
Abstract
Objective
The incidence, risk factors, and clinical presentation of deep venous thrombosis (DVT) vary with age. This study aimed to evaluate the differences in clinical characteristics of DVT among patients of different ages.
Methods
We retrospectively analyzed 938 patients with symptomatic lower extremity DVT admitted to our hospital between January 2020 and January 2024. Patients were categorized into youth (<40 years), middle-aged (40–64 years), and elderly (>65 years) groups. Demographic data, comorbidities, risk factors, clinical presentations, and management approaches were collected and analyzed.
Results
Most participants were middle-aged or elderly, with young patients constituting only 11.19% of the study population. The youth group had a slight female predominance, while the middle-aged and elderly group had a balanced gender distribution. The elderly group were more likely to have comorbidities such as diabetes and malignancies, though they had a lower prevalence of autoimmune diseases compared to younger patients. Congenital risk factors were relatively rare in the overall population, yet were present in 22.86% of young patients, a significantly higher proportion than in the middle-aged and elderly groups. Most patients with DVT were provoked, especially in the elderly group. The prevalence of concurrent congenital and acquired factors was 13.33% in the youth group, compared to only 4.97% in the middle-aged group and 2.88% in the elderly group. Proximal DVT was most frequent in middle-aged patients, while young patients were more likely to seek treatment in the acute phase and undergo surgical intervention. Anticoagulation noncompliance was noted in nearly 40% of elderly patients but only 6.67% of young patients.
Conclusion
Risk factors and clinical characteristics of DVT vary significantly with age, particularly between young and elderly patients. Young patients were more inclined to seek prompt and effective treatment and demonstrated better adherence to anticoagulation therapy.
Introduction
Deep venous thrombosis (DVT) is a common peripheral vascular disease with incidence rates that increase significantly with age. Recent studies, however, indicate a rising incidence of DVT among the younger population due to specific factors, such as pregnancy or postpartum status, inherited thrombophilia, and autoimmune diseases.1–4 Young patients often present with more pronounced symptoms and are generally more attentive to their health, leading to earlier detection, timely treatment, and a better prognosis.3,5 In contrast, elderly patients frequently show atypical symptoms due to multiple underlying conditions and physiological decline, which results in a higher rate of complications and poor outcomes.6,7 Certain diseases, such as acute myocardial infarction,8,9 lung cancer, 10 and stroke, 11 exhibit age-related differences in presentation and progression. However, detailed comparisons of risk factors and clinical presentations of DVT across different age groups are limited. This study aims to clarify the clinical characteristics of patients of different ages with DVT and investigate age-related differences in risk factors and presentations.
Methods
Patient population
We retrospectively reviewed medical records of consecutive patients with symptomatic lower extremity DVT admitted to the Second Affiliated Hospital of Chongqing Medical University between January 2020 and January 2024. According to the European Society for Vascular Surgery guidelines, 12 hospitalization is indicated for patients with DVT who present with severe symptoms (e.g., extensive limb swelling or pain), develop complications (e.g., pulmonary embolism), or require the initiation of parenteral anticoagulation therapy. This study was approved by the ethical committee of our hospital, and the requirement for patient informed consent was waived due to the retrospective nature of the study. Patients with abnormal hereditary factor test results who declined re-examination or were lost to follow-up were excluded. Patients were categorized into three age groups: youth (<40 years), middle-aged (40–64 years), and elderly (>65 years). Following established guidelines,4,13 we routinely screened for underlying risk factors, and thrombophilia testing (including tests for antithrombin deficiency, protein C or S deficiency, factor V Leiden mutation, prothrombin 2010A mutation, and methylenetetrahydrofolate reductase (MTHFR) C677 T mutation) was recommended for patients with a history of venous thromboembolism (VTE), age <40 years, or a first VTE associated with pregnancy or oral contraceptive use. All patients with suspected DVT initially underwent lower extremity venous ultrasonography. Those confirmed or suspected to have deep vein thrombosis subsequently underwent lower extremity venography to evaluate thrombus location, burden, and the presence of concurrent IVC thrombosis. Standard anticoagulation was routinely recommended for eligible patients without contraindications, and early thrombus removal strategies were considered for patients with symptomatic proximal DVT within our department.
Data collection
Data were collected from the centralized electronic medical record system of the hospital. Collected information included demographic characteristics (name, gender, identification number, and body mass index), personal habits (current smoking and alcohol consumption), comorbidities (diabetes, hypertension, hyperlipemia, coronary artery disease, chronic obstructive pulmonary diseases, heart failure, obesity, autoimmune diseases, nephrotic syndrome, severe infections, and malignancy), and medical history (recent surgery, recent fractures, immobilization, chronic venous insufficiency, pregnancy or postpartum status, estrogen replacement therapy, history of VTE, and central venous catheterization). Clinical manifestations and management details, including DVT location, disease course, occurrence of pulmonary embolism, surgical interventions (e.g., Catheter-Directed Thrombolysis (CDT), Percutaneous Mechanical Thrombectomy (PMT), surgical thrombectomy), and medication adherence, were also recorded.
Diagnostic criteria and variable definition
The diagnosis of DVT was confirmed using compression ultrasonography or venography in combination with D-dimer testing. The diagnosis of pulmonary embolism is established through an integrated approach incorporating clinical probability assessment (e.g., Wells score), D-dimer testing (for exclusion in low-probability cases), and definitive imaging confirmation (with computed tomography pulmonary angiography [CTPA] serving as the diagnostic reference standard, or ventilation-perfusion [V/Q] scintigraphy when contraindications exist). 14 The current alcohol consumption was defined as having consumed alcohol within the past 1 year. The current smoking was defined as having used any tobacco products within the past 30 days. Diabetes was defined as a chronic metabolic disorder characterized by either fasting plasma glucose ≥7.0 mmol/L or HbA1c ≥ 6.5%. Hypertension was defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least two separate measurements. Hyperlipidemia was diagnosed based on elevated LDL-C (>3.4 mmol/L), triglycerides (>1.7 mmol/L), or reduced HDL-C (<1.0 mmol/L in men or <1.3 mmol/L in women), as confirmed by serum lipid profiling. 15 Coronary artery disease was defined as atherosclerotic narrowing of the coronary arteries, confirmed by either invasive angiography (≥50% stenosis) or CT angiography, and associated with myocardial ischemia. 16 Chronic obstructive pulmonary disease (COPD) was diagnosed based on a post-bronchodilator FEV1/FVC ratio <0.70, along with structural lung changes (e.g., emphysema or airway thickening) observed on high-resolution CT. 17 Heart failure was defined as a clinical syndrome characterized by either reduced ejection fraction (LVEF <50%) or preserved ejection fraction (LVEF ≥50%) with elevated BNP/NT-proBNP levels, as assessed by echocardiography or cardiac MRI. 18 Malignancy was confirmed by histopathological evidence (biopsy) and metabolic activity (FDG-PET/CT SUVmax >2.5). 19 Autoimmune disease was diagnosed based on the presence of serological markers (e.g., ANA, anti-dsDNA) and imaging evidence of inflammation (e.g., synovitis or encephalitis on MRI/PET). 20 Recent surgery or fracture was defined as any surgery or fracture occurring within 3 months before the onset of DVT. Severe infection was classified as a systemic inflammatory response or organ dysfunction caused by pathogenic microorganisms, such as bacteria, viruses, fungi, or parasites. Immobilization was defined as continuous bed rest for ≥7 days. Distal DVT referred to thrombi located below the popliteal veins, such as in the calf or tibial veins, while proximal DVT involved thrombi in the veins above the popliteal veins, with or without involvement of distal veins. 4 According to guidelines, anticoagulation noncompliance was defined as follows: for provoked DVT, patients receiving anticoagulation for <3 months; for unprovoked DVT, patients receiving anticoagulation for <6 months; or patients with irregular medication use or nonstandard anticoagulant drug use.4,21,22
Risk factors were classified into congenital factors—such as proteins C and S and antithrombin deficiencies, as well as factor V Leiden, prothrombin 2010A, and MTHFR C677 T mutations—and secondary factors, which included recent surgery or fracture, immobilization, malignancy, autoimmune disease, obesity, iliac vein compression syndrome, antiphospholipid syndrome, pregnancy, history of VTE, nephrotic syndrome, and cardiopulmonary failure.4,22
Statistical analysis
Categorical variables are presented as absolute numbers or percentages and were compared among 3 groups using chi-squared tests. Statistical analysis was performed with IBM SPSS Statistics for Windows (version 26.0; IBM Corp., Armonk, NY, USA). A p-value <0.05 was considered statistically significant for all comparisons.
Results
The demographic characteristics of different age groups.
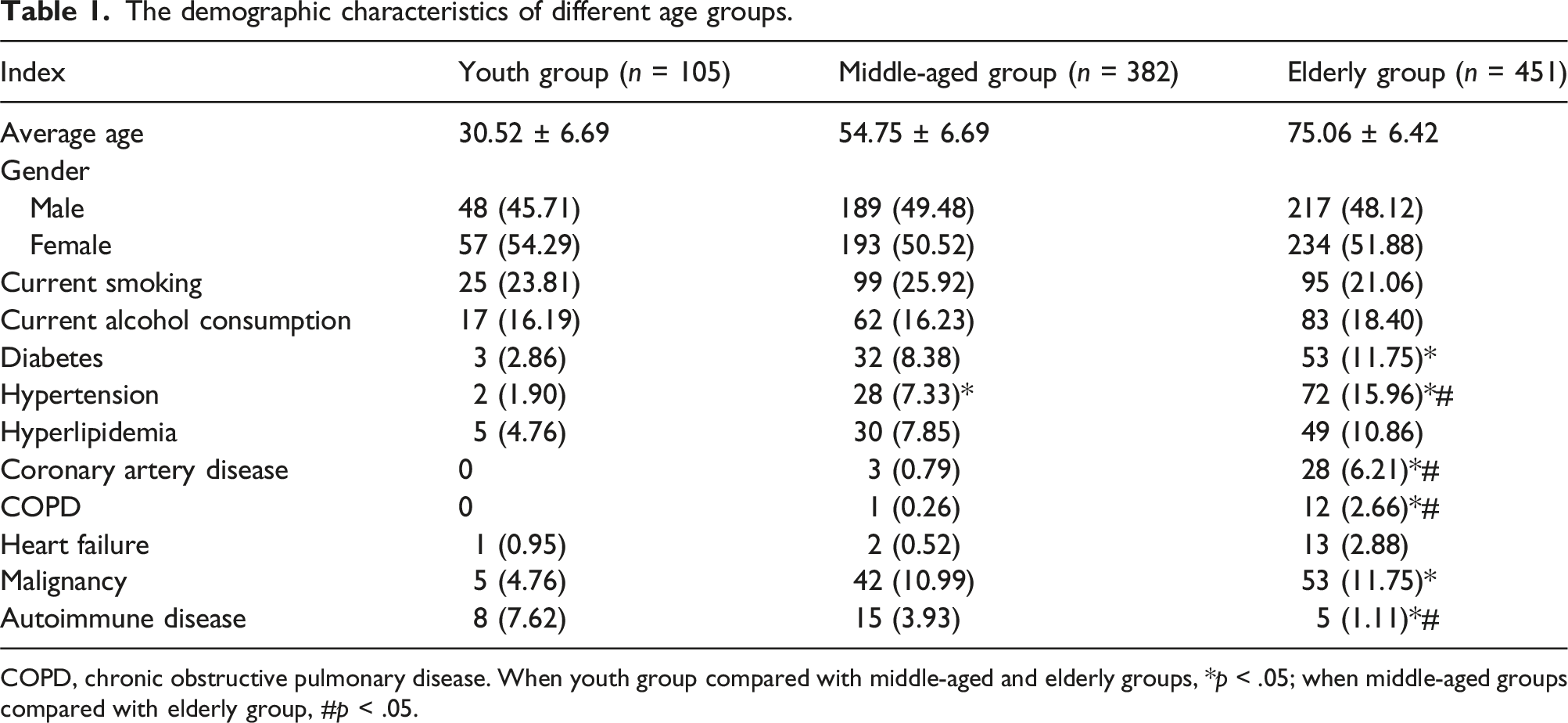
COPD, chronic obstructive pulmonary disease. When youth group compared with middle-aged and elderly groups, *p < .05; when middle-aged groups compared with elderly group, #p < .05.
The characteristics of congenital risk factors across three groups.
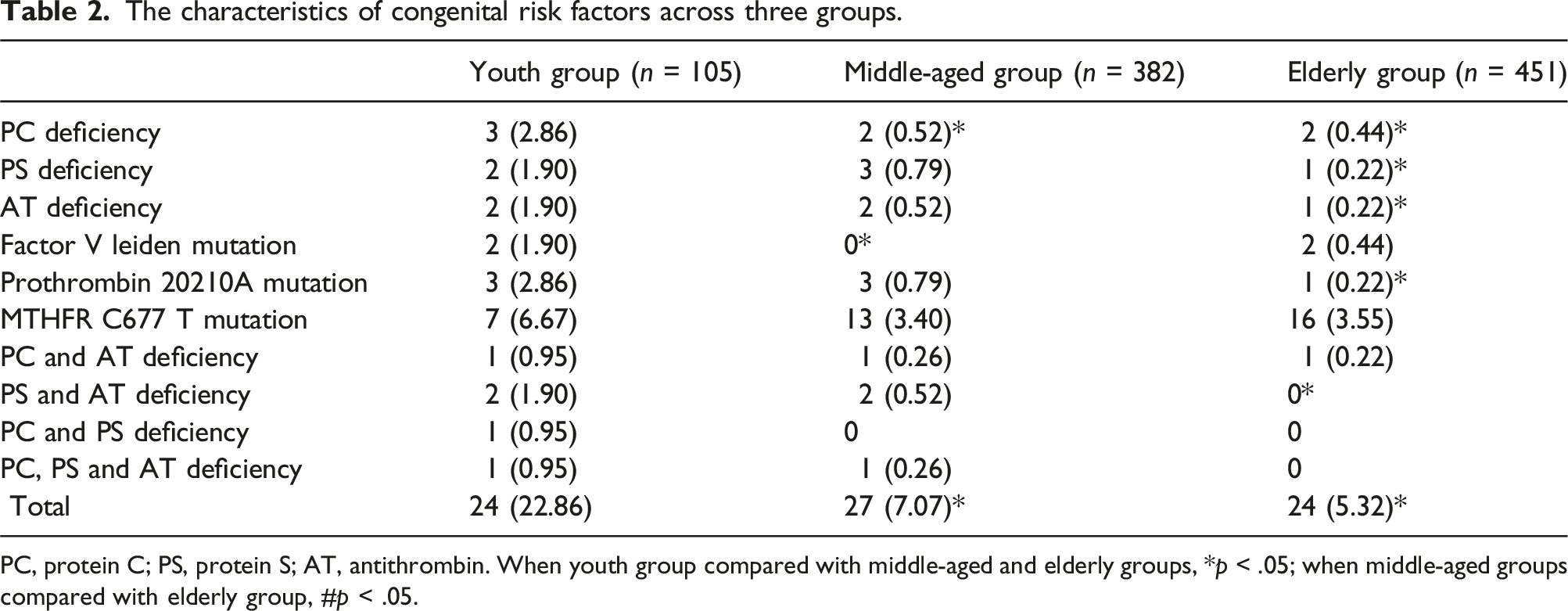
PC, protein C; PS, protein S; AT, antithrombin. When youth group compared with middle-aged and elderly groups, *p < .05; when middle-aged groups compared with elderly group, #p < .05.
The characteristics of acquired risk factors across three groups.
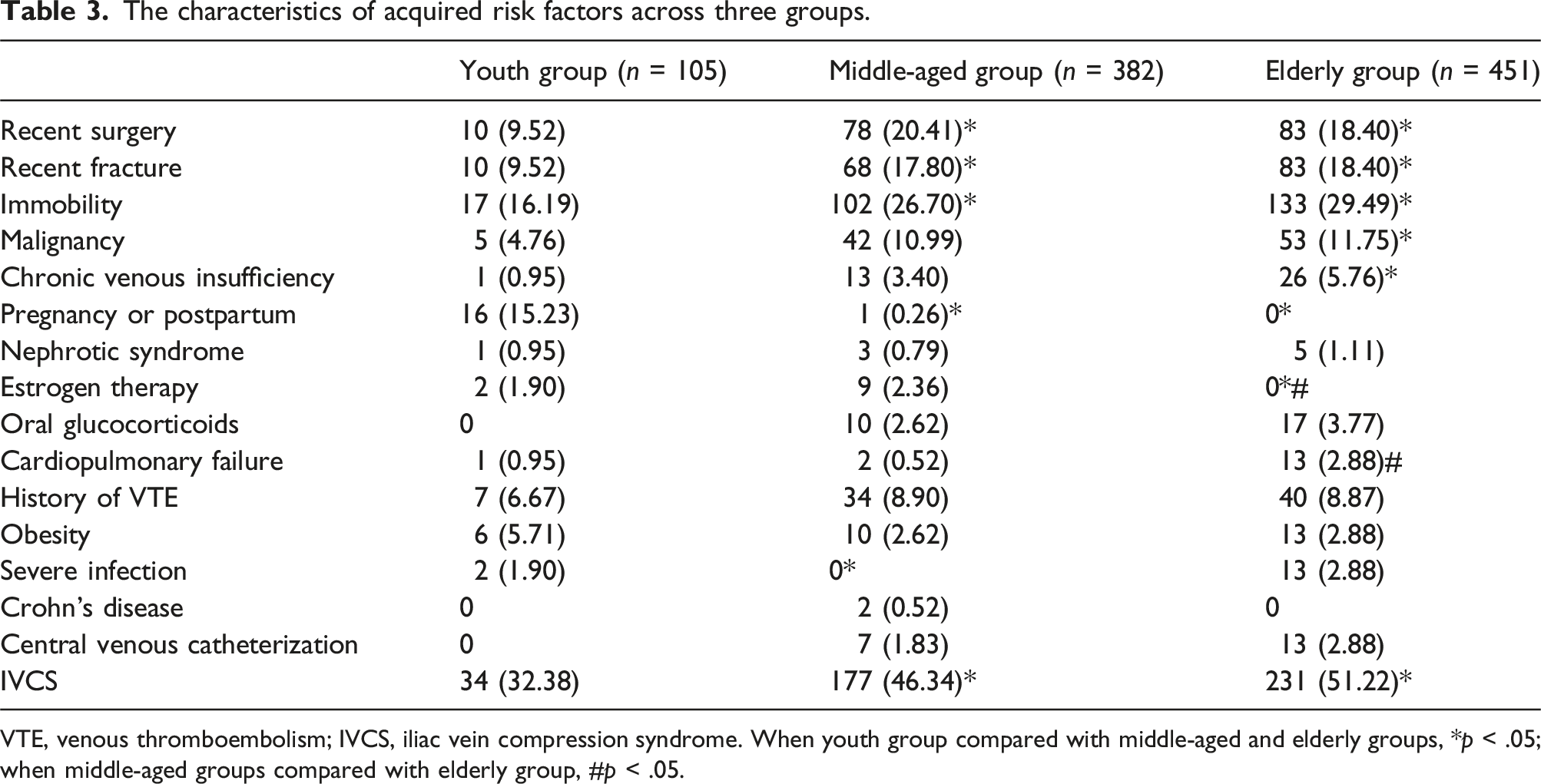
VTE, venous thromboembolism; IVCS, iliac vein compression syndrome. When youth group compared with middle-aged and elderly groups, *p < .05; when middle-aged groups compared with elderly group, #p < .05.
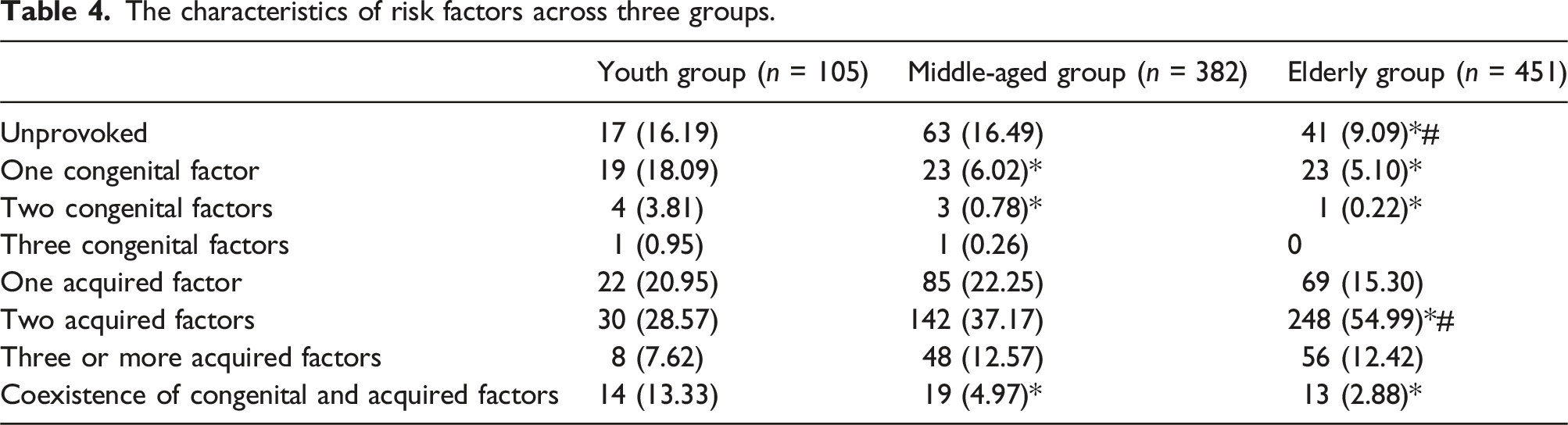
The characteristics of risk factors across three groups.
The clinical manifestations and treatment characteristics of three groups.
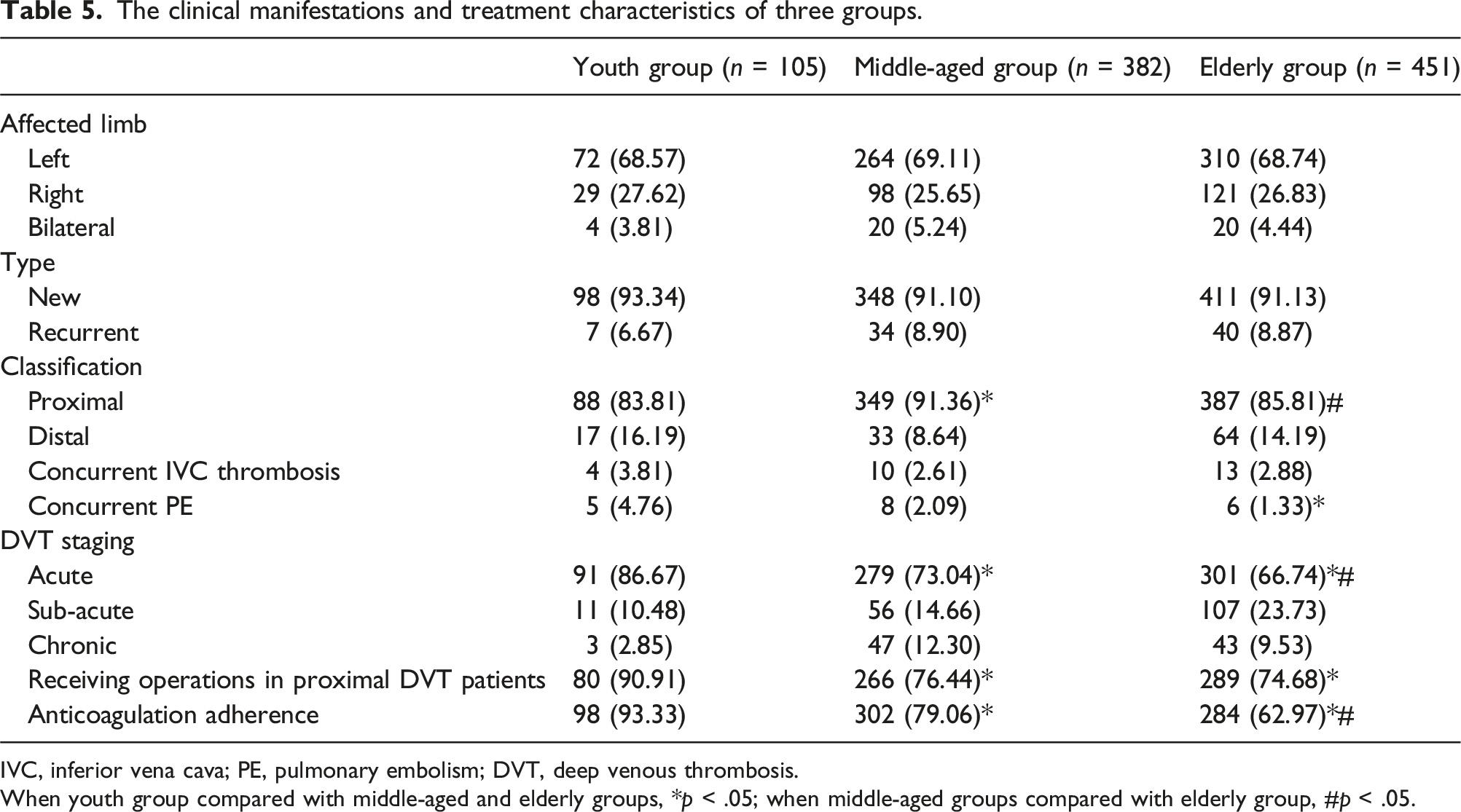
IVC, inferior vena cava; PE, pulmonary embolism; DVT, deep venous thrombosis.
When youth group compared with middle-aged and elderly groups, *p < .05; when middle-aged groups compared with elderly group, #p < .05.
Discussion
Numerous studies have confirmed that advancing age is positively associated with the incidence of DVT, primarily due to reduced mobility, coexisting medical conditions, and age-related changes in the coagulation system.1,3,6 In our study, the majority of patients were >40 years old, with only 11.19% of participants being <40 years of age, which aligns with previous studies.1,2 Interestingly, we observed a female predominance in the youth group, while middle-aged and elderly groups exhibited a more balanced gender distribution. This difference may be attributed to the procoagulant state associated with pregnancy or the postpartum period among the young female population. 23 Pregnant patients face a significantly elevated risk of DVT, estimated to be 5 times higher than that of non-pregnant individuals, with the risk increasing dramatically to 60 times during the first 6 weeks postpartum. 24 Furthermore, autoimmune diseases such as systemic lupus erythematosus and antiphospholipid syndrome were more prevalent in the youth group compared to the elderly group, particularly among the young female population. 25 This may further explain the higher proportion of females in the young patient population with DVT in our study.
Inherited thrombophilia is often characterized by a strong family history of VTE, recurrent VTE, DVT at unusual sites, and the occurrence of DVT at a young age. 13 In our study, we found that 22.86% of young patients were affected by inherited thrombophilia, a significantly higher proportion compared to middle-aged and elderly groups, which aligns with previous research.2,3 The primary inherited factors identified were proteins C and S and antithrombin deficiencies, differing from findings in Western populations (Factor V Leiden mutation and prothrombin G20210 A gene mutation). 26 Additionally, the prevalence of these deficiencies in our study was lower than that reported in a recent meta-analysis (3.8%–8.3%). 27 This discrepancy may be attributed to the fact that testing for inherited thrombophilia was conducted primarily in the suspected population rather than being universally performed on all patients at our hospital.
In contrast to congenital factors, acquired factors were the primary causes of DVT in this retrospective study. Middle-aged and elderly patients were more likely to have complications related to recent fractures or surgeries and immobilization than their younger counterparts, primarily due to underlying conditions, such as osteoporosis. Nearly 60% of fractures are associated with osteoporosis, which is more prevalent in older populations, consequently leading to a higher incidence of DVT among the elderly patients. 28 Furthermore, malignancies can release procoagulant proteins and directly compress adjacent veins, resulting in a hypercoagulable state. Recent report indicates that the incidence of cancer begins to rise significantly between the ages of 35 and 39, peaking at 80 to 84 years. 29 In our findings, malignancy was more commonly observed in the elderly population, with a proportion of nearly 11.75%, consistent with previous studies.1,2,6
Data on the characteristics of predisposing factors in patients with DVT and comparisons among different age groups are limited; most publications primarily describe the risk factors of the study populations.30,31 In our study, the proportion of patients with unprovoked DVT was significantly higher in the youth group, at approximately 16.19%, which aligns with previous reports.1,2 This difference may be attributed to the increase in underlying diseases with age, such as tumors and chronic cardiopulmonary insufficiency. Notably, 13.33% of young patients with congenital risk factors also presented with acquired factors, suggesting that these acquired factors likely serve as provoking factors. This underscores the importance of thoroughly investigating potential inherited factors in young patients. In contrast, the majority of risk factors identified in middle-aged and elderly patients were acquired. The coexistence of two acquired factors was more prevalent in elderly patients, highlighting the need for careful screening, particularly for malignancies in this age group. It has been reported that initial symptoms of VTE occur in 2.2%–12% of patients with occult tumors, such as leukemia and lung cancer. 32
In this research, left-sided DVT was predominant among patients of all ages, a phenomenon potentially linked to the anatomic predisposition of left iliac vein compression. 33 The majority of patients presented with proximal DVT, which can be partly attributed to the enrollment criteria, as only those with obvious symptoms were included in this study. The frequency of pulmonary embolism may have been underestimated, given that contrast-enhanced computed tomography was performed only when patients exhibited relevant symptoms at our center. Interestingly, young patients experienced a higher incidence of pulmonary embolism compared to their middle-aged and elderly counterparts. This difference may be due to a lower prevalence of iliac vein compression syndrome and a higher proportion of inherited thrombophilia in the young population. In contrast to the elderly, young patients typically had fewer underlying diseases and tended to be more proactive about their health, resulting in more pronounced symptoms. 3 This awareness likely contributed to a higher proportion of acute cases among young patients, many of whom underwent surgical intervention. Additionally, young patients demonstrated stronger medication adherence compared to elderly patients, a finding consistent with previous studies. This discrepancy may be attributed to age-related factors such as memory loss, diminished attention, and the challenges older patients face in obtaining anticoagulants. 34
The main strength of this study lies in its ability to elucidate the characteristics of risk factors and clinical manifestations among patients of different ages with DVT. However, there were also certain limitations. First, the study employed a retrospective design, and the number of young patients was lower than that of middle-aged and elderly groups, which may influence the results. Second, the limited number of certain events, such as medical histories of nephrotic syndrome and cardiopulmonary failure, restricted the scope of the statistical analysis. Third, only patients with symptomatic DVT were enrolled, and testing of congenital thrombophilia factors was conducted exclusively in suspected populations based on established guidelines. This approach may not fully capture the characteristics of the broader population. Finally, information regarding the prognosis of the study population was not available, as various treatment modalities were adopted based on individual patient preferences and the availability of resources.
Conclusion
The majority of patients with symptomatic DVT were middle-aged and elderly, with a notable female predominance among the young patients. Acquired factors were the primary causes of DVT, particularly in the elderly population, while young patients were more likely to have inherited thrombophilia, with the onset of DVT also associated with various acquired factors. Furthermore, young patients demonstrated a greater willingness to seek treatment during the acute phase and to undergo surgical procedures, exhibiting favorable adherence to anticoagulation therapy compared to their elderly counterparts.
Footnotes
Author contributions
Haiyang Wang conceived and designed the studies; Haoyuan Wang, Yujia Li, Jianming Sun analyzed the data; Lili Zhang prepared the tables; Bo Wu wrote the paper. All authors reviewed and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Natural Science Foundation of Chongqing, China Grant (No. CSTB2023NSCQ-MSX0723).
Guarantor
Haiyang Wang