
Abstract
Background
This study aimed to determine site-specific mechanical properties of the great saphenous vein (GSV) harvested from various sites in the same cadaver.
Methods
GSV samples were harvested from three sites: the thigh, knee, and lower leg. The thickness and diameter of the samples were measured, and the tensile test was performed to measure stiffness and Young’s modulus.
Results
The stiffness of the GSV harvested from knees in the longitudinal direction was lower than those from other sites, whereas the stiffness of the GSV harvested from the lower leg in the circumferential direction was lower than that from the thigh.
Conclusions
The GSV has site-specific mechanical properties. Thus, in addition to morphological evaluations such as echo and computed tomography in preoperative graft surgical evaluations, knowledge of the mechanical properties at each site can improve the patency rate and prevent aneurysmal expansion.
Introduction
The great saphenous vein (GSV) is the longest vein in the human body and is used as the principal conduit in autologous patch plasty, lower limb bypass, and coronary artery bypass graft (CABG). Compared with an arterial graft, a vein graft bypass results in a lower patency of <60% after 10 years for CABG. Furthermore, patch plasty is associated with the risk of the aneurysmal expansion and rupture of saphenous vein patches.1–4 To date, various strategies have been examined to improve patency and prevent aneurysm following a GSV graft.1, 4–6 In particular, vessel stiffness and Young’s modulus have been investigated as the factors associated with aneurysmal expansion and patency, as a mismatch between the bypass graft and host artery can affect the graft flow and patency.5, 7, 8 Many studies that examined the vessel stiffness and Young’s modulus of GSV used a part of the GSV harvested during CABG and varicose vein stripping. Although these studies relied on a portion of the GSV, the mechanical properties of the GSV at various sites of the same person have not been fully elucidated. Accordingly, understanding the variations in mechanical properties such as the stiffness and Young’s module throughout the entire length of the GSV can help identify the optimal site for harvesting GSV and thus improve the patency rate and prevent aneurysm following a GSV graft. To the best of our knowledge, no studies have investigated the mechanical properties of GSV at various sites in a single individual. In the present study, we aimed to compare the mechanical properties of the GSV at various sites in human cadavers.
Methods
Preparation and measurement of great saphenous vein parameters
This study included 10 formalin-fixed human cadavers from February 2019 to September 2019 (20 legs: 10 legs from five males and 10 legs from five females; median age: 83 [66–95] years) that were provided for education and research at Aichi Medical University, Japan and preserved for around 3–14 months until this study. This study’s experimental design was approved by the local ethics committee of Aichi Medical University (Permit Number: 2019–194). Cadavers were excluded if they had varicose veins, gross anomalies in the GSV, unilateral GSV, history of CABG, or leg surgery. Bilateral GSVs were exposed from the sapheno-femoral junction to the medial malleolus (Figure 1(a)). GSV samples were harvested from the following three sites: thigh (halfway between the great trochanter and lateral condyle), knee (around the joint space), and lower leg (halfway between the lateral condyle and lateral malleolus). Following the harvest, the samples were fixed and stored in formalin solution. Prior to the measurements, the samples were soaked in urea solution for 15 min to remove tissue formaldehyde, as previously described.
9
The thickness of the GSV wall was measured with a digital micrometer (Shinwa Rules Co., Ltd, Niigata, Japan), and the diameter of the GSV was measured with Vernier calipers (Shinwa Rules Co., Ltd). Briefly, three different points of each sample from each site (3 per site) were randomly selected. The average of the three measurements of the thickness and diameter of each sample was used as the representative value. (a) Medial aspects of a cadaver right leg with harvest sites for great saphenous vein samples (arrow head). Lower legs (1): Halfway between the lateral condyle and lateral malleolus, (b) Tensile test in the longitudinal direction. Vein with both sides clamped is loaded, (c) Tensile test in the circumferential direction. Vein with the pins of clamps both passing through the vein lumen is loaded to breaking force, (d) Typical load–displacement curves for the longitudinal and circumferential directions. Region 1: Non-linear curve because collagen fibers are not fully aligned. Region 2: The curve is nearly linear, and stiffness is defined as the maximum linear slope of the curve before failure force. Region 3: This represents the “yield” region. The addition of a load leads to the breaking point, (e) Typical stress-strain curve. This curve is derived from the load–displacement curve. Young’s modulus is defined as the maximum linear slope of the curve (Region 2').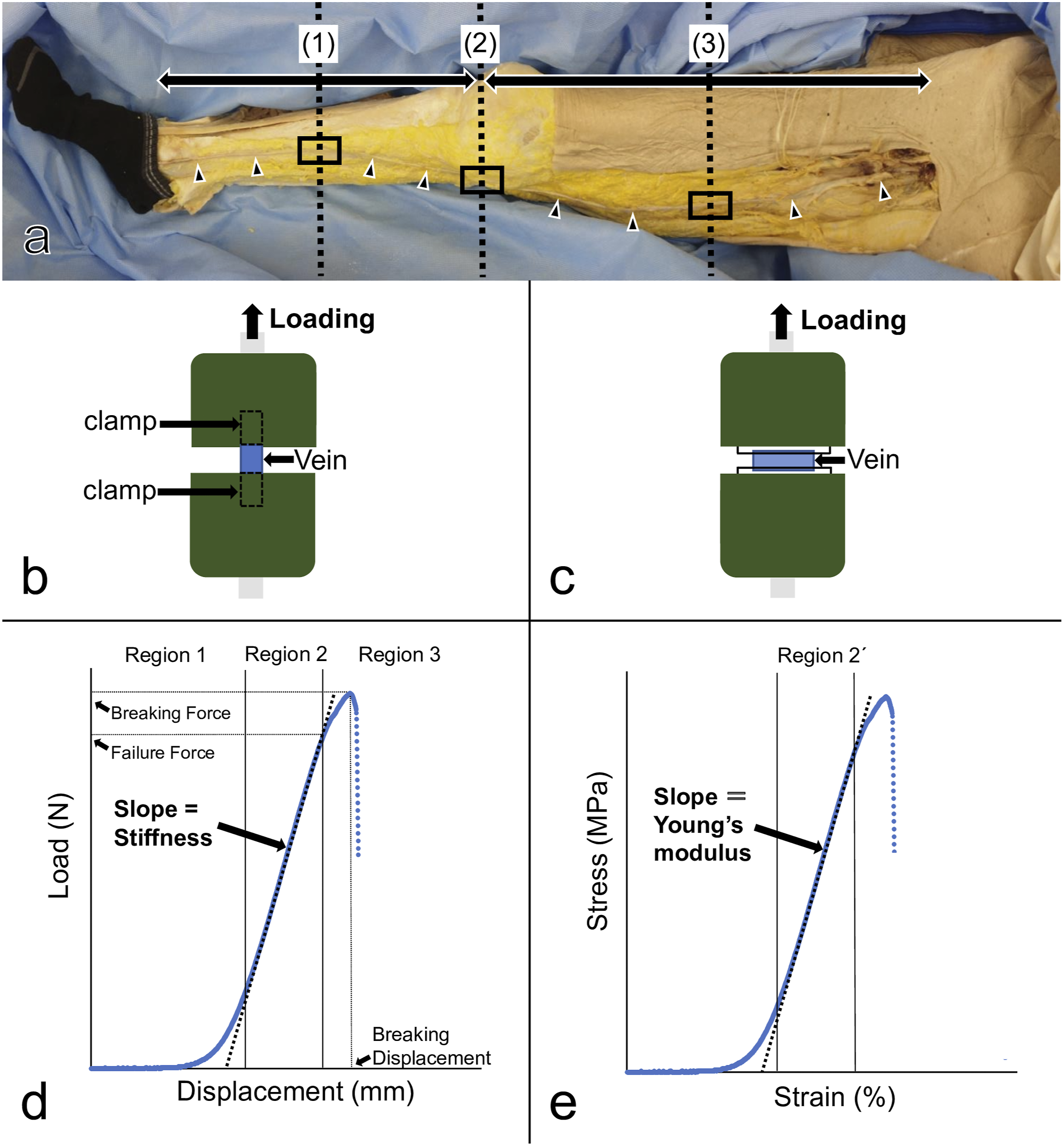
Tensile test and calculation of mechanical properties index
The tensile test was performed to examine the site-specific mechanical properties of the GSV samples. Based on a previously described method, 7 each sample was stretched both in the longitudinal and circumferential directions. Specifically, tensile test was performed using digital force gauges (ZTA-500N; Imada, Japan). Samples were prepared such that the total lengths would be 25 mm (clamp: 10 mm; stretch: 5 mm; Figure 1(b)) for the longitudinal stretch and 10 mm (Figure 1(c)) for the circumferential stretch. Samples were stretched until rupture with driving at 30 mm/min under room temperature (25°C). Load (N) and displacement (mm) during the tensile test were recorded using force-displacement graphing software (Force Recorder Professional, Imada, Japan). A typical load–displacement curve was divided into the three regions (Figure 1(d)). 10 The load–displacement curve started as non-linear (Region 1), became linear with loading (Region 2), reached to a failure force, returned to non-linear again (Region 3), and finally reached a breaking point. Stiffness was calculated from the slope of the linear region (Region 2). Stress (N/mm2) was calculated as load (N) divided by the cross-sectional area of the vein (mm2). Strain (%) was calculated as displacement (mm) divided by unloaded vein length (longitudinal: 5 mm; circumferential: vein diameter). A stress–strain curve was derived from the load–displacement curve, and Young’s modulus was calculated from the slope of the curve where the stress-strain curve is in a linear region (Region 2'; Figure 1(e)) according to Hooke’s law. The maximum point of the load (N) was defined as the breaking point, whereas the maximum load and displacement at the breaking point were defined as the breaking force (N) and breaking displacement (mm), respectively.
Statistical analysis
Statistical analysis was performed using SPSS (IBM SPSS Statistics 26, IBM, Armonk, NY, USA). Two-way repeated measures analysis of variance (ANOVA) was performed (regional difference × laterality, regional difference × anisotropy). When an interaction or main effect was observed, post hoc tests were subsequently performed using one-way ANOVA with Bonferroni correction (regional difference) and paired t-test (laterality or anisotropy). A p value <0.05 was considered statistically significant.
Results
Thickness, diameter
GSV harvested at the thigh (0.38 ± 0.07 mm) was significantly thicker compared with that at the knee (0.33 ± 0.07 mm) and lower leg (0.33 ± 0.06 mm) (p < 0.05) (Figure 2(a); Supplementary Table 1). Similarly, the diameter was greater in GSV harvested at the thigh (2.15 ± 0.66 mm) compared with that at the knee (1.78 ± 0.55 mm) and lower leg (1.54 ± 0.29 mm) (p < 0.05) (Figure 2(b)). No significant difference was found between the thickness or diameter of the GSV of the right and left legs for all sites. (a) Thickness and (b) diameter at each region. Values are expressed mean ± standard deviation (*p < 0.05).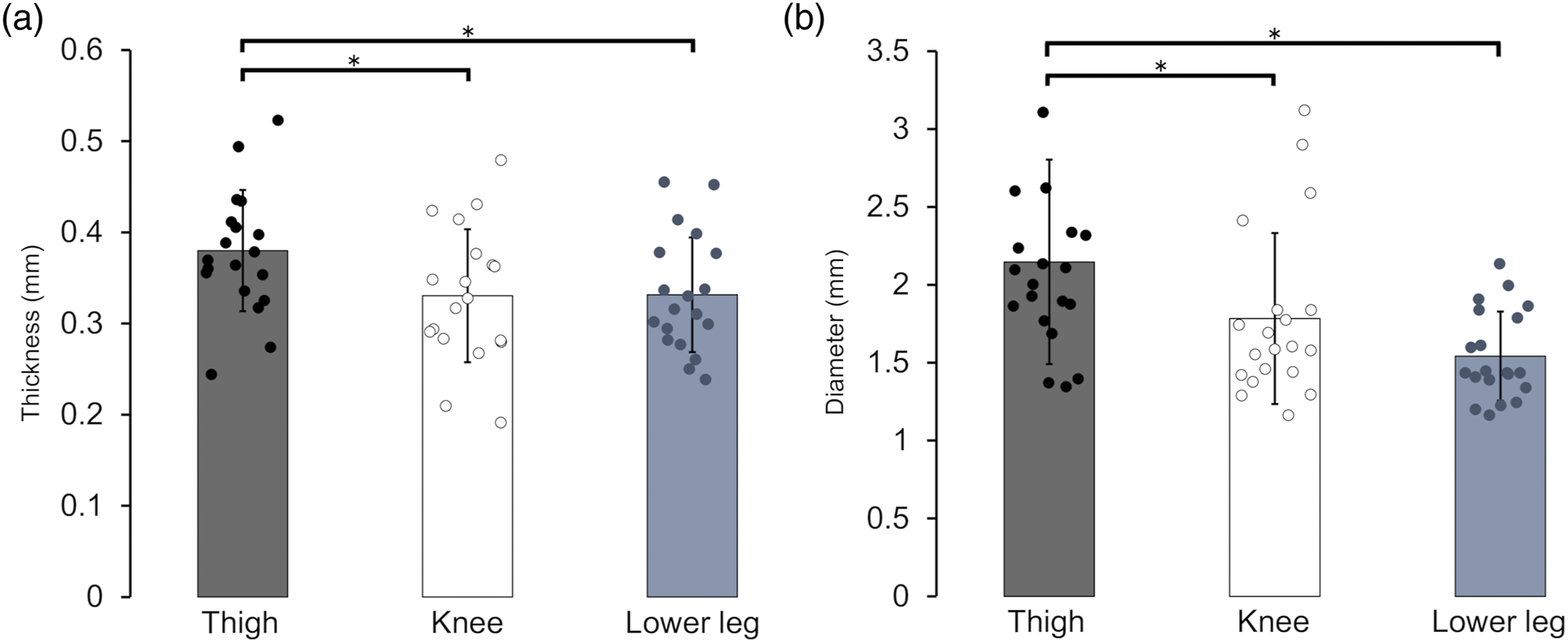
Stiffness
The stiffness of the GSV harvested at the knee and stretched in the longitudinal direction (17.17 ± 7.62 N/mm) was significantly lower than that at the thigh (22.32 ± 7.95 N/mm) and lower leg (24.43 ± 4.68 N/mm) (thighs vs. knees: p < 0.05; knees vs. lower legs: p < 0.01) (Figure 3(a); Supplementary Table 2). The stiffness of the GSV harvested at the thigh and stretched in the circumferential direction (5.88 ± 2.28 N/mm) was significantly higher than that at the lower leg (4.08 ± 1.67 N/mm; p < 0.05) (Figure 3(a)). No significant differences were observed between the right and left legs in any parameter; however, anisotropy was observed in all sites (p < 0.01). Results of the tensile test in the longitudinal and circumferential directions at each site. Values are expressed as mean ± standard deviation (▲: Longitudinal; ●: Circumferential; *p < 0.05; **,†p < 0.01). (a) Stiffness (N/mm), (b) Young’s modulus (MPa), (c) Breaking force (N), (d) Breaking displacement (mm)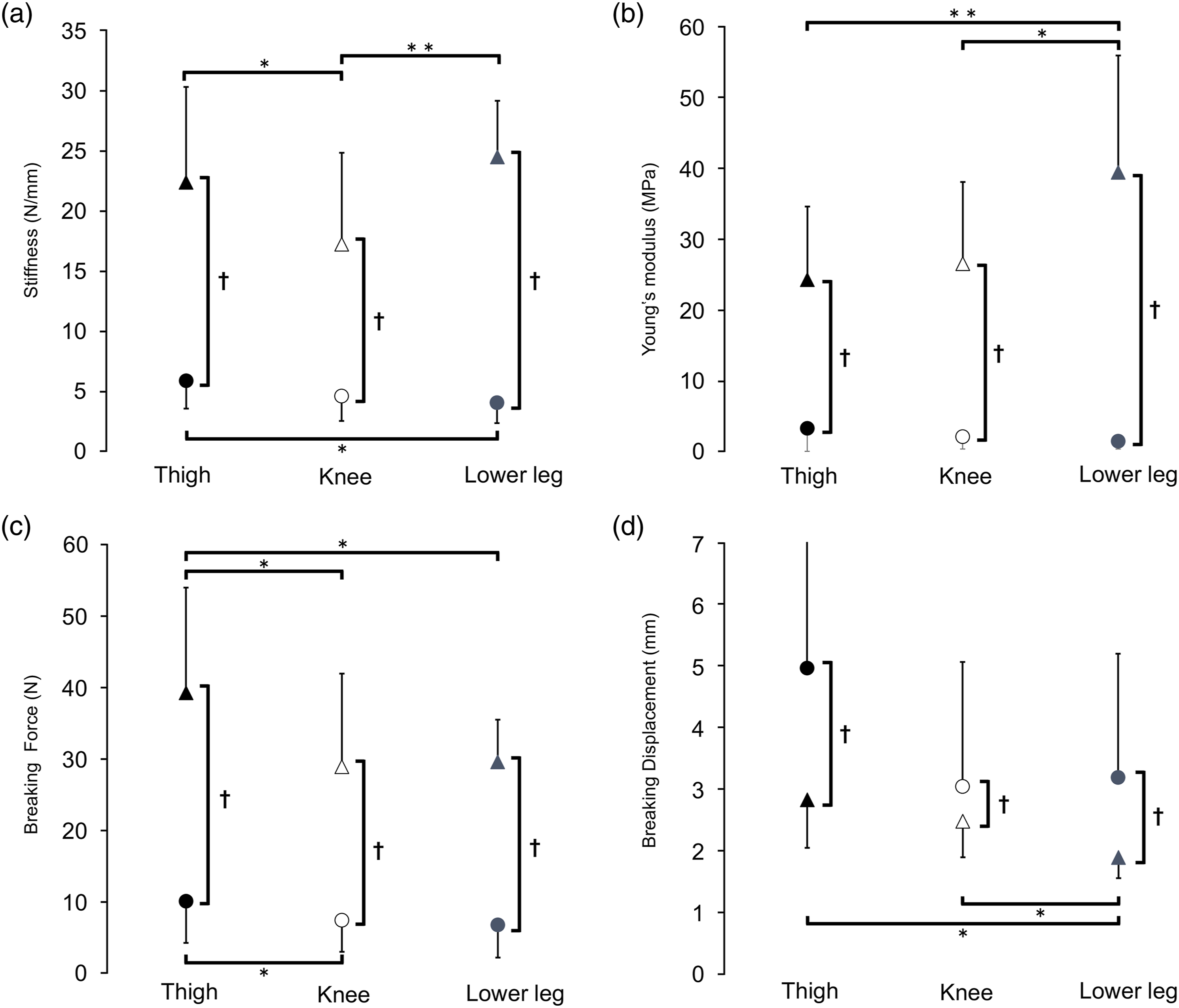
Young’s modulus
Young’s modulus of the GSV at the lower leg stretched in the longitudinal direction (38.99 ± 16.46 MPa) was significantly higher than that at the thigh (23.88 ± 10.30 MPa) and knee (26.13 ± 11.52 MPa) (thighs vs. lower legs: p < 0.01; knees vs. lower legs: p < 0.05) (Figure 3(b); Supplementary Table 2). No significant differences were observed between the right and left legs in any parameter, but anisotropy was observed in all sites (p < 0.01). No significant differences were observed among the thigh (3.67 ± 0.78 MPa), knee (2.51 ± 0.58 MPa), and lower leg (1.89 ± 0.33 MPa) (thighs vs. knees: p = 0.28; thighs vs. lower legs: p = 0.085; knees vs. lower legs: p = 0.41) (Figure 3(b)). No significant differences were found between the right and left legs in any parameter, but anisotropy was observed in all sites (p < 0.01).
Correlations between mechanical parameters
Stiffness in the longitudinal direction was positively correlated with thickness (r = 0.51; p < 0.01) (Figure 4(a)). In addition, stiffness in the circumferential direction, as measured through the tensile test, was positively correlated with diameter (r = 0.50; p < 0.01) (Figure 4(b)). The p values of the (a) thickness–stiffness and (b) diameter–stiffness relationships calculated using Pearson’s test for correlation (▲: Longitudinal; ○: Circumferential). Thickness and stiffness were correlated with longitudinal stretch, whereas diameter and stiffness were correlated with circumferential stretch.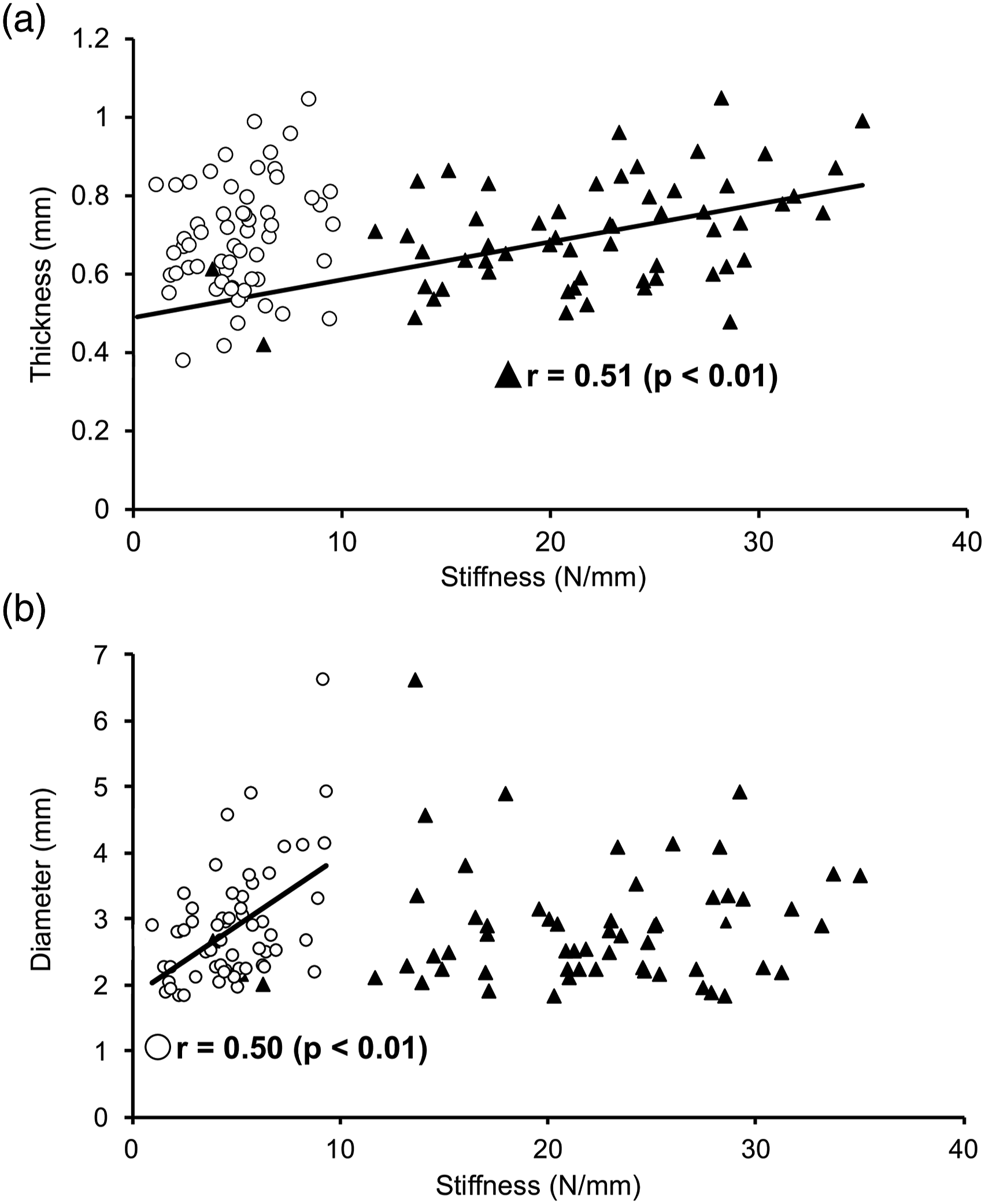
Breaking point
In the longitudinal stretch, the breaking force of the GSV at the thigh (39.20 ± 14.73 N) was significantly higher than that at the knee (28.84 ± 13.04 N) and lower leg (29.53 ± 5.91 N) (thighs vs. knees: p < 0.05; thighs vs. lower legs: p < 0.05) (Figure 3(c)). The breaking displacement of the GSV was significantly greater at the thigh (2.82 ± 0.77 mm) and knee (2.48 ± 0.58 mm) compared with that at the lower leg (1.89 ± 0.33 mm) (Figure 3(d)). In the circumferential stretch, the breaking force of the GSV at the thigh (9.75 ± 6.06 N) was significantly higher than that at the knee (7.00 ± 4.60 N) (p < 0.05; Figure 3(c)). No significant differences were observed in breaking displacement among the thigh (4.96 ± 2.91 mm), knee (3.04 ± 2.02 mm), and lower leg (3.19 ± 2.01 mm) (Figure 3(d)). Furthermore, no significant differences were found between the right and left legs in any parameter, but anisotropy was observed in all sites (p < 0.01).
Discussion
We demonstrated the site specificity of stiffness, Young’s modulus, breaking distance, and breaking force in the GSV harvested at the thigh, knee, and lower leg. No significant differences were observed in the parameters between the left and right legs. To the best of our knowledge, this is the first study that evaluated the stiffness and Young’s modulus of GSV harvested at the thigh, knee, and lower leg in human cadavers. No studies have examined the entire length of GSV; thus, the tensile test has not been applied previously to examine GSV at the thigh, knee, and lower leg in the same individual.
Donovan et al. 5 examined the stiffness of GSV below the knees and demonstrated that 1) stiffness in the circumferential direction was negatively correlated with age and 2) no correlations were found between longitudinal stiffness and site of origin. The authors collected GSV from the lower legs toward the direction of the knees during CABG; however, the site of GSV harvest was not consistent, and no indication of the site of harvest was found with respect to the joint. In contrast, we were able to harvest the entire length of the GSV to examine regional differences at the joint space level. Ukita et al. 11 suggested that increased bending of the knee causes more flexion of the popliteal artery. Moreover, they suggested that the hinge point or the maximum bending stress point when the knee bends affected arterial flexion and that this was due to cultural aspects (especially in the Japanese culture, where the sitting posture called “seiza” is commonly observed). We demonstrated that the stiffness of the GSV at the knee was lower compared with those at other sites. This could be attributed to the fact that GSV stretches and contracts repeatedly in the longitudinal direction during exercise engaging the knee joints, as it runs from the medial side of the lower leg, into the thigh, and through the medial side of the knee joint. Our findings also suggest that a lower Young’s modulus and thickness of GSV at the knee could also contribute to a lower stiffness of GSV at that knee.
Collectively, our findings suggest the importance of knowing the site-specific properties of the graft when performing an autologous vein bypass. Since a mismatch in the stiffness between the graft and host artery are considered an important factor in determining patency, Hamedani et al. 7 demonstrated that the stiffness of the GSV was higher than that of umbilical veins, suggesting that a greater blood flow would be achieved by using stiffer veins for CABG. In our study, the stiffness of the GSV stretched in the circumferential direction was significantly higher at the thigh compared with that at the lower leg and was positively correlated with its diameter. On the other hand, Buxton et al. 12 reported that a greater GSV diameter is a significant risk factor contributing to obstruction in CABG and that a diameter of 2.5–3.4 mm had the best patency rate. These findings indicate that the GSV graft needs to be close to the host artery, which has an optimal stiffness range, to obtain a better graft patency.
A few studies have examined the association of Young’s modulus with CABG or a lower limb bypass patency rate. George et al. 10 collected a portion of the vein used for brachial arteriovenous fistula surgery to perform the tensile test in the circumferential direction and demonstrated that the 30 -day occlusion rate was highly correlated with the Young’s modulus. This suggests that the Young’s modulus of the GSV affects the patency rate of the graft. We demonstrated site-dependent differences in the Young’s modulus of the GSV in the longitudinal direction. Chang et al. 13 reported that the patency rates of GSV harvested at the thigh and lower leg and used in CABG showed no significant difference. As no regional difference was found in the patency rate in past studies, this difference in Young’s modulus in the longitudinal direction may not significantly affect the patency rate. Furthermore, in our study, no significant differences were observed in the Young’s modulus values obtained in the circumferential direction. Stooker et al. 14 also reported no significant difference in the compliance of human GSV harvested at the thigh and lower leg. Furthermore, no site specificity of Young’s modulus was observed in the circumferential direction, suggesting that the site specificity of the stiffness of GSV in the circumferential direction may be affected by the GSV diameter when harvested in CABG. On the other hand, Andel et al. 15 demonstrated that the compliance calculated from Young’s modulus in the circumferential direction of the internal thoracic artery approximated that of the coronary artery used in CABG, suggesting that a mismatch in compliance with the host artery is a risk for obstruction. Measuring the Young’s modulus of GSV before and during an operation is difficult; thus, a better patency rate is needed to harvest GSV, considering that the diameter of the GSV affects its stiffness.
How stiffness or Young’s modulus affects the aneurysmal expansion of saphenous vein patches remains unclear. Donovan et al. 5 evaluated the stiffness of GSV in the circumferential direction using GSV harvested from the knee to the lower leg and demonstrated that postoperative aneurysm and rupture may be prevented using a graft with high stiffness. They also demonstrated that the stiffness of GSV is negatively associated with age, hypertension, and diabetes, suggesting that it may be a risk factor of aneurysmal expansion. Archie et al. 2 examined the association between the diameter and pressure load of GSV and demonstrated that veins with a smaller diameter had a higher risk of aneurysmal expansion and rupture. Indeed, a previous study demonstrated that patch rupture occurs in 0.5–4% of all cases. 1 Since most of these studies used ankle veins, some suggest the use of GSV above the knee. Berner et al. 16 also reported that GSV harvested below the knee had a higher risk of rupture. We demonstrated that stiffness in the circumferential direction was associated with the diameter of GSV, and that the stiffness of GSV at the thigh was higher than that at the knee and lower leg. These findings suggest that stiffness affects the risk of aneurysmal expansion and rupture. As no differences were observed between the right and left legs, the risk of aneurysm is likely equivalent between the two sides. Collectively, these findings suggest that GSV harvested at the thigh with high breaking force and stiffness may be optimal in preventing postoperative aneurysmal expansion and rupture following patch plasty. Given the risk of aneurysmal expansion, GSV harvested at the knee may not be suitable, considering the stiffness and breaking force of the knee GSV in the circumferential direction do not differ significantly from those of the lower legs.
This study has several limitations, given the use of cadavers. First, formalin fixation may have influenced the stiffness of the GSV. Rouleau et al. 17 compared the vascular thickness and Young’s modulus of vessels in vivo and before and after fixation using a canine aortic arch and demonstrated that while the vessel diameter did not change, crosslinking due to formalin fixation affected Young’s modulus. As urea is known to decompose formalin, 9 we soaked our samples in urea prior to performing the tensile test. Future studies are needed to determine the effects of formalin fixation and the use of urea on mechanical properties of GSV. Second, the general condition of the subjects in our study is different from those in previous studies. Many studies collected a portion of the veins at the time of CABG harvest in subjects in their 50s and 60s. Of note, Donovan et al. 5 reported age-related changes in venous wall thickness and compliance. Subjects in our study were older, with an average age of 82 years, and had no history of CABG. Thus, the characteristics of GSV in our study may be different from those in previous studies. Third, the detailed medical histories of the subjects were unknown because the identity of the cadavers could not be confirmed. Varicose veins, hypertension, and diabetes have been reported to affect stiffness. 5, 18 Although we excluded subjects with varicose veins based on visual inspection, some of the subjects possibly had regurgitation of GSV which may be examined on ultrasound. As we had no information on comorbidities such as hypertension and diabetes, these factors may have impacted our results. Further studies on the mechanism by which diabetes, hypertension, and varicose veins affect the stiffness of veins fixed in formalin are needed.
Our study evaluated site-specific mechanical properties of GSV and demonstrated that the longitudinal stiffness was low at the knee, whereas Young’s modulus was high at the lower leg. In addition to preoperative ultrasound or computed tomography-based morphological evaluations of grafts, our findings suggest the importance of characterizing the mechanical properties of each harvest site and harvesting from the optimal site to improve the patency rate of an autogenous vein bypass and prevent the aneurysmal expansion of saphenous vein patches.
Supplemental Material
Supplemental Material - Site-specific mechanical properties of the human great saphenous vein: Cadaveric comparisons among the thigh, knee, and lower leg harvest sites
Supplemental Material for Site-specific mechanical properties of the human great saphenous vein: Cadaveric comparisons among the thigh, knee, and lower leg harvest sites by Takahiro Arima, Shun Otsuka, Hiroki Mitsuoka, Munekazu Naito, Takashi Nakano and Hiroyuki Ishibashi in Phlebology
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Aichi Medical University as competitive research funding.
Ethical approval
The ethics committee of Aichi Medical University approved this study (Permit Number: 2019–194).
Guarantor
TA
Contributorship
TA, SO, HM, and HI were involved in study design. TA, SO, and MN were involved in data analysis. TA, MN, SO, HM, TN, and HI wrote the article. All authors reviewed and edited the article and approved the final version of the article.
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.