
Abstract
Introduction
Nowadays, incompetence of the great saphenous vein (GSV) is treated with minimally invasive endovenous thermal ablation (EVTA) techniques. EVTA has a low complications rate and can be performed without general anesthesia and thus, is recommended over open surgery of GSV high ligation and stripping (HLS). 1
Venous reflux elimination with HLS has been the gold standard treatment of varicose veins for many years. It should be noted that similarly to EVTA, HLS can be performed under tumescent anesthesia with ultrasound guidance. 2 Furthermore, EVTA and HLS do not differ in terms of clinical varicose vein recurrence or recurrent reflux detected by duplex ultrasound over the long term. 3
When you remove general anesthesia from the equation, EVTA and HLS should be compared based on complications rates and improved quality of life (QoL). Specifically, HLS has been associated with more bleeding and hematomas (4.8% vs. 1.3%), wound infections (1.9% vs. 0.3%), and paraesthesia (11.3% vs. 6.7%). 4 EVLA offers a faster postoperative recovery with a higher QoL than traditional high ligation and stripping procedures for varicose veins. 5
In the conventional approach of HLS the olive-shaped head that is mounted on the stripper can cause significant collateral trauma to the vein’s adjacent tissues, including nerves and lymphatics. Consequently, bleeding and hematoma may occur, also increasing the risk of surgical site infections (SSIs). On the other hand, it has been shown that an invaginated strip of the GSV may cause less trauma in the saphenous compartment and is associated with diminished blood loss and less discomfort compared to conventional stripping. 6
Lastly, there have been studies that question the necessity of high ligation and report that a more distal GSV stripping may produce similar, if not better results. 7 In essence, stripping without ligation of the saphenofemoral junction (SFJ) tributaries mimics the result of EVTA. Stripping may become a minimally invasive procedure if done distal to the SFJ, especially when standard endovascular techniques are used to facilitate the procedure and reduce the need for large incisions.
Based on the above, we present our technique of ambulatory EndoVenous-assisted Invaginated Stripping (EVIS) of the GSV and seek to explore uncertainties around the surgical intervention itself namely technical stability, delivery, safety and effectiveness by performing a pilot and feasibility study.
Methods
The is a prospective observational study that was approved by the Research Ethics Committee of the Hospital and was undertaken form December 2022 to September 2023. This study followed the reporting standards for STrengthening the Reporting of OBservational studies in Epidemiology (STROBE). Informed consent was obtained from all patients for participation in the study, analysis of their data, and publication of images and videos.
The inclusion criteria were primary chronic vein insufficiency of the GSV, greater than 18 years of age, and reflux of at least 0.5 seconds at the SFJ. Among the exclusion criteria were reflux at the anterior or posterior accessory saphenous veins, a body mass index of greater than 35, and prior treatment of the GSV in the same limb. The most severely affected leg was treated in patients with bilateral disease.
Based on the CEAP classification, the C component was used to assess the clinical stage. Preoperative duplex investigations, demographics, operative time, blood loss, technical success, and length of veins strapped were also recorded.
Blood loss due to vein stripping was considered the blood that accumulated in the subcutaneous upper-leg saphenous compartment. Weighed dry gauzes were used to absorb this blood as it was rolled out toward the groin. The bloody gauzes were weighed again, and the blood loss was calculated by subtracting the weight of the gauzes.
After the operation, patients were discharged home and told to resume normal activities immediately, as well as encouraged to walk regularly. A single dose of thromboprophylaxis with Low Molecular Weight Heparin (LMWH) was administered to all patients.
Patients reported their level of pain using a horizontal axis ranging from none (minimal, VAS = 0) to excruciating (maximum, VAS = 10). This was done immediately after the operation and at 48 hours, 1, 4, and 12 weeks. At one week, duplexes were performed to detect hematomas and Deep Venous Thrombosis (DVT), and at three months, the diameter of the residual stump was measured, and reflux was assessed to determine if it had transferred to the SFJ tributaries that have been left intact eg the anterior or posterior accessory saphenous veins.
To summarize the data, descriptive statistics were used, including mean as a measure of central tendency and range as a measure of variability. In the case of categorical variables, percentages were used.
Operative procedure
EVIS is performed as a day-case surgery as there is no need for general anesthesia or sedation. In addition to the preoperative hair removal, the patient receives a single dose of intravenous antimicrobial prophylaxis. Standard surgical drapes are applied after the skin has been prepared with chlorhexidine gluconate and alcohol solution.
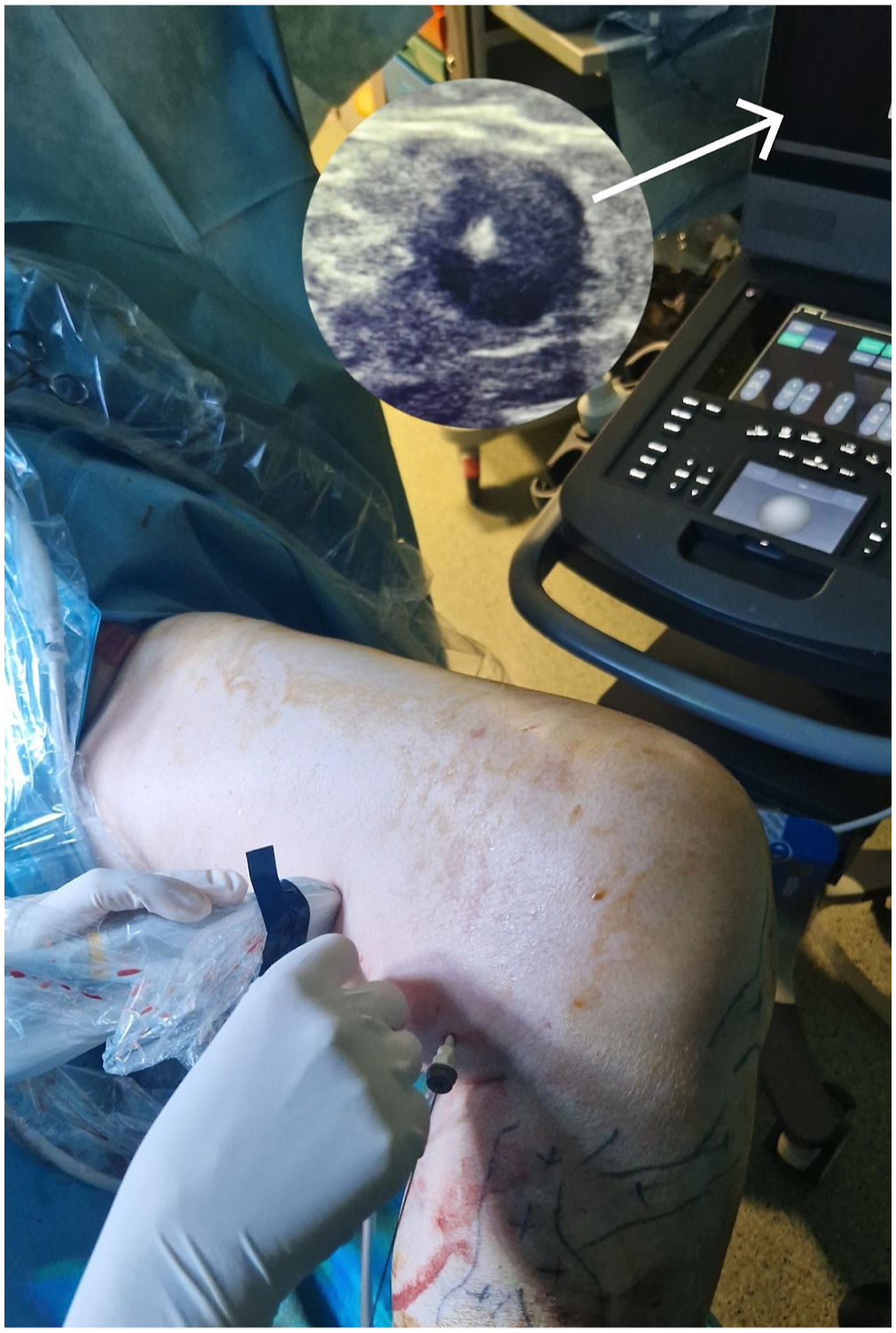
An anti-Trendelenburg position (head elevated by 15 degrees above the feet) is preferred for optimal visualization of the veins with ultrasound. In order to determine whether the GSV has tortuosity, aneurysms, or post-thrombotic changes, a duplex scan along its length is performed. The GSV is punctured under ultrasound guidance at the level of the knee with an 18-gauge needle, and a 5-F sheath is inserted into the vein (Image 1, Figure 1). A long 0.035″ PTFE-coated J-tip guidewire is then navigated across the GSV and through the SFJ to reach the common femoral vein (CFV). The position of the guidewire is secured and confirmed with ultrasound (Image 1). When there is tortuosity of the GSV or post-thrombotic stenoses that prevent easy navigation of the PTFE guidewire, a glide wire with hydrophilic coating may be used and then exchanged with the stiffer J-tip guidewire. Schematic drawing of the Endovenous-assisted Invaginated Stripping (EVIS) of the Great Saphenous Vein (GSV). 1: Percutaneous access at knee level. The guidewire is recovered at the groin and a braided thread is fixed at its tip. 2: The guidewire carrying the thread is retracted out of the access site. The sheath is removed. 3: Tying the thread on the GSV stump. 4: An epinephrine-soaked gauze pack is tied at the proximal end of the thread. 5: Traction of the distal end of the thread pulls down the packing within the saphenous vein, causing its invagination. Adapted from Perrin M. drawing.
17
Percutaneous access of the great saphenous vein (GSV) with a 5-F sheath at knee level. The position of the guidewire across the GSV is confirmed with ultrasound (arrow).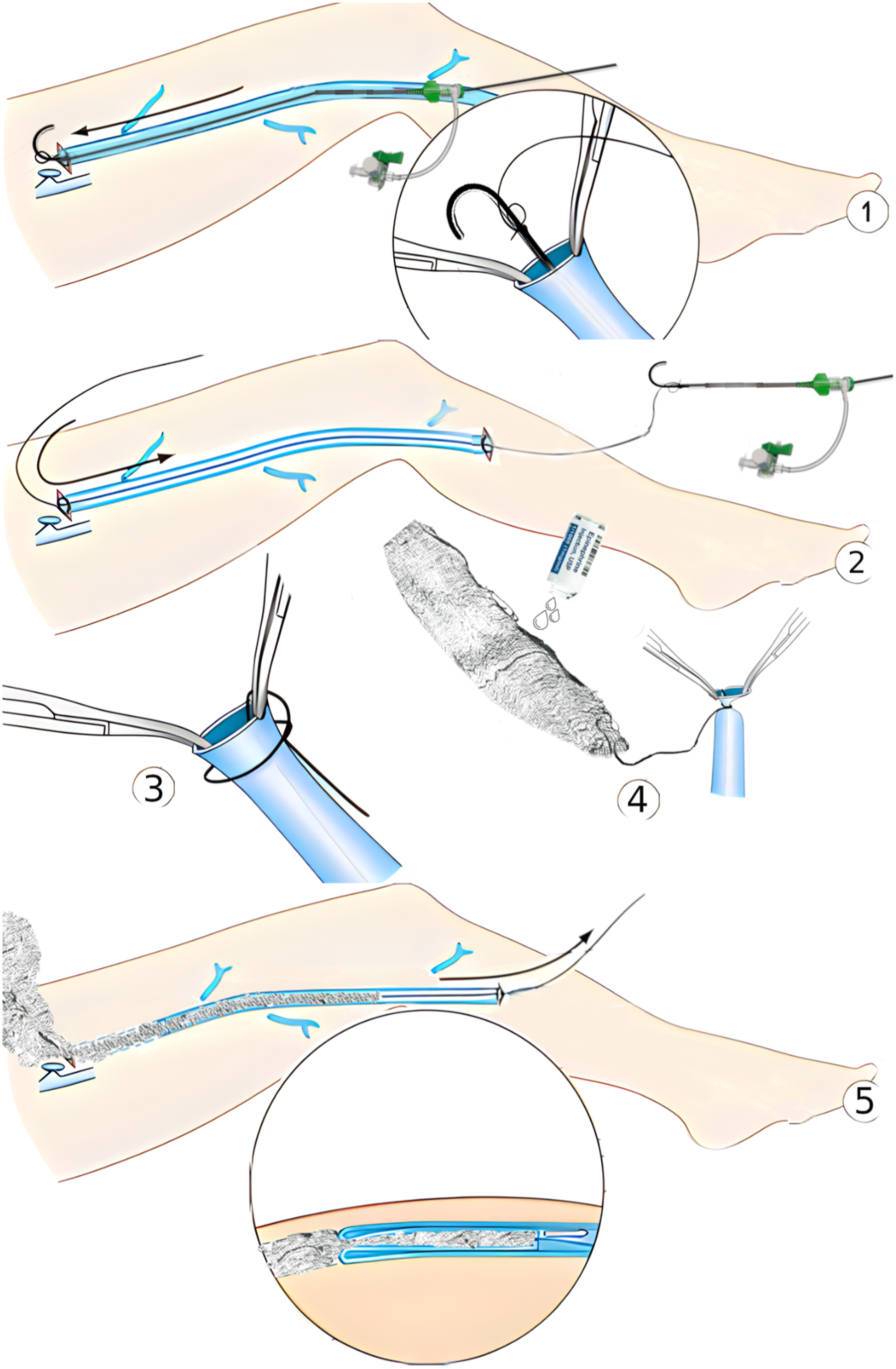
The saphenous compartment along the GSV is then infiltrated with tumescent anesthesia (50 mL of 1% lidocaine, 1 mL of epinephrine 1:1,000, and 12.5 mEq sodium bicarbonate diluted in 1 L of normal saline) from the knee to the groin under ultrasound guidance. There is no need to infiltrate the subcutaneous plane with tumescent anesthesia as normally done in EVTA where there is a risk of skin thermal injury.
The patient is then placed in the Trendelenburg position (head 15 degrees below the feet). A small 1 cm incision is done near the femoral crease. Ultrasound is used to mark the exact location of the incision. In the subcutaneous plane, the GSV carrying the stiff PTFE guidewire can be easily palpated. The vein is dissected free with a Lahey clamp and secured with a sling (Image 2). The PTFE guidewire is retracted distal to the sling and the GSV is ligated proximally. The ligation is tied about 1-2 cm below the inflow of the superficial inferior epigastric vein at the point where one would normally place the laser fiber tip when performing an EVTA. A small incision of 1 cm is made over the femoral crease. In the subcutaneous plane, the GSV carrying the stiff PTFE guidewire can be easily palpated. A Lahey clamp is used to dissect the vein (arrow).
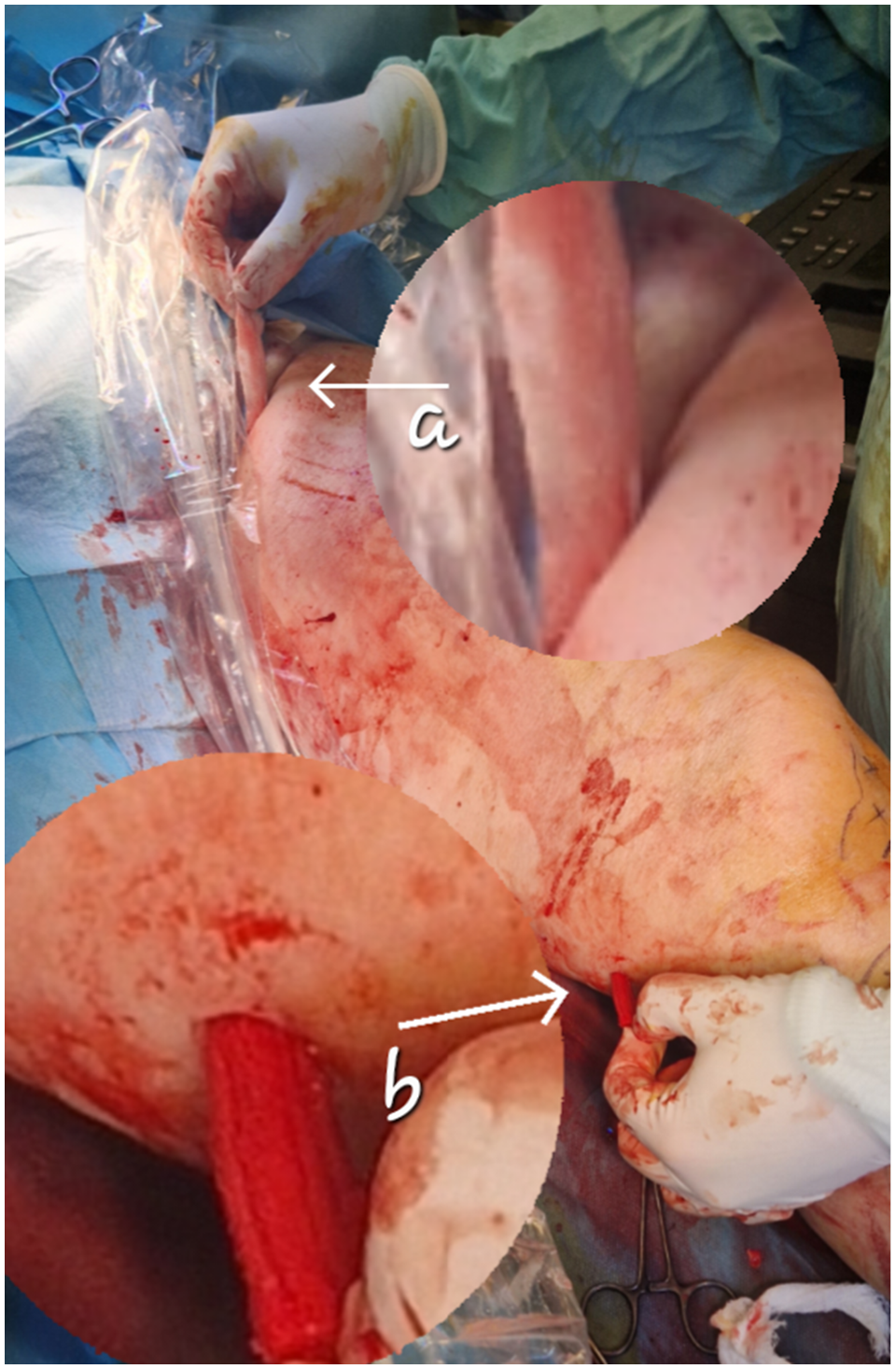
The PTFE guidewire tip is recovered from inside the GSV (Image 3). A strong braided thread of at least 70 cm in length, preferably Vicryl 2, is fixed to the guidewire tip (Image 3). The PTFE guidewire carrying the thread is then slowly retracted through the GSV and out of the percutaneous access site at knee level. At the proximal end, the thread is fixed on the GSV stump, in the groin (Figure 1). A further pull on the thread allows the vein to be invaginated and removed (Figure 1, Image 4, and Video). The guidewire tip is recovered from inside the GSV near the groin (arrow b). A strong braided thread is fixed to the guidewire tip (arrow a). Invaginated stripping of the Great Saphenous Vein (GSV) through the site of percutaneous access at knee level (arrow).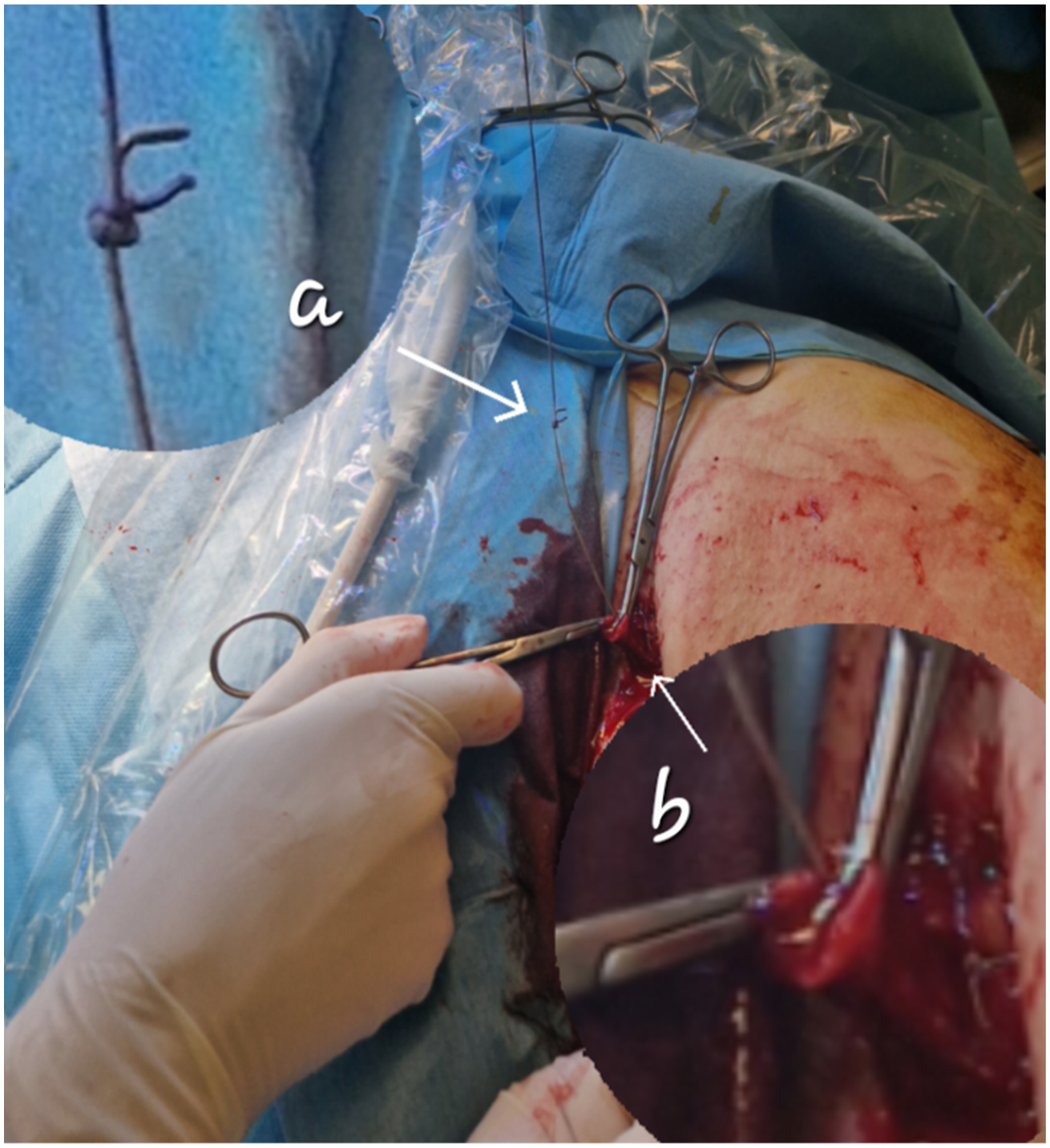
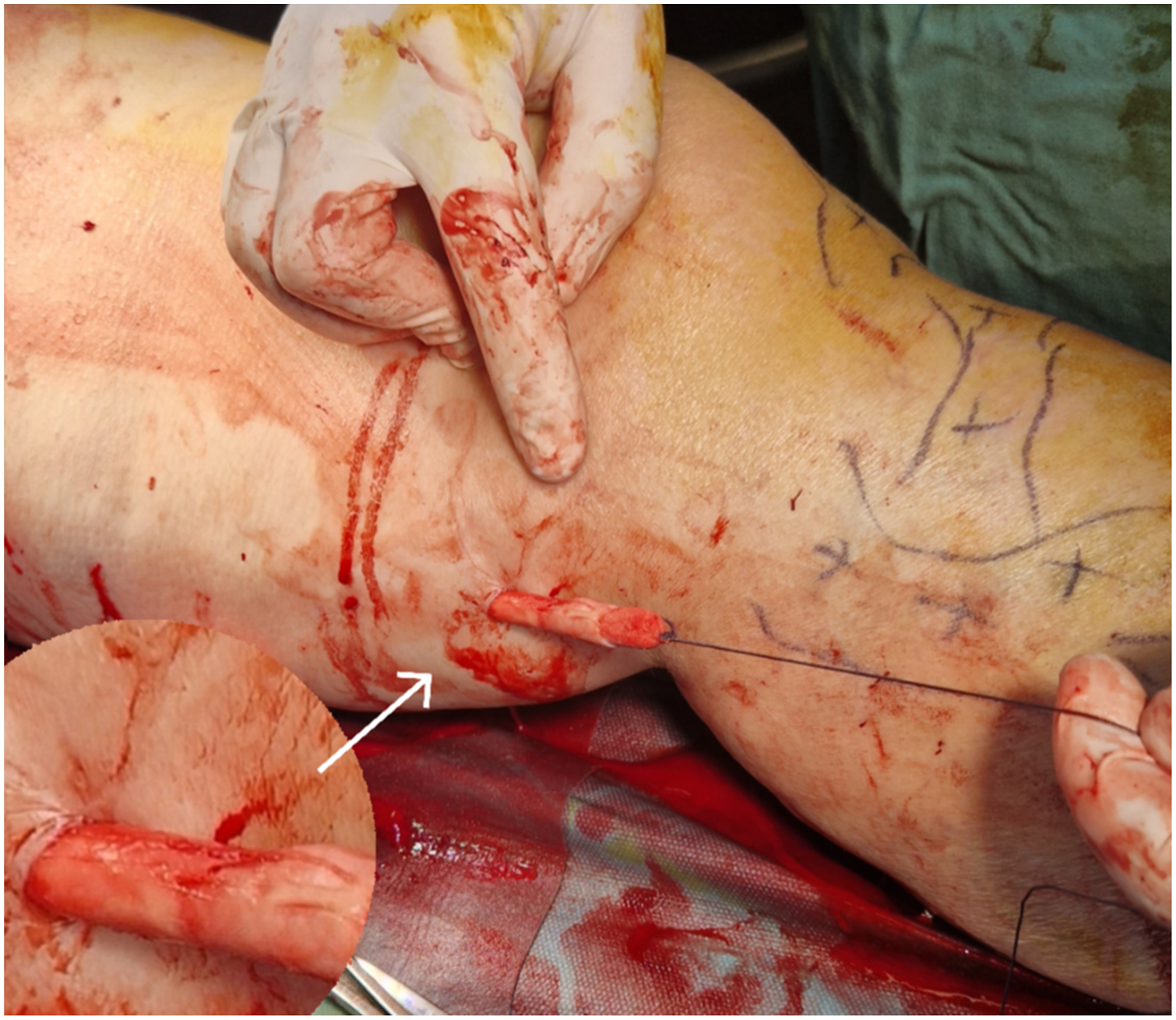
A useful addition to this technique is to allow the extra proximal length of the thread and tie down a 50 cm long gauze pack that has been socked with 2 mL of epinephrine 1:1,000 diluted in 20 mL of normal saline. Traction of the distal end of the thread, at the knee, pulls down the packing within the saphenous vein, causing its invagination. The GSV is turned outside-in over the packing as it comes out through the percutaneous access point at knee level (Image 4). This minimizes the risk of vein rupture (Image 5), and it also packs the saphenous compartment and aids in hemostasis (Image 6). The gauze is left in the saphenous compartment until all calf phlebectomies have been completed. The width of this gauze packing depends on the diameter of the saphenous vein. Pull down of the gauze packing within the GSV causes its invagination and at the same time minimizes the risk of vein rupture during stripping. The stripped vein is cut longitudinally to display the detail of the gauze pack invaginated in the GSV (arrow). The gauze packs the saphenous compartment and aids in hemostasis. The arrows point at the entry point (groin - arrow (a) and exit point (percutaneous access point at knee level - arrow (b) of the gauze.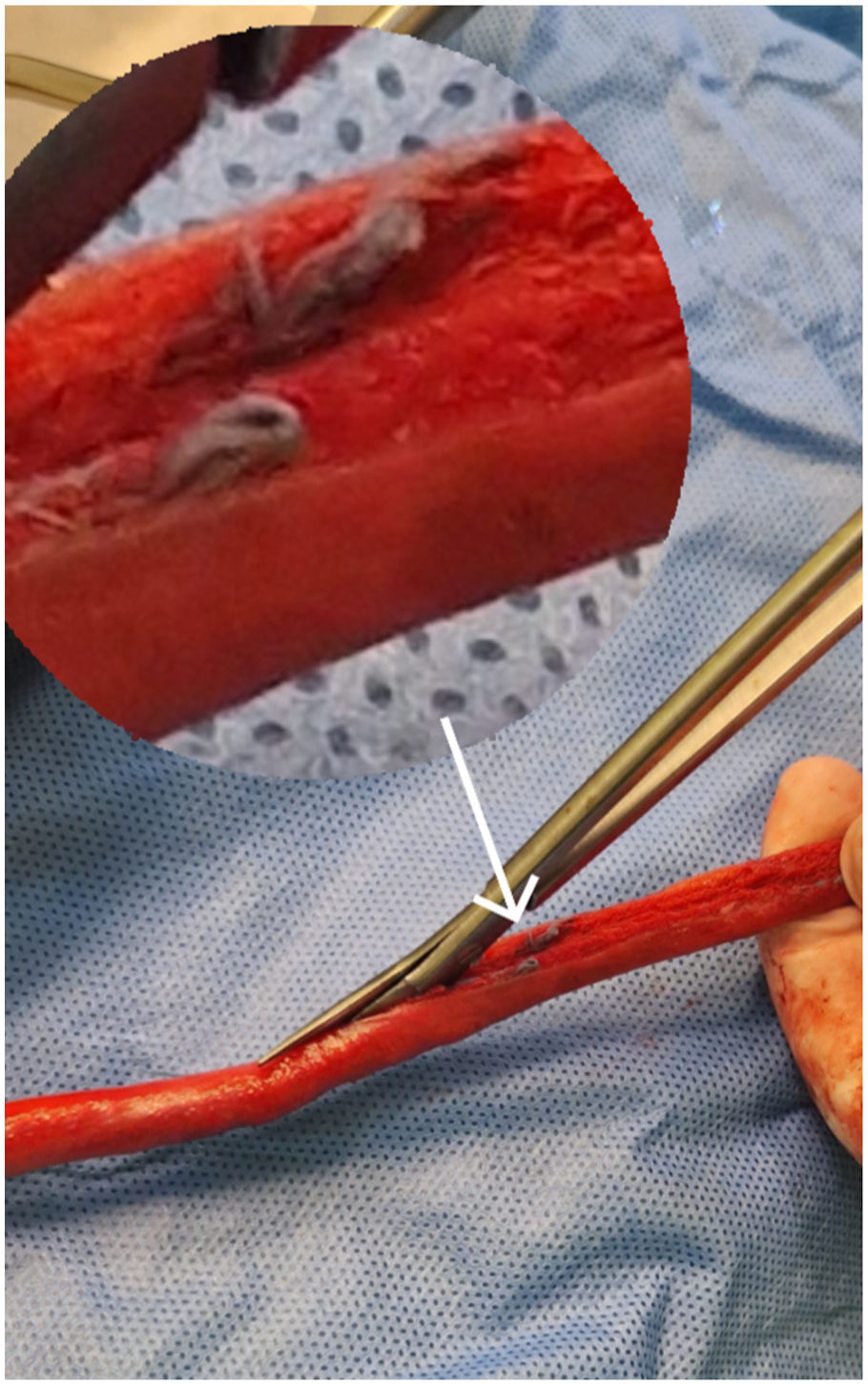
Incisions are closed according to the surgeon’s preference and the leg is dressed and compressed with thigh-level Class II stockings (25-32 mmHg).
Results
Twenty patients were operated with EVIS and followed up for three months. Fourteen (70%) of the 20 patients were female and the mean age of the sample was 47.9 years. Four patients (20%) had varicose veins without any complications (C2), 10 patients (50%) had varicose veins with oedema (C3) and 6 patients (30%) had skin changes (C4). Three patients did not attend the 4 weeks follow-up consultation and one did not attend the 7-day follow-up consultation, but all remained in the study for 3 months.
The mean operative time was 45 minutes (range 35-70 minutes). An intraoperative pain VAS of 4.8 (range 2-7) was recorded, and a postoperative pain VAS of 2.5, 1.8, 1.2, 0.5 at 48 hours, 1, 4 and 12 weeks, respectively. A mean blood loss of 15 mL was observed (range 5-50 mL) and the mean length of GSV strapped was 19 cm (range 14-27 cm). There were no complications such as deep vein thrombosis, surgical site infections, or nerve injuries.
At 1 week follow-up, the patients did not have any hematomas in the saphenous compartment and the only noticeable skin change was minor bruising of the thigh. The incision at the groin is really small and has a good cosmetic result (Image 7). (a) The incision at the groin is really small and has an excellent cosmetic result. (b) Minor bruising of the thigh without any significant haematoma at 1 week follow-up.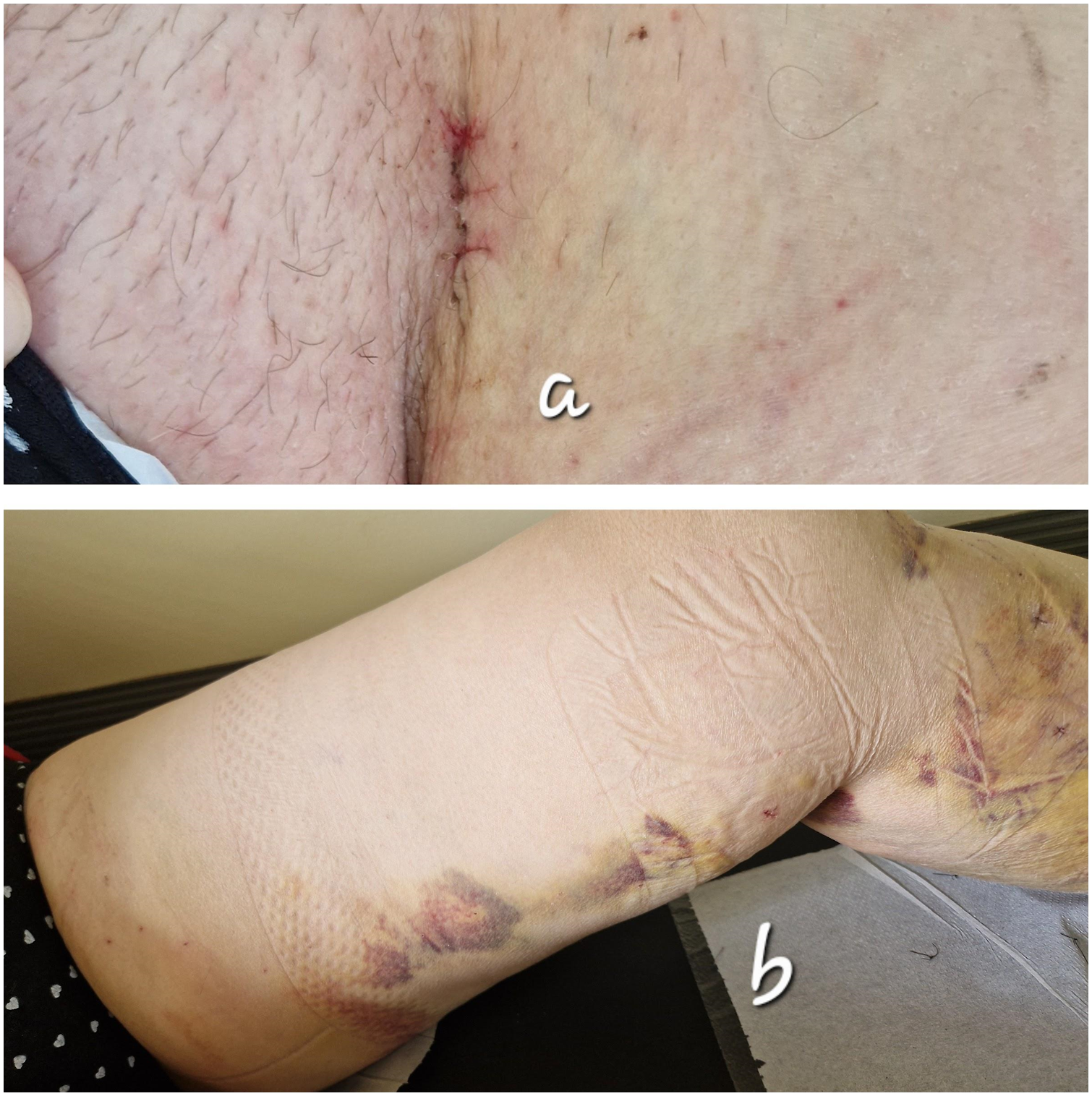
The GSV stump diameter retracted in all cases compared to the preoperative SFJ diameter at 3 months, and SFJ tributaries vein reflux was not detected.
Discussion
With a creative approach, we have tried to combine the ease and flexibility of endovascular techniques with the benefits of open surgery and get the best of both worlds. There are no revolutionary changes to what has already been described and done over decades of venous insufficiency surgery. However, EVIS may have some considerable advantages over standard HLS and EVTA.
By percutaneously accessing the GSV at knee level, we avoid the incision and tissue handling required to dissect the distal part of the GSV. Studies have shown that there is no need to ablate or strip the GSV below the level of the knee; the clinical results are similar, plus you avoid sural and saphenous nerve injury.8,9 No such complications occurred in our study.
Furthermore, endovascular techniques help tackle anatomic issues such as tortuosity and post-thrombotic stenoses. In the conventional approach of HLS, the surgeon may need to partially strip the GSV or proceed with additional incisions and cut-downs of the vein. Similarly, a laser fiber may not be able to navigate through post-thrombotic stenosis, aneurysm, or acute angulation of the vein and the GSV may need to be partially ablated or ablated in segments. This can be avoided in EVIS by using a vascular catheter and glide wire with a hydrophilic coating. One patient with post-thrombotic segment was managed with this approach in our cohort.
The anatomic result of saphenous stripping without ligation of the SFJ tributaries is comparable to that of EVTA. Similarly to a previous study, 10 our results indicate that the GSV stump diameter is reduced and reflux is not transferred to the SFJ tributary veins. Finally, placing a stiff guidewire across the GSV allows excellent visualization under ultrasound and makes dissection of the GSV possible through a “keyhole” incision at the groin. With less handling, there is less surgical trauma and hematoma, better cosmesis, and even fewer neovascularizations.
It has been well documented that most recurrences in HLS can be attributed to the neovascularization that occurs following surgical dissection of the SFJ. 11 The selective high ligation technique is to ligate the SFJ keeping some of the tributary veins. It has been shown that it decreases the incidence of neovascularizations and recurrent varicose veins in the operated groin. 12 In EVIS all SFJ tributaries are left intact and there is no dissection of the SFJ. The GSV is ligated and cut at about 1-2 cm below the inflow of the inferior epigastric vein at the point where one would normally place the laser fiber tip when performing an EVTA. Based on the above evidence, we can advocate that neovascularization recurrences might be limited in EVIS. It will be necessary to follow up for a longer period of time to prove this.
Furthermore, when the tributaries are kept open to blood flow, the venous reflux from the groin is reduced and there is no thrombosis of the GSV stump. 12 Thus, in theory, thrombus propagating from the GSV stump to the CFV might be less likely in EVIS compared to HLS. In EVTA, endothermal heat-induced thrombosis (EHIT) is a recognized complication that has controversial clinical significance. 13 EHIT is a thrombus that develops at the SFJ after EVTA. EHIT thrombus results from thermomechanical damage and coagulation effects. 14 DVT may develop in 0.3% and Pulmonary Embolism (PE) in 0.1% of patients treated with EVTA. 15 The rates of DVT and PE are similar in HLS but these numbers refer to operations done under general or spinal anesthesia. The risk for DVT is significantly lower in ambulatory procedures. We did not observe DVT or stump thrombus in our small cohort.
“Modern” stripping does not require general anesthesia. This strategy has not been followed in most RCTs comparing open surgery with endovenous techniques. However, there are studies that have shown that stripping can be safely done without any sedation.3,16 EVIS under tumescent has been really well tolerated by the limited number of patients that we have operated on. All patients managed to ambulate immediately following the procedure and were discharged home on the same day. The pain scores reported by patients included in this study are similar to what has been published for EVTA.
EVIS aims to transform GSV stripping into a minimally invasive procedure by incorporating an endovascular component. It is significantly cheaper compared to EVTA and even HLS. There is no cost for a fiber, stripper, general anesthesia, and hospitalization. The vasc ular sheaths and guidewires are cheap and readily available in all vascular surgery units. The described procedure may also be performed in a clean room, depending on the policy of the hospital or health system. The cost of a vascular sheath in our hospital is approximately 20 euros. When the anatomy is straight, the included starter J wire is enough in most cases. Finally, due to its minimally invasive nature, EVIS may offer faster recovery and improved QoL similar to EVLA. This is a poor man’s technique that may provide at least non-inferior results.
The main limitation of EVIS is that a diseased and degenerative GSV may rupture during stripping. However, with invagination, GSV is turned outside-in and the vein wall is significantly reinforced. The vein invagination starts from the proximal part where the GSV is thicker and stronger. Additional strength is achieved by pulling down a gauze pack within the invaginated vein. In our small cohort, there ware no cases of vein rupture. Furthermore, there is some bleeding in the saphenous canal from tributaries and perforators to the deep venous system. We try to limit this by packing the space with epinephrine-soaked gauze. However, bruising will certainly develop and patient satisfaction may be less compared to EVTA. Finally, it should be noted that we have applied EVIS to a limited number of selected patients and no safe conclusions can be drawn regarding outcomes and complications.
To conclude, this is the first technical report and cohort study of the Ambulatory Endovenous-assisted Invaginated Stripping of the GSV. EVIS is a smart and cheap combination of standard vascular and endovascular techniques that may prove valuable in managing patients with chronic venous insufficiency. It is an ambulatory minimally invasive procedure that revisits the way saphenous vein stripping can be done in the modern era. EVIS clinical outcomes and complications need to be further studied and directly compared with EVTA in a clinical trial.
Supplemental Material
Supplemental Material - EndoVenous-assisted invaginated stripping of the great saphenous vein: A pilot and feasibility study
Supplemental Material for EndoVenous-assisted invaginated stripping of the great saphenous vein: A pilot and feasibility study by Vangelis G. Alexiou, Areti Vassiliou, Michail Mitsis and Michail Peroulis in Phlebology.
Footnotes
Author contributors
VGA and AV have conceived the study, have recruited the patents, performed surgery, analysed data, and drafted the manuscript. MM and MP have contributed to the conception or design of the work. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Guarantor
VGA.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.