
Abstract
Objectives
An open label, single-centric, post market clinical study was undertaken to evaluate the safety and efficacy of a new antimicrobial wound dressing (VELVERT) as an adjuvant therapy in the treatment of venous leg ulcer (VLU).
Methods
Patients with VLU of grade C-5 according to CEAP classification and above were evaluated using doppler ultra sound. The efficacy of new antimicrobial wound dressing (VELVERT) was assessed in terms of wound area reduction within a time frame of 60 days and surgeon questioners. Patients were evaluated for VELVERT safety and pain level on a scale of 0-10 Numeric Pain Chart. Presence of micro-organism load was monitored at regular time interval.
Results
VELVERT treatment was effective as 71.43% reduction in the ulcer area was observed. After 60 days, a total of 9 (45%) patients had complete ulcer closure. A remarkable decrease in the severity of pain was observed with 11 (55%) patients expressing no pain at the EOT. Swab test showed negative result for micro-organism growth. No serious adverse events were observed during the trial.
Conclusion
The data indicates that VELVERT is an effective treatment for VLUs and showed the potential in the wound care of VLUs.
Introduction
VLUs, an open lesion between the knee and ankle, are late manifestations of venous hypertension and chronic venous insufficiency (CVI).1,2 According to CEAP classification chronic venous disease (CVD) is a progressive disease and divided into different stages based on increasing severity of the symptoms.3,4 The initial stages (C1-C2) of CVD are asymptomatic, however later stages (classes C3 and above) are designated as chronic venous insufficiency. CVD results in varicose veins with or without edema and leg ulcers in up to 5% of population
5
at later stages of disease progression. The pathogenesis of VLUs is divided into reflux and obstruction [insert Figure 1]. Venous reflux results from the valve incompetence, inflammation, venous hypertension and hemodynamic factors. VLUs in immobile subjects or patients with stiff joints can be further aggravated by abnormal functioning of muscles and vascular pumps. Venous valves are designed to maintain the circulatory flow of blood and lymph and their dysfunctionality can results in a fluid retention in the lower limbs and consequently oedema. Changes in hemodynamic parameters and venous hypertension induces the release of vasoactive substances and activation of immune system. The noxious soup of inflammatory mediators, immune cells infiltration, and increased collagen expression in the vessel walls is associated with chronic venous disease and ultimately leads to development of leg ulcers.
3
On the other hand, obstruction of the vessels due to thrombosis impede with natural blood flow. Obstruction alone or together with venous reflux results in VLUs and is a debilitating problem associated with significant financial cost. Pathophysiology and CEAP classification of CVD. Venous leg ulcer is a complication of chronic venous insufficiency.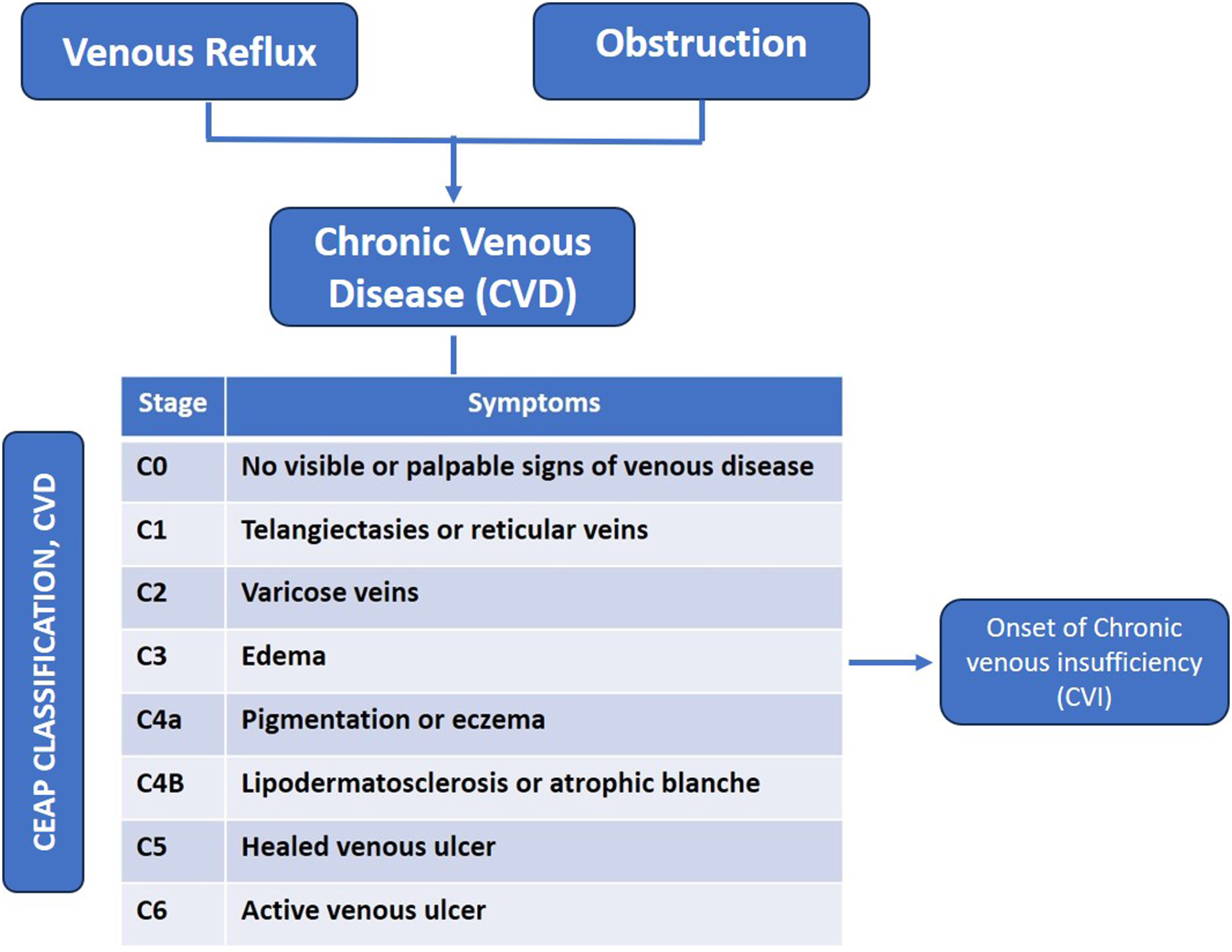
Effective management of wound exudate while treating hard-to-heal VLUs is crucial as heavy exudate from wounds can cause distress in the patients and can negatively impact the patient’s quality of life. Maintaining moist environment at the site of wound is crucial, however excess moisture can cause maceration of the surrounding skin. 6 Exudate accumulation within dressings might predispose the wounds to infection. 7 In addition, chronic wound exudates contain high levels of inflammatory mediators, which extends the inflammatory phase of normal healing. 8 A comprehensive management of VLU is thus required to reduce the need for prolonged medical care, which should include wound assessment, exudate management, pain assessment and infection control.
The aim of the present study was to assess the safety and efficacy of a new antimicrobial wound dressing (VELVERT) as an adjuvant therapy in the treatment of VLUs. VELVERT is a patented herbal anti-microbial barrier dressing. The polymeric sponge and formulation used in VELVERT is biocompatible, non-toxic and is therefore safe for human use. In addition to working as an antimicrobial barrier, as a result of its porous structure the dressing can absorb up to 20 times its own weight in fluid and thus can manage exudate efficiently. This may reduce the chance of further infection and also aids in faster wound closure and wound healing. The antimicrobial formulation act by reducing microbial load at application site. VELVERT is highly flexible and can conform to various wound shapes and sizes.
The primary objectives of the current study are: (1) To assess the efficacy of antimicrobial wound dressing (VELVERT) as an adjuvant therapy in the treatment of VLU in terms of reduction in wound area (pre and post dressing) and surgeon questioners, (2) Assessment of safety by monitoring adverse events and incidences. The secondary objectives included: (1) To assess the microbial growth at the site of ulcers, and (2) Assessment of VELVERT efficacy based on reduction in subject’s pain levels.
Material and method
Study type and patients
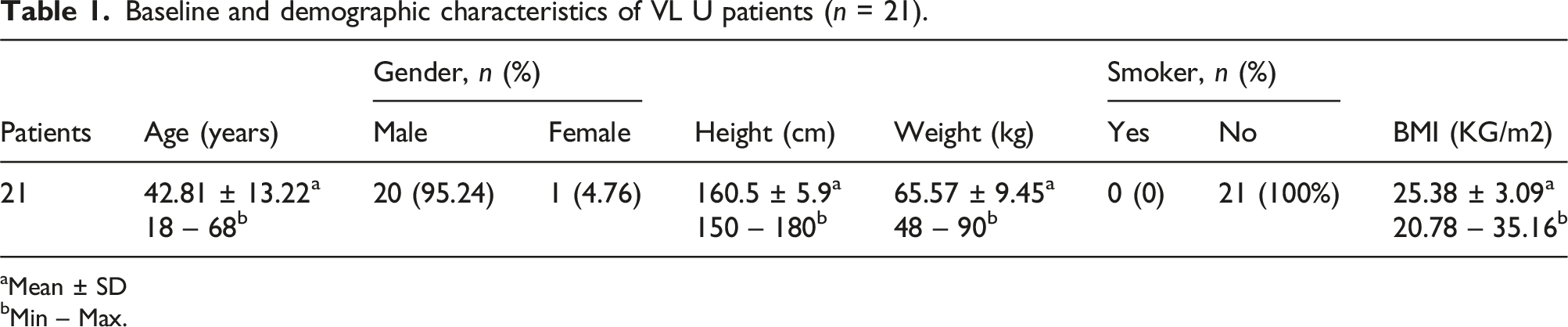
This study was an open label, single center, single arm, post market surveillance study. After evaluating the eligibility criteria, 22 patients were enrolled in the study after getting a signed written consent [insert Figure 2]. A unique ID was allotted to all the study subjects to maintain identity confidential. Patients were also assessed for any medical history or prior surgical procedure that can interfere with physiology of the ulcers and can affect the results of the trial. Blood samples were collected for the laboratory tests of Hematology, Blood Group, Biochemistry (FBS, HbAlc, LFT, KFT) and Serology as a part of screening procedure. Vital examination was performed at every visit. Concomitant medications and assessment for any infection was also monitored. Doppler test was performed to measure blood flow in the leg veins at the screening and last follow-up visit. Photographs of the wound and its measurement was performed on every dressing change. Principal investigator and senior resident doctors were trained by manufacturer for the steps involved in the “application of dressing” before initiation of the trial during site initiation visit. The maximum duration of each participant in the current study was 60 days after first dressing application including all visits. All potential patients with VLUs of both genders between 18 and 70 years of age, and patients of all socio-economic status were enrolled in the study. Subjects enrolled in the trial fall in C6 of the CEAP classification [ insert Figure 1]. If subject have more than one VLU, then largest ulcer meeting criteria shall be considered for the study and only one wound will be considered. Demographic characteristics of the study participants are defined in Table 1. Subjects were enrolled in the study when they met inclusion criteria and none of the exclusion criteria (Supplemental Table 1). The rights, safety and well-being of the participants was the priority during the trial. Flowchart of the study. Baseline and demographic characteristics of VL U patients (n = 21). aMean ± SD bMin – Max.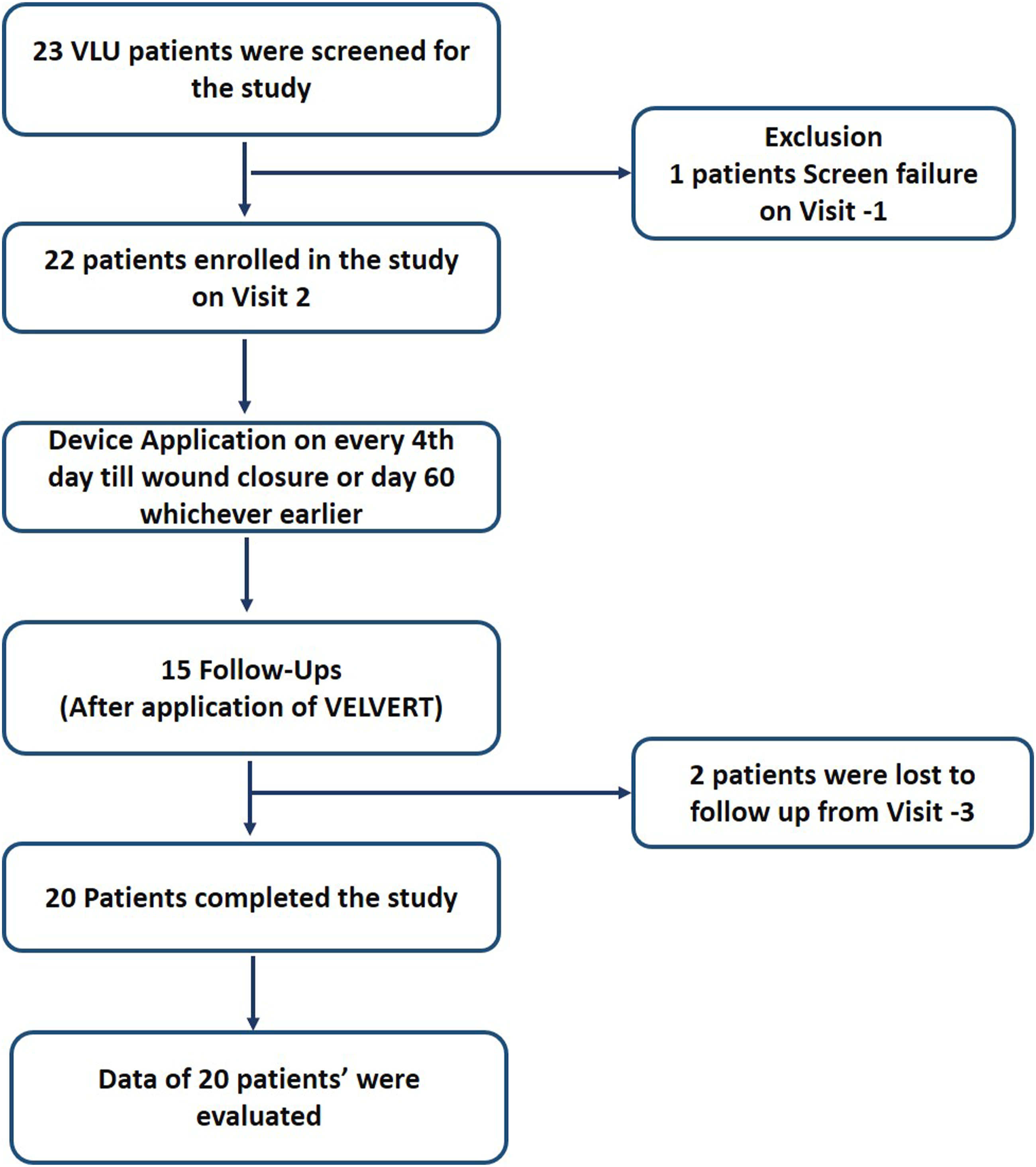
Outcomes measures
The study period involved a total of 16 visits after screening and VELVERT was changed every 4th day by trained principal investigator or senior resident doctors. Wound size assessment was done following every dressing change using a disposable paper ruler. Wound area was calculated by multiplying the longest length with greatest width. As, our aim was to assess wound healing without affecting the physiology of wounds with another intervention, no compression therapy or endovenous ablation therapy 9 was given during the trial. AEs and SAEs were summarized by counting both the number of events and the number of subjects experiencing events that occurred during the study period. MedDRA is used to classify adverse event, per system organ class and preferred term. Furthermore, adverse events were stratified according to the seriousness, severity, and relationship to the medical device used.
Bacterial load assessment was carried out using swab test before the application of the dressing (Day 0), on visit 6 (Day 16), visit 10 (Day 32) and last visit. Pain relief was evaluated at regular interval using a 0-10 Numeric Pain Chart, with the numerical scale ranging from 0 (indicating no pain) to 10 (representing the worst pain imaginable). On last visit, doppler test was performed to measure blood flow in the leg veins.
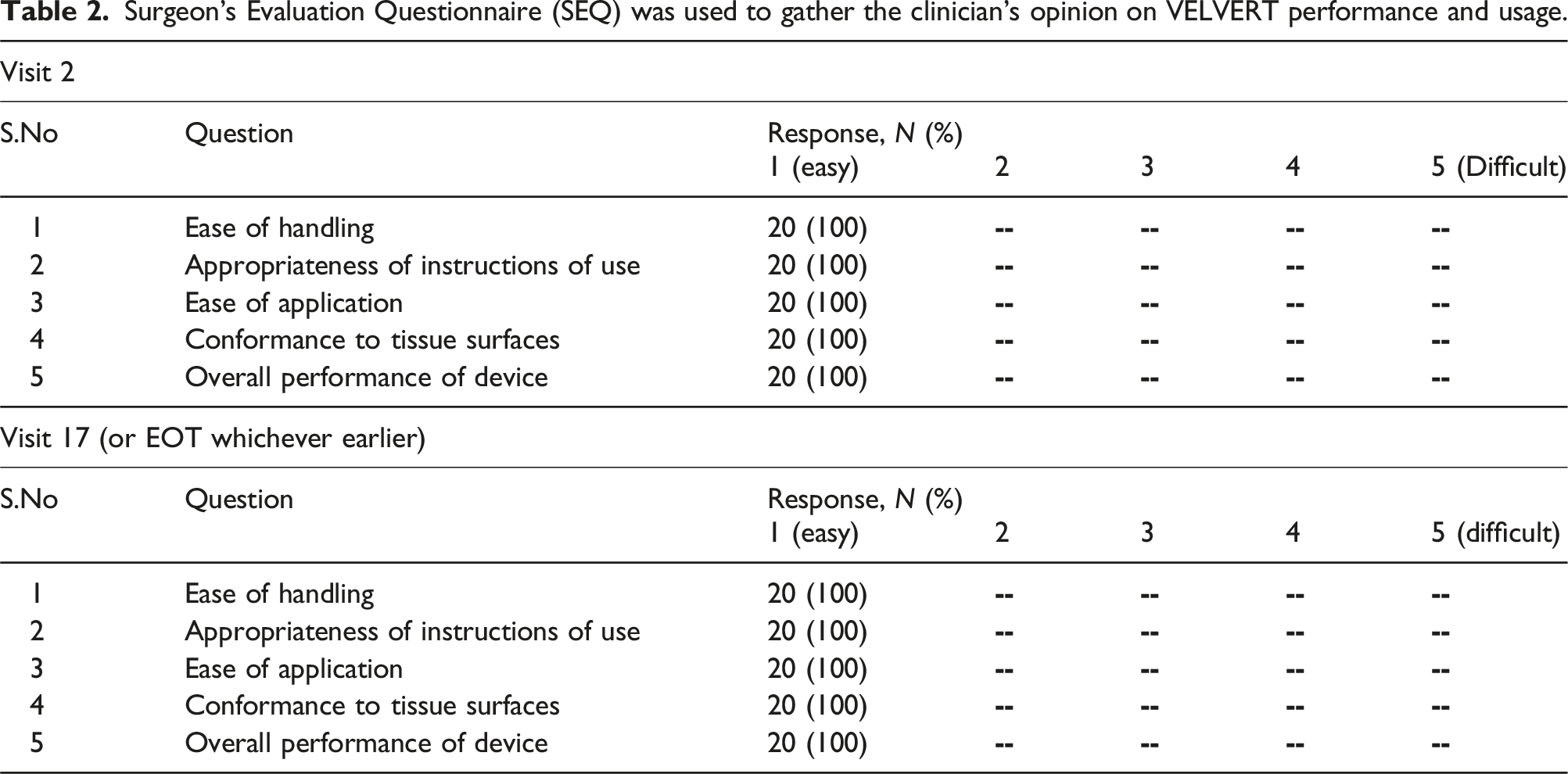
Surgeon’s Evaluation Questionnaire (SEQ) was used to gather the clinician’s opinion on VELVERT performance and usage.
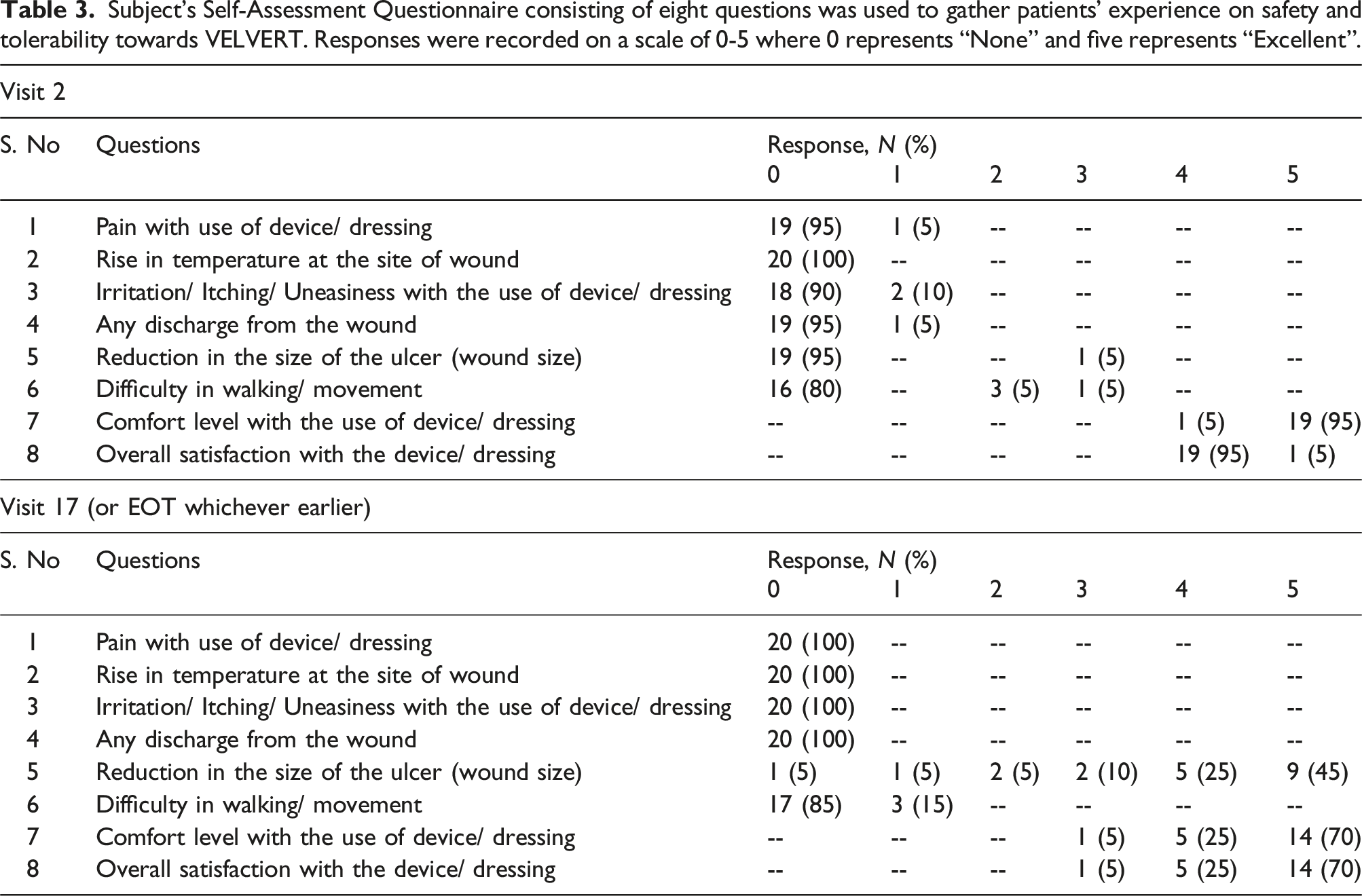
Subject’s Self-Assessment Questionnaire consisting of eight questions was used to gather patients’ experience on safety and tolerability towards VELVERT. Responses were recorded on a scale of 0-5 where 0 represents “None” and five represents “Excellent”.
Ethical approval
Patients were enrolled in the study following the receipt of ethical approval from the institutional ethics committee approval letter; 3797/EC/S.C-1/2023, dated 19-Sep-2023, MLB medical college Jhansi Uttar Pradesh, India) and CTRI registration CTRI/2023/10/058211. Subject confidentiality was maintained throughout the study while obtaining data. The study was conducted after meeting all the local ethical requirements and was in accordance with International Conference on Harmonization Guideline-Good Clinical Practice (ICH-GCP), the Declaration of Helsinki, ISO 14155:2020 and applicable regulatory requirements.
Statistical analysis
All statistical tests were performed using MS Excel. Between group p-values are based on two-sample t test. The results are presented in frequencies, percentage and Mean ± SD
Results
A total of 22 patients aged between 18 and 70 years were enrolled in study. Out of 23 screened patients, data of only 20 were assessed, as two patient’s follow-ups were lost (at visit 3), and one was excluded due to screen failure [insert Figure 2]. No patient had any prior medical history which could interfere with clinical evaluation or interpretation of results. Vital signs were monitored at every visit in terms of hemodynamic parameters and respiratory rate, no major changes were observed in these parameters.
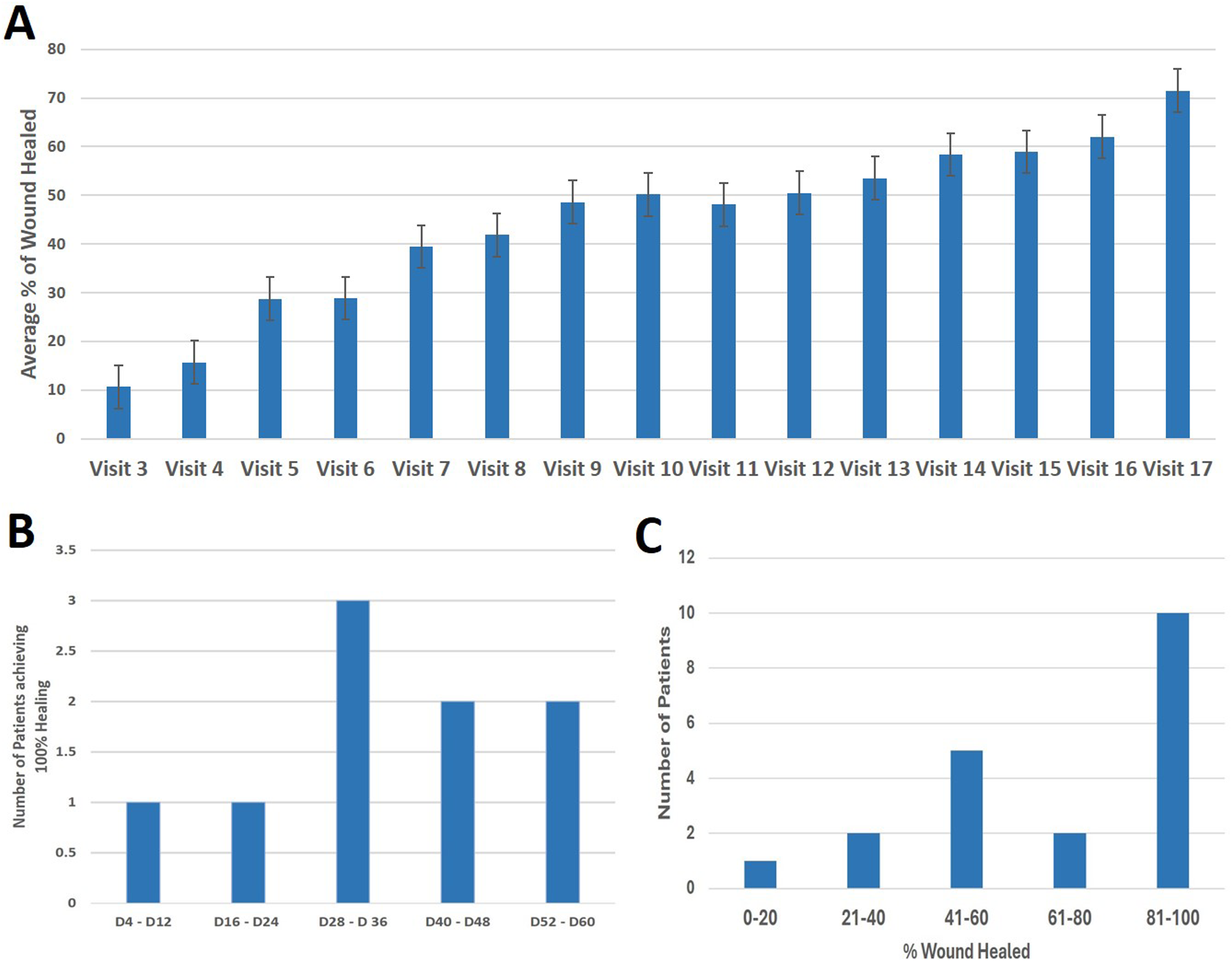
The main clinical outcomes of interest were wound area reduction within a time frame of 60 days in comparison to initial area and number of adverse events and wound complications due to dressing material or other cause. Another primary outcome was the overall performance of the product was evaluated in terms of ease of handling and application, and conformance to the tissues. A positive trend towards healing was observed at each visit following VELVERT application [insert Figure 3] with an average of 71.43% wound healing at the end of the treatment (EOT) [insert Figure 4]. At EOT (Day 60 or before), wound was completely closed in nine patients [insert Figure 4], 80-90 % wound closure was observed in 1 (5%) patient, more than 60-70 % wound closure was observed in 2 (10 %) patients, 50%–60% wound closure was observed in 1 (5%) patient, 40%–50% wound closure was observed in 4 (20%) patients, 30-40 % wound closure was observed in 2 (10 %) patients and 10%–20% wound closure was observed in 1 (5%) of the patient. Surgeon’s Evaluation Questionnaire (SEQ) and Subject’s Self-Assessment Questionnaire (SSAQ) was used to evaluate the data on various characteristics related to the performance and, user and patients’ experience of VELVERT dressing. SEQ included five different questions and SSAQ included eight questions (Tables 2 and 3). For each question in SEQ, rating was done on a scale of 1-5 where one represents “Easy” and five represents “Difficult”. For questions in SSAQ, rating was done on a scale of 0-5 where 0 represents “None” and five represents “Excellent”. SEQ data indicates a consistently positive user experience, with users finding the device easy to handle, appropriate in terms of instructions, easy to apply, and effective in conforming to tissue surfaces at different visit (Table 2). Safety, tolerability, and performance evaluated using SSAQ showed positive responses by patients (Table 3). No increment in pain or rise in temperature was observed with the usage of bandage. No irritation, itching, uneasiness and/ or discharge was observed. Patient found the dressing comfortable and less hindrance in walking. In the present study, two non-serious adverse events (vomiting and lower back ache) of mild intensity were observed. Venous leg ulcer images of the patients’ at the enrollment day (a) and at the end of the treatment (b). Rate of wound healing measured by % of wound that had healed visit-by-visit following first and subsequent applications of the VELVERT (a), number of patients showing 100% wound healing at the end of the treatment (EOT) (b) and number of patients falling in varying range of % of wound healing at the EOT (c). Data is represented as mean ± S.E.M., N = 20. D = Day.
Secondary outcomes were patient comfort in terms of pain reduction and assessment of micro-organism load. The efficacy of VELVERT was assessed based on the reduction in subjects’ pain levels at every visit. Patients were evaluated on a scale of 0- 10 Numeric Pain Chart with rating 1-3 showing mild pain, 4-6 moderate pain, 7-10 severe pain and 0 represents no pain. Pain alleviation to mild or no pain was achieved in 75% of patients following four applications of VELVERT dressing (data not shown). A comparison between pain level at the application of the device and at the last visit showed a remarkable change in the pain level with 11 patients (55%) experiencing no pain at last visit [insert Figure 5]. At the last visit, no patients reported severe pain and only one patient (5%) reported moderate pain [insert Figure 5]. Swab samples taken showed negative results for micro-organisms growth throughout the study. Pain intensity was measured on a scale of 0- 10 Numeric Pain Chart with rating 1-3 showing mild pain, 4-6 moderate pain, 7-10 severe pain and 0 represents no pain. A significant increase was observed in the patients expressing no pain and no patient showed severe pain at the end of the treatment.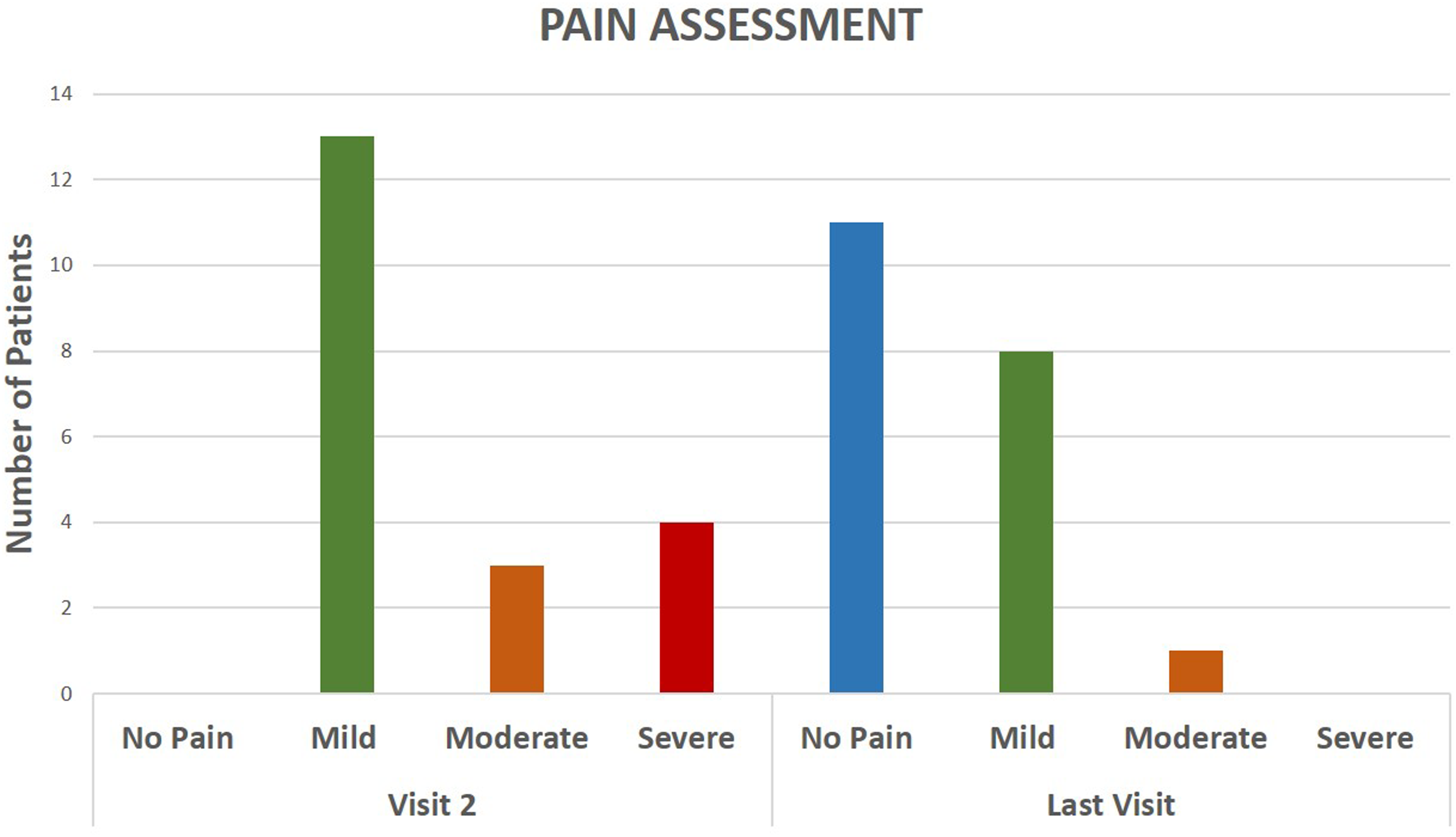
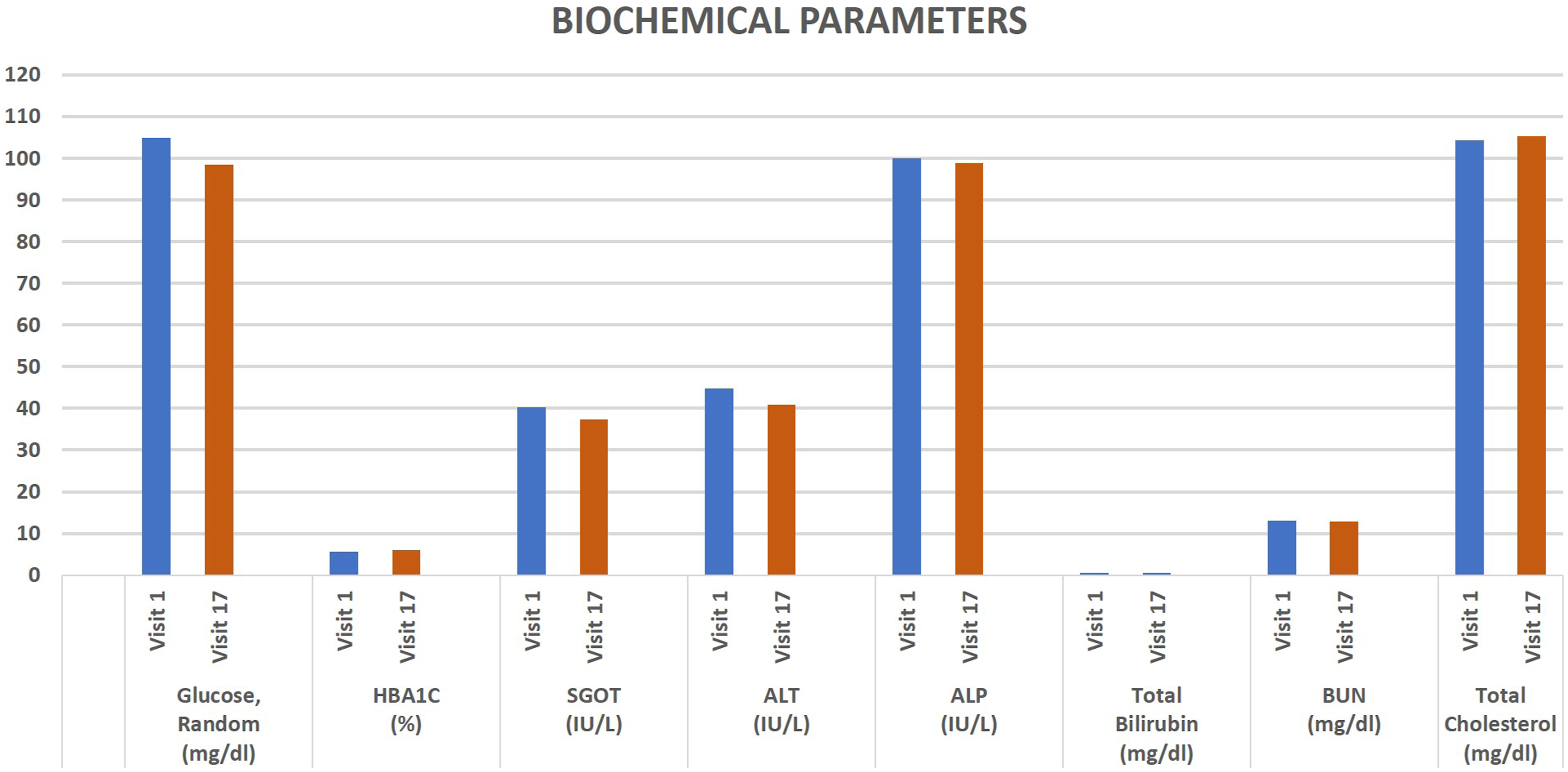
In addition to primary and secondary observation, blood samples were collected for hematological tests and biochemical tests, including hemoglobin levels, RBC and WBC count, and platelets count, and also for the measurement of cholesterol, glucose, and liver enzymes. No clinically significant changes were observed in the hematological parameters [insert Figure 6]; however, a non-significant decrease (p = .08) was seen in erythrocyte sedimentation rate. No clinically significant changes were observed in any of the biochemical parameters [insert Figure 7]. Mean value of different hematological parameters of patients at screening day (visit 1) and last follow-up visit (visit 17). Mean value of biochemical parameters monitored on screening day (visit 1) and last follow-up visit (visit 17).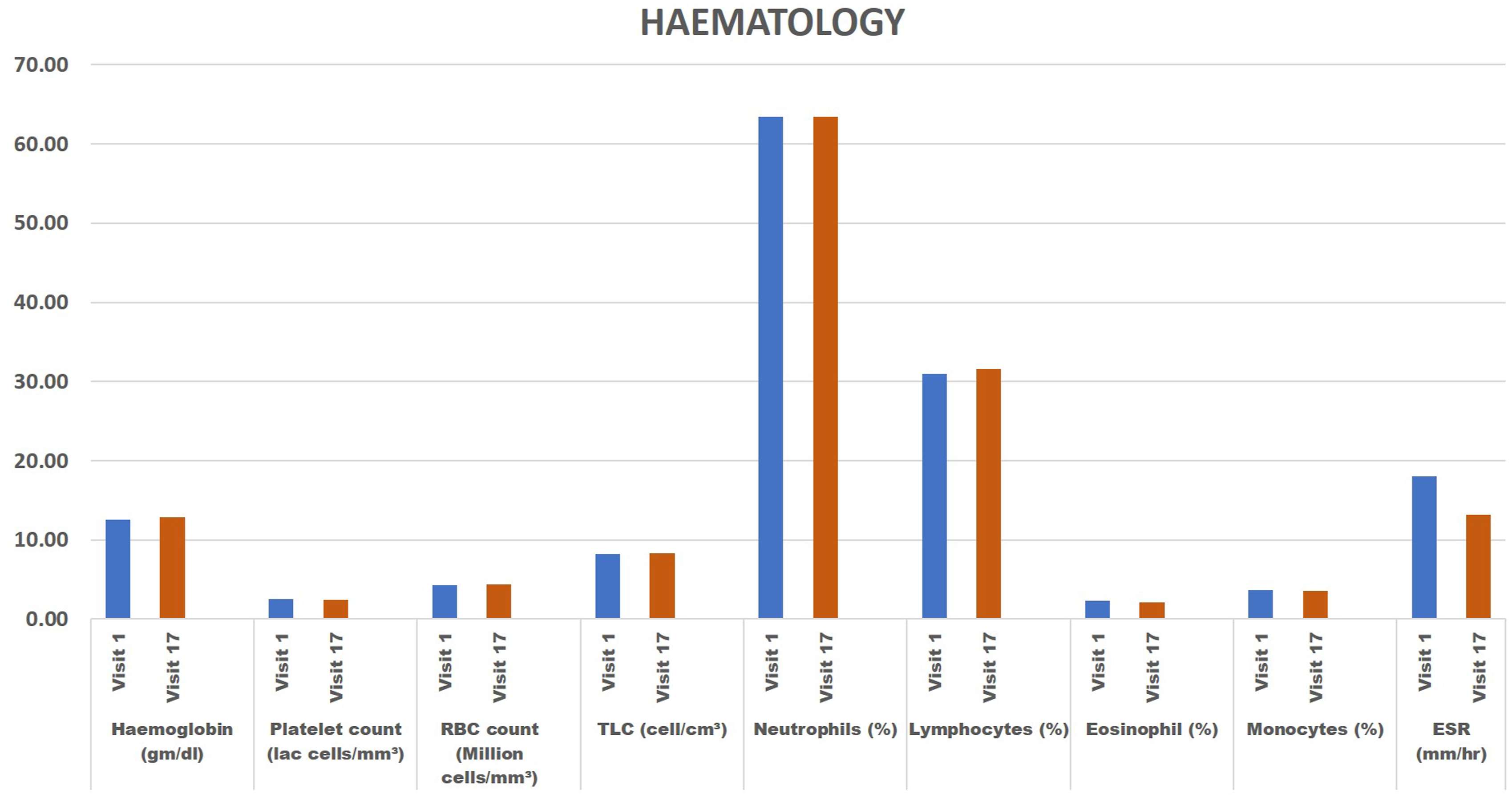
Discussion
VLUs have been associated with pain, infection, restriction of daily work due to impaired mobility, social isolation and impaired mobility. Leg ulceration can reduce psychological well-being and affects the quality of life. 10 The first-line treatments for venous leg ulcers are leg elevation, wound care, compression, and debridement. Leg elevation and application of external pressure assists venous return; thus, wound dressings are commonly used in combination with compression therapy, also, the common practice in our clinical setup. 11 In this study, antimicrobial wound dressing VELVERT was evaluated for its efficacy and safety as an adjuvant therapy for VLUs. VELVERT is a foam based, herbal antimicrobial dressing that comprises of a porous flexible matrix designed to absorb wound exudate and maintain a moist wound surface.
VELVERT was found to be an effective dressing as complete wound closure was attained in nine out of the 20 patients by EOT (60 days) and wound size reduction was observed in all the patients without giving any compression therapy. In a comparative analysis of two foam-based dressings for managing chronic venous leg ulcers, cumulative healing rates were assessed over 90 days, demonstrating a healing rate of 47.5% for Allevyn and 50.7% for Mepilex. 12 Interestingly, in our current study, approximately 45% of VLUs patients exhibited wound healing within 60 days or earlier, indicating a notably accelerated healing process for venous leg wounds. In the same study, 12 bandage-related withdrawals and wound deterioration occurred in 17 patients on Mepilex compared with 14 patients on Allevyn. Principal reasons for dressing-related incidents were found to be maceration and Eczema. In the present study, two non-serious adverse events (vomiting and lower back ache) of mild intensity were observed. These events were not related to dressing application. Moreover, patients did not complain of irritation, itching and/or uneasiness with the use of dressing as evaluated from SSAQs. Though, swab test was negative for microbial infection at the baseline (before application of VELVERT), wounds were monitored regularly for possible colonization of micro-organism. Swab test was done for monitoring microbial growth at regular interval, results were found negative throughout the trial. An infected wound can lead to sepsis, limb loss and increased mortality. 13 Thus, prevention of colonization/infection due to microbial growth can reduce the mortality rate and other wound complications. Velvert revealed promising results in terms of complete wound closure, percentage wound reduction and infection control.
In this study, two questionnaires were developed, one for the physicians and one for the patients. Physicians’ opinion was evaluated through questionnaire (Table 2) to provide clarity on their understanding of the IFU, the usage of dressing and performance of the dressing. The questionnaires were designed by the surgeons and clinical team based on their experience on the usage and by taking into the consideration the management and impact of leg ulceration on patients’ quality of life.14–17 It is even more important to know the perspective of patients on the experience with the usage of dressing. These surrogate endpoints provide a clear picture of patients’ opinion and experience with the intervention in addition to the quantitative measurements. Patients’ perspective may differ from those of the physicians; thus, it is more important how a patient feels after the treatment and consequently a clearer picture of clinical benefits (Table 3). A positive response from physicians was obtained indicating a consistently good experience with handling, usage, overall performance and appropriate in terms of instructions for use (Table 2). SSAQs were designed for evaluating safety, tolerability, and performance by assessing patients’ responses on these questionnaires (Table 3). No pyrogenic activity was observed with the usage of bandage. No irritation, itching, uneasiness and/ or discharge was observed. Patient found the usage of dressing comfortable and experienced less hindrance in walking.
There was evidence of reduction in the intensity of pain over the time in comparison to the baseline levels. A remarkable decrease in the pain level was observed after merely 4th application of the dressing. At the end of the study, more than half of the patient experienced no pain. Dressing changes is associated with pain and causes substantial stress for patients and clinicians. 18 Dressing changes, involve the movement at the wound site and, therefore, provide a mechanical trigger that causes or increases pain, similar to movement-evoked pain. Pain experienced during dressing changes, therefore, is similar to pain induced by mechanical stimuli. 19 In this study, VELVERT was changed every 4th day, the non-adherent property of the dressing is advantageous in the management of pain during wound care process. Pain was not experienced with the use of dressing throughout the study as assessed by SSAQs.
Further studies focusing on antimicrobial dressings are required to shed light on the benefits associated with their usage and guide medical professionals in making informed decisions regarding the management of VLUs.
One of the major limitations of this trial was that this was a single-arm study. The study outcome would have been more pronounced if a comparative arm was included. However, the clinical insights from this present study are compared to existing commercial products to provide information on safety and efficacy of the product. Also, the cost-effectiveness analysis can help doctors in decision-making process for using this intervention, however, cost-analysis was beyond the scope of current study. We encourage further research to evaluate the cost-effectiveness of the product. Further studies are required to establish whether outcome of this study may be generalized to the larger population.
Conclusion
The dressing was well-tolerated by patients and a positive response was received form clinicians. VELVERT showed the potential to offer advancements in wound care for patients with VLUs. This is a promising novel herbal dressing that could offer significant advantages to improve the quality, and convenience for wound management.
Supplemental Material
Supplemental Material - An open label, single-centric, post market clinical study to evaluate the safety and efficacy of a new antimicrobial wound dressing (VELVERT) as an adjuvant therapy in the treatment of venous leg ulcer
Supplemental Material for An open label, single-centric, post market clinical study to evaluate the safety and efficacy of a new antimicrobial wound dressing (VELVERT) as an adjuvant therapy in the treatment of venous leg ulcer by Sudhir Kumar, Suvash Sahu and Shivam Sharma in Phlebology
Footnotes
Acknowledgements
The authors acknowledge the Datt Mediproducts Pvt. Ltd for sponsoring the trial.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Datt Mediproducts Pvt Ltd NA.
Ethical approval
Institutional ethics committee approval letter was obtained for this study.
Guarantor
Dr. Sudhir Kumar.
Contributorship
The authors, Dr. Sudhir Kumar, Dr. Suvash Sahu and Dr. Shivam Sharma have made significant contributions to this manuscript, its conceptualization, data collection, interpretation, analysis, manuscript writing and editing. Authors drafted the article and approved its current format.
Registration Number
CTRI/2023/10/058211.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.