
Abstract
Objective
To investigate and compare the outcomes of the available treatment modalities for anterior accessory saphenous vein (AASV) incompetence.
Methods
A systematic literature search was performed in MEDLINE, Embase, and the Cochrane Library. Studies reporting the outcomes of patients who were treated for primary AASV incompetence were included. The methodologic quality of the articles was assessed using the Methodological Index for Non-Randomized Studies (MINORS). A random-effects model was used to estimate anatomic success, defined as AASV occlusion. The secondary outcomes were pain during and after treatment, venous clinical severity score, quality of life, esthetic result, time to return to daily activities, and complications.
Results
The search identified 860 articles, of which 16 met the inclusion criteria. A total of 609 AASVs were reported. The included studies were of poor or moderate quality according to MINORS score. The pooled anatomic success rates were 91.8% after endovenous laser ablation and radiofrequency ablation (EVLA, RFA, 11 studies), 93.6% after cyanoacrylate closure (3 studies), and 79.8% after sclerotherapy (2 studies). The non-pooled anatomic success rate was 97.9% after phlebectomy and 82% after CHIVA. Paresthesia was seen after EVLA in 0.7% of patients (6 studies). Phlebitis was seen in 2.6% of patients after RFA (2 studies), 27% after sclerotherapy (1 study), and 12% after the phlebectomy (1 study). Deep venous thrombosis and skin burn did not occur.
Conclusion
Treatment of AASV incompetence is safe and effective. Despite limited evidence, occlusion of the AASV can be achieved with endovenous thermal ablation and cyanoacrylate. There does not appear to be a benefit of EVLA compared to RFA regarding treatment efficacy. Phlebectomy shows promising results if the saphenofemoral junction is competent. Lower results are seen after sclerotherapy and CHIVA. However, studies with sufficient sample sizes of solely treatment of AASV incompetence are needed to draw firm conclusions.
Introduction
The treatment of varicose veins has been revolutionized in recent decades by the introduction of minimally invasive endovenous ablation techniques. Although varicose veins are frequently associated with great saphenous vein (GSV) incompetence, anterior accessory saphenous vein (AASV) reflux is responsible for approximately 10% of all varicose vein disease. 1 The AASV, present in 41% of people, lies anterior and lateral to the GSV, superficial to the deep venous system over the proximal anterior thigh, and also drains into the saphenofemoral junction (SFJ). The GSV and the AASV are visualized by Duplex-scanning through the “saphenous eye," however, the AASV lies more anterior and laterally and overlies the femoral vein and artery, the so-called “alignment sign.” 2
AASV incompetence possesses similar disease severity and morbidity to that caused by the incompetent GSV. 3 However, recently, a large epidemiology study showed a significantly higher incidence of superficial vein thrombosis in patients with isolated AASV reflux compared to patients with GSV incompetence. 4 This advocates that patients suffering from reflux in the AASV do have a meaningful problem and treatment is necessary. However, whereas many clinical studies report on the outcomes of treatment modalities for GSV insufficiency, valid data are still limited regarding the optimal therapy for AASV incompetence.
This systematic review and meta-analysis summarizes and compares the outcomes of the currently available treatment modalities for incompetent AASVs, such as endovenous thermal ablation (ETA) including endovenous laser ablation (EVLA) and radiofrequency ablation (RFA), cyanoacrylate closure (CAC), sclerotherapy, and surgical excision.
Methods
This report was written in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting systematic reviews and meta-analyses. 5
Literature search
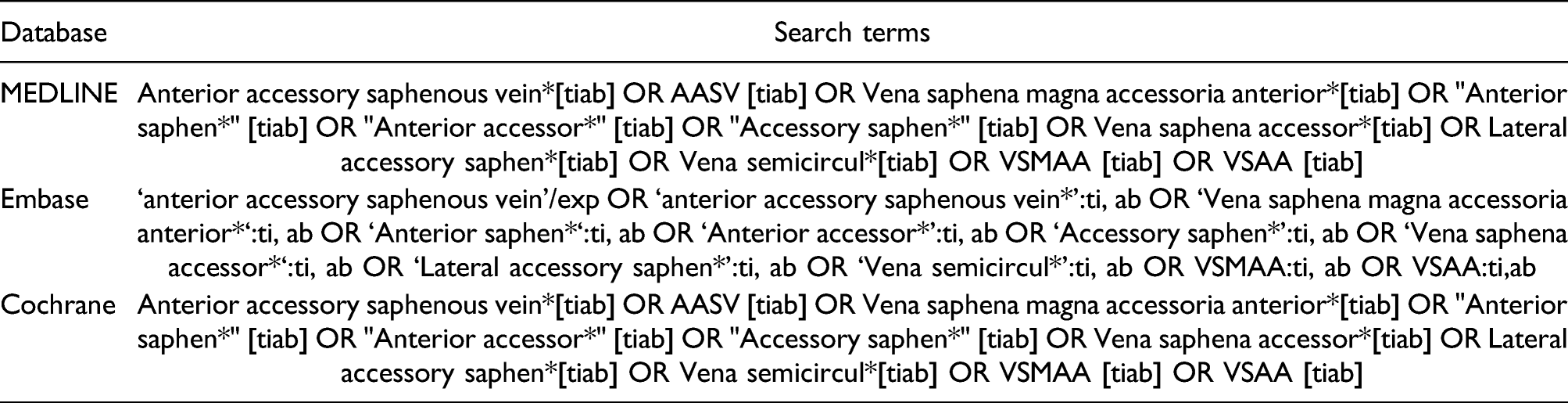
A systematic search was performed using the MEDLINE, Embase, and the Cochrane Library. The following keywords or abbreviations were used: anterior accessory saphenous vein, vena saphena magna accessoria anterior, vena saphena accessoria, lateral accessory saphenous vein, vena semicircularis. The final search was performed on November 30, 2020. The reference lists of retrieved articles and Google Scholar were used to identify studies that were not found in the original search. A full search strategy can be found in Appendix 1. Individual authors of the included articles were not contacted.
Inclusion and exclusion criteria
Studies: Studies were eligible if they had included patients treated for primary AASV incompetence, had been reported in English, and had the full text available. Exclusion criteria were case reports, commentaries, letters to the editor, surveys, and conference abstracts. Cohorts which not solely treated AASV incompetence were only included if the data for patients with AASV incompetence could be extracted. If more than one study reported the same patient cohort, only the most recent and complete study was included in this review.
Participants: Studies reporting the outcomes of patients who were treated for primary AASV incompetence were included.
Outcome measures: The primary outcome was anatomic success, defined as successful occlusion with no flow through the treated AASV. Terms such as closure, obliteration, ablation, reflux, recanalization, patent or open were also used. Failure rates were deducted from 100% to standardize the primary outcome. The secondary outcomes were pain during and after treatment, venous clinical severity score (VCSS), quality of life, patient satisfaction, esthetic result, time to return to daily activities, and complications (deep venous thrombosis [DVT], skin burn, paresthesia, phlebitis, and hyperpigmentation), which were only reviewed if data for AASV incompetence was extractable.
Data collection and extraction
After duplicates were removed, two authors (TA, EH) screened the titles and abstracts of the identified studies for relevance. Of the relevant studies, the two authors read the full text and made a final selection. Data extraction was performed by the two authors independently. When studies included patients with treatment of AASV and other truncal veins, only the data of patients with AASV were extracted.
Validity assessment
The methodologic quality of the articles was assessed using the Methodological Index for Non-Randomized Studies (MINORS) score, with a global ideal score of 16 for noncomparative studies and 24 for comparative studies. 6 The MINORS score was reported as a percentage of the global ideal score. For this review, a score of ≤8 was considered poor quality, 9–14 moderate quality, and ≥15 good quality for noncomparative studies. For comparative studies, a score of ≤15 was considered poor quality, 16–22 moderate quality, and ≥23 good quality. Discrepancy between the authors during the search, selection, and quality assessment were resolved by discussion. If necessary, a third author (ÇÜ) was consulted until agreement was reached.
Data analysis
OpenMetaAnalyst software (CEBM, Brown University, Providence, Rhode Island) was used for the meta-analysis. Meta-analysis was performed for the primary outcome of anatomic success. To provide a reliable outcome, only two or more studies of the same treatment modality were used for pooled analyses. Loss to follow-up was not included in the calculation of the anatomic success rates. The DerSimonian–Laird random-effects model was used for pooled data analysis. Results are presented as proportions with the 95% confidence intervals (CIs). Heterogeneity between studies was determined with forest plots and I2 indices. The secondary outcomes were calculated for each treatment modality.
Results
Study selection
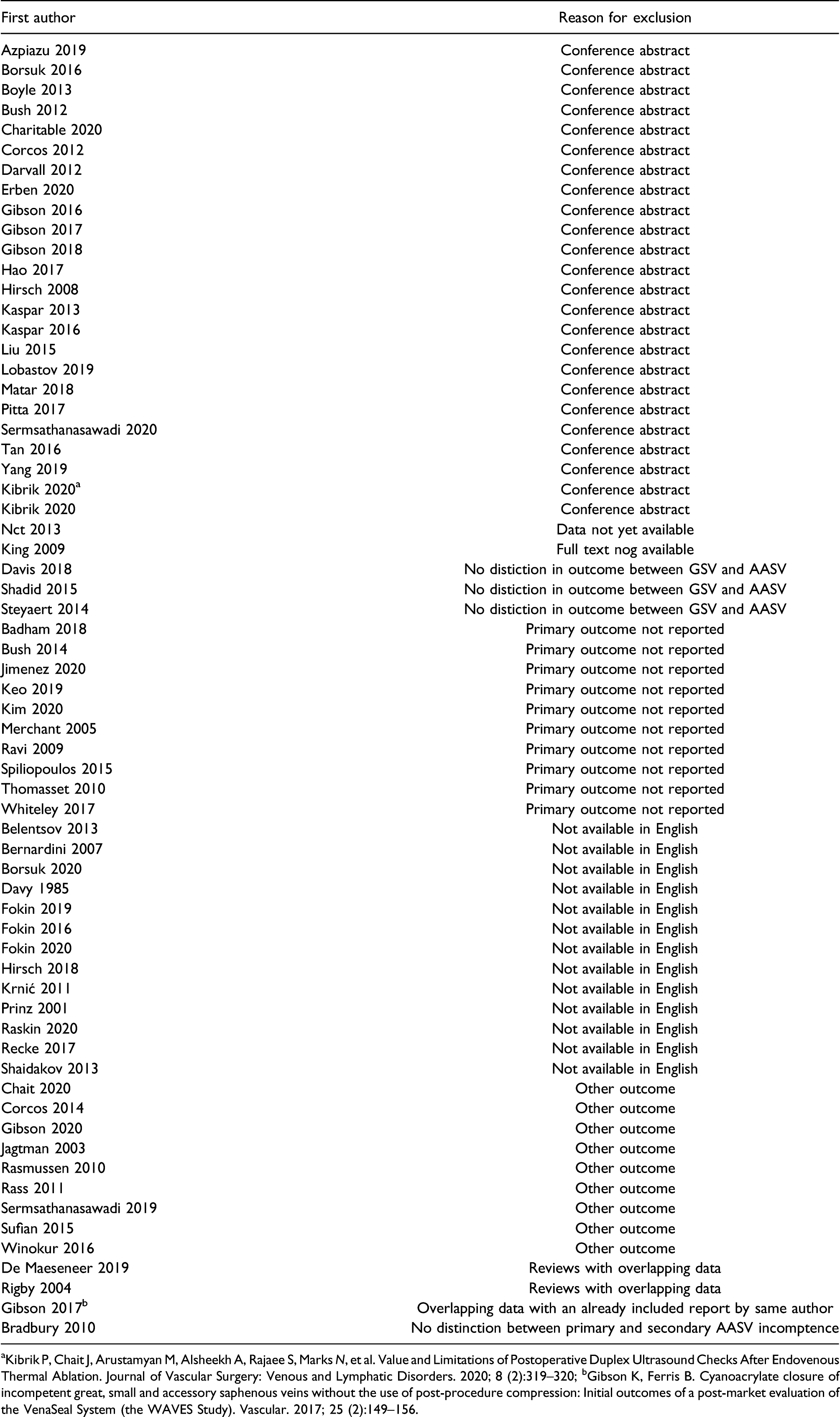
The search identified 861 studies. After duplicates had been removed and the titles and abstracts screened for relevance, 81 articles were eligible for the full-text review. The full-text reading and application of the inclusion and exclusion criteria resulted in the inclusion of 16 studies in the present systematic review. We excluded 65 studies for the following reasons (Appendix 2): reviews with overlapping data,7,8 primary outcome not reported,9–18 not written in English,19–31 conference abstracts,32–55 overlapping data with an already included report by same author,
56
data not yet available,
57
full text not available,
58
no distinction between primary and secondary AASV incompetence,
59
no distinction in outcome between GSV and AASV,60–62 and other outcome.63–71 A flow chart of the selection procedure is shown in Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for literature search to identify studies reporting on anterior accessory saphenous vein incompetence.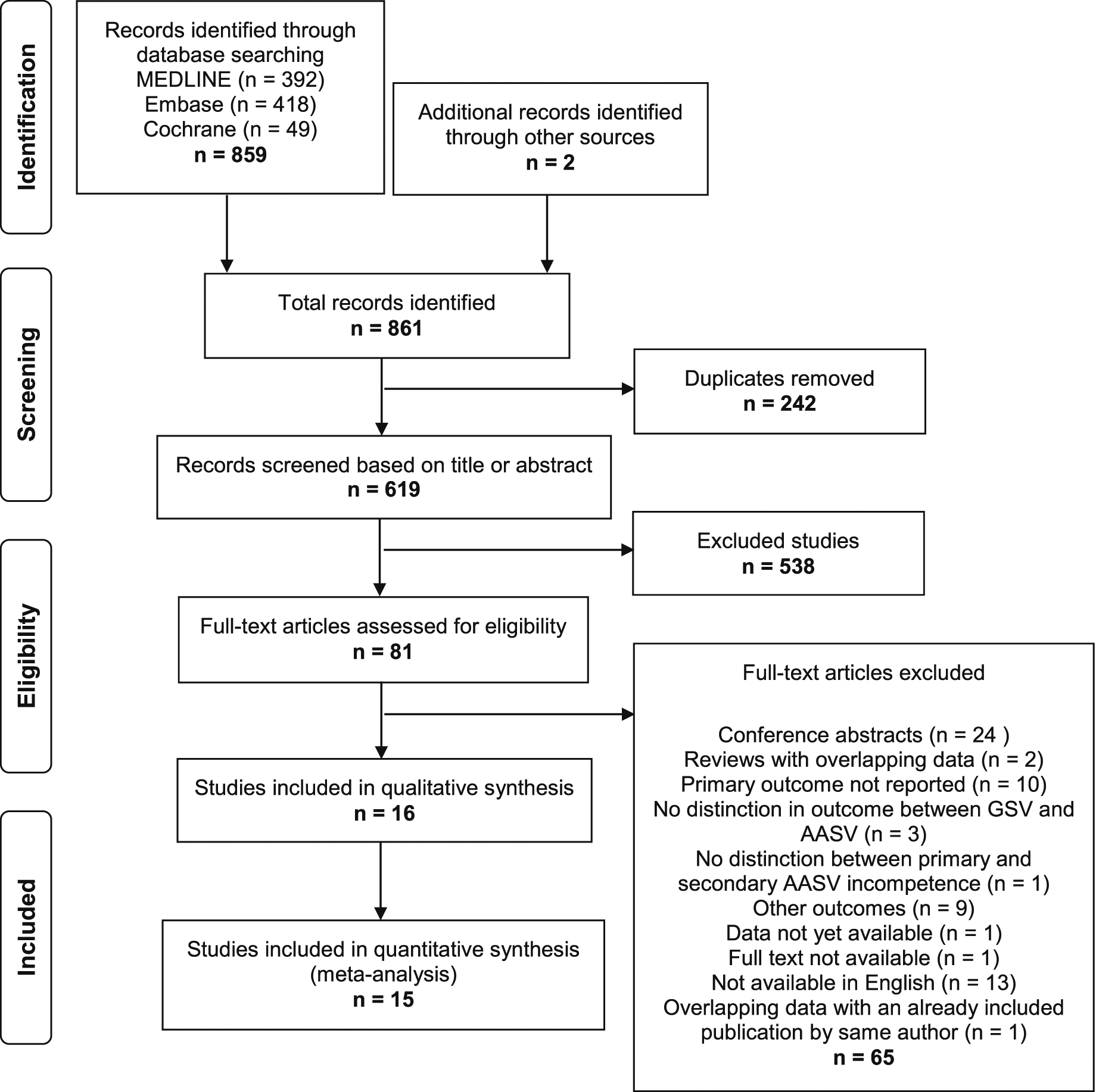
Validity assessment
Quality appraisal (MINORS score).
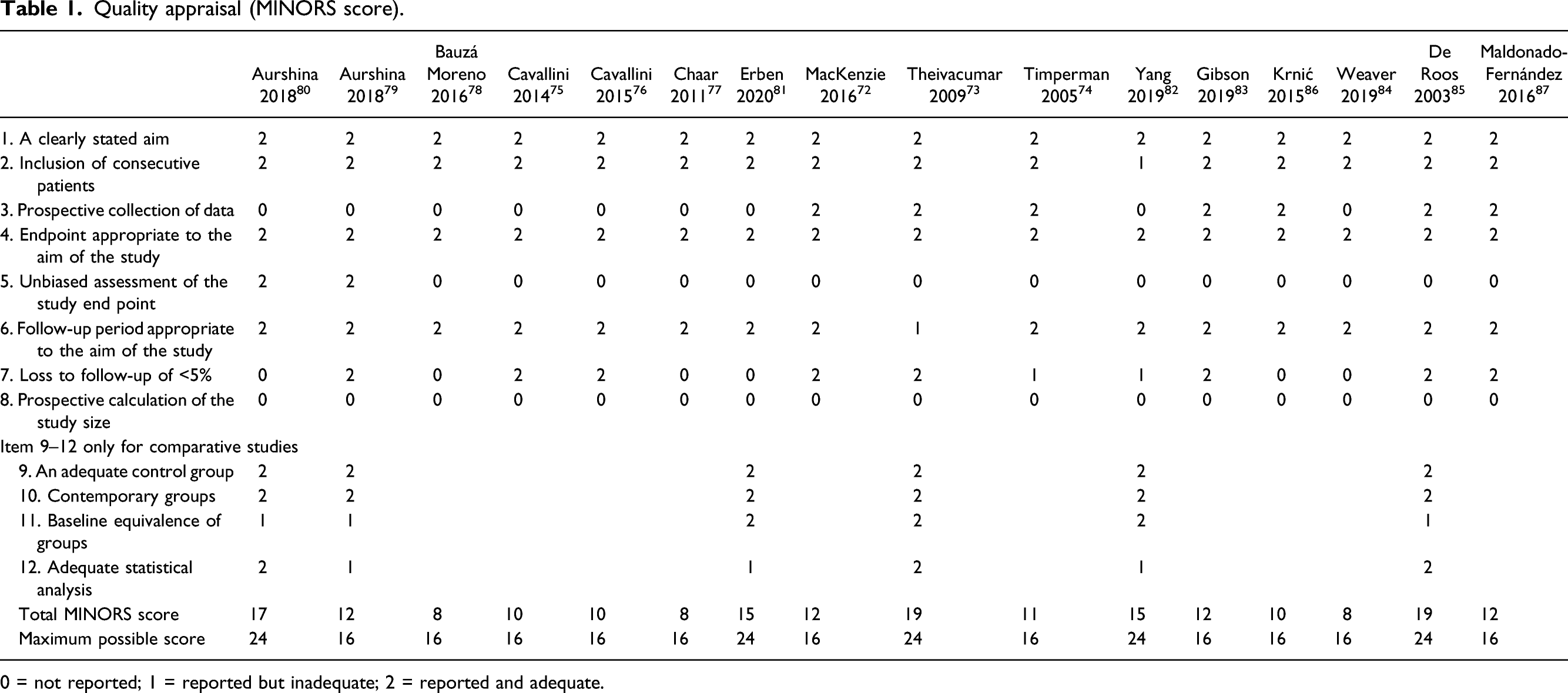
0 = not reported; 1 = reported but inadequate; 2 = reported and adequate.
Endovenous thermal ablation
Study characteristics and results—Endovenous thermal ablation.
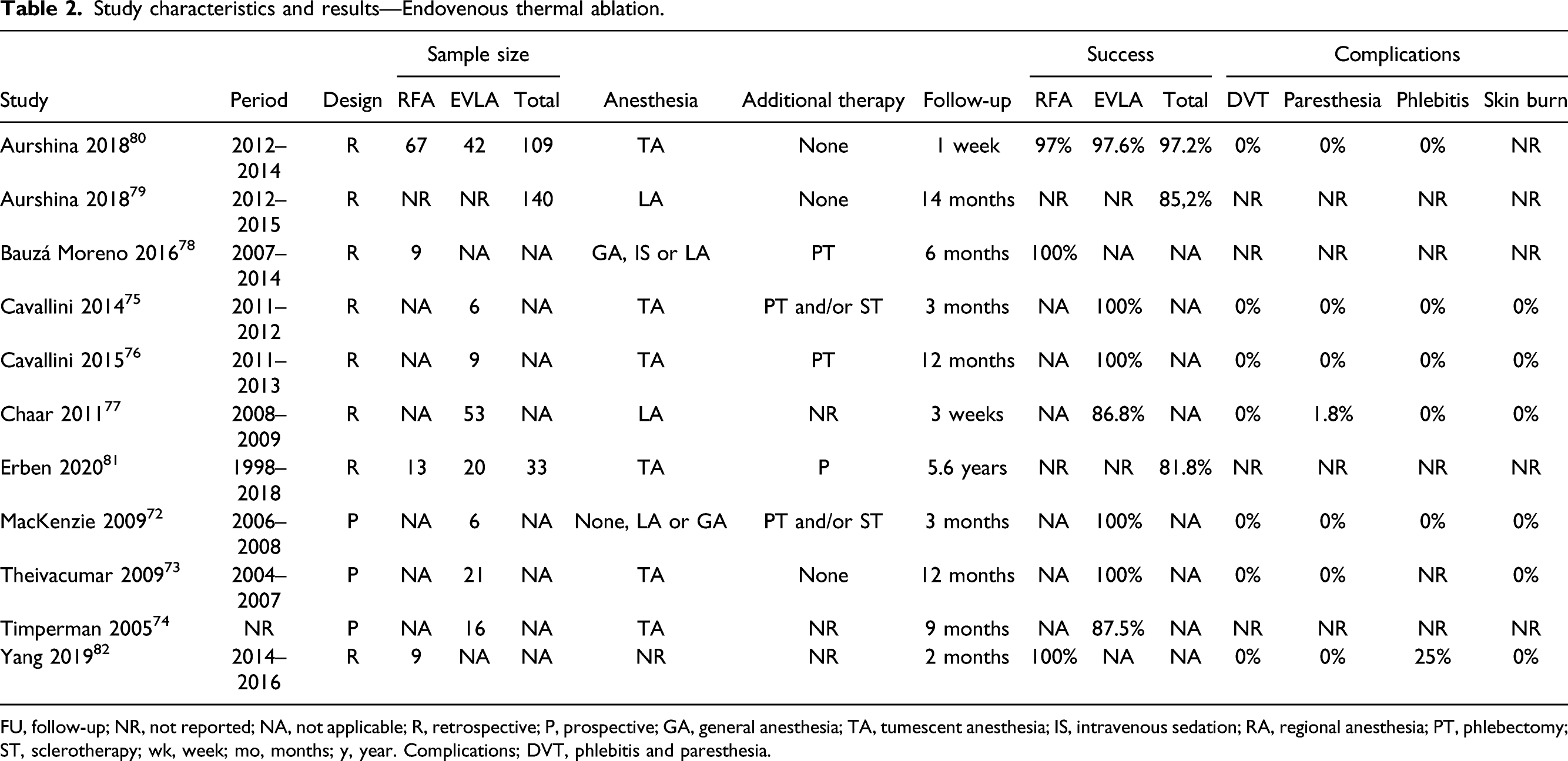
FU, follow-up; NR, not reported; NA, not applicable; R, retrospective; P, prospective; GA, general anesthesia; TA, tumescent anesthesia; IS, intravenous sedation; RA, regional anesthesia; PT, phlebectomy; ST, sclerotherapy; wk, week; mo, months; y, year. Complications; DVT, phlebitis and paresthesia.
Endovenous laser ablation: Eight studies described EVLA of 173 AASVs. 72,77,80,81 One study had included patients with solely AASV incompetence. 76 Three studies reported concomitant reflux of the SFJ.73,75,76 The CEAP clinical score was reported by two studies: 63% C2, 37% C3 76 and 85% C2, 12% C3, 3% C4, 0% C5/6. 73 Studies were heterogeneous regarding energy deliverance. Wavelengths differed between studies: 810 (n = 4),72–74,77 980 (n = 3),79–81 and 1540 nm (n = 2).75,76 Pulsed and continuous modes were both used, and there was no uniform amount of Joules per centimeter (range, 60–120 J/cm). Anatomic success of EVLA after a mean follow-up of 5.7 months ranged from 86.8 to 100%. One study reported a patient-satisfaction score of 84% calculated from a 10-cm visual analog scale and an improvement in Aberdeen Varicose Vein Symptom Severity Scores (AVVSS) of 64.6% (p= 0.001); median 4.1 (IQR: 2.1–5.2) at baseline vs 11.6 (IQR: 6.9–15.1) at 1 year. 73 The AVVSS in this group was similar to an age- and sex-matched control group with GSV incompetence. The VCSS, postprocedural pain, and time to return to daily activities were assessed by Cavallini et al. 76 The VCSS improved from a mean of 3.2 (SD: 1.42) before treatment to 0.13 (SD: 0.35) at day 30, became 0 at 3 months and kept at 0 at every subsequent follow-up. The mean postprocedural pain assessed on a 6-point scale ranging from no pain at all (0) to very painful (5) was 0.1 (SD: 0.4) at day 1, 1.3 (1.6) at day 10, and 0.6 (1.2) at day 30. Analgesics were used by 13% of patients. Patients returned to daily activities after a mean of 3.8 days (SD: 3.5). No DVT was seen in 137 patients and no phlebitis was seen in 116 patients.72,73,75–77,80 Postprocedural paresthesia was reported by six studies,72,73,75–77,80 of which one study reported paresthesia in 1.8% of patients. 76
Radiofrequency ablation: Four studies described radiofrequency ablation (RFA) of 98 AASVs.78,80–82 Yang et al. 82 compared CAC with RFA retrospectively. Three studies reported results of the ClosureFast device (Medtronic, San Jose, CA, USA/Covidien, San Jose, CA, USA/Medtronic, Minneapolis, MN, USA) and one study reported results of the Venefit Targeted Endovenous Therapy System (Medtronic of Canada Ltd, Vancouver, BC). In one study, the proximal segment of the vein was treated twice to ensure closure. 79 The anatomic success after a mean follow-up of 2.8 months ranged from 97 to 100%. No DVT and paresthesia were detected in 76 patients.80,82 Phlebitis occurred in 25% of patients reported by Yang et al. 82 Other secondary outcomes were not reported.
Non-thermal ablation
Study characteristics and results—Non-thermal ablation.
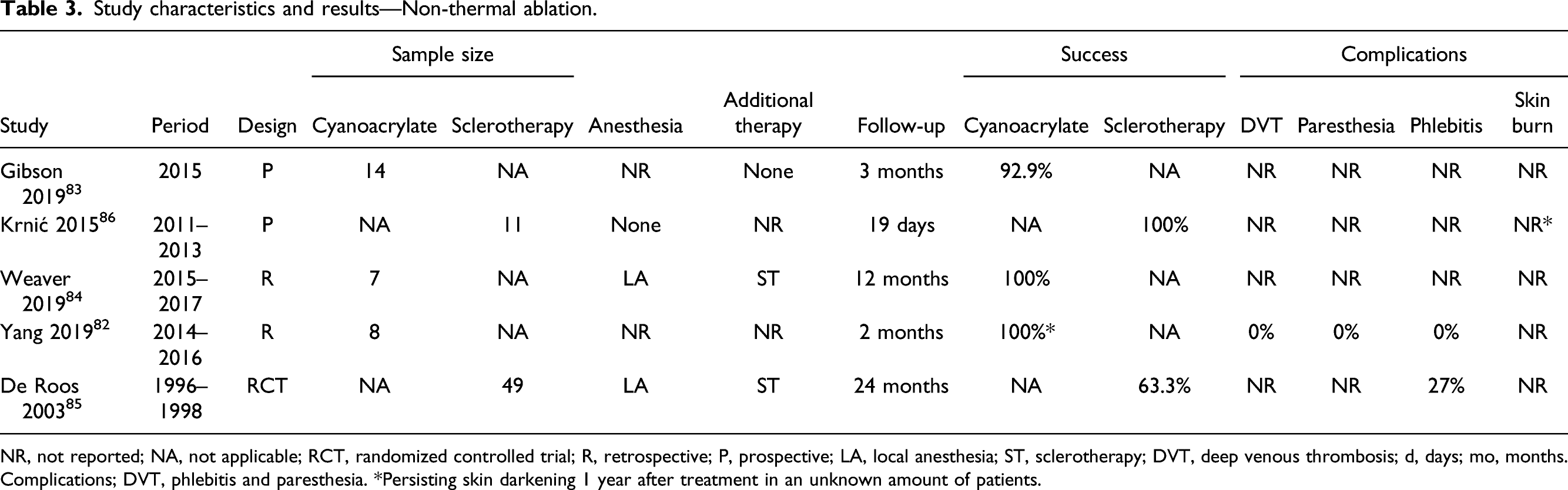
NR, not reported; NA, not applicable; RCT, randomized controlled trial; R, retrospective; P, prospective; LA, local anesthesia; ST, sclerotherapy; DVT, deep venous thrombosis; d, days; mo, months. Complications; DVT, phlebitis and paresthesia. *Persisting skin darkening 1 year after treatment in an unknown amount of patients.
Sclerotherapy: Two studies reported the results of sclerotherapy in 60 AASVs (Table 3).85,86 De Roos et al. 85 randomized between ambulatory phlebectomy and sclerotherapy using 3% Polidocanol. The mean Polidocanol dosage was 2.54 mL (range, 1–4 mL). The anatomic success rate after sclerotherapy was 63.3% after 24 months of follow-up. Retreatment with sclerotherapy was allowed 2 and 4 weeks after the initial treatment session. Krnić used a liquid Aethoxysklerol with air at 1:4 ratio and did not administer more than 18 mL of foam per session. If this amount could not solve the entire problem, the treatment was stopped and continued a week later. The anatomic success rate was 100% at 19 days of follow-up. None of the studies reported on DVT and paresthesia. Phlebitis was detected in 27% of patients by De Roos et al. 85 Persisting skin darkening 1 year after treatment was reported by Krnić et al. 86 The amount of patients was not reported. Other secondary outcomes were not reported by any of these studies.
Surgery
Study characteristics and results—Surgery.
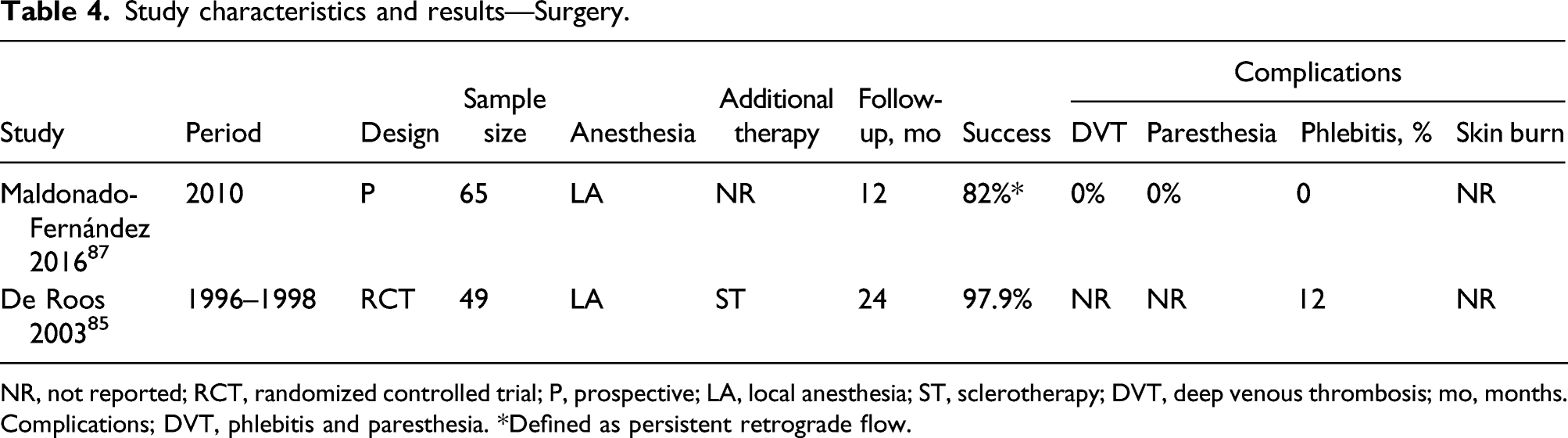
NR, not reported; RCT, randomized controlled trial; P, prospective; LA, local anesthesia; ST, sclerotherapy; DVT, deep venous thrombosis; mo, months. Complications; DVT, phlebitis and paresthesia. *Defined as persistent retrograde flow.
Phlebectomy
CHIVA: In the other study, the ambulatory conservative hemodynamic correction of venous insufficiency (CHIVA, Conservatrice Hemodynamique de l’Insuffisance Veineuse en Ambulatoire) was used to treat 65 AASVs. The baseline CEAP clinical classification was: 58% C2, 26% C3 and 15% C4–6. 87 Disconnection of the varicose veins from the AASV with extensive phlebectomy with multiple incisions was performed. The CHIVA-method is based on the theory that removal of the side-branches of the truncal veins will abolish the reflux in the truncal vein. The basic thought for this treatment is that development of varicose and refluxing side-branches of the truncal veins finally leads to truncal insufficiency. Postoperative low molecular weight heparin at prophylactic doses (bemiparin 2500–3500 units/day) was prescribed for 10 days. The anatomic success was 82% after 12 months of follow-up. At 12 months, the CEAP clinical score was improved (C1-3) in all patients. Fifty-seven percent of patients were asymptomatic, in 80% of patients no varicosities were visible, and aesthetics was good to excellent, all assessed by means of the Fligelstone scale. 88 DVT, phlebitis, and paresthesia did not occurred in this study. Results on skin burn and hyperpigmentation were not reported.
Pooled data
Data on the primary outcome, anatomic success, was pooled for ETA, CAC, and sclerotherapy (Figure 2). The pooled anatomic success rate was 91.8% (95% CI, 87.6–96.0%) after ETA, 93.6% (95% CI, 85.0–102.2%) after CAC, and 79.8% (95% CI, 47.9–111.7%) after sclerotherapy. The pooled data of CAC showed no heterogeneity (I2 = 0%), the pooled data of ETA were associated with moderate heterogeneity (I2 = 52%), and the pooled data for sclerotherapy showed substantial heterogeneity (I2 = 92%). Forest plots of pooled data on anatomic success (A) endovenous thermal ablation, (B) cyanoacrylate closure, and (C) sclerotherapy. CI = confidence interval. The solid squares denote the mean difference, the horizontal lines represent the 95% CI, the diamonds denote the weighted mean differences, and the tips indicate the 95% CI.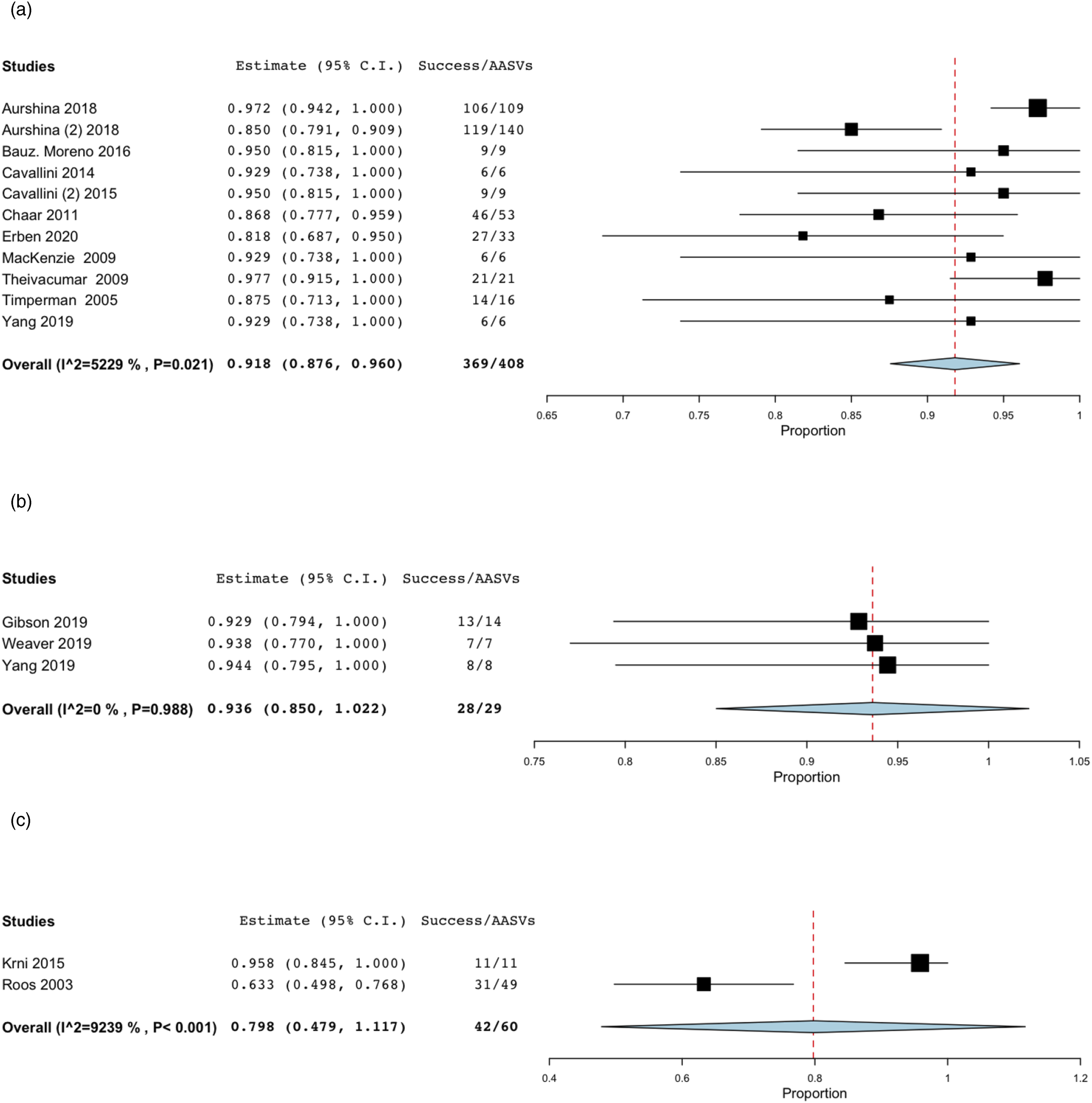
Discussion
The present systematic review and meta-analysis summarizes the currently available literature on the different treatment modalities of AASV insufficiency. The pooled anatomic success rates were 91.8% at a mean follow-up of 4.3 months, 93.6% at a mean follow-up of 5.7 months, and 79.8% at a mean follow-up of 12 months after ETA (RFA, EVLA), CAC, and sclerotherapy, respectively. The non-pooled anatomic success rate was 97.9% at 24 months after phlebectomy and 82% at 12 months after the CHIVA procedure.85,87
The available AASV data remains heterogeneous regarding the technical procedure. ETA shows a high pooled anatomic success rate, however, the mean follow-up was relative short. In the EVLA studies, three different laser wavelengths were used. Although previous studies have shown comparable anatomic success of different laser wavelengths, there may be differences in adverse effects.89,90 Furthermore, the position of the laser tip varied from 1 to 5 cm below the SFJ. It is known that a residual saphenofemoral stump can contribute to the formation of recanalization. 91 The high pooled anatomic success rate after CAC was derived from a small sample of 29 AASVs, nevertheless this non-thermal and tumescentless technique should be considered promising regarding its patient-friendly character. Regarding sclerotherapy different types of sclerosans were used in the included studies. This is of importance as previous studies showed that foam sclerotherapy is more effective than liquid sclerotherapy. 96 This was also noticed in the current review as there was a substantial difference in anatomic success of 63.3 vs 100% after liquid versus foam sclerotherapy, respectively. Although no crossectomy was performed during both procedures, the anatomic success rate after phlebectomy was higher compared with CHIVA. The high anatomic success rate after phlebectomy could be explained by the fact that there was no SFJ insufficiency and concomitant total or partial extraction of the AASV might have been performed. Another previous study reporting on CHIVA in patients with incompetence of the SFJ and reflux in the GSV, showed recurrence of GSV reflux in 53 of 58 patients after 3 years 92 Last, is the use of additional treatments may influence the anatomic success and contribute to the risk of side effects. No data on the innovative mechanochemical endovenous ablation (e.g., ClariVein and Flebogrif) of AASV is available. However, this relatively new technique shows fewer incidence of nerve injury, deep vein thrombosis, and skin burns compared to ETA in the treatment of GSV/SSV. 93
Secondary outcomes could not be analyzed because of the poor quality of the data. The VCSS, postprocedural pain, and time to return to daily activities after EVLA were assessed by Cavallini et al. 76 Symptoms and esthetic outcome were only assessed after CHIVA. 87 However, these outcome measures are of importance as EVLA of the small saphenous vein (SSV) showed a higher success rate, fewer complications, and earlier return to work compared with surgery but no significant differences in quality of life measures. 94
The risk of paresthesia may be an important limitation of ETA of AASV due to anatomy. In most cases, there is only a short proximal intrafascial segment and continuing treatment of the suprafascial segments gives a higher risk of skin nerve damage. However, paresthesia was detected in 0.7% of patients after EVLA.72,73,75–77,80 Which is lower than reported after EVLA of the GSV. 95 In this review skin burn was not seen, reported by three studies using EVLA.72,75,76 Hyperpigmentation was seen after foam sclerotherapy in an unknown amount of patients. 86 Phlebitis was seen in 2.6% of patients after RFA,80,82 27% after liquid sclerotherapy, 85 and 12% after phlebectomy. 85 It is known that sclerotherapy can lead to blood clot formation and inflammation which could be an explanation for the higher rate of “phlebitis” after sclerotherapy. 71 Phlebitis after phlebectomy can occur if some residual parts of the vein could not be extracted. No DVT was reported in any of the studies. A note of caution is due here since from some of the included studies we could not extract the complications rates specifically reported on AASV. This can result in an underestimation or overestimation of the true complications rates.
Due to the quality of the included studies, the ability to draw firm conclusions is limited. The small amount of studies per treatment modality and the small sample sizes in most of the studies can be considered the major drawback of this review. Moreover, two-thirds of the included studies failed to report on loss to follow-up, thereby inducing potential bias regarding the calculation of anatomic success rates during follow-up. Statistical power calculations were not performed in any of the prospective cohort studies and most of the studies were retrospective analyses. In addition, the pooled data included studies with different follow-up periods. Interpretation of this review might have been hampered by publication bias and selective reporting cannot be excluded.
Despite these limitations, the present systematic review provides a helpful overview of the available data on treatment options of primary AASV insufficiency collected from a number of independent studies. This saves time for clinicians because they would not need to perform their own research which could be a challenge since most treated AASVs have been included in GSV clinical trials.
Conclusion
Treatment of primary anterior accessory saphenous vein (AASV) incompetence is safe and effective. Despite limited evidence, occlusion of the AASV can be achieved with endovenous thermal ablation and cyanoacrylate. There does not appear to be a benefit of EVLA compared to RFA regarding treatment efficacy. Phlebectomy shows promising results if the saphenofemoral junction is competent. Lower results are seen after sclerotherapy and CHIVA. However, studies with sufficient sample sizes of solely treatment of AASV incompetence are needed to draw firm conclusions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
TA
Contributorship
Conception and design: TA, EH, MS, MCM, CJV, WW, ÇÜ.
Analysis and interpretation: TA, EH.
Data collection: TA, EH.
Writing the article: TA.
Critical revision of the article: TA, EH, MS, MCM, CJV, WW, ÇÜ.
Final approval of the article: TA, EH, MS, MCM, CJV, WW, ÇÜ.
Statistical analysis: TA.
Search strategy.
Excluded studies.
| Database | Search terms |
|---|---|
| MEDLINE | Anterior accessory saphenous vein*[tiab] OR AASV [tiab] OR Vena saphena magna accessoria anterior*[tiab] OR "Anterior saphen*" [tiab] OR "Anterior accessor*" [tiab] OR "Accessory saphen*" [tiab] OR Vena saphena accessor*[tiab] OR Lateral accessory saphen*[tiab] OR Vena semicircul*[tiab] OR VSMAA [tiab] OR VSAA [tiab] |
| Embase | ‘anterior accessory saphenous vein'/exp OR ‘anterior accessory saphenous vein*':ti, ab OR ‘Vena saphena magna accessoria anterior*‘:ti, ab OR ‘Anterior saphen*‘:ti, ab OR ‘Anterior accessor*’:ti, ab OR ‘Accessory saphen*’:ti, ab OR ‘Vena saphena accessor*‘:ti, ab OR ‘Lateral accessory saphen*’:ti, ab OR ‘Vena semicircul*’:ti, ab OR VSMAA:ti, ab OR VSAA:ti,ab |
| Cochrane | Anterior accessory saphenous vein*[tiab] OR AASV [tiab] OR Vena saphena magna accessoria anterior*[tiab] OR "Anterior saphen*" [tiab] OR "Anterior accessor*" [tiab] OR "Accessory saphen*" [tiab] OR Vena saphena accessor*[tiab] OR Lateral accessory saphen*[tiab] OR Vena semicircul*[tiab] OR VSMAA [tiab] OR VSAA [tiab] |
| First author | Reason for exclusion |
|---|---|
| Azpiazu 2019 | Conference abstract |
| Borsuk 2016 | Conference abstract |
| Boyle 2013 | Conference abstract |
| Bush 2012 | Conference abstract |
| Charitable 2020 | Conference abstract |
| Corcos 2012 | Conference abstract |
| Darvall 2012 | Conference abstract |
| Erben 2020 | Conference abstract |
| Gibson 2016 | Conference abstract |
| Gibson 2017 | Conference abstract |
| Gibson 2018 | Conference abstract |
| Hao 2017 | Conference abstract |
| Hirsch 2008 | Conference abstract |
| Kaspar 2013 | Conference abstract |
| Kaspar 2016 | Conference abstract |
| Liu 2015 | Conference abstract |
| Lobastov 2019 | Conference abstract |
| Matar 2018 | Conference abstract |
| Pitta 2017 | Conference abstract |
| Sermsathanasawadi 2020 | Conference abstract |
| Tan 2016 | Conference abstract |
| Yang 2019 | Conference abstract |
| Kibrik 2020a | Conference abstract |
| Kibrik 2020 | Conference abstract |
| Nct 2013 | Data not yet available |
| King 2009 | Full text nog available |
| Davis 2018 | No distiction in outcome between GSV and AASV |
| Shadid 2015 | No distiction in outcome between GSV and AASV |
| Steyaert 2014 | No distiction in outcome between GSV and AASV |
| Badham 2018 | Primary outcome not reported |
| Bush 2014 | Primary outcome not reported |
| Jimenez 2020 | Primary outcome not reported |
| Keo 2019 | Primary outcome not reported |
| Kim 2020 | Primary outcome not reported |
| Merchant 2005 | Primary outcome not reported |
| Ravi 2009 | Primary outcome not reported |
| Spiliopoulos 2015 | Primary outcome not reported |
| Thomasset 2010 | Primary outcome not reported |
| Whiteley 2017 | Primary outcome not reported |
| Belentsov 2013 | Not available in English |
| Bernardini 2007 | Not available in English |
| Borsuk 2020 | Not available in English |
| Davy 1985 | Not available in English |
| Fokin 2019 | Not available in English |
| Fokin 2016 | Not available in English |
| Fokin 2020 | Not available in English |
| Hirsch 2018 | Not available in English |
| Krnić 2011 | Not available in English |
| Prinz 2001 | Not available in English |
| Raskin 2020 | Not available in English |
| Recke 2017 | Not available in English |
| Shaidakov 2013 | Not available in English |
| Chait 2020 | Other outcome |
| Corcos 2014 | Other outcome |
| Gibson 2020 | Other outcome |
| Jagtman 2003 | Other outcome |
| Rasmussen 2010 | Other outcome |
| Rass 2011 | Other outcome |
| Sermsathanasawadi 2019 | Other outcome |
| Sufian 2015 | Other outcome |
| Winokur 2016 | Other outcome |
| De Maeseneer 2019 | Reviews with overlapping data |
| Rigby 2004 | Reviews with overlapping data |
| Gibson 2017b | Overlapping data with an already included report by same author |
| Bradbury 2010 | No distinction between primary and secondary AASV incomptence |
aKibrik P, Chait J, Arustamyan M, Alsheekh A, Rajaee S, Marks N, et al. Value and Limitations of Postoperative Duplex Ultrasound Checks After Endovenous Thermal Ablation. Journal of Vascular Surgery: Venous and Lymphatic Disorders. 2020; 8 (2):319–320; bGibson K, Ferris B. Cyanoacrylate closure of incompetent great, small and accessory saphenous veins without the use of post-procedure compression: Initial outcomes of a post-market evaluation of the VenaSeal System (the WAVES Study). Vascular. 2017; 25 (2):149–156.