
Abstract
Objective
The present study aims to compare the changes of venous flow parameters of the lower limbs under the assessment based on the duplex ultrasound scanning in obese and non-obese individuals by complying with body mass index during laparoscopic cholecystectomy.
Methods
A prospective cohort study was conducted in non-obese (body mass index <25 kg/m2) and obese individuals (body mass index >30 kg/m2) during laparoscopic cholecystectomy to analyze venous hemodynamics of the lower limbs. The assessment was conducted on Femoral vein diameter, Femoral vein cross-sectional area, Femoral vein peak velocity, and Femoral vein volume flow. The change values (%) of venous flow parameters of the lower limbs were calculated as a percentage by: (intra-operative parameter-pre-operative parameter)/ pre-operative parametersX100%.
Results
45 right lower limbs were examined in 45 non-obese individuals and 33 right lower limbs in 33 obese individuals during laparoscopic cholecystectomy. The statistically significant difference was identified in the pre-operative and intra-operative values of Femoral vein diameter, Femoral vein cross-sectional area, Femoral vein peak velocity, as well as Femoral vein volume flow in both groups when these were analyzed independently (p = .00). When the change values of venous flow parameters of the lower limbs of the two groups were compared, more changes were identified significantly in the obese group, Femoral vein diameter (p = .042), Femoral vein cross-sectional area (p = .013), Femoral vein peak velocity (p = .002), and Femoral vein volume flow (p = .032).
Conclusion
The changes of lower limb venous flow parameters showed more significant difference in obese than in non-obese individuals during laparoscopic cholecystectomy. The mentioned findings may in part explain why obese patients undergoing laparoscopic cholecystectomy have a higher rate of post op deep venous thrombosis.
Introduction
As revealed from existing studies, obesity acts as a risk factor for chronic venous insufficiency (CVI) and venous thromboembolism (VTE).1–3 Central obesity causes increased intra-abdominal pressure (IAP) by abdominal fat. 4 The elevated IAP is postulated to be transmitted to the lower limbs via the femoral veins, leading to venous stasis and distensions of the veins of the lower limbs, which can further cause thrombosis and venous valve dysfunction. 5
In 1985, Erich Mühe successfully performed the initial laparoscopic cholecystectomy (LC). 6 LC refers to a safe and low-risk procedure, so it is considered a gold standard treatment for gallbladder disease. It exhibits numerous advantages (e.g., early mobilization, small wound, less postoperative pain, short hospital stay, and little bleeding). 7 However, it has been extensively reported that increased IAP attributed to pneumoperitoneum can affect cardiovascular, respiratory, and renal functions on account of the decrease in the venous flow return to the heart. 8 It was also reported that increased IAP attributed to pneumoperitoneum is associated with thromboembolic events during the post-operative period. 9
During LC, patients are in head-up position, and standard pressure pneumoperitoneum is maintained at 12–14 mmHg by CO2 insufflation. This high-pressure pneumoperitoneum and head-up position act as risk factors for venous stasis in the lower limbs. 10 Lower limb venous stasis is recognized as a major pathophysiological element involved in perioperative deep vein thrombosis (DVT) and postoperative pulmonary embolism (PE) development. 11
Color duplex ultrasound imaging contributes to a noninvasive and accurate flow assessment of the venous flow parameters of the lower limbs. The present study aimed to compare venous flow parameters changes of the lower limbs under the assessment by the duplex ultrasound scanning in obese and non-obese individuals by complying with body mass index (BMI) during the laparoscopic cholecystectomy (LC).
Materials and Methods
This study was conducted in the Department of Vascular Surgery, Jinan City People’s Hospital, Shandong Province, China, from 1 July 2017 to December 31st 2019. The experimental protocol and informed consent were approved by the institutional review board (Committee of Medical Ethics of the Jinan People’s Hospital Affiliated to Shandong First Medical University, No:2,019,017).To be specific, a total of 78 patients undergoing elective LC were enrolled.
All adult patients aged over 18 years of age and scheduled for elective LC were included. All patients provided the valid informed consents. Inclusion criteria were a body mass index (BMI) < 25 kg/m2 (Group A) or >30 kg/m2 (Group B). Exclusion criteria were individuals with clinical signs of chronic venous insufficiency, Doppler Ultrasound (DU) evidence of venous valve dysfunction or outflow obstruction, prior limb surgery or sclerotherapy, history and clinical signs of arterial disease, connective tissue disorders, leg trauma or swelling, clinical signs of lymphedema, history of chronic obstructive pulmonary disease, as well as cardiac failure. According to the protocol, participants should provide a medical history and undergo a clinical examination and DU imaging to exclude venous incompetence or thrombosis.
Venous hemodynamics of the right lower limbs were studied in 45 limbs of non-obese individuals (Group A) and in 33 limbs of obese individuals (Group B) having undergone the elective laparoscopic cholecystectomy (LC). BMI was determined to be patients’ weight (kg)/height (m2).
Surgery was performed by the identical operation and anesthesia team based on the standard LC technique with three ports. Carbon dioxide pneumoperitoneum was created with the closed technique by Veress needle and then maintained under 12 mmHg pressure. Anesthesia was standardized by employing the identical sedatives, narcotics, and muscle relaxants for all patients enrolled here throughout the surgery. All patients were administrated with a single dose of antibiotic before the surgery.
A recording was conducted for the pre-operative and intra-operative Femoral vein diameter (FVD), Femoral vein cross-sectional area (CSA), Femoral vein peak velocity (PV), as well as Femoral vein volume flow (VVF). The change values (%) of venous flow parameters were determined as a percentage by: (intra-operative parameter-pre-operative parameter)/ pre-operative parametersX100%.
The mentioned measurements were performed by experienced vascular physicians from the same team. They all learned the measurement standard before taking part in the measurement. These measurements were conducted on the right groin just at the bifurcation of femoral vein. A portable ultrasound system was used with a transducer with a 4–16 MHz frequency. The first measurement (pre-operative) was performed just after the induction of anesthesia before the creation of pneumoperitoneum. The second measurement (intra-operative) was conducted just before the surgery was completed with pneumoperitoneum maintained.
Statistical analysis
Data are expressed as mean ± standard deviations. Data were analyzed with the Mann Whitney U test for the intergroup comparison between obese and non-obese patients. In addition, all data were analyzed with SPSS software (SPSS Inc, Chicago, IL). A value of p ≤ .05 was significant.
Results
On the whole, 78 patients having undergone elective LC were enrolled in the study. They fell to two groups, that is, Group A (n = 45) that was non-obese individuals, as well as Group B (n = 33) that was obese individuals.
Patient characteristics and intra-operative variables of the two groups
Group A had a mean age of 43.18 ± 10.17 years, and that in group B was 41.08 ± 11.71 years. The number of males in group A and group B reached 18 and 10, respectively, and the number of females reached 27 and 23, respectively. No statistical significant difference regarding age and sex was identified between the two groups (P > .05).
Six patients in group A and five patients in group B had diabetes, while three patients in group A and four patients in group B had hypertension. Two groups were comparable based on these comorbidities (P > .05). The mean duration of surgery for group A was 60.16 ± 14.59 min, and that for group B was 63.32 ± 11.31 min (p = .124). For this reason, both groups were comparable by complying with the intra-operative variables.
Comparison of femoral vein parameters of the two groups
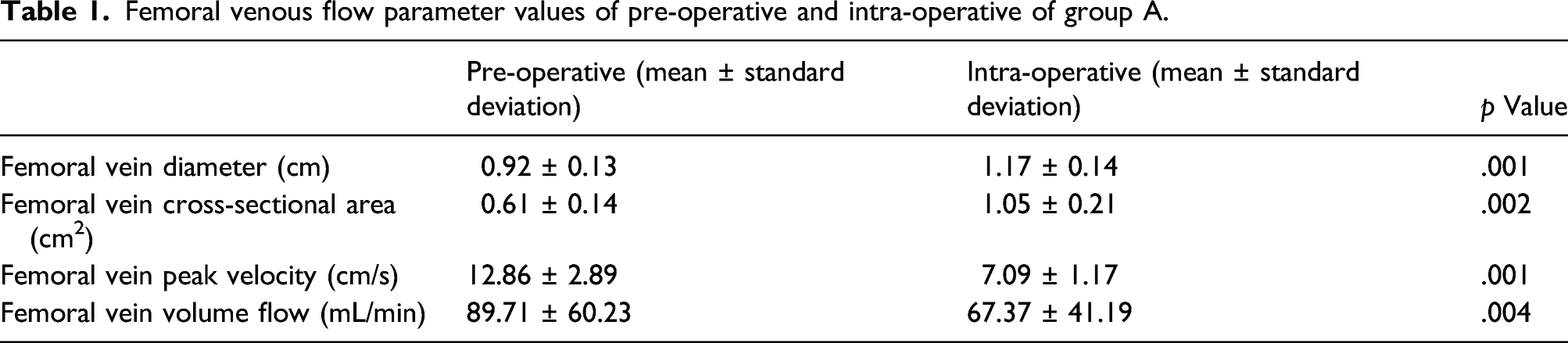
Femoral venous flow parameter values of pre-operative and intra-operative of group A.
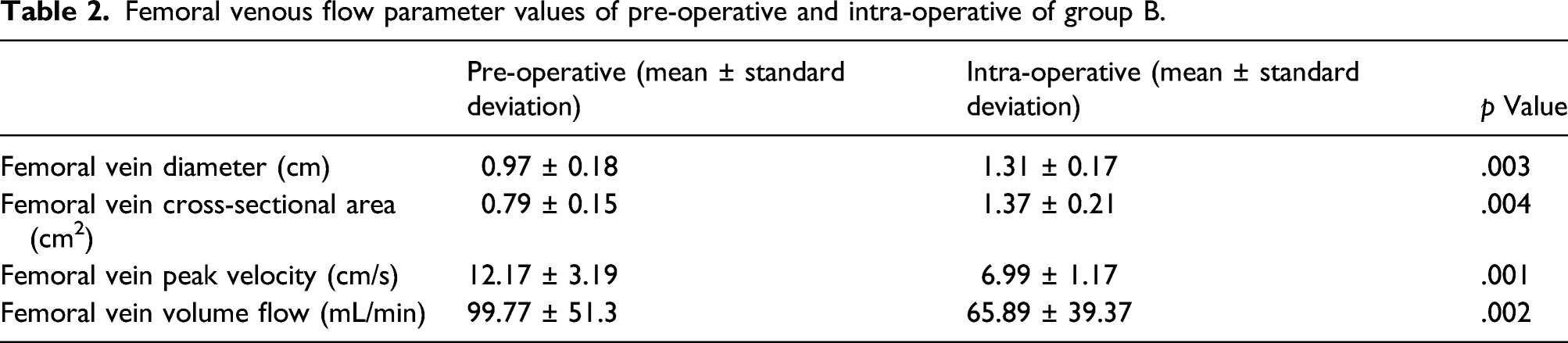
Femoral venous flow parameter values of pre-operative and intra-operative of group B.
Femoral venous flow parameter change values of pre-operative and intra-operative of group A and group B.

Discussion
A number of studies strongly evidenced that obesity affects venous flow parameters of lower limbs. Excess body weight is a risk factor for a first VTE event and recurrent VTE events. 12 Abdominal obesity elevates the IAP transmitted to the veins of the lower limbs. Accordingly, a greater tension is caused on the venous vessel wall, so the diameter increases. Increased stasis and reduced forward flow velocity might be a consequence. The mentioned findings can be explained by outflow obstruction attributed to elevated IAP that gives the credit to abdominal fat. The BMI was adopted for obese versus non-obese group definition since this marker of overweight and obesity is established and correlated significantly with total body fat content in adults. 4
VTE refers to one of the critical causes of morbidity and mortality after surgery. Open abdominal surgery causes transient hypercoagulable state during the postoperative period. It was extensively reported that conventional open cholecystectomy is followed by activation of coagulation mechanism.13,14 Bergqvist et al. reported 7–10% incidence of VTE diagnosed by using the venography in patients having undergone conventional open cholecystectomy. 15
As opposed to conventional open cholecystectomy, LC is a minimally invasive procedure for gallbladder disease. In comparison with open surgery, there is a minimal risk of deep venous thrombosis (DVT) during the perioperative period of LC on account of the early mobilization and the short hospital stay, whereas such a risk cannot be excluded completely. Kasuda S et al. describe the case of a 50-year-old patient with sudden death due to PTE at 24 h after laparoscopic cholecystectomy. The origin of the thrombi were bilateral deep vein thromboses in both the lower extremities. They believe that the accumulation of minor risk factors may have contributed to the onset of PTE. Hence, a more cautious assessment of the risk factors for PTE prior to surgery is required in such cases. 11 Pneumoperitoneum acts as a vital component in the laparoscopic surgery (e.g., LC). Pneumoperitoneum is capable of increasing the intra-abdominal pressure which contributes to venous stasis in the lower limbs. The head-up position during LC can further reduce the venous blood flow return from lower limbs to heart. The decrease in venous blood flow return to heart in head-up position in combination of raised intraperitoneal pressure was found over 40%. 18 Venous stasis attributed to pneumoperitoneum is a vital component of Virchow’s triad for thrombosis. Besides, general anesthesia affects the hemostatic state by affecting platelet function and bleeding time during LC.16,17 Moreover, carbon dioxide pneumoperitoneum may cause an increase in the blood viscosity, red cell aggregation, and decrease in red cell deformability, thereby increasing the possibility of thrombosis.
Numerous methods (e.g., color Doppler ultrasound, venography, photoplethysmography, or spiral computed tomographic angiography) are adopted to study the hemodynamics of veins of lower limbs. To identify the venous hemodynamics changes during LC, Güleç B et al. measured the cross-sectional area (CSA) and the peak flow rate (PFR) of femoral and saphenous veins in 60 patients having received LC by color Doppler ultrasound. 19 As revealed from their study, the CSA increased, and the PFR decreased in lower limbs veins during LC. The decrease in PFR is proportional to the increase in intra-abdominal pressure, which is of statistical significance. As revealed from another study by Jorgensen et al., a significant decrease was found in femoral vein blood flow velocity with a significant increase in the diameter of femoral vein during LC. 20 In the present study, intra-abdominal pressure was suggested to cause a significant increase in the FVD and the CSA and a decrease in the PV and the VVF of femoral vein in both groups during the LC. Besides, as indicated from the comparison between the change values of venous flow parameters of the lower limbs of the two group, the significantly more changes were reported in the obese group, FVD (p = .042), CSA (p = .013), PV (p = .002), and VVF (p = .032). The mentioned findings may in part explain why obese patients undergoing LC have a higher rate of post op deep venous thrombosis (DVT).
Accordingly, patients having received laparoscopic cholecystectomy, especially those who are obese, are recommended to undergo thrombosis prevention. Numerous methods have been recommended (e.g., using intermittent pneumatic compression, low molecular weight heparin injection and graduated elastic compression stockings).21,22 A graduated elastic compression stocking is capable of reducing venous stasis and increasing the flow in femoral veins; it can reduce the incidence of DVT of 10%. As proved from study conducted by Jorgensen et al., intermittent pneumatic compression (IPC) and intermittent elastic cuff stimulators (IECS) are capable of achieving pulsatile venous blood flow at insufflations of 12 mmHg during laparoscopic cholecystectomy. Furthermore, they concluded that high pressure pneumoperitoneum during the laparoscopic cholecystectomy could cause a significant stasis in the lower limbs. 20 Thus, low molecular weight heparin is recommended for DVT prevention in perioperative period during laparoscopic cholecystectomy in combination of graduated elastic compression stockings.
Conclusion
The findings of this study reveal that the changes of lower limb venous flow parameters show more significant difference in obese individuals than those in the non-obese individuals during LC. The mentioned findings may in part explain why obese patients undergoing LC have a higher rate of post op deep venous thrombosis (DVT).
Footnotes
Acknowledgments
The authors would like to thank Mr Changjiang Zhou for his advice and assistance with color duplex ultrasound examination.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The experimental protocol and informed consent were approved by the institutional review board (Committee of Medical Ethics of the Jinan People’s Hospital Affiliated to Shandong First Medical University, No:2,019,017).
Guarantor
Mingshu Lu, MD
Contributorship
Mingshu Lu researched data and outlined the article. Jingpeng Bi researched data for the article and wrote the manuscript. Yunhui Li and Zhiqiang Hao reviewed/edited the manuscript before submission.