
Abstract
Objectives
This study aims to investigate the impact of change in limb volume on the levels of functional mobility, health-related quality of life, social appearance anxiety, and depression before and after complex decongestive physiotherapy in patients with lower extremity lymphedema.
Method
Twenty-seven patients with unilateral lower extremity lymphedema were included. The treatment period was 20 sessions. The outcome measures were the limb volume, the Timed Up and Go test, the Short Form-36, the Social Appearance Anxiety Scale, and the Beck Depression Inventory.
Results
A statistically significant decrease in the limb volume (p < 0.001) and statistically significant improvements in the Timed Up and Go test performance (p < 0.001), the Short Form-36 Physical Component Summary score (p < 0.01), the Social Appearance Anxiety Scale score (p < 0.001), and the Beck Depression Inventory score (p < 0.001) were found. No statistically significant difference was found on the Short Form-36 Mental Component Summary score (p > 0.05).
Conclusion
The decrease in the limb volume improves the functional mobility, physical health-related quality of life, social appearance anxiety, and depression in patients with lower extremity lymphedema, but not the mental health-related quality of life.
Introduction
Lymphedema is a chronic progressive condition resulting from damage or dysfunction in the lymphatic system, and characterized by accumulation of protein-rich lymph fluid in the interstitial space. 1 Lymphedema can occur in any part of the body, 2 and is classified as primary and secondary lymphedema based on the underlying etiology. Primary lymphedema results from a congenital abnormality or dysfunction of the lymphatic system, whereas secondary lymphedema is caused by damage to the lymphatic system due to disease or iatrogenic causes.3,4
In lower extremity lymphedema, the main symptom reported by patients is swelling. 5 Physical complaints such as heaviness, tightness, and pain are also seen, 5 which can cause a decrease in functional mobility.6,7 In addition to these physical implications, the health-related quality of life and psychosocial deteriorations (e.g., social anxiety and depression) have been reported.8,9 Patients with lower extremity lymphedema expressed that swelling alters their body image; this raises concerns about their appearance, and depresses them. 10 A recent systematic review suggests that swelling has a negative relationship with health-related quality of life and psychosocial well-being in this patient population. 9
Based on these information and our clinical experience, edema status is seen the major causative factor in the above-mentioned impairments. Complex decongestive physiotherapy (CDP) is the most common treatment approach in the management of lymphedema. 4 The effect of CDP to reduce the limb volume in patients with lower extremity lymphedema is well documented,11–15 but evidence is lacking on the extent to which the reduction in limb volume can modify mobility, health-related quality of life, and psychosocial challenges.
The aim of this study was to investigate the impact of change in limb volume on the levels of functional mobility, health-related quality of life, social appearance anxiety, and depression before and after CDP in patients with lower extremity lymphedema.
Materials and methods
Study design and patients
This study was a prospective study conducted at a physical therapy clinic. Inclusion criteria were patients diagnosed with unilateral lower extremity lymphedema (primary or secondary) based on clinical examination and imaging techniques, over 18 years of age, and ability to understand written and oral information. Exclusion criteria were having a neurological disease, having a history of surgery in the spine or lower extremity that affects functionality, having a current spine or lower extremity injury, and having edema related to venous insufficiency based on clinical examination and imaging techniques.
According to the eligibility criteria, 30 patients were enrolled the study. The planned treatment period was 20 sessions. Patients who did not comply with the treatment plan were excluded in the analysis. Finally, 27 patients were included for statistical analysis.
The study was approved by the Noninvasive Research Ethics Board of Dokuz Eylül University School of Medicine (protocol no. 5686-GOA, decision no. 2020/26-59).
Interventions
The patients were treated with CDP that included patient education, skin care, manual lymph drainage, multilayer compression bandaging, and exercises. 4 Manual lymph drainage was started at the neck and then progressed to the abdomen, inguinal regions, and lymphedematous leg from proximal to distal. 16 The drainage was performed with a light pressure without causing redness or pain on the skin. The manual techniques were as follows: stationary circles at the neck and inguinal regions, parallel rotary technique and effleurage with breathing at the abdomen, and pump and pump-push techniques at the leg. 16 The techniques were repeated five to seven times. 16 A low pH skin lotion was applied on the leg and then bandaging was done. The fingers were wrapped in gauze and the leg was wrapped in a stockinette and a layer of cotton, respectively. Short stretch bandages (8, 10, 12, and/or 15 cm) were applied on the leg, with a highest tolerated compression by the patients and with gradually decreasing the compression from distal to proximal. Deep diaphragmatic breathing and muscle-pumping exercises were performed under guidance of a physical therapist to enhance lymphatic flow and improve mobility. 1 The patients were also instructed to perform these exercises at home.
The treatment period was 5 days a week for 4 weeks (20 sessions). A treatment session lasted 60 min on average. The patients were asked to wear the bandage for 24 h and to perform the exercises at home.
Outcome measures
All assessments were performed at baseline and after 20th session of the treatment.
Measurement of limb volume
First, circumference measurements of both legs were taken with a tape measure with the patients in supine position. The circumference was measured every 5 cm, beginning at the lateral malleolus to 60 cm proximal of the leg. Measurements were recorded in centimeters. The volume of each segment was then calculated by using the frustum formula (lateral malleolus–5 cm = V1, 5–10 cm = V2, …, 55–60 cm = V12). 17 The limb volume was obtained by summing the volume calculations of all segments (V1+V2+…+V12 = limb volume).
Severity of lymphedema was evaluated by comparing differences of affected and unaffected limb volumes, and classified as follows: > 5 to < 20%, minimal; 20–40%, moderate; and >40%, severe. 4
Measurement of the level of functional mobility
The Timed Up and Go (TUG) test was used to assess functional mobility of the patients. The patients were asked to sit on a standard chair and instructed that with a start command, they would stand up, walk a distance of 3 m at their own speed, turn, walk back, and sit down again. The patients were permitted to use their regular walking aid. No physical assistance was given. A stopwatch was used to measure the time elapsed. 18 The task was performed three times for each patient and a shorter time was selected for further analysis.
Measurement of the level of health-related quality of life
The Short Form-36 (SF-36) was used to assess health-related quality of life of the patients. The SF-36 is a general health-related quality of life measure and yields two composite scores, the Physical Component Summary (consisting of Physical Functioning, Role Physical, Bodily Pain, and General Health), and the Mental Component Summary (consisting of Vitality, Social Functioning, Role Emotional, and Mental Health). 19 The composite scores were calculated and interpreted according to the SF-36 user manual. 20 Higher scores indicate better health status. 19
Measurement of the level of social appearance anxiety
The level of anxiety of the patients was measured by the Social Appearance Anxiety Scale (SAAS). The SAAS is used to measure fear of being judged negatively based on social anxiety, body image dissatisfaction, and body dysmorphic disorder. The SAAS has 16 items rated on a five-point Likert-type scale ranging from 1 to 5. The total score ranges from 16 to 80 where a higher score indicates a stronger anxiety level. 21
Measurement of the level of depression
The level of depression was measured by the revised version of the Beck Depression Inventory (BDI). The BDI has 21 items, and each item is rated on a four-point scale ranging from 0 to 3. The total score ranges from 0 to 63, with a higher score indicating more severe depression. 22
Statistical analysis
Statistical analyses and graphics were performed using the R software (https://www.r-project.org). The Wilcoxon signed-rank test was used to compare outcomes between before and after the treatment. A p-value < 0.05 were considered statistically significant (*p-value < 0.05, **p-value < 0.01, and ***p-value < 0.001).
Sample size estimation
The sample size was calculated by using G*Power software (Heinrich-Heine University Dusseldorf, Germany). The sample size calculation was performed using the data of a previous study, which investigated whether CDP had an effect in limb volume and health-related quality of life. 12 In this study, the authors reported that the mean ± standard deviation values of the SF-36 Physical Functioning scores were 61.86 ± 15.05 and 66.39 ± 14.20 for before and after the treatment, respectively. 12 With α = 0.05 and a power of 80%, a minimum of 66 patients would be required.
Results
Demographic and clinical characteristics of the patients.
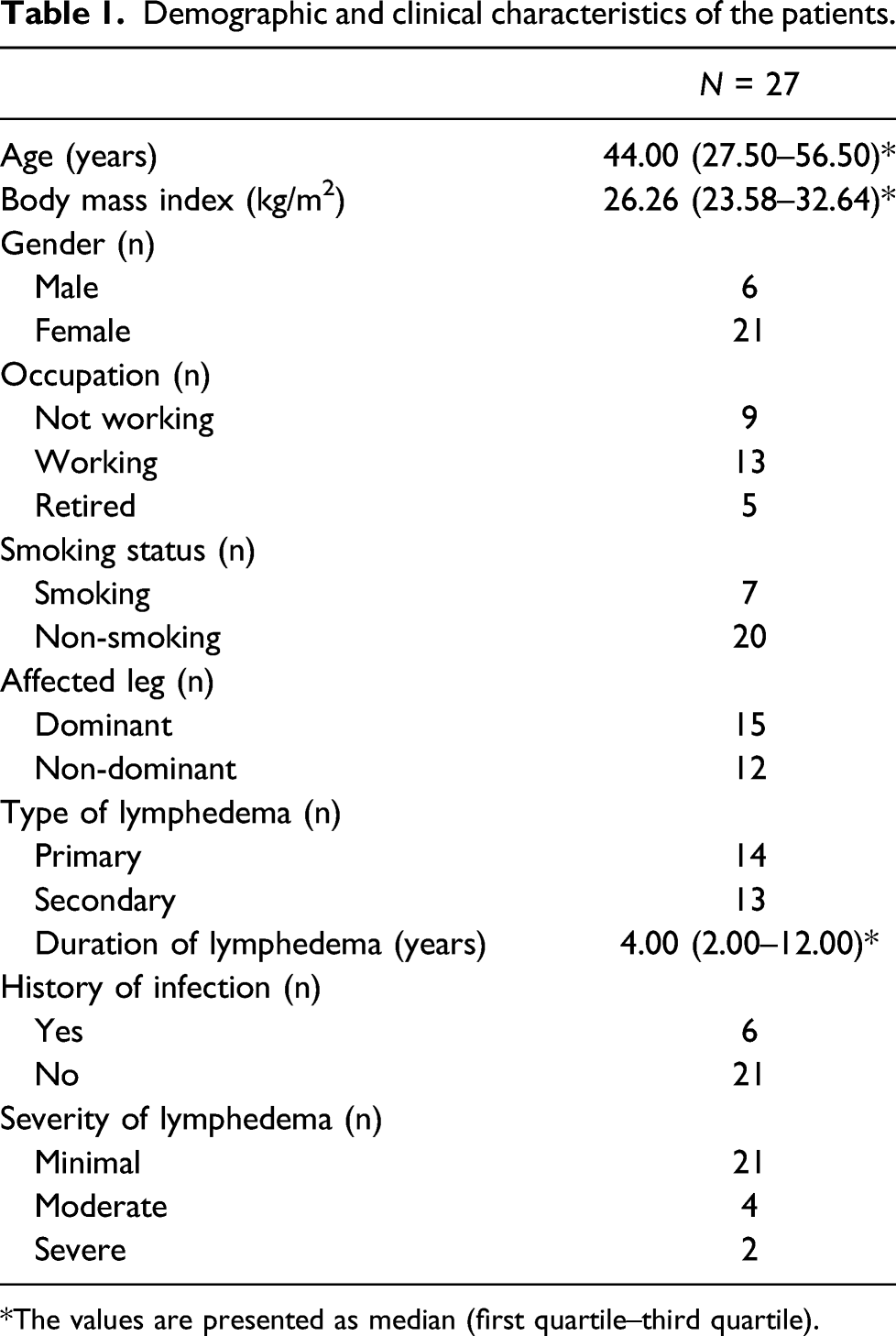
The values are presented as median (first quartile–third quartile).
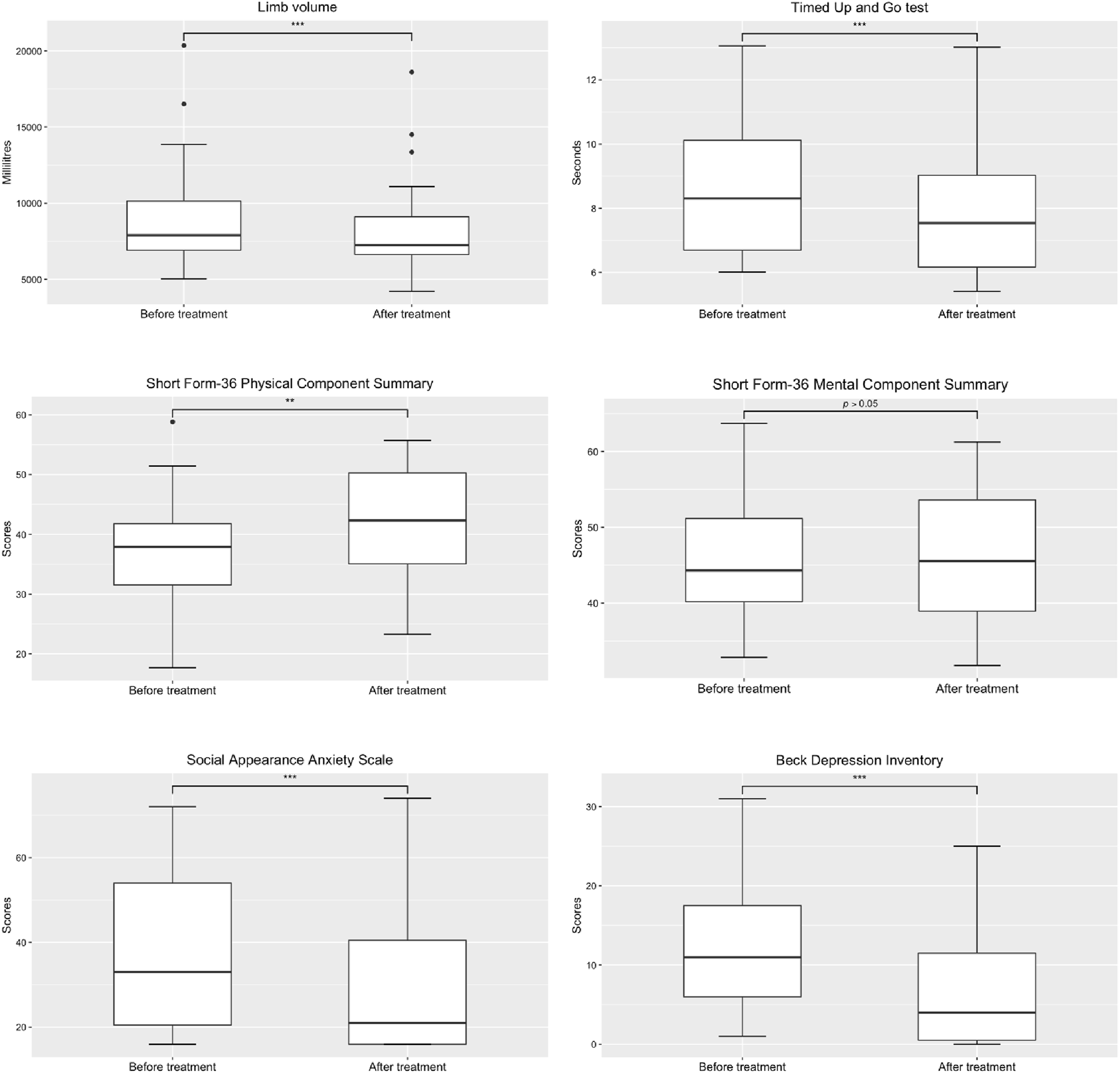
The comparisons of the outcome measures before and after the treatment (**p < 0.01, ***p < 0.001).
Discussion
The present study showed that the decrease in the limb volume improved the functional mobility, physical health-related quality of life, social appearance anxiety, and depression in patients with lower extremity lymphedema, but this decrease did not affect the mental health-related quality of life.
Functional mobility improved in our population. We think that the functionality of the patients increased due to a decrease in a heaviness of the limb as a result of the decrease in the limb volume. A previous study that studied patients with lymphatic filariasis found no significant effect of reducing limb volume on functional mobility. 23 Differences of studied populations among studies may explain this discrepancy. Filariasis is a complex disease due to its etiology and effects on many body systems. Muscle spasms, myositis, tendinitis, and joint stiffness in the lower extremity can be seen in patients with lymphatic filariasis because of the effects of the disease and drugs taken. 24 Therefore, only reducing limb volume by CDP may not be enough to improve functional mobility in patients with lymphatic filariasis; additional treatments such as stretching and strengthening exercises or mobilization techniques may be required for further functional improvement. This warrants further investigation.
The finding of this study in respect to the physical aspect of health-related quality of life is consistent with previous studies,12,14 but the present study offers a novel finding that the decrease in the limb volume does not affect the mental aspect of health-related quality of life in patients with lower extremity lymphedema. It can be said that in our population, physical limitations and disabilities (e.g., physical activities or bodily pain) of the patients improved by reducing the limb volume, but social and role disability due to emotional problems did not improve at 4-week follow-up. We suppose that the reason for this may be that the follow-up period was not long enough to improve the mental aspect of the patients. If the patients maintain their decreased limb volume (e.g., using a compression garment), it may be seen that the mental aspect of the patients may continue to improve at a longer follow-up period. However, it may be related with the chronicity of the disease. Negative emotions such as fear, loneliness, and/or worry can cause emotional disturbance in patients with lymphedema because of lymphedema as a lifelong condition. 8 Therefore, a treatment strategy based on a biopsychosocial model in addition to CDP may be useful to improve emotional wellness.25,26 Cognitive behavioral therapy can be added to the standard treatment for improvement of the mental aspect of health-related quality of life in this patient population; a multidisciplinary cooperation such as among physical therapists and psychologists may help. These assumptions should be examined in future studies.
Patients with lymphedema have concerns about their appearance in social settings. They think that swollen appearance of their limb may impact perceptions of their friends or partner. 8 In our clinical experience, most patients with lower extremity lymphedema state that they prefer dresses that hide their swollen limb. They also state that the swelling is noticed by people and questions are asked. 27 Thus, social well-being of patients is impacted and this situation contributes to the social isolation. 27 In our population, the level of social appearance anxiety of the patients decreased with reducing the limb volume. Although this is beyond the scope of the present study, the decrease in the limb volume may also reduce the social isolation in the patients.
Depression is a major psychosocial problem in patients with lymphedema.8,9 The present study showed that the decrease in the limb volume improved the depression score, but we think that the improvement on depression is not solely due to the decrease in the limb volume. Some patients with lymphedema think that clinicians provide inaccurate or minimal information about their disease, 8 and this may create uncertainty in patients and depresses them. In this study, the patients were informed about what lymphedema is, what factors affect their disease well and badly, and possible positive effects of the treatment. This information process may have eliminated uncertainty of the patients and thus may also have contributed to the improvement of depression. Furthermore, the decrease in the limb volume may have caused a domino effect. As the patients’ functional mobility and social appearance anxiety have improved, the level of depression of the patients may have decreased.
This study presents the data after Phase 1 treatment. Using a compression garment after Phase 1 treatment program—in Phase 2 treatment—is recommended to conserve the gains obtained in Phase 1. 4 Some patients either do not use the compression garment or use it sporadically; the edema status in these patients may change. Therefore, the findings in this study may not be generalized to patients in Phase 2 treatment program. Future research should assess the effect of the edema status in this patient population on the mentioned outcome measures in a long-term.
The main limitation of this study is that the planned sample size was not reached due to problems in recruiting participants and a small number of patients who meet eligibility criteria. So, we decided to present the data of the study with the current sample size. Nevertheless, our study fills the gap in the literature, knowledge about effects of the decrease in the limb volume on the functional mobility, the health-related quality of life, and the psychosocial impairments in patients with lower extremity lymphedema. The strength of this study includes the patients with primary and secondary lymphedema; this increases external validity of the results.
Conclusion
The reduction in the limb volume by CDP improves the functional mobility, the physical aspect of health-related quality of life, the level of social appearance anxiety, and the level of depression in patients with lower extremity lymphedema, but not the mental aspect of health-related quality of life.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Noninvasive Research Ethics Board of Dokuz Eylül University School of Medicine (protocol no. 5686-GOA, decision no. 2020/26-59).
Guarantor
EŞ
Contributorship
EŞ, GE, and DK researched the literature and conceived the study. EŞ and GE were involved in protocol development, patient recruitment, and data analysis. EŞ was the principal writer of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.