
Abstract
Objectives
The objective is to investigate the interaction of sclero-embolic and contrast agents with the polymerisation of medical grade n-butyl-cyanoacrylates.
Methods
An in vitro spectrophotometric absorbance method was developed to detect changes in light transmission to measure n-BCA polymerisation. The initiation and the rate-of-polymerisation of mixtures of n-BCA with sclero-embolic and contrast agents were investigated.
Results
Initiation of polymerisation: VENABLOCK™ and HISTOACRYL® were the fastest agents to polymerise, while VENASEAL™ was the slowest. Rate of polymerisation: Hypertonic saline inhibited the polymerisation of all n-BCAs, while hypertonic glucose prolonged the polymerisation rate. ETHANOL and detergent sclerosants had no effect. Contrast agents OMNIPAQUE™ and ULTRAVIST® initiated and prolonged the polymerisation of n-BCA, but in contrast, LIPIODOL® failed to initiate the process.
Conclusions
The commercially available medical cyanoacrylates differ in their polymerisation rates. These polymerisation rates are further affected when these products are used in conjunction with other compounds, such as sclero-embolic and contrast agents.
What this paper adds
Liquid embolic agents, and in particular cyanoacrylates, are used in endovascular and interventional settings for the treatment of vascular anomalies. Its use has been steadily increasing, and so have the reports of serious adverse events. Although the mechanisms associated with these adverse events remain poorly understood, reports have suggested a delay in the polymerisation of cyanoacrylates, and in particular cyanoacrylate and contrast agent mixtures, may be the cause. In this in vitro study, we measured the polymerisation rates of various commercially available cyanoacrylates and showed that the creation of mixtures of cyanoacrylates and contrast agents profoundly delays the polymerisation rates.
Introduction
n-Butyl cyanoacrylates (n-BCAs) are used in cyanoacrylate adhesive closure (CAC) procedures to treat superficial veins, in interventional radiology to treat vascular anomalies and in gastric surgery to treat gastric varices.1–5 There have been significant developments and advancements in the Interventional Neuroradiology (INR) speciality over the past five decades. Kerber et al. were the first to describe super-selective embolisation of intracranial vascular anomalies using a novel method involving isobutyl cyanoacrylate and a calibrated leak balloon system as early as 1978, 6 and Professor Kerber was the first to perform a carotid angioplasty in 1979.7,8 It is also worth noting that although the earliest liquid embolic agents used were isobutyl cyanoacrylate (branched chain), n-butyl cyanoacrylate (straight chain) has been since favoured, for its greater flexibility.
n-Butyl cyanoacrylates are produced as liquid agents that must undergo a polymerisation process to form a solid mass to occlude the target vessels. The polymerisation process comprises the three stages of initiation, propagation and termination. This process occurs within minutes of administration and follows exposure to blood, water or other anionic-containing compounds. The polymerisation rate of n-BCA is an important determinant of clinical outcomes. Accelerated polymerisation may result in catheter fixation and premature and incomplete occlusion of the intended treatment target. 9 Delayed polymerisation can result in entry and occlusion of the agent into non-target structures, increasing the risk of remote non-target embolisation and complications such as pulmonary and paradoxical embolism and strokes. 10
Commercially available n-BCA products are often used in interventional settings with radiopaque iodinated contrast agents under fluoroscopic guidance and not infrequently with sclero-embolic agents such as sclerosant foams to achieve better treatment outcomes. The effects of these adjunct products on the polymerisation rate of medical n-BCAs remain poorly understood. 11
This study aimed to investigate and directly compare the polymerisation activity of various commercially available n-BCA products in isolation and as mixtures with various compounds. To emulate the pre-injection and compound preparation phase, this in vitro study evaluated n-BCA initiation and polymerisation following contact with various additive compounds, including contrast agents, sclerosants and catheter priming agents.
Materials and methods
Ethical approval
Neither human subjects nor animal models were used in this in vitro study, and as such, Institutional Review Board (IRB) approval was not required.
Materials
VENASEAL™ (Medtronic, USA) and VENABLOCK™ (Invamed Saglik Liac A.S., Turkey), commercially available in Australia, approved by the Australian Therapeutic Good Administration as Class 2b medical devices, and categorised as venous adhesive occlusion system medical devices. HISTOACRYL® (B. Braun, Germany) is identical in all respects except is categorised as a Class 3, adhesive, soft tissue approximation medical device. All of these compounds contain the exact, same active ingredient, n-BCA. For comparison with other cyanoacrylates, a non-medical industrial adhesive SUPAGLUE™ (ethyl 2-cyanoacrylate; Selleys, NZ) was included.
Contrast agents used in the creation of mixtures included LIPIODOL® (Guerbet, France); ULTRAVIST®, Iopromide (Bayer Australia Ltd, Australia) and OMNIPAQUE™, Iohexol (GE Healthcare, Australia). OMNIPAQUE™ and ULTRAVIST® were chosen for their hydrophilic properties and ubiquity of use in the diagnostic radiology setting. In contrast, LIPIODOL® is a hydrophobic compound and possesses lipophilic properties.
n-butyl cyanoacrylates characteristics and classifications characteristics and classifications of commercially available n-BCAs, including polymerisation times reported in the medical literature and in this study.
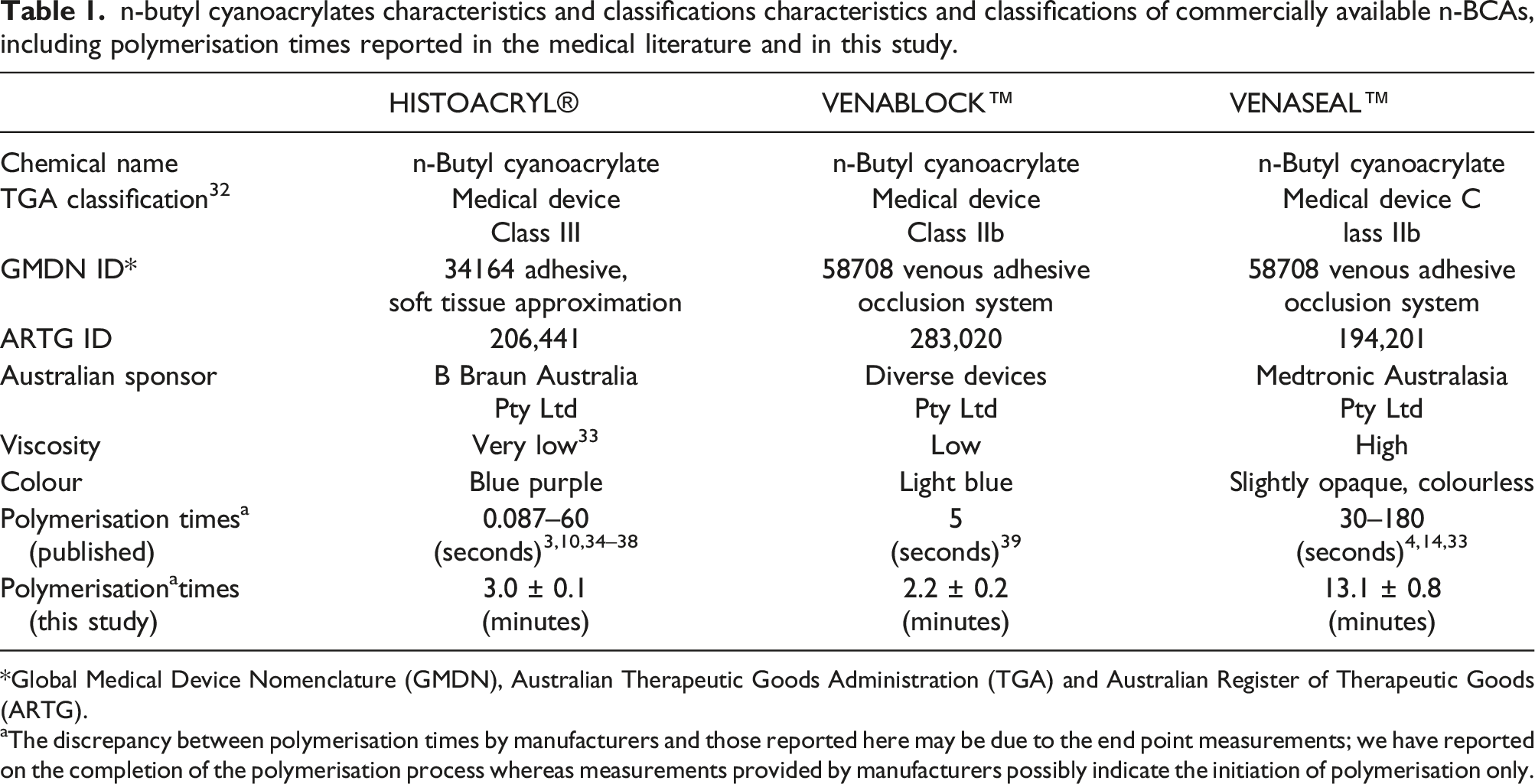
*Global Medical Device Nomenclature (GMDN), Australian Therapeutic Goods Administration (TGA) and Australian Register of Therapeutic Goods (ARTG).
aThe discrepancy between polymerisation times by manufacturers and those reported here may be due to the end point measurements; we have reported on the completion of the polymerisation process whereas measurements provided by manufacturers possibly indicate the initiation of polymerisation only.
Sclerosants used in this study included sodium tetradecyl sulphate (STS 3%; FIBROVEIN, STD Pharmaceuticals Ltd, UK), polidocanol (POL 3%; AETHOXYSKLEROL, Chemische Fabrik Kreussler & Co, Germany), hypertonic saline and absolute ethyl alcohol (ETHANOL; Thermo Fisher Scientific, NZ).
Other agents used in this study included glucose 75% (DEXTROSE; Victa Laboratorio de Manipulacao Ltda, Brazil) diluted with water for irrigation (Baxter, NSW, Australia), bovine serum albumin (BSA; Sigma-Aldrich, Australia), phosphate buffered saline (PBS; Gibco®, Life Technologies Ltd, Scotland, UK) and water for irrigation (Baxter, Australia).
Microplates: 96 well, flat-bottomed (Corning Inc, Jiangsu, China) were used to create and contain the n-BCA compounds and mixtures. Absorbance densitometry was performed using a FLUOstar® Omega (BMG Labtech, Germany) microplate reader.
Methods
n-Butyl cyanoacrylates polymerisation was assessed in vitro using absorbance densitometry as described previously. 12 The change in physical properties of n-BCA during polymerisation is associated with a change in the absorption of light at certain wavelengths. The densitometer enables the measurement of absorbance and, by proxy, polymerisation. The optical properties of n-BCA during polymerisation were examined using absorption densitometry, and the changes in absorption values were plotted over time, thus acting as a proxy for the polymerisation rate.
n-Butyl cyanoacrylates liquid monomer absorbance spectra
30 µL of each cyanoacrylate was pipetted into 96 well flat-bottomed microplates and pre-incubated at 37°C. All samples were examined within 10 min for absorbance in their native, liquid monomeric form and exposed to wavelengths ranging from 350 nm to 650 nm.
n-Butyl cyanoacrylates polymerisation in water
150 µL of water, pre-incubated at 37°C for 10 min, was added to the liquid monomers of each cyanoacrylate (30 µL) and allowed to polymerise spontaneously within the microplates. Samples were examined for absorbance [Abs (450 nm)] at 30-s intervals for 60 min. The time to achieve the maximum photo-absorbance of 3.0 units following initiation of polymerisation was defined as polymerisation time at 100% absorbance and was reported in minutes.
n-Butyl cyanoacrylates mixture polymerisation
30 µL of each n-BCA was pre-incubated in microplates for 5 min at 37°C. n-BCA mixtures were created by adding 150 µL of the respective agents. This equated to an n-BCA to agent ratio of 1:5 for all samples tested. Absorbance densitometry was used to quantitatively measure the absorbance of light through the mixtures at 450 nm over 60 min. All samples were maintained at 37°C during testing.
The following mixture groups were created by the addition of n-BCA to contrast agents, glucose (5%, 25% and 50%), sclerosants, BSA (4% and 10%) and in a range of pH.3,7,11
For clarity, changes in polymerisation were classified and reported according to the changes observed in the absorption curves as accelerated, unchanged, prolonged/delayed or incomplete. Accelerated: A more rapid rise in absorbance over time compared to the n-BCA standard. Unchanged: No change in absorbance rate compared to the n-BCA standard. Prolonged/delayed: A slower and more gradual rise in absorbance over time compared to the n-BCA standard. Incomplete: A rise in absorbance that fails to reach maximum absorbance compared to the n-BCA standard.
Temperature
Variations in temperature have been shown to alter polymerisation times and thus require attention. Warming reduces the viscosity of n-BCA liquid monomers; cooling prolongs polymerisation and preserves the monomeric state. 11 Testing was performed at 37°C in this study.
Statistical analysis
All experiments were independently repeated three times (n = 3). Results have been reported as mean values, with error bars representing the standard error of the mean. Statistical analysis was performed using Prism software (version 9.0).
Results
n-Butyl cyanoacrylates liquid monomer absorbance spectra
To determine the appropriate wavelength to assess n-BCA polymerisation, the absorbance of each un-polymerised agent was assessed from 350 to 650 nm (Figure 1). The 450 nm wavelength was selected to assess the polymerisation of n-BCA for the remainder of the study. The absorbance values measured for the liquid monomeric n-BCA provided the benchmark for negative controls used throughout this study (Figure 1). The values recorded for VENABLOCK™ and HISTOACRYL® demonstrated a peak in absorbance for wavelengths between 500 and 650 nm (Figure 1: inset). This is consistent with the blue colour observed for these compounds. n-BCA absorbance spectra measurements. (a) Liquid-monomeric state: The absorbance spectra of n-BCA for wavelengths from 350 to 650 nm. The dotted line indicates the wavelength (450 nm) selected to examine n-BCA mixtures for the remainder of the study. Inset: values recorded for VENABLOCK™ and HISTOACRYL® demonstrate a peak in absorbance for wavelengths between 500 and 650 nm. (b) n-BCA polymerisation of cyanoacrylate in water over time: 5-min pre-incubation period (shaded grey) before polymerisation was initiated with water. (c) The time to complete polymerisation was calculated for water. Bars represent the mean and error bars represent the standard error of the mean.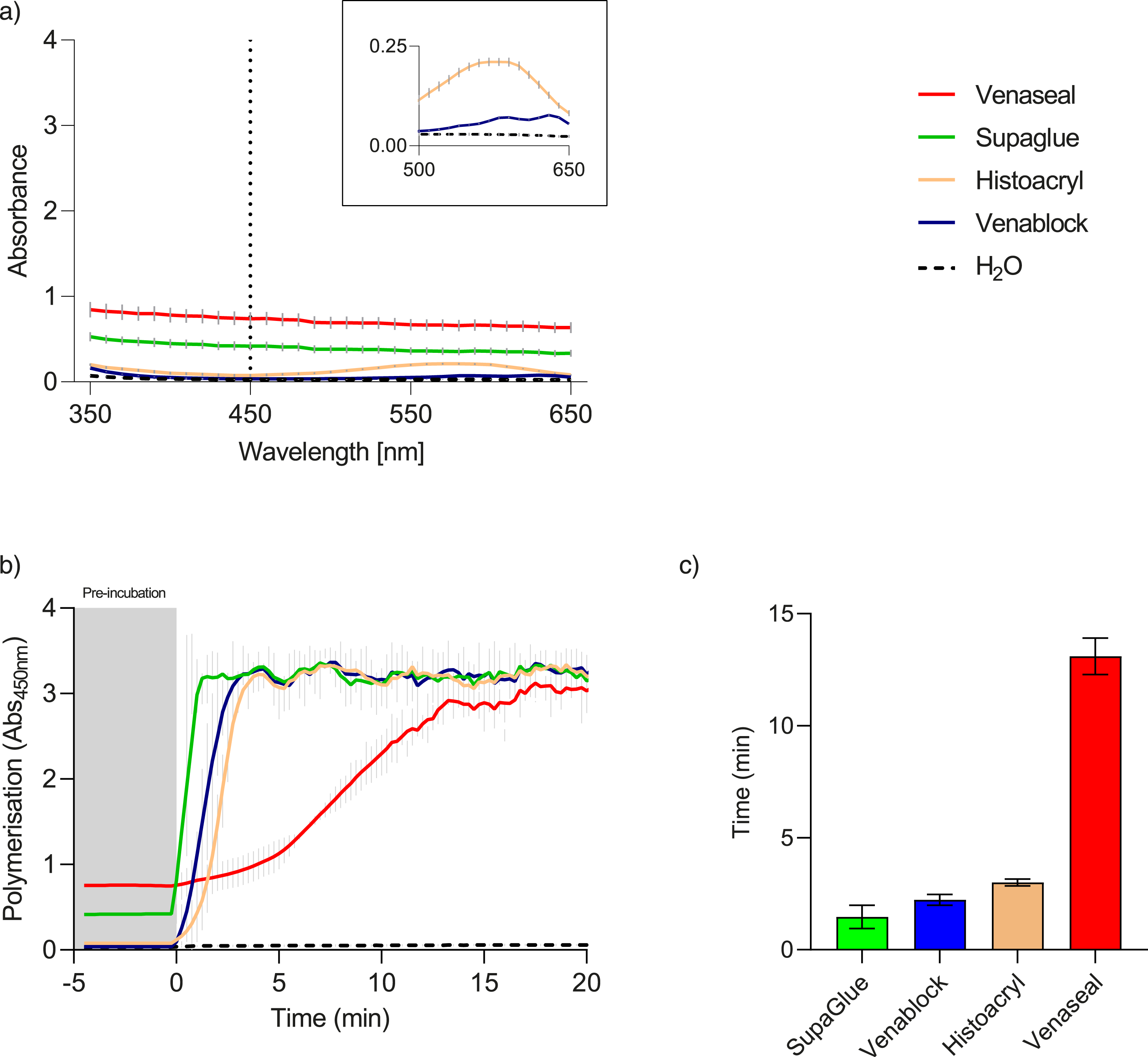
Polymerisation of n-butyl cyanoacrylates in water
Following initiation of polymerisation with water, all n-BCA agents examined showed an increase in absorbance over time. SUPAGLUE™ demonstrated the shortest polymerisation time (1.4 ± 0.5 min), followed by VENABLOCK™ (2.2 ± 0.2 min), HISTOACRYL® (3.0 ± 0.1 min) and finally VENASEAL™ (13.1 ± 0.8 min) (Table 1). VENABLOCK™ and HISTOACRYL® both demonstrated a rapid increase in absorbance that peaked within minutes. For VENASEAL™, this change in absorbance was slower, taking approximately 15 min to reach a peak (Figure 1).
Polymerisation of n-butyl cyanoacrylates in mixtures
n-Butyl cyanoacrylates plus contrast agents
There was no change in the absorbance of n-BCA and LIPIODOL® mixtures (n = 3), indicating that the n-BCA polymerisation was not initiated by LIPIODOL® and there was no polymerisation activity detected for the duration of the testing period (60 min). By contrast, the polymerisation of VENASEAL™ was initiated by ULTRAVIST® and OMNIPAQUE™, though polymerisation was prolonged when compared to controls. Other cyanoacrylates, including VENABLOCK™, HISTOACRYL® and SUPAGLUE™, underwent incomplete polymerisation with the addition of ULTRAVIST® and OMNIPAQUE™ (Figure 2). Polymerisation times for n-BCA in mixtures with contrast agents. There was no detectable polymerisation for either of the n-BCA and LIPIODOL® contrast agent mixtures (n = 3). By contrast, the polymerisation of VENASEAL™ was prolonged by ULTRAVIST® and OMNIPAQUE™ compared to controls. VENABLOCK™, HISTOACRYL® and SUPAGLUE™ showed incomplete polymerisation with the addition of ULTRAVIST® and OMNIPAQUE™.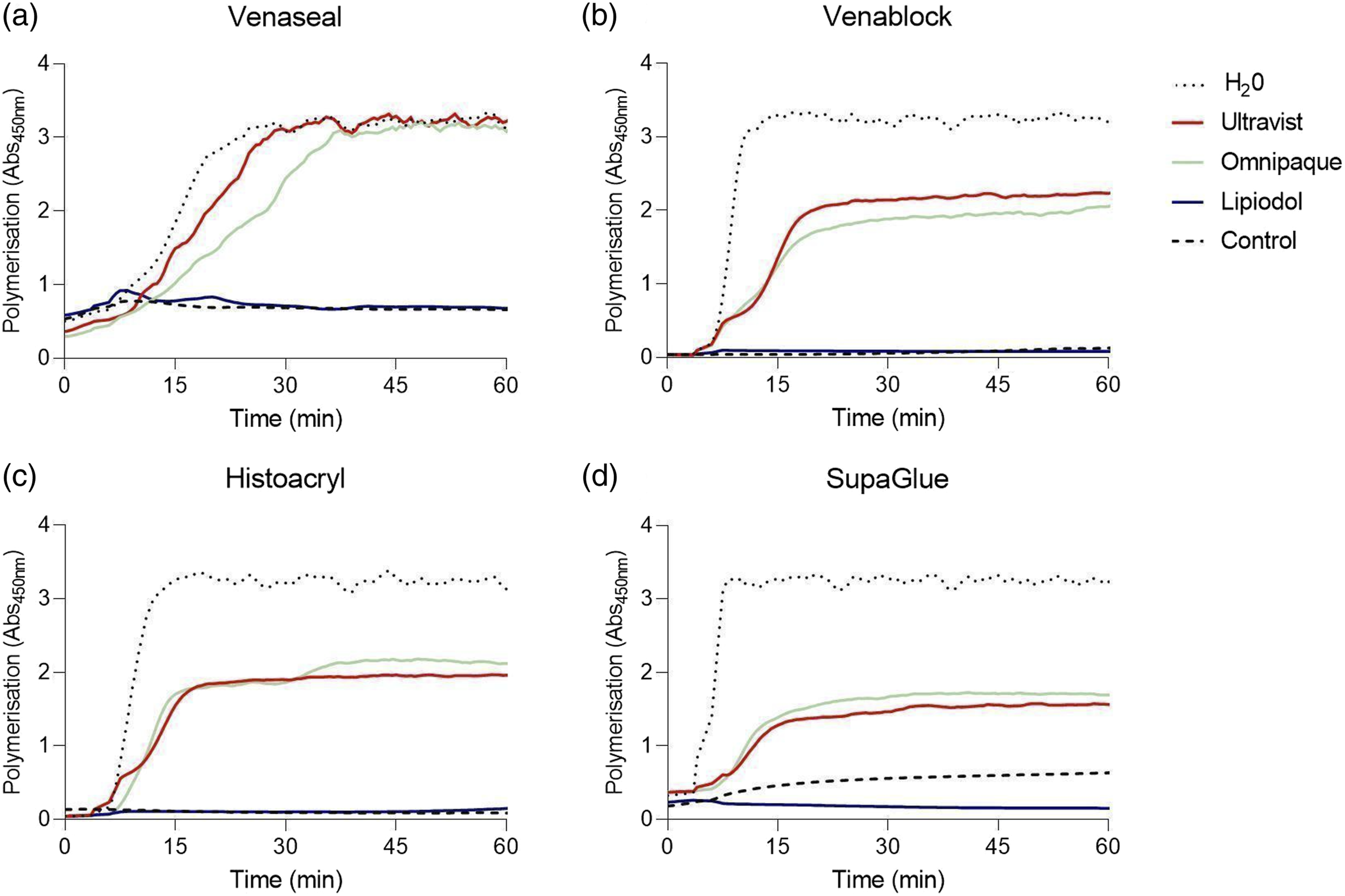
n-Butyl cyanoacrylates plus glucose
The mixture of n-BCA with 50% glucose resulted in the incomplete polymerisation of VENASEAL™ and prolonged polymerisation of the other n-BCAs. 25% glucose mixtures resulted in prolonged polymerisation of all n-BCAs and 5% resulted in only a minor change in polymerisation (n = 3, Figure 3). Polymerisation times for n-BCA in mixtures with varying concentrations of glucose. There was a prolongation of the polymerisation rate in all n-BCA and glucose mixtures resulting in a delay in polymerisation (n = 3). This effect was concentration dependent, with the mixtures containing the greatest concentrations of glucose requiring more time to polymerise.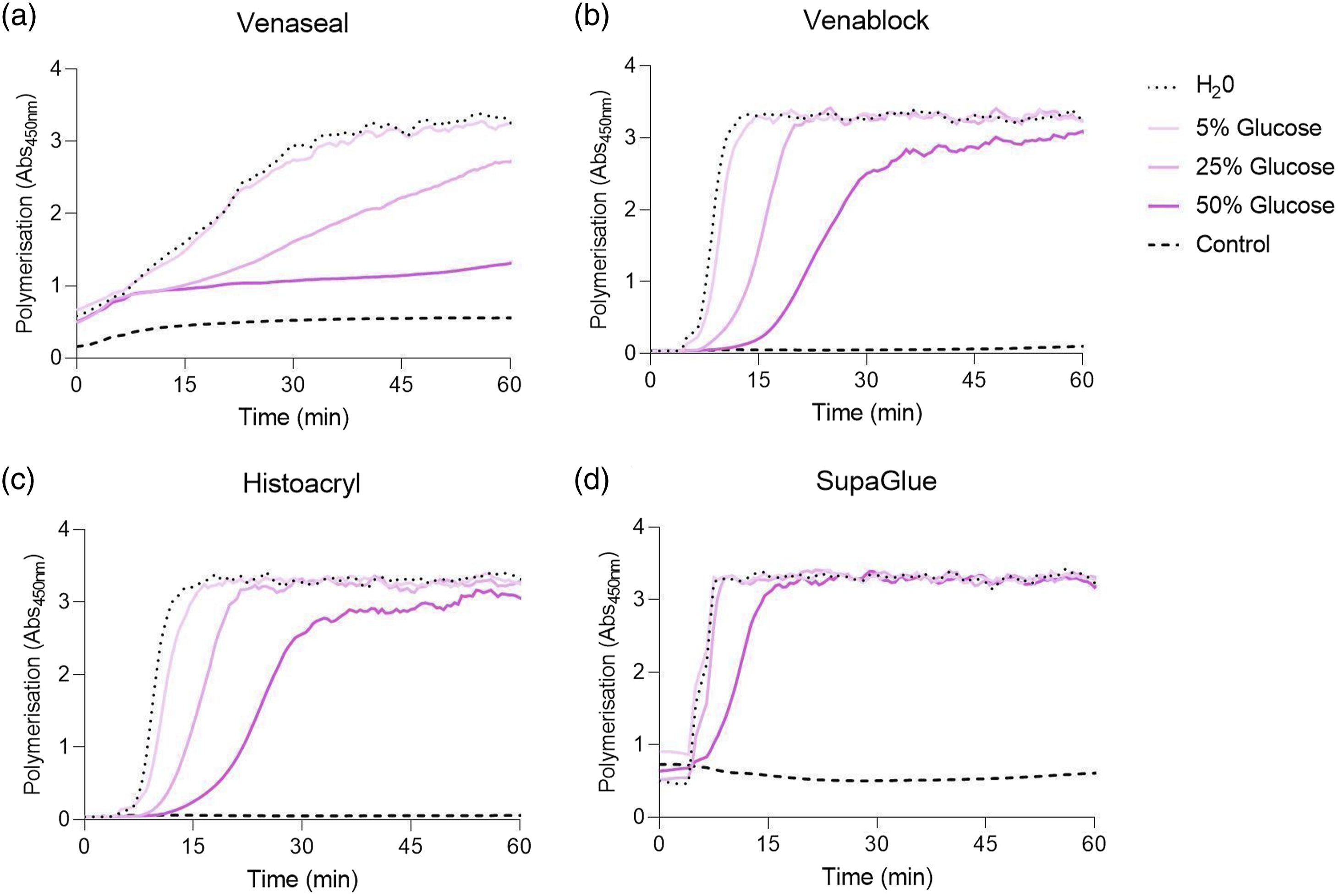
n-Butyl cyanoacrylates plus sclerosants
Hypertonic saline: The mixture of n-BCA with hypertonic saline resulted in the incomplete polymerisation of VENASEAL™, and prolonged polymerisation of VENABLOCK™ and HISTOACRYL®. Detergents sclerosants and ETHANOL: STS, POL and ETHANOL had little effect on VENASEAL™, VENABLOCK™ or HISTOACRYL® polymerisation. The addition of these agents resulted in incomplete polymerisation of the commercial SUPAGLUE™; however, this effect was not seen for the medical n-BCAs (Figure 4). Polymerisation times for n-BCA and various sclerosants. Only n-BCA and hypertonic saline mixtures resulted in the prolongation of polymerisation and this effect was most marked in the VENASEAL™ and hypertonic saline mixtures (n = 3). Notably, mixtures of n-BCA and the other sclerosants, including polidocanol (POL), sodium tetradecyl sulphate (STS) and ETHANOL, had little or no effect on polymerisation times.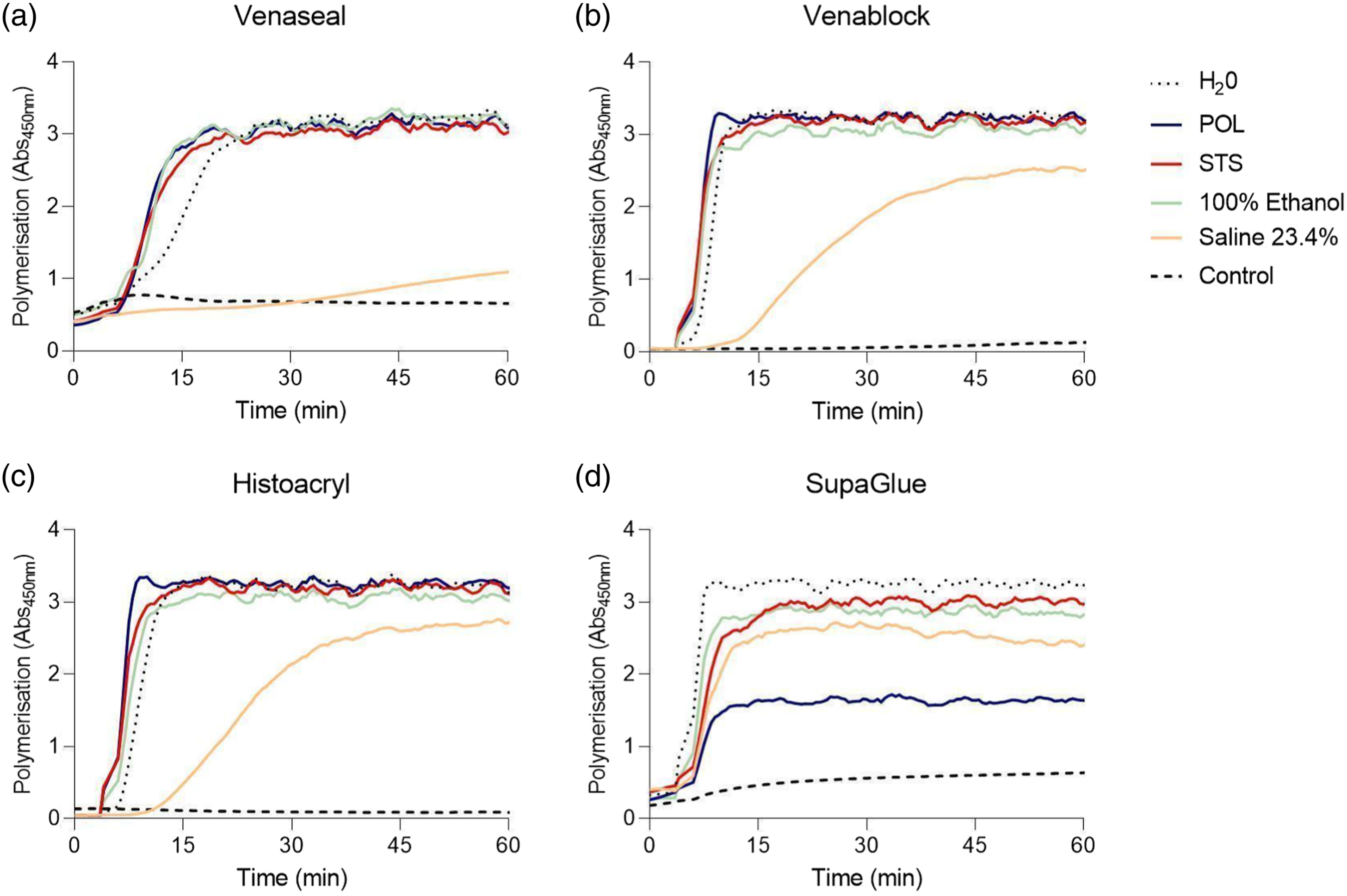
n-Butyl cyanoacrylates plus BSA
The presence of either 4% or 10% BSA in the n-BCA mixture had little effect on the polymerisation of HISTOACRYL® or VENABLOCK™; however, the presence of BSA accelerated the polymerisation of VENASEAL™. There was incomplete polymerisation of the commercial SUPAGLUE™ in BSA mixtures (Figure 5). Polymerisation times for n-BCA and protein mixtures. n-BCA polymerisation was accelerated in the VENASEAL™ and protein mixtures only and was most pronounced in the n-BCA and 10% protein mixtures (n = 3). This effect was not seen in any other n-BCA and protein mixtures.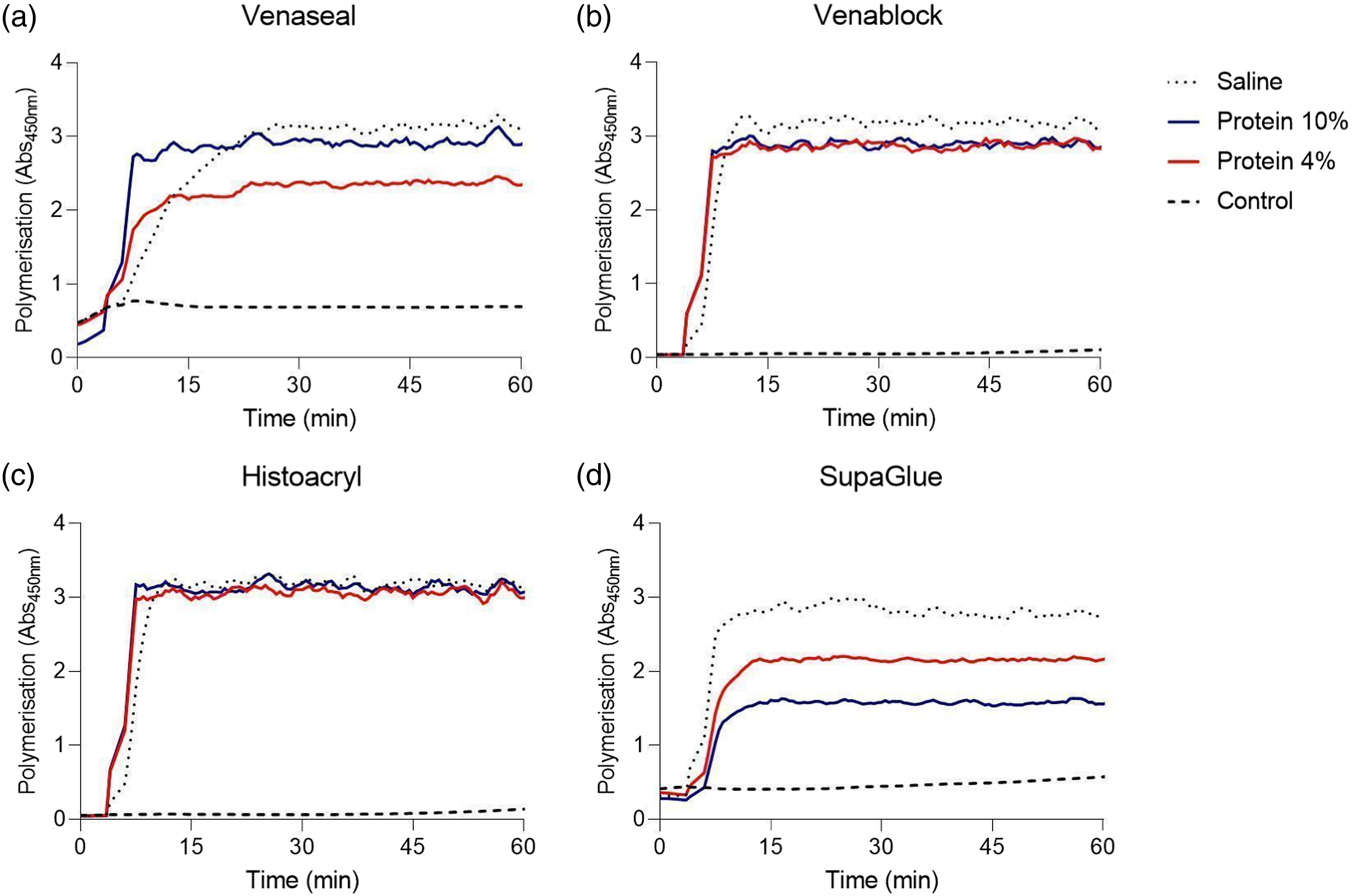
The effect of pH
There was only a slight delay in the polymerisation of n-BCA and pH three mixtures and a slight acceleration in the pH 11 mixtures in all n-BCA. This effect was most notable in the VENASEAL™ group (Figure 6), (n = 3). These data are consistent with findings previously reported by other authors.
13
Polymerisation times for n-BCA and various pH solution mixtures. There was a slight delay in the polymerisation of n-BCA and pH-3-mixtures and a slight acceleration in the pH-11-mixtures in all n-BCA (n = 3). This effect was most notable in the VENASEAL™ group.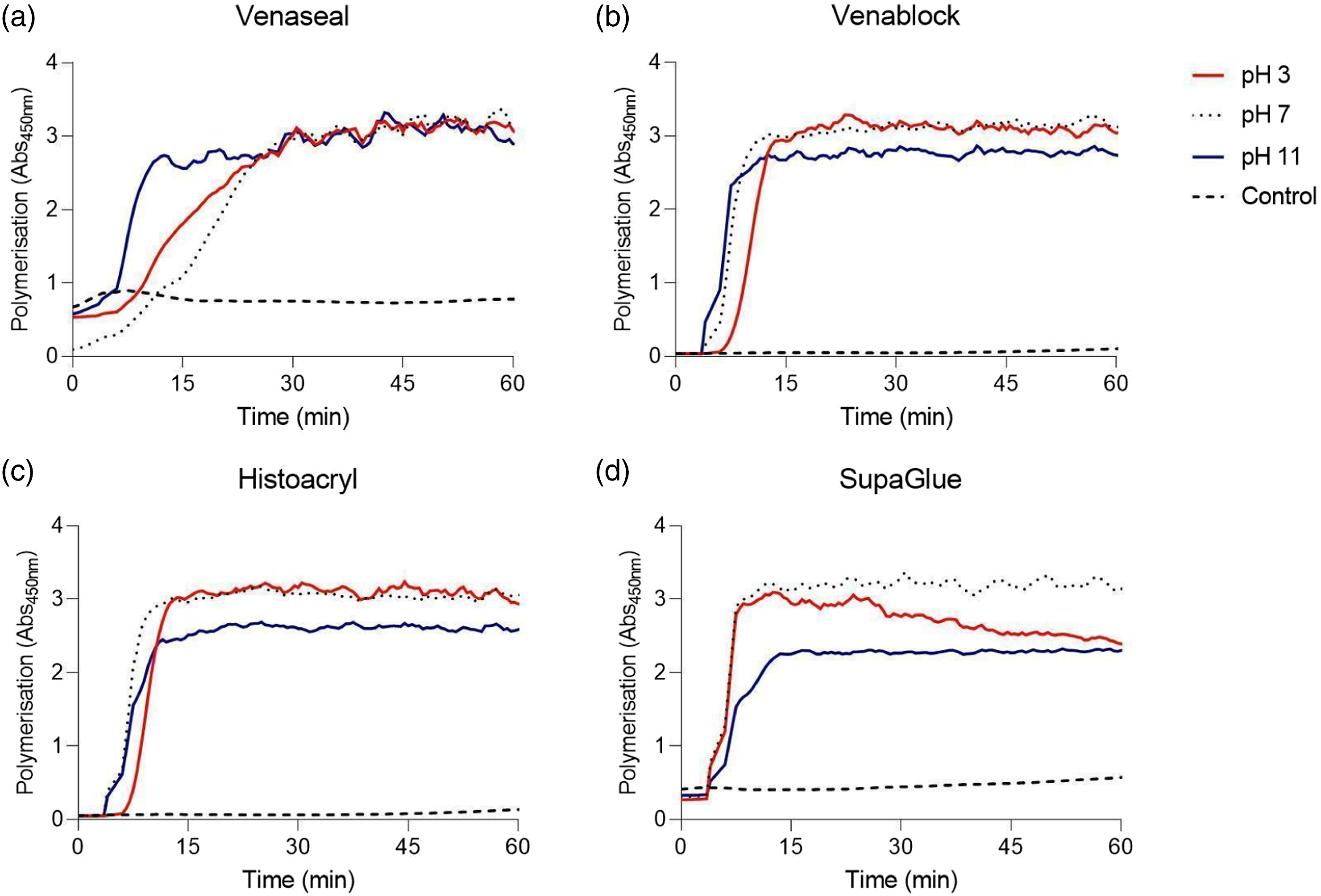
Discussion
Physicochemical properties of the n-BCA medical adhesives including viscosity and polymerisation kinetics are complex 14 and play an important role in the clinical utility of these agents.15,16 Here, we report on the polymerisation rates of cyanoacrylates, both in their native liquid monomeric forms and in mixtures with contrast and sclerosing agents (Table 1). Consistent with the published literature, VENASEAL™ was the slowest n-BCA to polymerise, while VENABLOCK™ and HISTOACRYL® were the fastest. Sclerosing agents, including ETHANOL, detergent sclerosants, hypertonic glucose and hypertonic saline, initiated the polymerisation of n-BCA products. However, these agents had varying effects on the polymerisation rate of cyanoacrylates. Osmotic sclerosants, including hypertonic glucose and hypertonic saline, prolonged the polymerisation rate of most n-BCAs. The addition of hypertonic saline resulted in incomplete polymerisation of VENASEAL™. By contrast, detergent sclerosants and ETHANOL (a chemical irritant) had no effect on the polymerisation rates of n-BCAs when compared with controls. Contrast agents OMNIPAQUE™ and ULTRAVIST® prolonged, while LIPIODOL® failed to initiate the n-BCA polymerisation.
In this study, the time taken for complete polymerisation was 2.2 and 13 min for VENABLOCK™ and VENASEAL™, respectively. These figures are significantly longer than those previously provided to the authors by the manufacturers (Table 1). To date, the manufacturers have not disclosed the industry methods for the measurement of viscosity or the polymerisation rate of n-BCA products. Viscosity and polymerisation data included in Table 1 were provided by the manufacturers following a request by the authors for inclusion in a consensus document of the Australasian College of Phlebology (ACP). 4 The discrepancy between the data provided by the manufacturers and those of the current study may be due to several reasons. Here, we measured the time taken from initiation to precipitation, cross-linking and curing, following initiation with pure water, and a range of contrast agents, sclerosants and hypertonic solutions, in a laboratory setting. 17 It is not clear whether the data provided by the manufacturers represent laboratory measurements or clinical indicators of polymerisation. Further methodological disclosures from manufacturers may help explain the reason for discrepancies.
An important finding of this study was the varying effects of contrast agents on the polymerisation of medical adhesives. LIPIODOL®, being an oil-based solution, failed to initiate the polymerisation of n-BCAs. This was most likely due to the immiscibility of oil molecules with the liquid adhesive. 16 LIPIODOL® and n-BCA mixtures are formulated with the goals of adding radio-opacity and slowing down the polymerisation rate. This method is leveraged by interventionalists and neurointerventionalists to enhance the precise placement of n-BCA. 18 By postponing its polymerisation, the n-BCA can extend further from the catheter's position to optimally reach and fill the target for vessel closure and n-BCA casting. This technique is especially useful when the microcatheter cannot be advanced further to the desired site of vessel occlusion. This effect is well understood clinically and is used to prevent inadvertent fixation of delivery catheters to target vessels.3,19 In the authors’ experience, a 1:1 ratio of n-BCA and LIPIODOL® would result in the glue setting in 1 s, a 1:4 ratio sets in 4 s and a 1:8 combination would set in 8 s 20 The exposure of intravascular blood to the n-BCA-LIPIODOL® mixture would initiate the polymerisation but a higher content of LIPIODOL® in the mixture would reduce the exposure of n-BCA to blood and hence slow down the polymerisation rate. By contrast to LIPIODOL®, the non-oil-based contrast agents OMNIPAQUE™ and ULTRAVIST® could initiate the polymerisation, but similar to LIPIODOL®, both agents prolonged the rate of the process.
There have been numerous case reports of remote, and paradoxical embolisms in patients who have been treated with n-BCA/LIPIODOL® mixtures. 21 The mechanisms are poorly understood; however, it has been suggested that the risk of embolic complications may depend on multiple factors, including injection volume, injection pressure and n-BCA/LIPIODOL® mixture ratios. 20 The complete absence of initiation of n-BCAs by LIPIODOL® in this study should raise clinical concern for the treating Interventionalist. A similar reduction in the sclerosant effect was observed and reported by the authors with the interaction of sclero-embolic agents and LIPIODOL® mixtures. 22
In this study, the volumes of cyanoacrylate and dilution medium in a 1:5 ratio were selected for methodological reasons, based on the minimum volume for cyanoacrylates that could be evaluated in a 96-well plate and sufficient volume of medium to measure a response within the limits of detection of the spectrophotometer. We acknowledge the various dilutions of contrast media and cyanoacrylate are used according to clinical indications and target-lesion treatment strategy; however, the results from this study would be comparable for all these dilutions and cyanoacrylates.
n-Butyl cyanoacrylates products have been reported to be used in conjunction with sclerosing foams to potentiate the occlusion rates achieved by these products. 23 In our study, the addition of STS, POL and ETHANOL initiated the polymerisation of n-BCA but did not alter the rate. Exposure of liquid n-BCA monomers to anionic polar molecules such as blood or water initiates the polymerisation process. 11 STS is an anionic polar detergent. All alcohols including ETHANOL and POL are polar compounds. The commercial form of POL, AETHOXYSKLEROL, contains 5% (v/v) ethanol and water for injection. These additional components, ethanol and water, further potentiate the initiating effects of POL on n-BCA. Clinically, the mixing of the two liquid agents (liquid n-BCA with a liquid sclerosant) would result in premature polymerisation of the glue before its intravascular injection. However, the mixing of liquid n-BCA with foam sclerosants would not have the same immediate effect. The gas component of the sclerosing foam would reduce the exposure of the n-BCA liquid monomer to the active detergent allowing its clinical use. 23 The clinical benefits of mixing the n-BCA liquid monomers with sclerosing agents are yet to be conclusively determined.
Glacial acetic acid (GAA) and the creation of mixtures of this compound with n-BCAs may be used in the interventional setting to achieve a beneficial delay in polymerisation. In this study, the sample mixtures containing cyanoacrylate and acidic solution (pH = 3) demonstrated a delay in polymerisation, which is consistent with the observed delay in polymerisation associated with GAA and n-BCA mixtures. In scenarios where target lesions are injected under fluoroscopy guidance, Tantalum may also be added to the mixture to enhance the radio opacity of the active liquid embolic agent. The advantage provided by the use of Tantalum and GAA in place of LIPIODOL® is that only small amounts (3.7%–7.1% by volume) of GAA and Tantalum are required to achieve significant delays in polymerisation times (from 2.3 s to 7.8 s) without excessive dilution and consequent loss of embolisation efficacy. 24 It has been shown that the use of higher volumes of LIPIODOL® in n-BCA mixtures may be associated with a higher incidence of unwanted treatment failures due to multiple factors, including the reduction in the sump effect, eventual steal phenomenon and endothelial cell-mediated mechanisms. 25
Therapeutic microcatheters and intravascular access devices are often rinsed with a non-ionic solution, such as glucose or dextrose solution, to remove residual blood and to prevent the risk of catheter adhesion within the target vessel. 26 In the study, it was demonstrated that glucose of increasing concentrations caused a shift of the polymerisation curve to the right, correlating with increased polymerisation times; this effect was observed across all n-BCAs tested (Figure 3). Therefore, the findings in this study provide a rationale for the use of glucose solution as a catheter priming agent.
It is worth noting that cyanoacrylate polymerisation is an exothermic reaction and that with a reduction in the alkyl chain length, there is a corresponding increase in polymerisation temperature. 27 It has been shown that with a reduction in temperature, cyanoacrylate viscosity increases, and this may also alter polymerisation rates. 28 To standardise our measurements across all samples and for the duration of the testing period, the samples were therefore incubated at 37°C. This was done to ensure that the samples were not exposed to the ambient temperature of the lab, but rather 37°C consistent with the expected temperatures in vivo and that all samples were subjected to the same corresponding increase in temperature that would be expected to occur in vivo.
Endovenous glue induced-thrombosis (EGIT), defined as thrombus extension from the treated superficial veins, such as saphenous trunks, into the adjoining deep veins, has been described as a complication of CAC in 5%–13% of patients.29,30 The manufacturers recommend a minimum of 2–5 cm distance between the tip of the catheter and the saphenofemoral junction to prevent glue extension and a subsequent EGIT. Exposure of the deep veins to the injected n-BCA and prolonged polymerisation may result in the occlusion of adjoining deep veins and possible embolisation to remote and distant sites. 15 Agents with low viscosity and/or prolonged polymerisation rate are more likely to end up in a deep vein following a high-pressure injection, resulting in an increased risk of EGIT. Further studies are required to assess the influence of polymerisation kinetics on the clinical incidence of EGIT. In an attempt to reduce inadvertent embolic agent efflux or reflux and non-target embolisation, clinicians have used coils immediately prior to cyanoacrylate embolisation. 20 The rationale behind this approach is to minimise the collateral flow of the embolic agent by reducing the number and size of intralesional high-flow vessels. 31 Techniques such as this, however, cannot be performed in peripheral venous occlusive procedures.
The main limitation of this study was its lack of access to basic product information of the commercially available n-BCA products held as proprietary information by the manufacturers. Medical cyanoacrylates are registered as medical devices, and manufacturers are not required to disclose the chemical composition of these products. Medical n-BCAs differ in their physicochemical properties, including viscosity and polymerisation rates. The differences are most likely related to the composition of the additives and solvents not disclosed by the manufacturers and held as proprietary information. This group is undertaking further studies to detect excipients and degradation products of medical-grade cyanoacrylates. This will help us understand the biochemical composition of medical n-BCA agents and assess their safety in their medical application. Whole blood was not used to initiate polymerisation in this study because of the photo-absorbance properties of red blood cells. In our absorption densitometry model, the presence of red cells in the test samples would shift the absorbance levels above the limits of detection. In the case of n-BCA initiation of the mixtures with contrast agents, sclerosants and hypertonic solutions, the additives were the only compounds used to initiate polymerisation. This is most relevant in the clinical setting because these compounds are created outside the body prior to injection. Therefore, a technical limitation of this study was its lack of incorporation of blood in the experimental designs. For similar reasons, the foam format of detergent sclerosants could not be included in the experimental design. In vivo, blood is the key initiator of the n-BCA polymerisation and foam sclerosants are routinely used in clinical settings. Future laboratory-based studies should incorporate sclerosing foams and blood in experimental settings that use alternative methods.
In conclusion, n-BCA polymerisation was initiated by all sclerosing agents, including detergent sclerosants, ETHANOL, hypertonic glucose and hypertonic saline. Osmotic sclerosants prolonged the polymerisation rate of most n-BCAs, while detergents and ETHANOL did not alter the polymerisation rate. Contrast agents OMNIPAQUE™ and ULTRAVIST® prolonged, while LIPIODOL® failed to initiate the n-BCA polymerisation.
Footnotes
Acknowledgements
The authors acknowledge the facilities and the support of the St Vincent's Centre for Applied Medical Research (AMR) and the University of New South Wales Faculty of Medicine. We wish to thank Dr David Roboinson for his insights into the manuscript and Dr Simon Thibault, Dr Fabricio Santiago and Dr Stefania Roberts for donating materials used in this study.
Author contributions
Joseph Gracé was involved in; study design, experimentation and interpretation, analysis, statistical analysis and manuscript preparation. Chris Rogan and Lourens Bester were involved in the study design, analysis, and manuscript contribution. David Connor was involved in the performance of experiments, supervision of experiments performed by Joseph Gracé, study design, statistical analysis and manuscript preparation. Kurosh Parsi was involved in study design, analysis and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.