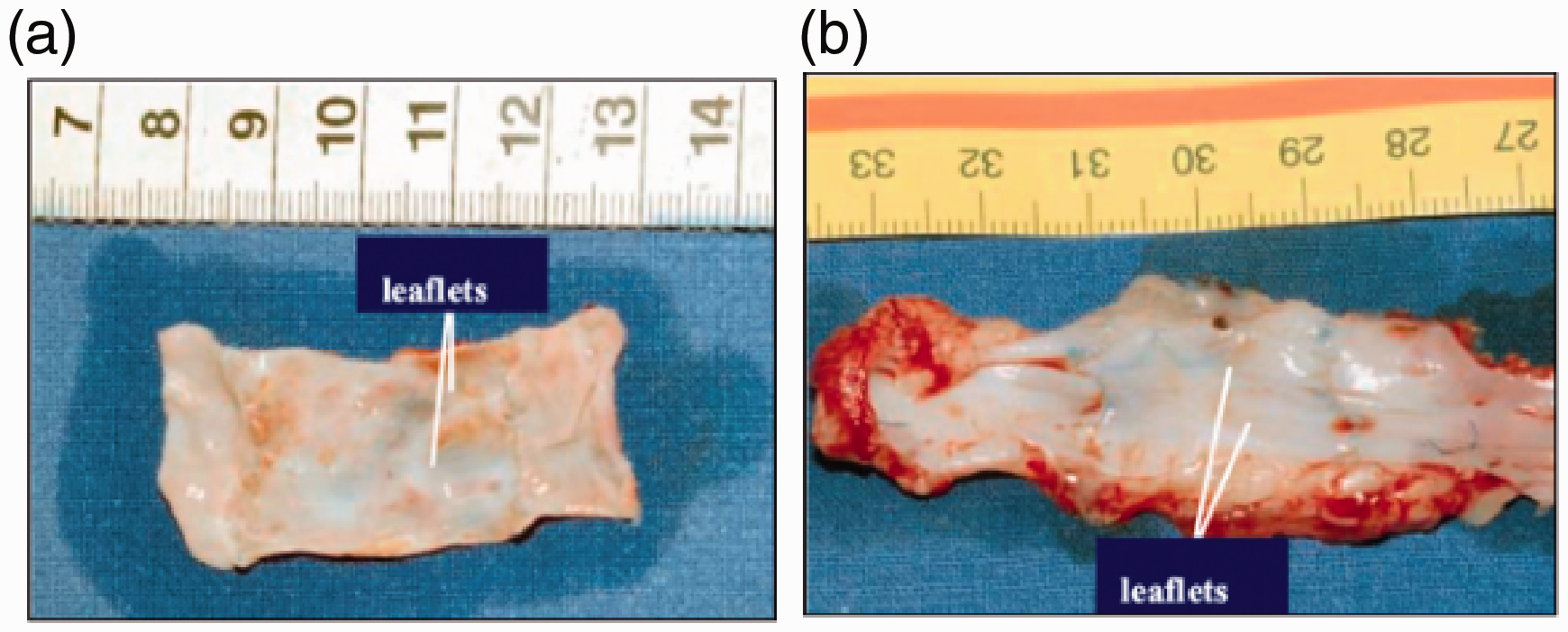
Tissue-engineered valved venous conduits: (a) small thrombi at the sinuses after one week, (b) after six weeks. With permission from Elsevier. 15
In 2002, Pavcnik et al. carried out a long-term study in sheep with percutaneous bioprosthetic venous valves (BVV). 16 The reasoning being that several attempts were made to develop prosthetic valves; however, none were followed up for a long-term period. This study aimed to test the BVV in sheep jugular veins and to assess the long-term function, competency, patency, stability and biocompatibility. 16 The valves were made up of square stents, with four barbs and a sheet of small intestinal submucosa sutured with prolene monofilament (Figure 4). 16 The positive of this study was that only one BVV failed to open as planned and migrated to the right pulmonary artery. The migrated valve was replaced with another viable one which remained intact. 16 Different sizes of the valves were available; which could be personalised for each patient. 16 One of the main findings of this study was that small intestinal submucosa valves are resistant to thrombosis. The negatives of the study were that the barbs penetrated through the vein wall in around 50% of the cases and valves tilted leading to reflux and thrombosis. 16
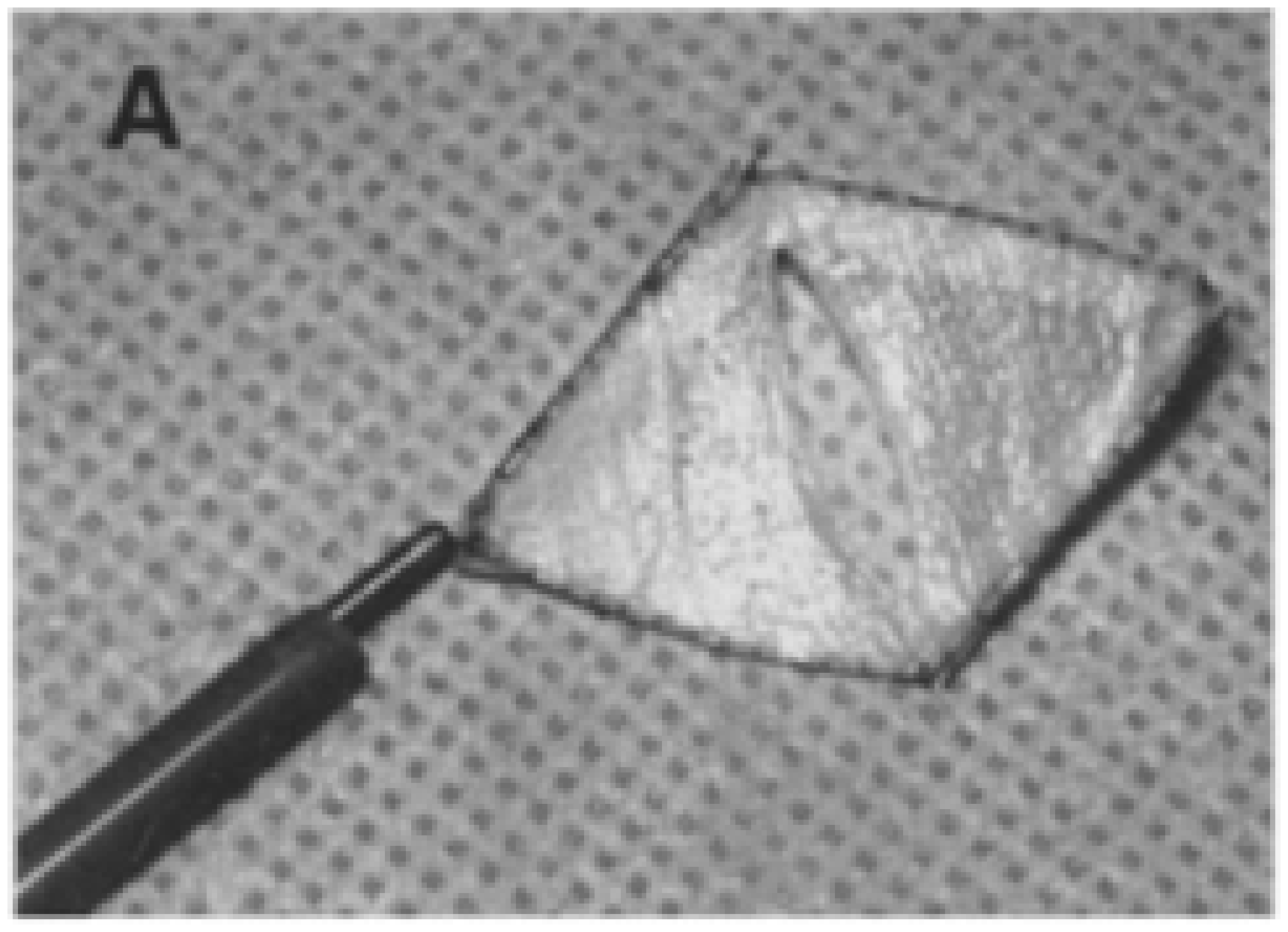
Bicuspid venous valve (BVV) 14 to 15mm in diameter A., Non restricted BVV 20mm long with four barbs retained by retention wire pusher connected to one barb. With permission from Elsevier. 16
Pavcnik et al. in 2004 proceeded to create a second-generation valve to try and combat the tilting of the valves, which led to thrombosis in the previous experiment. 17 The second-generation valve almost mimics the design of the first generation; however, to facilitate the BVV placement as well as prevent valve tilting, an additional stent was attached to the original. 17 Ultimately, two designs were made. One consisted of stainless steel valves while the other used nitinol. The final products were a Z stent BVV (ZS – BVV) and a double stent BVV (DS – BVV) as shown in Figure 5. 17
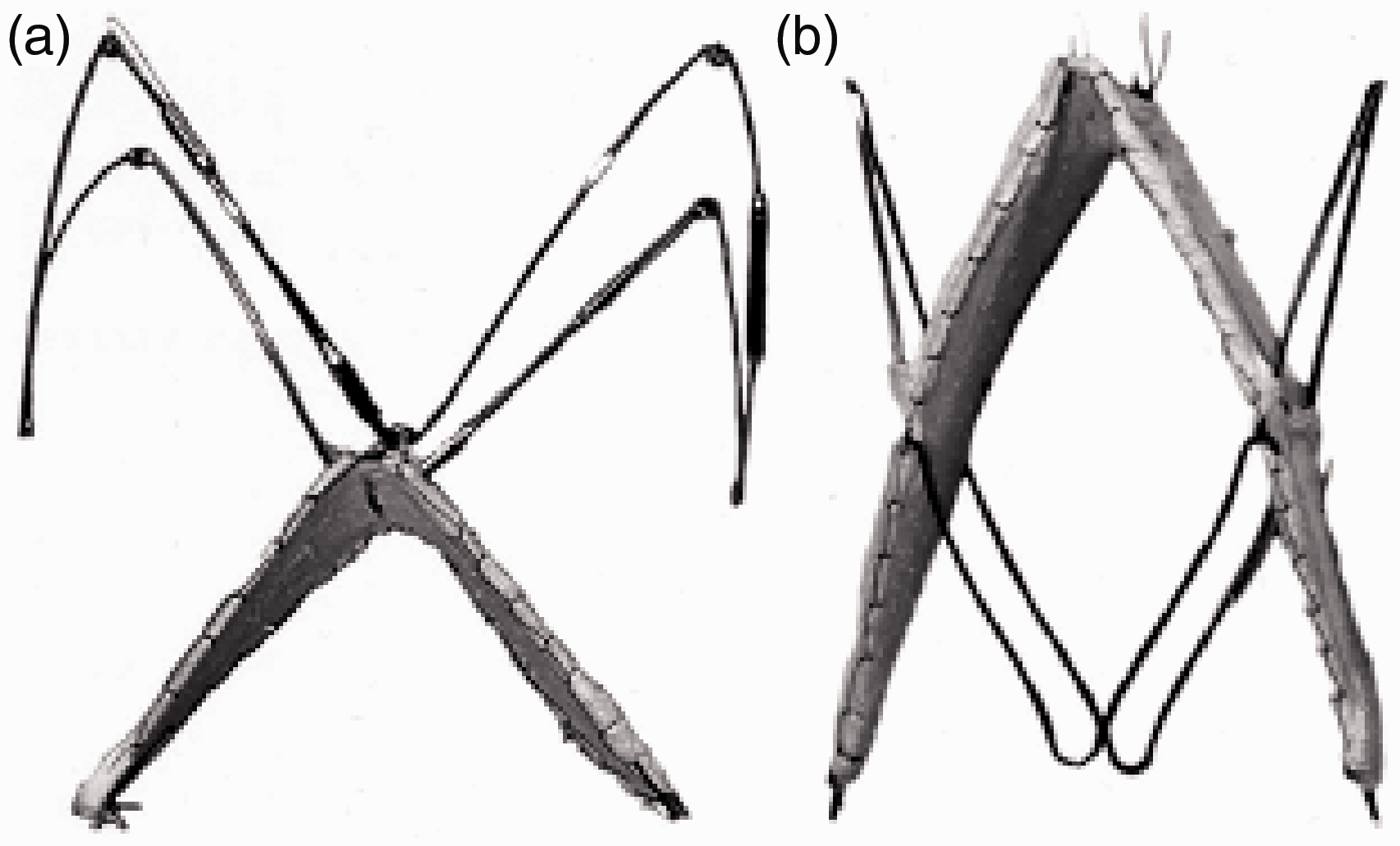
Second-generation bioprosthetic venous valve. A. Stainless steel Z-stent is attached to the apex of the original square stent-valve. Z-stent has barbs at its upper bends. B. Nonrestrained nitinol double-stent bioprosthetic venous valve with four barbs for maxima vein diameter of 12 to 14 mm. With permission from Elsevier. 17
In total, 48 valves were involved in the experiment. The conclusion of this second experiment found that the new valve design assisted in not tilting the valves in the veins. 17 100% patency was also noted at an immediate venogram and the 6 – week follow-up (see Figure 6 for 6-week follow up venogram). 17 However, of the 48 valves, four were no longer competent at the 6 – week follow-up as they had significant leakage. 17 Despite the successful removal of the tilting, the second generation BVV had certain drawbacks such as the stainless steel BVV requiring a large introductory sheath which was made by hand, which deemed it labour intensive. 17 The overlapping stainless steel square stent, which had an expansible force on the vein wall led to intimal hyperplasia. 17 Pavcnik et al. 17 therefore, in the end, suggested that future long term second-generation valves focus on the nitinol BVV as it had lesser drawbacks as compared to the others.
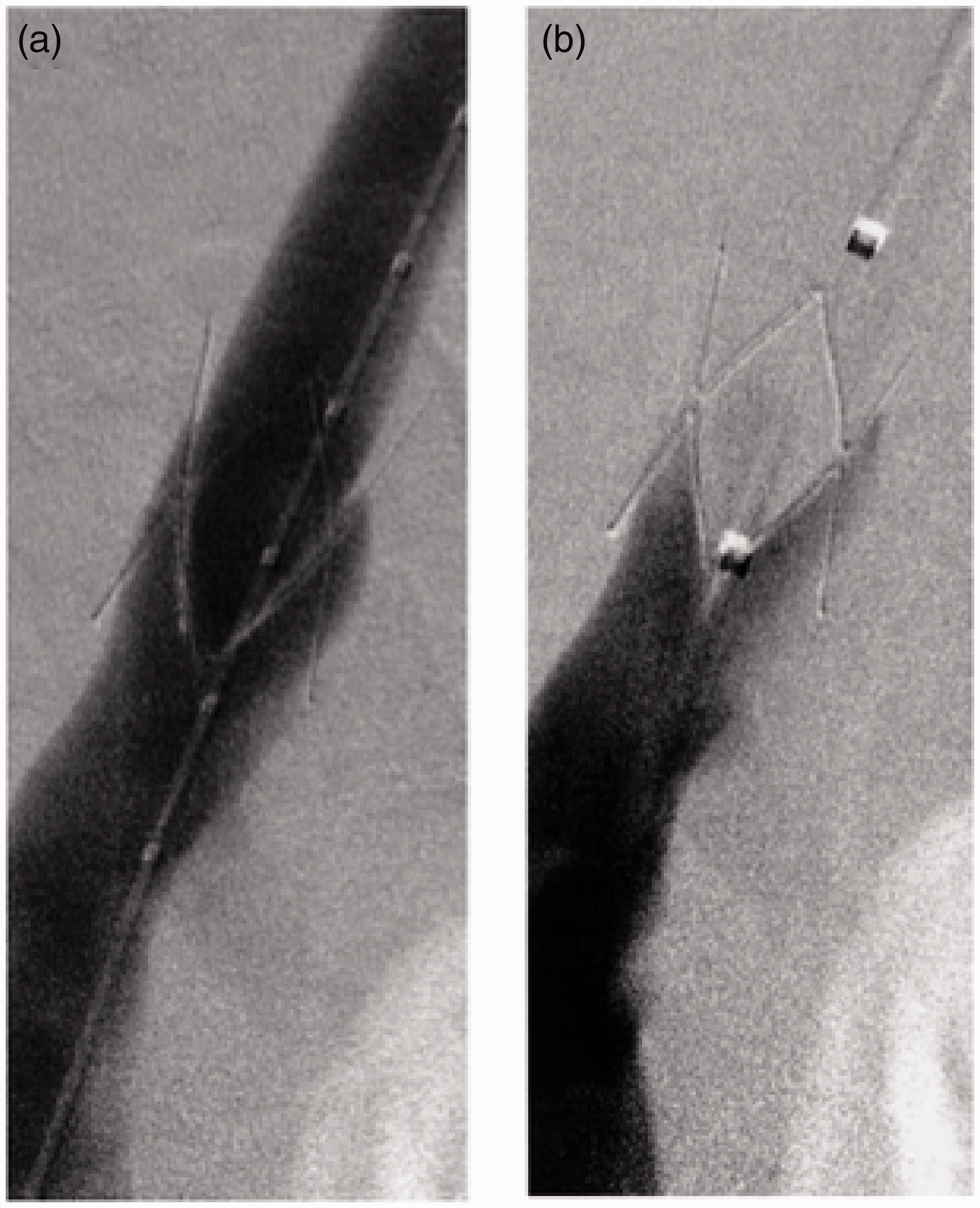
The function of double-stent bioprosthetic venous valve placed in sheep jugular vein 11 mm in diameter at 6-week follow- up. A. Jugular venogram with injection above valve demonstrates valve patency. B. High-volume injection of contrast medium below valve does not reveal any reflux and demonstrates valve closure. With permission from Elsevier. 17
Neovalves provide promise in this field as the idea is to be able to obtain and construct an autologous valve by using the patient's venous tissue. Theoretically, this should limit the risk of infections as well as thrombosis. Oscar Maleti produced one of the most notable neovalves. The procedure includes dissection of the vein wall and obtaining a flap that can function as a valve once appropriately fixed. This procedure was applied to 7 patients to whom the conventional operation was not a possibility, and initial results were promising. 8 In 2009, Maleti and Perrin 18 reported having tested their valves on 40 limbs in total using either monocuspid or bicuspid valves. The subjects were followed for a mean of 28.5 months, and 68% of the valves remained competent, with only 17% showing signs of ulcer recurrence or no initial healing. The study goes on to show that the technique constructed by Maleti held better outcomes than procedures such as transposition, valvuloplasty or transplantation. 8 Maleti and Perrin also mention that application of non-autologous artificial vein valves is not recommended in humans. 18 Opie et al. carried out a surgery that consisted of a monocuspid valve being applied to the venous system. 19 Fourteen surgeries were carried out in 11 patients, and a 48-month period follow up showed a 92% valve competency with zero claims of ulcer recurrence. 19
Post-2012 advancements
The progress post-2012 regarding valve development has been relatively slow. Not much has been published, which raises further interesting questions. Is there a valve on the market? Have the other treatment options started to outweigh the benefits of a prosthetic valve? Has funding been discontinued due to lack of progress made in recent years? Dalsing 20 mentions that surgical and percutaneous methods have been used; however, they have not been successful. To this day, there is no commercially available artificial venous valve that carries out the same functions as a native one, due to high failure rates and biocompatibility issues. 20
Recent advancements, however, have been made. Firstly, in 2012 Acosta and Kick 21 described their implantable design of a venous vein prosthesis that includes a cylindrical conduit with two leaflets in one opening. 21 Hence, this mimicry of the natural valve allows blood to pass in one direction. It is surrounded by a support membrane that contains attached struts that support the leaflets facilitating their collapse to close the valve preventing the backflow. This valve resembles the function of the native valve yet different in structure with the lack of any biological material. In 2013, Haverkost et al. took a step further to design a sinus or a socket to help the radial closure of the valve due to fluid dynamics. 22 The bulbous component of the valve prevents the fusing of the leaflets in the vein wall, and it is made up of different curvilinear chambers that together form a bulbous shape that will accommodate the changes of the lumen of the venous system by decreasing the pressure on the wall and give the valve flexibility to any change in the pressure. Also, the presence of the sinus will considerably clean the blood micro-thrombus that get stuck between the leaflets and the venous valve wall. Haverkost et al. suggests the option of using a radiopaque material that will be easily visualised under proper imaging, for better positioning of the valve in a natural orientation. 22 The ability to track the valve through imaging will help in decreasing the risk of improper placement of the valve. Also, Haverkost et al. explain the importance of the material of choice to make the leaflets in determining the shape of it. The type of material used will guide the shape of the leaflets to have optimal strain resistance due to the different properties each material possesses; for instance, leaflets that are made from stiffer material like PTFE can have a concave shape rather than a straight shape. 22
On the other hand, in 2017, Huang and Lu studied the biaxial behaviour of the venous in different valves on the jugular vein. 23 After doing peak stress tests (at 60% strain), tangent moduli were calculated to compare between different valves and inside the valve itself. It was found that there is inter-valve variability and intra-valve variability, as well. The variability of strain response between valves is multifactorial. It could be due to the difference in concentration of collagen. Collagen is one of the main structural proteins that surrounds the cells in the extracellular matrix. Collagen provides cellular stability and plays a role in controlling the properties of the tissue. Collagen distribution and organisation contribute to the valve's structural dynamics. For example, high collagen concentration in distal valves is consistent with higher tangent modulus. The orientation of collagen, its solubility, the thickness of the vein or the number of leaflets, the distal valves tend to be tricuspid rather than bicuspid; all are contributors to the variation in the valves’ behaviour. Also, the valve itself behaved with anisotropy and non-linearity, mainly the proximal ones (p<0.01), meaning that there was a difference in the behaviour of each leaflet of the valve. In 2019, Benson and Haung worked more on the tissue composition of bovine the jugular valve to study the anisotropic behaviour of the valves. 24 By studying the distribution of elastin and collagen in the extracellular matrix and their orientation, it was found that the collagen aligns circumferentially while elastin orients radially which is causing the valve to be more compliant toward the radial direction as opposed to that of the circumferential one. 24
Recently, more attempts at producing a sustainable valve have been noted. In 2018, Garcia et al. 2 published a paper where three valves were being investigated in both animals and humans. 2 The first one was known as the Blueleaf system. The Blueleaf system 25 is a valve that was similar to the Maleti one, as it was non-implantable, and the valve was an autologous one created from the vein wall. The procedure is carried out percutaneously with the assistance of ultrasound. This technique has been performed in cadavers, animals and was attempted in two humans. No results of either have been published. The second valve discussed by Garcia et al. was referred to as the SailValve (Figure 7). 26 The SailValve is a self-expanding valve made of polytetrafluoroethylene (PTFE) cusp that floated in both directions. It was inserted in five pigs, in ten iliac veins. Two of the ten valves were reported as mispositioned, and 5 of the remaining eight were fully functioning at weeks 2 or 4. No thrombosis was reported on any valve. 26 However, a follow-up paper on the SailValve reported progressive inflammatory reactions occurring on the valve. 26
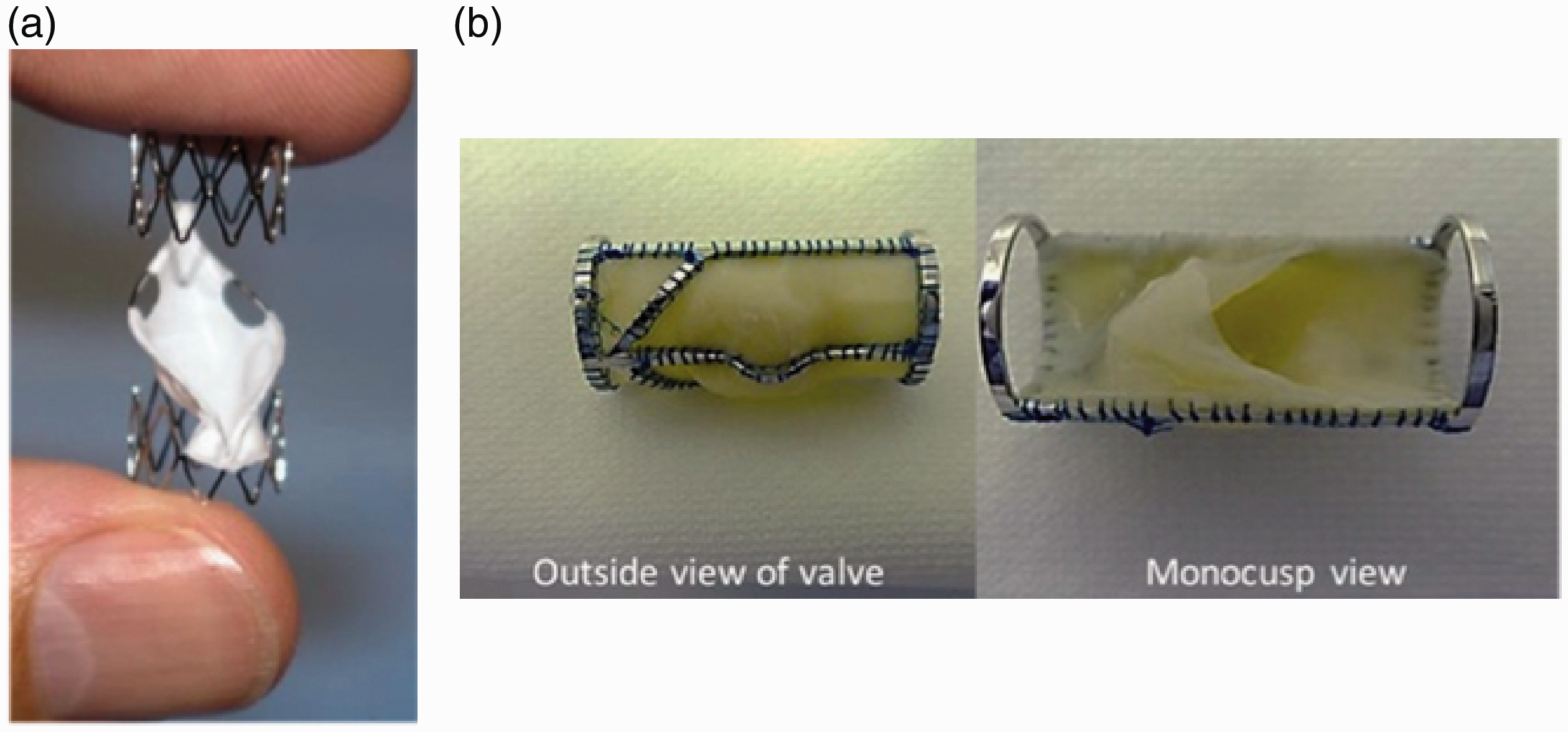
A. The SailValve is self- expanding and consists of a single polytetrafluoroethylene cusp that floats in both directions. B. Monocusp valve (VenoValve) derived from porcine heart valve placed on a cobalt metal frame. The tissue covers half of the ring, as shown in the image. With permission from Elsevier. 2
The final valve discussed was the VenoValve (Figure 7). 27 It consisted of porcine-derived monocusp from the heart valve and was mounted on an alloy frame with a 3-mm sinus protrusion. It is surgically placed at the target site via the femoral vein and is placed securely with running sutures on both ends. This procedure allows the surgeon to tailor the inflow and outflow through the valve. 2 The ability to surgically place a valve could be crucial as it is an essential factor for optimal venous flow. 2 This valve has been tested on animals, and a human trial is pending. Although no advancements have been made in designing an actual valve, the understanding around what an ideal valve should consist of is getting stronger. Currently, through different publications, there is a better understanding of factors that may affect a valve's functionality, and these can be addressed in future designs. Examples of some of these factors include the importance of sinus pockets 1 as well as prosthetic - vein wall diameter mismatch. 28
The future of prosthetic venous valves
It is challenging to address the future of venous valve prosthesis as at the moment. There seems to be no promising prototype that provides the longevity required. For the ideal valve to be created, several requirements need to be met. These are requirements that will ensure the full functionality of the valve, as well as ensure no side effects, and longevity can be guaranteed. Requirements are:
Surgery type
The ideal surgery type is a minimally invasive one. Most preferably a percutaneous surgery as this allows the patient to be able to exercise and return to regular activity after a day of the procedure. The procedure is also beneficial as it causes less pain post-op and leaves a smaller scar in comparison to regular surgery. 29
Sinus pocket
Research done by Tien et al. 1 found that the majority of venous valve designs did not include sinus pockets and are also often attached in non-sinus segments of veins. 1 Their study aimed to establish whether the sinus pocket had a role to play in the flow dynamics and whether new designs should start to consider adding sinus pockets. They concluded that sinus pockets altered the flow around the valve and regulated the flow. The alteration could play a role in reducing the number of thrombotic cases in post-op patients. 1 Along with the above mentioned, the sinus pocket has been reported to hold several other benefits; such as, avoids flow stasis, 30 reduces substantial stress on valve leaflets, 31 assists in the closure of the valve 32 and lowers wall shear stress. 19 Keeping the advantages as mentioned above in mind, all future prosthetic developments will benefit from adding sinus pockets in their designs.
Prosthesis-vessel diameter mismatch
In 2016, Tien et al. published a paper on another variable that could contribute to valve functionality. 28 This study aimed to assess whether size mismatch had any effect on venous valve function and to discover what mismatch limit affects the hemodynamic performance. The study concluded that valve regurgitation volume, closing time and pressure difference was elevated significantly when a mismatch ratio of greater than ∼ 15% existed. The final findings stated that there is a relationship between valve size matching and the hemodynamic performance of the valve. Tien et al. went a step further by suggesting that future valve implants for the treatment of CVD should have a size mismatch of <15% to optimise hemodynamic flow. 28
Tilting
One of the reported difficulties that venous valves faced included the tilting of the valve. The tilting of the valve would cause turbulent flow and eventually cause thrombosis. Possibly a more in-depth look into what Pavcnik et al. did in the second experiment to remove tilting from the veins can be taken and implemented in most valves. 17
Thrombosis
Thrombosis is one of the main issues that prosthetic venous valves face. Thrombosis can be caused by anything from a narrow valve, to a tilted valve. Therefore, the design of the valve needs to make sure that blood flow remains the same as it did with the native valve or arguably even better. Thrombosis, however, has been addressed by several valves that reported no cases of thrombosis. Most notably in small intestinal submucosa valves - resistance to thrombosis was noted in one of Pavcnik et al. 16 initial publications.
Migration
Similar to tilting, migration of the valves is a recurrent issue that intravascular prosthesis face. This issue has yet to be resolved in cases where migration did occur. There has been no publication addressing the issue of migration of valves and how to address it, other than replacement of the said valve. However, the solution to this could be to compare and contrast the valves that had migration incidences with the valves that had no incidences reported. The comparison could reveal the cause of migration and could be addressed when designing future valves.
Longevity
It is beneficial for the patient if the valves can maintain optimum function for an extended period. The longevity will reduce the number of surgeries required, would reduce the financial cost of patients and will overall improve the quality of life. Zervides and Giannoukas suggest five years as the optimum time for the valve to be able to function correctly. 8
Leak
Leaks have been reported in several valves where the pressure from the flow overpowered the valve or valves not being fixed correctly to the lateral walls. Leaking is a severe issue as it may not resolve the reflux issue. It is best to confirm the valve's capacity to handle high-pressure flow as well as to ensure correct attachment to the wall to avoid any cases of leakage.
Material
Zervides and Giannoukas, in their review of a range of prosthetic venous valves, concluded with their thoughts on the ideal venous valve. 8 Amongst their ideas, they mention that either synthetic or biomaterials should be used for the valves. As through their review, they discovered these materials to be the most beneficial. Along with synthetic or biomaterials, Haverkost et al. suggest the usage of a radiopaque material for better positioning of the valve. 22
Durability and stability
It goes without mentioning the importance of the valve to be durable and stable. The valves need to maintain their primary function through a diverse range of physiological conditions and not get damaged. It is therefore suggested that the valves go through stress tests – such as the one carried out by Reeves et al. 14 As normal pressure in large veins has been reported to be around 4–15 mmHg. 33 Most cases of CVD patients also develop venous hypertension. It is, therefore, safe to assume that the pressure in the large veins of such patients, is much higher than the pressure range mentioned above. Therefore, stress implemented on valves should be considerably higher to account for an increase in pressure that is associated with CVD, increased cardiac output and other conditions that can elevate venous pressure. Zervides and Giannoukas suggest no migration under pressure differences of up to 200mmHg is the standard that future valves should be aiming for. 8
The importance of the durability of the valve in the veins has been discussed in detail by Zervides et al. 34 In this specific paper, Zervides et al. mention that a person standing inactively for an extended period will experience full hydrostatic pressure gradient in the venous system. The veins in the foot would potentially have a pressure of 100 mmHg.The importance of the valves is noted when there is a need to alleviate the transient maximum that would occur if posture change occurred – such as that of a person standing up from a sitting or lying position. 34 Zervides et al. mention that if a valve was missing or had incompetency in the legs, a posture change would result in the doubling of the final standing pressure. 34 It is therefore suggested that incompetent valves cannot provide maximum shielding against this transient change and thus can end up causing the formation of varicosities. 34 It is, therefore, crucial to also test future prosthetic valves in their ability to withstand pressure gradients from statuses of low pressure to a sudden increase, – to mimic the action of a person standing up from a sitting or lying position.
Microstructure
The behaviour of the jugular valve sheds light on the importance of considering the microstructure of the valve in order to come up with a design that resembles the native valve with the least side effects possible. 24 Further studies need to be done to accurately quantify the microenvironment of the venous valve hence prevent any incompetence and improve the existing designs.
Conclusion
The primary purpose of this review was to shine a light on the lack of progress made on prosthetic venous valve post-2012. The lack of progress leaves room open for prospective valves to be designed and experimented as the ‘ideal’ valve is yet to hit the market. The ultimate goal is to be able to have a valve that is easy to place, maintains proper functionality, does not cause thrombus formation and has longevity. Prosthetic valves have the potential to be implemented in two situations. Firstly, as an elective decision for a patient in the early stages of chronic venous disease who does not wish to wait until the end stages to get a replacement. Implementing a valve that functions well and provides longevity could be a viable option. Secondly, in patients whose quality of life has been reduced, and no other treatment options seem to affect. These patients can also consider valve implementation. Attempts have been made in designing valves. However, a positive step towards a final valve design is yet to be achieved; this is primarily due to the complexity of the physiology that surrounds blood flow, primarily through a valve. The recent publications surrounding the better understanding of what the ideal valve should consist of provides hope in this field. The results of future studies carried out in this field are awaited with great enthusiasm.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This research was excluded from ethical approval from the University of Nicosia Medical School Research Committee.
Guarantor
CZ.
Contributorship
CZ, conceived the study and got it approved and excluded from ethical approval by the University of Nicosia Medical School Research Committee. HM, RAS and HJ researched the relevant literature and co-wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
No.