
Abstract
Objectives
This study aimed to investigate the impact of post-interventional compression therapy on clinical outcomes after endovenous laser ablation (EVLA) of incompetent saphenous veins.
Methods
This prospective, controlled, multicenter study in Germany involved 493 varicose vein patients followed-up for 6 months.
Results
Compression therapy significantly reduced symptoms compared to no compression (VCSS: 1.4 ± 1.6 vs 2.2 ± 2.2; p = .007). Post-interventional therapy duration of up to 14 days was found to be most effective for improving patient-reported disease severity (p < .001) and higher quality of life (p = .001). Patient compliance was high (82%), and non-compliance was linked to worse disease severity (VCSS 1.4 ± 1.5 vs 2.1 ± 2.3, p = .009).
Conclusion
In conclusion, post-interventional compression therapy is beneficial by reducing symptoms and improving quality of life. High patient compliance with the therapy is observed, and non-compliance is associated with worse disease severity.
Keywords
Introduction
Chronic venous insufficiency is a disorder commonly caused by varicose veins and affects up to 50% of the adult population in Western countries, with 25% displaying visible varicose veins.1,2 This disease is typically associated with reflux in the epifascial lower extremity veins, particularly the great saphenous vein, leading to hyperpigmentation, edema, lipodermatosclerosis, and eventually ulceration.2,3 For many years, endovenous laser ablation (EVLA) of incompetent saphenous veins is used successfully with an excellent side effect profile.4–7 Historically, post-interventional compression therapy has been recommended as an adjunct strategy to reduce the risk of recurrence through mechanical occlusion of the ablated vein. 8 Further, compression has been hypothesized to reduce post-interventional pain, hematoma, edema, risk of thrombosis, and time to return to work following venous intervention.8–10
However, the effectiveness and required duration of compression therapy following EVLA is subject to an ongoing debate as previous studies led to partially conflicting results.3,9–12 Bakker et al. and Bootun et al. reported less pain and improved physical function early post-intervention when patients received compression therapy for more than 2 days compared to no compression, however with no remaining differences at 6 weeks.9,11 In 2016, Ye et al. reported that compression therapy did not significantly affect quality of life or time to return to work but may reduce swelling during the first week post-intervention. 10 Similarly, Hu et al. concluded that the use of compression stockings after EVLA did not result in improved outcomes, except for transient pain relief. 12 Moreover, the available literature is limited by inconsistent study designs, widely varying compression durations, ranging from hours to weeks and often small sample sizes.9,10,13 Similarly, inconsistent patient compliance with post-interventional compression has been reported, with rates ranging from 40% to 94%.13,14 Krasznai et al reported a compliance rate of 94%; however, they only recommended compression therapy for 72 h. 13 Other studies have found rates of 91.5% and 87% after one and 2 weeks, respectively. 10 In contrast, Hamel-Desnos et al reported poor compliance with the compression regime, with patients wearing compression stockings for an average of 11 days out of the 21 scheduled days, and only 40% of patients wearing them daily. 14 Thus, we aimed to determine predictors for patient compliance and quantify the effect of short versus long-term compression therapy on occlusion rate, post-interventional complications, and quality of life following EVLA in one of the largest prospective multicenter studies to date.
Methods
This controlled, multicenter study was performed in a prospective setting including 493 patients with insufficient great saphenous veins (GSV) with a medical indication for elective thermal ablation. Only patients with complete data sets regarding the compression therapy were included in the analysis. This project is a sub-study of the SYNCHRONOUS study which aims to examine the influence of the anterior accessory saphenous vein (AASV) on the development of recurrent veins within a prospective controlled environment. The aim of the study is to determine the potential benefits for patients undergoing preventive ablation of a sufficient AASV. The study was conducted in accordance with the Declaration of Helsinki principles (2013) and written informed consent for the procedure was obtained by all patients. Patient recruitment took place between February 2019 and June 2021 in 9 study centers throughout Germany. Participating study centers were: Venenzentrum der Dermatologischen und Gefaßchirurgischen Kliniken Bochum, Venenzentrum Freiburg, Praxis fur Innere Medizin und Gefaßkrankheiten Halle/Saale, Venenzentrum am Bruhl Leipzig, MVZ Dr. Ph. Zollmann & Kollegen, Jena, Venenzentrum Pforzheim Pforzheim, Venen-Fachpraxis Regensburg, Dermatologikum Hamburg and Private Practice Dermatology and Phlebology Bonn. Patients presenting at the study centers with venous reflux were screened for the eligibility criteria and subsequently enrolled into the study. Initially, the study was approved by the independent ethics committee of the medical faculty of the University of Heidelberg (Ethics approval number S-596/2018) and registered at the German Clinical Trial Register (DRKS00015486).
Objective of this study was to assess the impact of postoperative compression therapy on different clinical outcome measures, such as occlusion rate, postoperative complications and pain, patient satisfaction, quality of life, and patient-reported disease severity. Furthermore, impact of short versus long term compression therapy on the outcome measures was evaluated. Another objective was to determine patients’ compliance with the compression therapy and to identify potential predictors of non-compliance. Patients who completed the recommended duration of compression, or longer were considered compliant.
Patients were followed-up over a period of 6 months. In total, 4 study visits were performed. Patients were examined at the time of recruitment, the day of EVLA, 10 days and 6 months after EVLA. All patients were examined clinically and by duplex ultrasound by experienced phlebologists. According to the standard operating procedures at the respective study centers, the treatment of the AASV occurs simultaneously in patients undergoing EVLA for an insufficient GSV or not. In all study centers, EVLA is conducted using a 1470 nm two-ring radial laser (Biolitec, Jena, Germany). The laser fiber is introduced into the GSV at the point of insufficiency distally, using a sheath, and is then positioned at the Sapheno-Femoral Junction (SFJ) while under sonographic guidance. The entire EVLA procedure is performed with sonographic monitoring and local tumescent anesthesia. If necessary, additional procedures, that is, miniphlebectomies and sclerotherapy were performed.
Postoperative compression therapy was initiated immediately after EVLA in all study centers using class I (18–21 mmHg) or II (23–32 mmHg) A-G medical compression stockings. The post-interventional compression regime was predefined for each center based on their preference and patients were subsequently grouped according to the recommended time of compression in short (1–14 days), long (>14 days), or no compression (0 days). At the 6-months visit, the patients were asked how long they actually wore the compression stockings.
At 6 months post-intervention, all treated veins were examined by duplex ultrasound, and occlusion status was documented by means of four different categories: “closed” and “partially closed with antegrade flow” was defined as a therapy success. The categories “partially closed with reflux” and “open with reflux” indicated a therapy failure.
Postoperative pain was assessed by means of the NRS (numerical rating scale 1–10) 10 days and 6 months after EVLA. Patient satisfaction was evaluated on a scale of 1–5, quality of life using the Aberdeen Varicose Vein Questionnaire (AVVQ), and disease severity through the Venous Clinical Severity Score (VCSS) at baseline and 6 months post-intervention.15,16
Post-interventional complications were documented within the first 10 days and 6 months after the intervention. Post-interventional complications were grouped according to their severity in none, mild (matting, pain, hematoma, ecchymosis, hyperpigmentation), moderate (par- or dysesthesia, numbness, superficial vein thrombosis, burn, post-interventional thrombus extension grade II (PATE II)), and severe (PATE III and IV and deep vein thrombosis).
The data is reported as mean with standard deviation for normally distributed data, median with interquartile range for non-normally distributed data, or as a proportion for categorical data. Patients with incomplete data for each respective outcome were excluded from the analysis. Demographic and clinical characteristics of the patients were compared using a chi-squared test for categorical variables, a t-test for normally distributed variables, or a Mann–Whitney’s U test or Wilcoxon test for non-normally distributed and ordinal variables. In the comparison of multiple groups, a chi square test, an ANOVA, or Kruskal–Wallis test was implemented. Since this was a sub-study of the Synchronous study, all presented results are based on exploratory analyses with no confirmatory value. A p-value < .05 was considered statistically significant with no adjustment for multiple testing. All statistical analyses were performed using R 17 in combination with the packages DescrTab2, 18 readxl, 19 dplyr, 20 finalfit, 21 and ggplot2. 22
Results
Univariate analysis of patient characteristics.
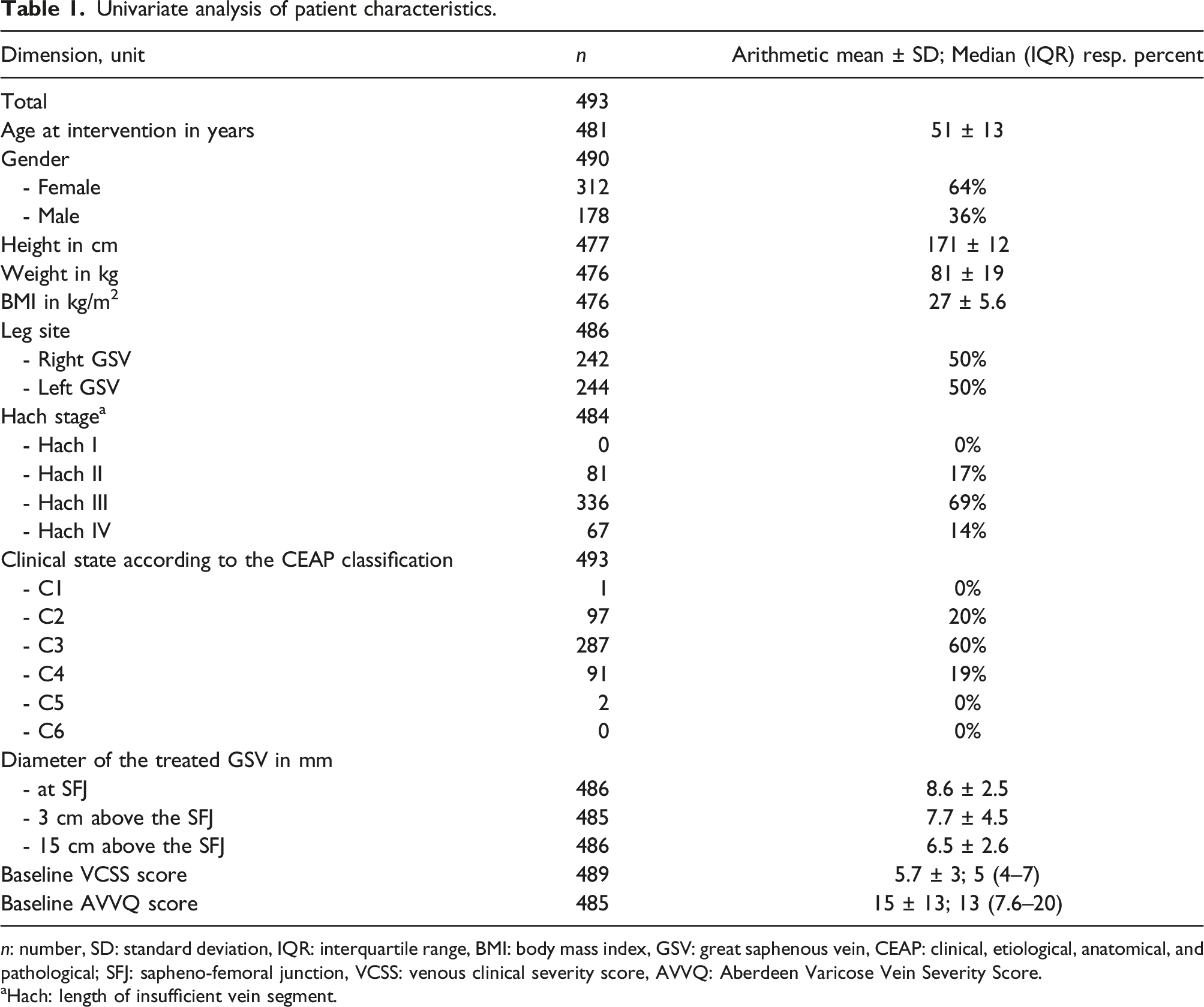
n: number, SD: standard deviation, IQR: interquartile range, BMI: body mass index, GSV: great saphenous vein, CEAP: clinical, etiological, anatomical, and pathological; SFJ: sapheno-femoral junction, VCSS: venous clinical severity score, AVVQ: Aberdeen Varicose Vein Severity Score.
aHach: length of insufficient vein segment.
Adjunctive procedures
Subgroup analysis comparing patients with and without post-interventional compression.
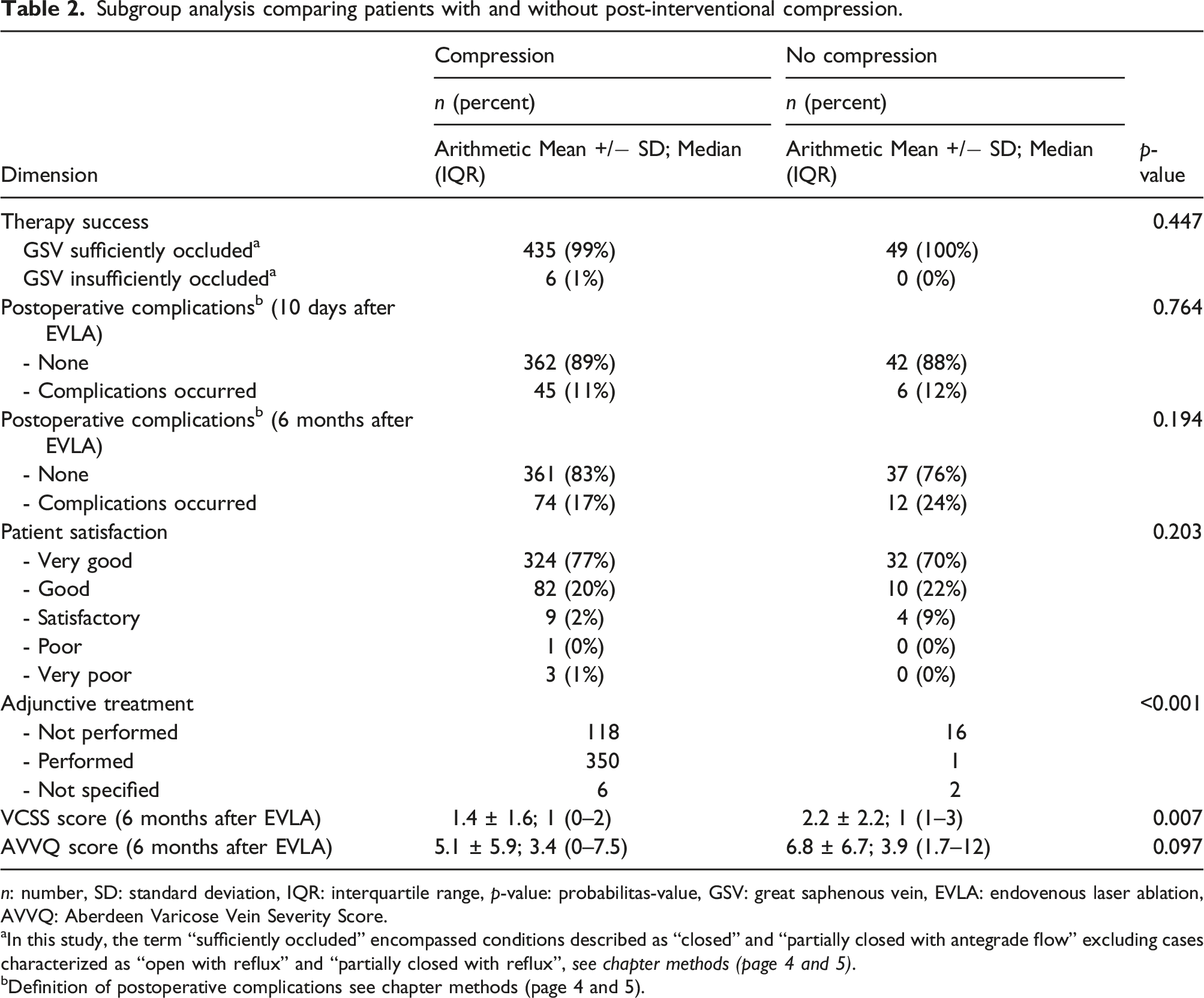
n: number, SD: standard deviation, IQR: interquartile range, p-value: probabilitas-value, GSV: great saphenous vein, EVLA: endovenous laser ablation, AVVQ: Aberdeen Varicose Vein Severity Score.
aIn this study, the term “sufficiently occluded” encompassed conditions described as “closed” and “partially closed with antegrade flow” excluding cases characterized as “open with reflux” and “partially closed with reflux”, see chapter methods (page 4 and 5).
bDefinition of postoperative complications see chapter methods (page 4 and 5).
Impact on clinical outcome measures
Occlusion rate
Subgroup Analysis of different compression therapy durations.
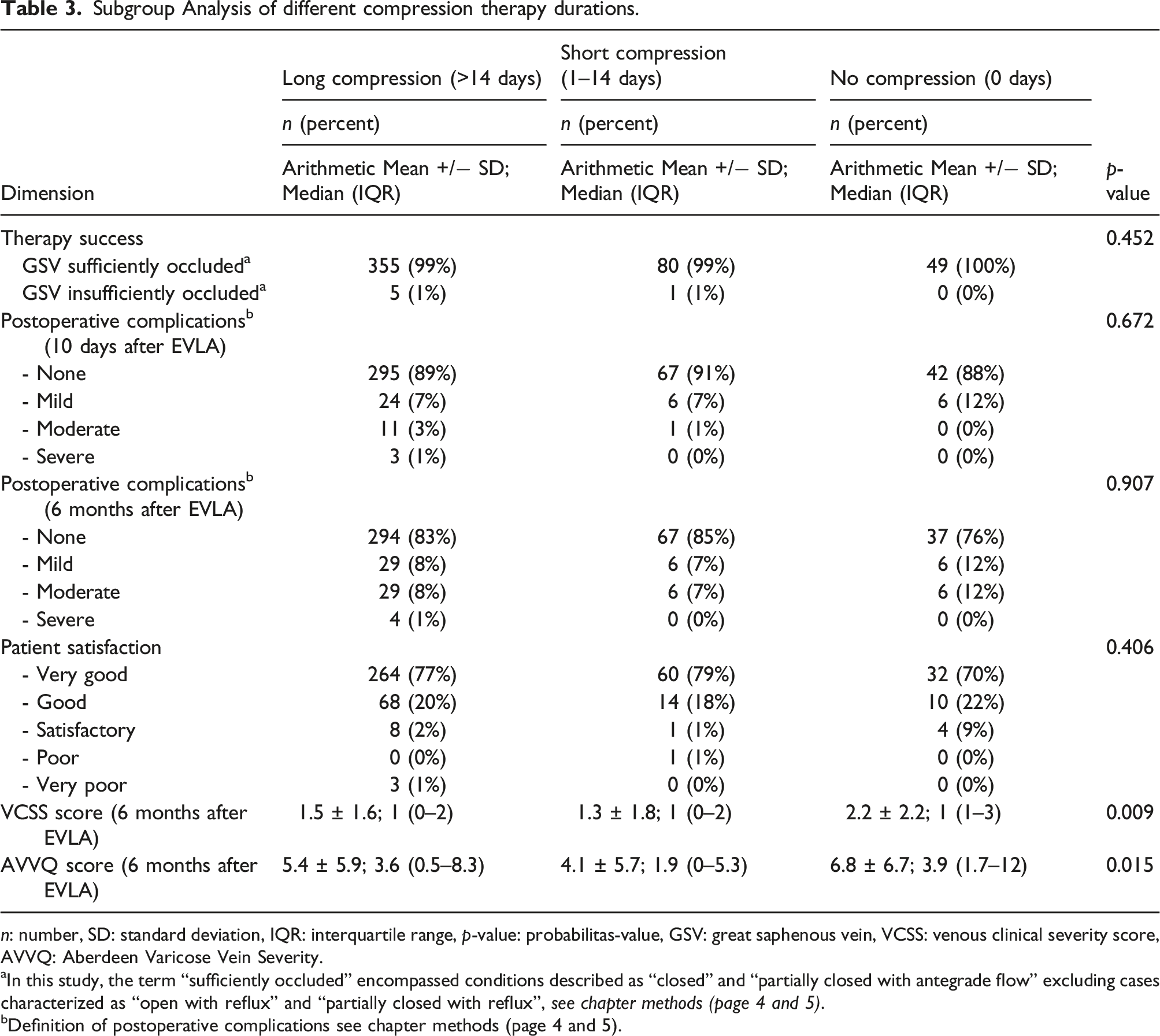
n: number, SD: standard deviation, IQR: interquartile range, p-value: probabilitas-value, GSV: great saphenous vein, VCSS: venous clinical severity score, AVVQ: Aberdeen Varicose Vein Severity.
aIn this study, the term “sufficiently occluded” encompassed conditions described as “closed” and “partially closed with antegrade flow” excluding cases characterized as “open with reflux” and “partially closed with reflux”, see chapter methods (page 4 and 5).
bDefinition of postoperative complications see chapter methods (page 4 and 5).
Post-interventional complications
Six months complication rates following endovenous laser ablation.
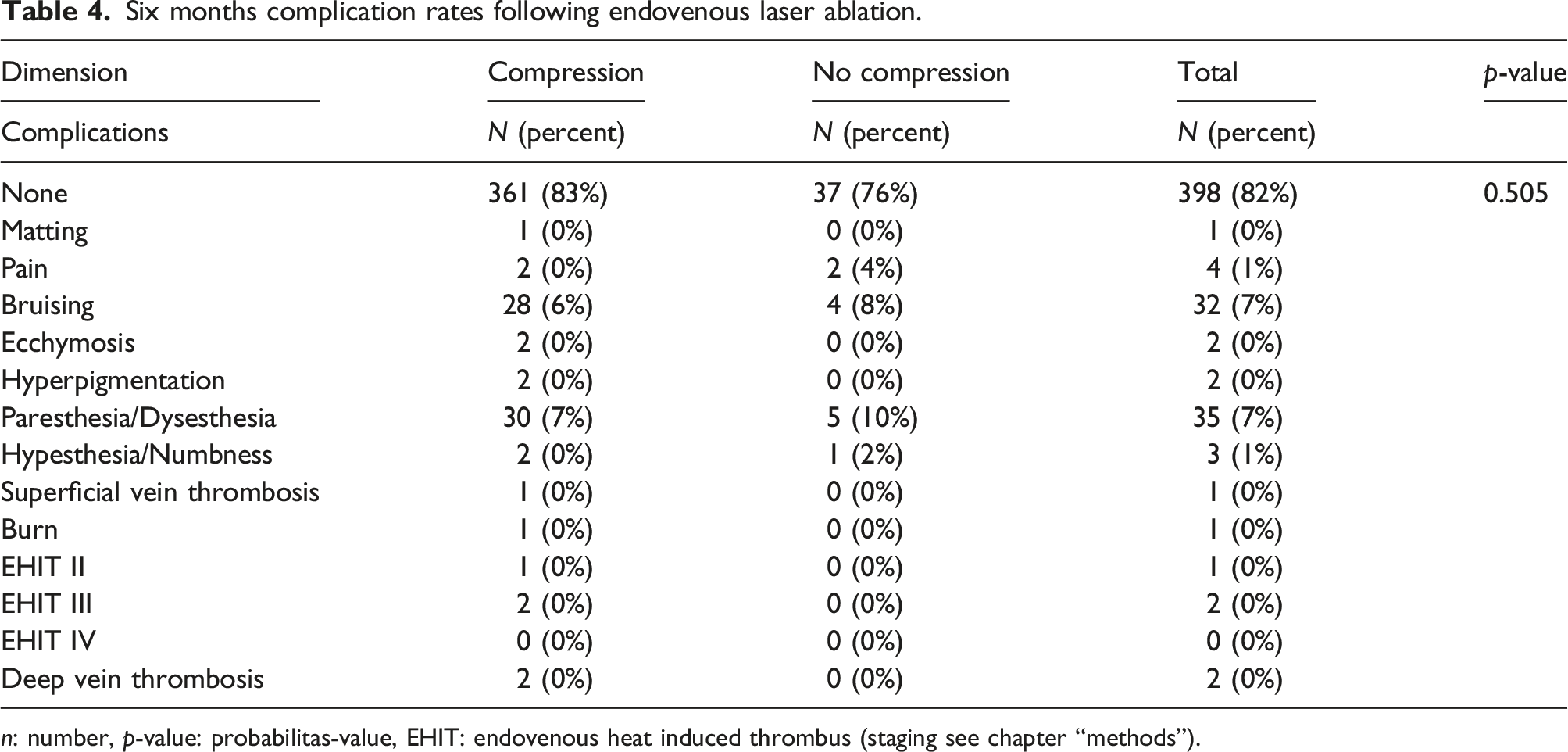
n: number, p-value: probabilitas-value, EHIT: endovenous heat induced thrombus (staging see chapter “methods”).
Duration of post-interventional pain
On average, patients reported a post-interventional pain duration of 2.5 (±4.5) days with no significant difference between the cohort with and without post-interventional compression (p = .248). Patients that experienced longer periods of pain, tend to adhere to significant longer durations of compression therapy (p = .043).
Disease severity (VCSS score), quality of life (AVVQ score), and patient satisfaction after 6 months
Univariate Analysis of outcome measures 6 months after endovenous laser ablation.
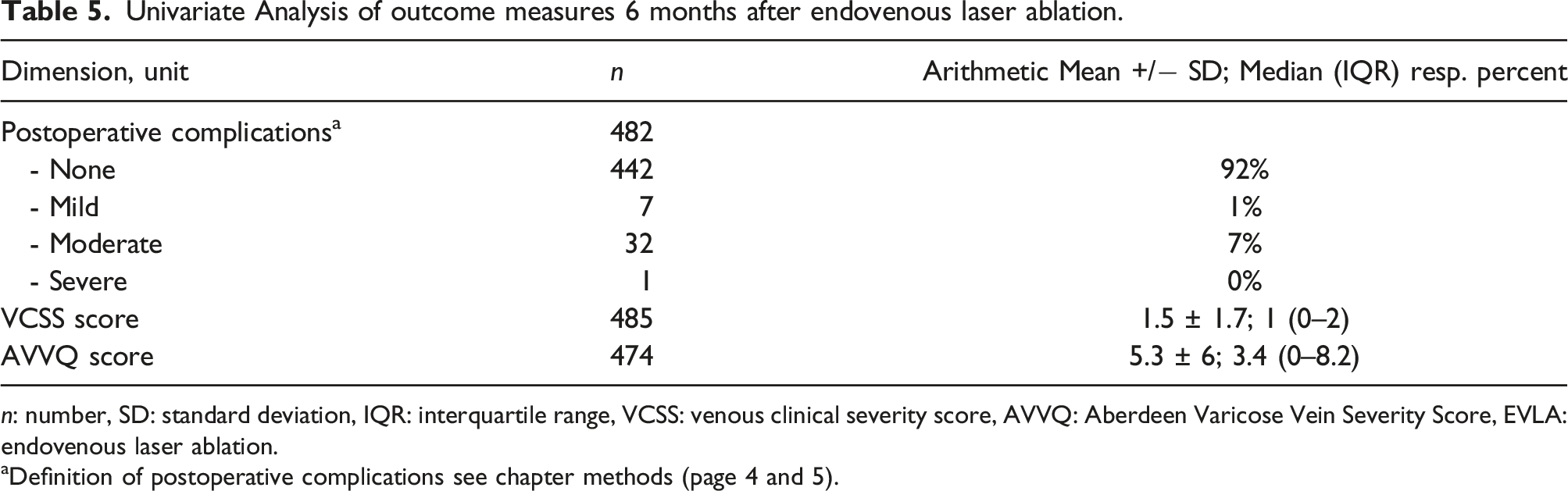
n: number, SD: standard deviation, IQR: interquartile range, VCSS: venous clinical severity score, AVVQ: Aberdeen Varicose Vein Severity Score, EVLA: endovenous laser ablation.
aDefinition of postoperative complications see chapter methods (page 4 and 5).
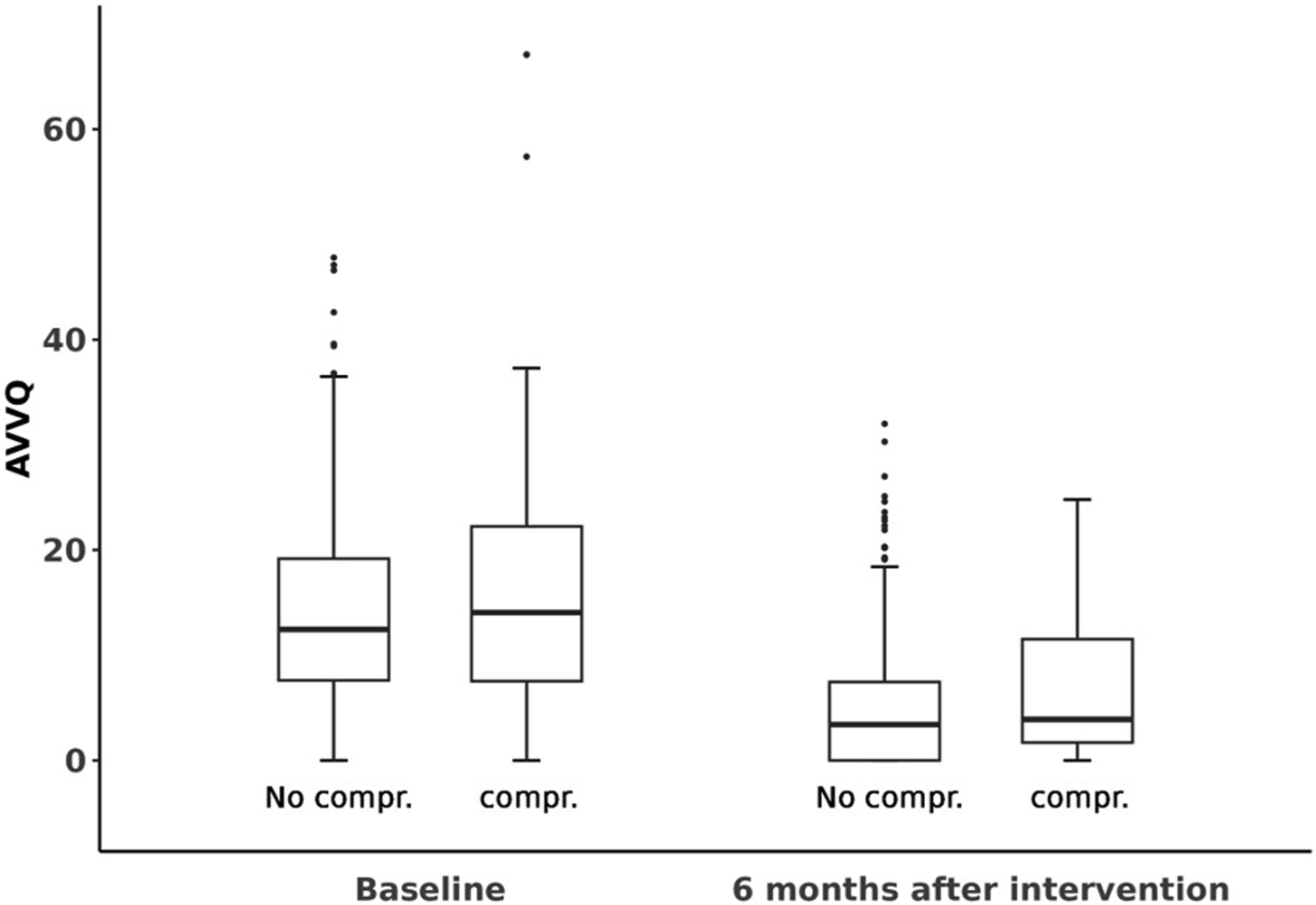
Quality of life measured with the Aberdeen Varicose Vein Questionnaire (AVVQ) 6 months post-intervention. The AVVQ score ranges from 0, indicating no effect on the patient’s quality of life from varicose veins to 100, indicating severely affected quality of life. The Boxplots indicate the distribution of the AVVQ score at baseline and 6 months after intervention of those patients receiving post-interventional compression and those who did not. The upper and lower bounds of boxes indicate the 25th and 75th percentiles while the median is indicated by the line intersection.
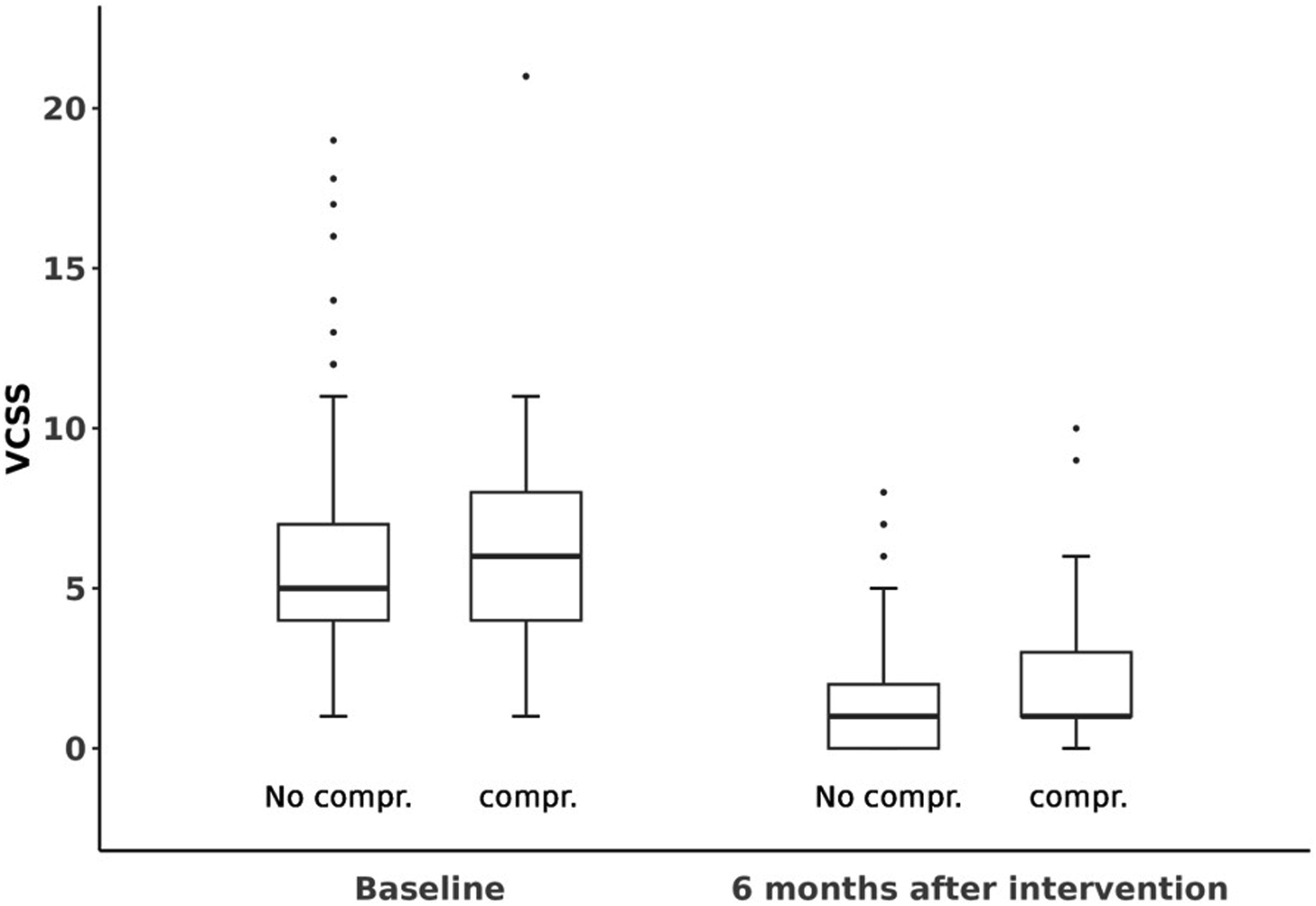
Patient-reported disease severity on the Venous Clinical Severity Score (VCSS) 6 months after intervention The VCSS scale ranges from 0, indicating low patient-reported disease severity to 30, indicating high disease severity. The Boxplots indicate the distribution of the VCSS score at baseline and 6 months after intervention of those patients receiving post-interventional compression and those who did not. The upper and lower bounds of boxes indicate the 25th and 75th percentiles while the median is indicated by the line intersection.
After 6 months, a group comparison of the cohort with post-interventional compression (n = 441) versus no post-interventional compression therapy (n = 49) was carried out. We observed that patients with compression therapy reported significantly fewer symptoms, for example, skin changes (pigmentation), inflammation, and induration, and ulcers (VCSS 1.4 ± 1.6) compared to patients without compression (VCSS 2.2 ± 2.2; p = .007; Mann-Whitney’s U test) (see Table 2). After 6 months, the AVVQ score showed no statistically significant difference (p = .097; Mann–Whitney’s U test) in a group comparison (with and without compression; see Table 2).
Furthermore, a subcategorization of compression duration into none (0 days, n = 49), short (1–14 days, n = 81), and long (>14 days, n = 360) was done and showed a significant difference between groups in both, the disease severity (VCSS) (p = .009) and the quality of life (AVVQ) (p = .015), after 6 months (see Table 3). The VCSS score in the short compression subgroup (n = 81; 1–14 days) was 1.3 ± 1.8 compared to 1.5 ± 1.6 in the long compression subgroup (n = 360; p = .005) indicating lesser disease severity in the short compression group. The quality of life (AVVQ) was also the best in the short compression group with a score of 4.1 ± 5.7 compared to 5.4 ± 5.9 (long compression), and 6.8 ± 6.7 (no compression; p = .015; Kruskal–Wallis test). Similarly, a short duration of compression was significantly superior to no compression regarding disease severity (VCSS) (p < .001) and quality of life (AVVQ) (p = .001; Mann–Whitney’s U test) at 6 months.
Patient satisfaction was reported as “very good” in 76% (n = 356) of cases, “good” in 20% (n = 94) of cases, “satisfactory” in 3% (n = 13) of cases, and “poor” in 1% (n = 3) of cases after 6 months. After 6 months, there were no significant differences between the cohort with and without post-interventional compression (p = .203) (see Table 2) and between groups using none, short, and long compression (p = .406) regarding patient satisfaction.
Compliance
The recommended duration of compression therapy was 19 (±13) days on average. The average actual performed compression duration was 25 ± 19 days. Overall, 82% (n = 398) of patients were considered “compliant” regarding the post-interventional compression, as they adhered to, or even exceeded the recommended compression duration. Age, gender, weight, side of localization, Hach stage (length of insufficient vein segment), clinical state according to the CEAP classification, VCSS baseline score, and AVVQ baseline score did not significantly affect patient compliance. However, patients with longer duration of pain were more likely to be compliant compared to patients that experienced less pain (p = .002).
Accordingly, patients who were non-compliant with recommended post-interventional compression therapy had significantly worse disease severity scores (VCSS) after EVLA (2.1 ± 2.3 vs 1.4 ± 1,5; p = .009). In contrast, no significant differences were found in the AVVQ score, patient satisfaction, and post-interventional complications between the two groups “compliant” and “non-compliant”.
Discussion
Chronic venous insufficiency is a common disorder, which affects up to 50% of the adult population in Western countries.1,2 Endovenous laser ablation (EVLA) of incompetent saphenous veins has been used successfully for many years with an excellent side effect profile.4–7 Post-procedural compression therapy has been hypothesized to reduce the risk of recurrence, pain intensity, leg edema, and improve physical function; however, its effectiveness and optimal duration are subject to an ongoing debate.9,10,13,23 This multicenter, controlled, prospective study investigated the effects of post-interventional compression therapy, the optimal therapy duration and predictors for compliance in 493 patients who underwent endovenous laser ablation (EVLA) for the treatment of great saphenous vein reflux. Compared to previous studies, this represents one of the largest cohorts reported to date.9,10 The analyzed patient population was representative of the general population in terms of age, gender, height, weight, BMI, and other factors.
First, we evaluated the impact of post-interventional compression on clinical outcome measures including the occlusion rate, complications, pain, patient satisfaction, quality of life (AVVQ score), and disease severity (VCSS score). In this multicenter cohort, an occlusion rate of 99% was achieved in all patients undergoing EVLA of the great saphenous vein. This finding is in agreement with previous studies reporting also very high success rates after EVLA.7,24 Accordingly, post-interventional compression therapy of various durations did not further improve the occlusion rate at 6 months post-intervention. In fact, patients with post-interventional compression therapy had a lower occlusion rate (99%) compared to patients who did not conduct compression therapy (100%). This could be attributed to the fact that patients with more pronounced findings or risk factors for therapy failure (e.g., obesity and anticoalition) were more likely to be recommended post-intervention compression therapy. Furthermore, the complications within the first 10 days and after 6 months were examined in the study. In our entire patient cohort, there were in general few complications, most of which were not serious. Within the first 10 days, 89% (n = 407) of the patients in the entire cohort reported no complications at all. The most common complications within the first days after EVLA in our patient cohort were hematoma (7%), hyperpigmentation (1%), and sensory disturbances (2%). At 6 months, 82% (n = 400) reported no current complications and 8% (n = 41) reported mild complications such as matting, pain, hematoma, ecchymosis, and hyperpigmentation. In this study, severe complications were defined as PATE Ill and IV and deep vein thrombosis. These adverse events occurred extremely rare with 1% (n = 3) within the first 10 days and 1% (n = 4) at 6 months after EVLA in our entire cohort. This is in accordance with other studies, also reporting that complications following EVLA are generally very rare. 25 Three of the total four severe complications have already occurred in the first 10 days after EVLA. To investigate the influence of compression on post-interventional complications, a comparison of the cohorts with and without post-interventional compression therapy was done. There was no significant difference between subjects with no compression versus subjects with compression in terms of post-interventional complications within the first 10 days (p = .764) and after 6 months (p = .194).
In addition, we examined if compression has an impact on post-interventional pain following EVLA. Comparing post-interventional pain 6 months after EVLA, there was no significant difference between patients performing compression and patients with no compression in our study cohort. Although not reaching significance in this study, patients with compression reported a slightly shorter pain interval compared to patients without post-interventional compression (1.6 ± 2.3 vs 2.1 ± 2.5 days). This is in agreement with previous findings, describing positive effects of post-interventional compression therapy on pain following EVLA. 10
In this study, some patients received additional procedures such as miniphlebectomy, liquid sclerotherapy, and foam sclerotherapy on the day of EVLA. Data analysis showed that patients who received an additional treatment were more likely to adhere to compression therapy compared to those without adjunct procedures. However, this observation could be partially attributable to a selection bias, since patients who underwent an additional procedure were also more likely to receive recommendations for compression therapy. Additionally, the uneven allocation of extra procedures across the groups (those receiving post-interventional compression vs those not) might have influenced the study’s outcomes. Notably, patients in the compression group underwent a higher number of additional treatments. Consequently, one might anticipate these patients to report more symptoms (as measured by the Venous Clinical Severity Score, VCSS), experience greater pain, and have a reduced quality of life (as assessed by the Aberdeen Varicose Vein Questionnaire, AVVQ) following the intervention. Contrary to expectations, our findings show that the compression group actually reported significantly fewer symptoms (VCSS) (p = .007) compared to the group without compression, despite undergoing more additional procedures. This suggests that the benefits of compression therapy may outweigh any negative impacts of undergoing additional procedures, underscoring the importance of including compression therapy as a standard part of post-interventional care.
The long-term efficacy of compression therapy after EVLA is still a matter of debate. 23 This is why the intention of this prospective, multicenter study was to investigate any long-lasting effect of compression therapy post-EVLA in addition to any potential short term relieve of symptoms. This is why a long-term follow-up has been included in the study protocol. We, as others, can only speculate on the underlying mechanism of action for any observed long-term effects of compression. Reduction of post-interventional fluid extravasation and associated edema formation with consequently less interstitial inflammation may be involved. 23 Alternatively, or additionally, gentle tactile stimulation has been shown to relieve pain in the same dermatome due to multimodal sensory neurons responding to both nociceptive and tactile inputs. 26 Tactile stimuli, for example, due to compression, may reduce the neurons response to nociceptive stimuli and thereby may contribute to pain relieve and prevent chronification. 26
In this multicenter cohort disease severity and quality of life was documented using the common questionnaires VCSS and the AVVQ. Hereby significant improvements in patient-reported disease severity (VCSS) and quality of life (AVVQ) following EVLA was observed. Although the between group differences in AVVQ scores observed in our study ranged below the traditionally recognized clinical important difference, one may argue that the recognized enhancement is clinically meaningful within this patient cohort. This perspective is reinforced by significant reductions in disease severity (VCSS score) and high patient satisfaction, indicating a positive impact from the patient’s perspective. The subgroup of patients that received compression therapy following EVLA reported significantly fewer symptoms in the VCSS score (1.4 ± 1.6) 6 months after intervention compared to patients with no compression (2.2 ± 2.2) (p = .007). This suggests that compression may help to reduce disease severity following EVLA. However, although a statistically significant difference has been found among groups for the VCSS, the clinical difference might be moderate and its clinical relevance can be debated. However, given the low cost and absence of relevant side effect of compression therapy one may argue that any significant improvement of the clinical outcome justifies this adjunct treatment. In addition, we found that a short compression duration (1–14 days) led to a significant improvement in clinical symptoms (VCSS) and quality of life (AVVQ) compared to no or long post-interventional compression. This may reflect patients with less severe conditions or complicative procedures that were recommended shorter compression periods. Further, we observed that patients who did not undergo compression at all had significantly more complaints (VCSS) compared to those who did, regardless of the duration of compression. This contrasts with previous studies reporting that compression therapy did not significantly impact quality of life or time to return to work. 10
Another objective of this study was to analyze compliance with the recommended post-interventional compression therapy in our cohort. This is important, as compliance is a key factor in the safety and success of medical treatment. In this study, patients who completed the recommended duration of compression, or longer were considered compliant. In the entire cohort, we observed a compression compliance rate of 82% among nine institutions. This is in accordance with previous studies reporting compliance rates of 87% and 94%, respectively.10,13
We found that age, gender, height, weight, severity (Hach, CEAP classification, diameter), VCSS at baseline, and AVVQ at baseline did not predict patient compliance. Even the recommended lengths of compression therapy did not affect patient compliance. We can only speculate as to why some patients were compliant and others were not. We are aware that outstanding compliance in selected patients could, in part, be an artifact of the study itself as patients may be more inclined to closely follow the instructions of their treating physician when observed in a study setting. However, patients with longer post-interventional pain tend to be more compliant with compression. Thus, we hypothesize that adverse symptoms post-intervention such as pain or discomfort are key drivers of patient compliance and may motivate patients to follow recommended compression protocols.
This study has several limitations, including a relatively short 6-months follow-up period, results only applicable to patients with great saphenous vein incompetence treated by EVLA, absence of blinding or randomization, and unequal group sizes in the subcategories of compression duration. In addition, we acknowledge the limitation of this retrospective evaluation including a recall bias as patients were asked for how many days they wore their stockings for only after 6 months. Another potential source of bias could be that there were no standardized instructions on discharge as this was based on the treating physicians’ preference due to our multicenter study design. Furthermore, the analyses are based on data from a subpopulation of the SYNCHRONOUS study. The statistical tests and the corresponding p-values are purely explorative and have no confirmatory value. However, strengths of this study include the multicenter, controlled, and prospective design and the large sample size including representative patients of nine institutions across Germany. In addition, information from the patient’s perspective was collected in the form of patient reported data, which gives the medical staff insights into the subjective state of health of a patient.
In conclusion, this study underscores the potential advantages of post-interventional compression therapy for patients, as it demonstrates a noteworthy reduction in symptoms and an improved quality of life. Additionally, patient adherence to compression therapy was found to be notably high, whereas those who deviated from the recommended treatment duration reported significantly greater disease severity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Guarantor
CMC.
Contributorship
CMC conceived the study, obtained ethical approval, managed the study supervision and participated in writing the manuscript. CD was involved in protocol development, data analysis and wrote the first draft of the manuscript. LU made the statistical analysis. All authors were involved in patient recruitment and data curation and contributed to the manuscript and approved the final version of the manuscript.