
Abstract
Objectives
To assess the incidence of secondary telangiectasias (TAEs) after endovenous laser ablation (EVLA) of the great saphenous vein (GSV) and discuss the possible risk factors for its development.
Method
This prospective observational study enrolled 123 lower limbs of 103 patients with varicose veins of C2 or C4 clinical classes who underwent EVLA of the GSV trunk from the saphenofemoral junction to the below knee level without simultaneous removal of varicose tributaries and/or perforating veins. The primary outcome was the occurrence and amount of secondary TAEs (matting) that developed at the medial aspect of the thigh along the treated GSV within a 3-month follow-up. The assessment was made by analysis of before and after photos by three experienced surgeons using a four-point scale. Fleiss’ Kappa was used to measure the agreement between the assessors.
Results
Secondary TAE development was reported in 26 limbs (21.1%; 95% CI, 15.0-29.0%). Almost perfect agreement was observed between assessors for any matting (κ = 0.92; p < .0001) and different amounts of it (κ = 0.93, κ = 0.90, κ = 0.85, and κ = 1.00 for the score of 0, 1, 2, and 3, respectively). The most prevalent was a low amount of new TAEs (score of 1 in 17.9%). The only significant difference between the patients with and without secondary TAEs was age: 52.5 (IQR, 43-61) versus 40 (IQR, 34-53) years old.
Conclusions
In most cases (96,8%), secondary TAEs are either absent or could be found in a low amount. Older patients are more predisposed to its development.
Introduction
Primary varicose veins (VV) are a common manifestation of chronic venous disease (CVD), affecting about 19% of the population. 1 Valvular insufficiency with reflux on the great saphenous vein (GSV) is the most common reason for VV appearance. 2 According to the current guidelines, the first line of treatment for GSV reflux is thermal ablation by laser or radiofrequency.3,4 It is a practical approach providing significant technical success and clinical improvement with minimal risk of complications and side effects that may include postoperative venous thromboembolism, phlebitis, ecchymosis and bruising, postprocedural pain, paresthesia, and nerve injury, hyperpigmentation, skin burns.5,6 However, such a complication as the development of secondary telangiectasia (TAE), also known as matting along the ablated vein, is mentioned among others in the exclusive document. 7 At the same time, its prevalence, natural history, and mechanisms of development are still not established.
Thus, Kadam P et al., among 27 possible risk factors for the development of matting, found statistically significant associations with previous endovenous laser ablation (EVLA) during univariate analysis. However, only three risk factors demonstrated an independent association within multivariate analysis: recurrent nose bleeding, previous sclerotherapy, and hypersensitivity. 8
At the same time, secondary TAEs can appear along the treated GSV on the medial aspect of the thigh in some patients after thermal ablation. They tend to be thicker and bluish than thin and reddish matting, which develops after sclerotherapy. A few authors in publications in early 2000 and a letter to the editor mentioned this phenomenon in the first weeks after the procedure.9–11 Matting after thermal ablation and sclerotherapy may differ due to underlying mechanisms, particularly the role of inflammatory neoangiogenesis and blocked or reversed blood outflow. This assumption may support the approach of saphenous vein sparing to prevent disturbance of blood drainage and development of secondary TAEs. 12
This study aimed to assess the instance of secondary new TAE appearance after laser ablation of GSV and discuss the risk factors for its development.
Methods
This prospective observational non-comparative single-center study with independent outcome assessment occurred at the base of the Clinic of Outpatient Phlebology of the South Ural State Medical University (Chelyabinsk, Russia). It enrolled patients with varicose veins who underwent EVLA of the GSV trunk from the saphenofemoral junction (SFJ) to the level below the knee without simultaneous removal of tributaries and/or perforating veins.
The inclusion criteria were: primary varicose veins of lower limbs with pathological reflux on the GSV trunk for more than 0.5 seconds as detected by duplex ultrasound scan (DUS); i-type or h-type of GSV trunk (by International Union of Phlebology anatomical classification 13 ); the suitability for isolated GSV ablation without treatment of varicose tributaries and perforating veins; given informed consent. The institutional policy considered routine isolated EVLA of GSV trunk with deferred sclerotherapy of varicose tributaries in those patients who preserve symptoms and/or aesthetic complaints at ≥3 months after primary intervention. This approach corresponded with the actual National clinical recommendations and does not contradict the modern International guidelines.3,4
The exclusion criteria were: the presence of pronounced TAEs and reticular veins on the medial aspect of the thigh before intervention; s-type of GSV trunk (by International Union of Phlebology anatomical classification 13 ); the necessity for concomitant removal of tributaries and perforating veins; the ipsilateral pathological reflux in the anterior accessorial saphenous vein, small saphenous vein, perforating vein in the middle third of the thigh; individual history of deep or superficial vein thrombosis; venous malformation; arterial insufficiency (claudication and/or decreased pulsation on peripheral arteries); the presence of dermatological diseases in the active phase. The exclusion of patients with preexisting TAEs and reticular veins in the zone of assessment was done to increase the accuracy and agreement of evaluation. The interpretation of TAEs increasing in number or size after the intervention may be confusing. Additionally, the pronounced TAEs implied their visibility in the pretreatment photos, which was assessed subjectively.
Patients’ demographic data, including age, sex, and body mass index (BMI); the clinical class of CVD by Clinical, Etiological, Anatomic, and Pathophysiologic (CEAP) classification; the CVD severity by venous clinical severity score (VCSS) were collected. The maximal GSV diameter at the distance of 3 cm below the SFJ and in the middle third of the thigh was measured by DUS. The medial aspect of the thigh was captured in photos before and after the intervention. For this purpose, the patient stood vertically with his weight bearing on both limbs; the treated leg was rotated externally. The photos were taken with a “Nikon D90” camera (Nikon Corporation, Japan) and a “Nikon Speedlight SB-700″ external flash (Nikon Corporation, Japan) in a warm, well-lit room in the morning time.
EVLA was performed in the standard mode under tumescent anesthesia with a Klein solution, a wavelength of 1470 nm (laser generator “Lahta-Milon”, Lahta, Russia), and power of 7W by automatic traction (automatic pulling device “Diotech”, DIOTECH Co., Ltd, South Korea) of the radial fiber (“ELVES Radial”, Biolitec, Germany) with a speed of 1 mm/s, which provided LEED of 70 J/cm. The power settings did not depend on the vein diameter based on the data suggesting a high occlusion rate with a similar linear endovenous energy density of ∼70 J/cm irrespective of the energy power. 14 The tumescent anesthesia was performed with a 21G needle “Sterican” (B. Braun, Germany) of 12 cm in length. All interventions were carried out by a single surgeon with more than 15 years of experience in phlebology.
Patients were followed the next day and 3 months after the procedure, when, besides clinical examination and DUS, the medial aspect of the thigh was captured in photos again.
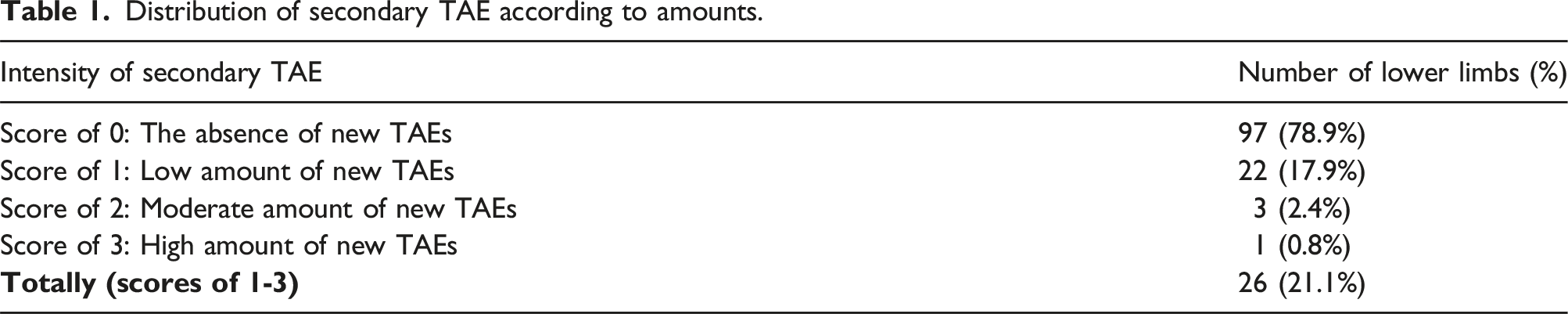
The primary outcome was the occurrence and amount of secondary TAEs (matting) that developed at the medial aspect of the thigh along the treated GSV trunk. To assess it, the photos before and 3 months after the intervention were analyzed independently by three surgeons with experience in phlebology of ≥5 years according to the four-point scale: 0 – the absence of new TAE, 1 – low amount of new TAE (a few new thin TAEs diffusely located and occupying no more than 10% of the medial aspect of the thigh), 2 – moderate amount of new TAE (several new TAEs of small and medium size closely located and occupying from 10 to 25% of the medial aspect of the thigh), 3 – high amount of new TAE (many small and big new TAEs located closely and occupying >25% of the medial aspect of the thigh). The assessors were provided with reference pictures of new TAEs of different amounts.
The study was performed under the Helsinki Declaration. The protocol was approved by the Institutional Review Board of the South Ural State Medical University (Approval no.10 from 23.10.2015) as a part of global work on the assessment of EVLA efficacy and safety started in 2015, and informed consent was obtained from all participants before the trial.
Statistical analysis
The R statistical programming language was used for the analysis. The data are represented as absolute values with medians and interquartile ranges (IQR) of 25-75 percentile. For the relative values as percentages, 95% confidence intervals (CI) are calculated using the method of Sison and Glaz (realized in R library MultinomialCI). The Mann-Whitney-Wilcoxon test was utilized to determine the significant differences between patients with and without secondary TAEs in numerical variables and Fisher’s exact test in categorical variables. Fleiss’s Kappa analyzed the agreement between assessors (irr: Various Coefficients of Interrater Reliability and Agreement; R package version 0.84.1). It was interpreted as almost perfect agreement if > 0.8, substantial agreement if 0.6-0,8, moderate agreement if 0.4-0.6, fair agreement if 0.2-0.4, slight agreement if > 0, and no agreement if < 0. 15 Additionally, a Predictive Power Score (PPS) was used to reveal all possible associations of demographic factors with the development of new TAEs (ppsr: Predictive Power Score; R package version 0.0.2). The higher values range between 0 and 1, representing possible associations. The main unit of the analysis was the lower limb. Due to some patients having bilateral disease and interventions on both limbs, a sensitivity analysis was performed in the subgroup of individuals with unilateral intervention. The p-value of <0.05 was considered statistically significant.
Results
The study enrolled 143 lower limbs of 121 patients, who were consequently treated from February to October 2020. Of them, 18 had no follow-up visit within a specified time. Thus, 123 limbs of 103 patients were included in the analysis.
They were 40 men (38.8%) and 63 women (61.2%). Age varied from 18 to 82 years old (median of 43 with IQR of 34.5-57.5), and BMI ranged from 17.7 to 36.9 kg/m2 (median of 26.3 with IQR of 23.6-28.9). CEAP clinical class was С2 in 113 (91.9%) and С4 in 10 (8.1%) lower limbs. There were no patients of С3, С5, and С6 clinical classes. According to the VCSS, the severity of CVD ranged from 2 to 9 scores (median of 4 with IQR of 3-5). The maximal GSV diameter ranged from 6.0 mm to 29.1 mm (median of 10.1 with IQR of 8.6-11.6) at 3 cm below the SFJ and from 3.5 to 10.5 mm (median of 6.0 with IQR of 5.1-7.0) in the middle third of the thigh. At the 3-month follow-up, no signs of vein recanalization, defined as the presence of anterograde or retrograde blood, was found by DUS.
Distribution of secondary TAE according to amounts.
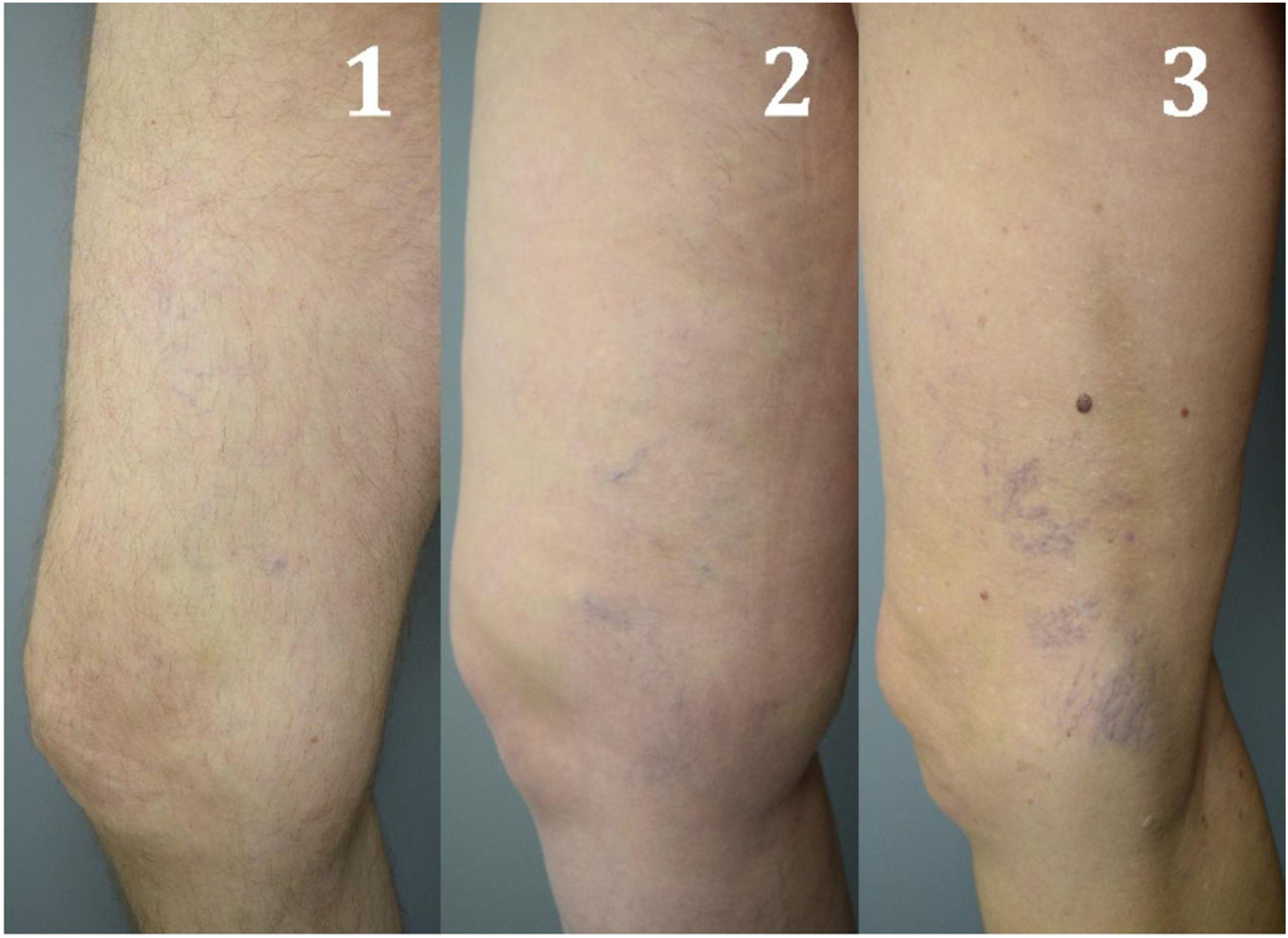
Examples of secondary TAE at 3 months after EVLA of the GSV trunk: 1-low amount, 2-moderate amount, 3-high amount.
The median age in the individuals without TAEs was significantly lower than in those who developed matting: 40 (IQR, 34-53) and 52.5 (IQR, 43-61) years old, respectively (p = .006). No significant differences between patients without and with new TAEs were found in BMI (median of 25.9 with IQR of 23.5-29.1 vs median of 26.8 with IQR of 24.1-28.6; p = .715), VCSS score (median of 4 with IQR of 3-5 vs median of 4 with IQR of 3.25-5; p = .099), GSV diameter below the junction (median of 10.0 with IQR of 8.4-11.4 vs median of 10.5 with IQR of 9.3-12.7; p = .166) and in the middle third of the thigh (median of 6.0 with IQR of 5.0-6.8 vs median of 6.5 with IQR of 5.3-7.6; p = .104). No significant association was observed for sex (p = .648) and CEAP clinical class (p = 1.000).
According to the PPS test, the possible predictive values were observed for the age (pps = 0.03), GSV diameter at the middle third of the thigh (pps = 0.05), and BMI (pps = 0.03). However, the modeling was unstable due to the small sample size and limited number of indicators.
The subgroup analysis of different amounts of matting was unavailable due to a limited number of observations.
Of the 103 patients, 20 had bilateral disease in 40 limbs, so the subgroup of 83 individuals with 83 treated limbs was analyzed separately within sensitivity analysis. The secondary TAEs were reported in 18 limbs (21.7%; 95% CI, 14.1-31.8%). The patients with matting were significantly older (median age of 52.5 with IQR of 38.3-64 vs 38 with IQR of 31-52, p = .016) without any differences according to other parameters. Based on the results of the PPS test, the possible predictive values were observed only for the age (pps = 0.09). So, the subgroup analysis confirmed the sustainability of the results obtained in the total sample.
Among 20 patients with bilateral disease, the secondary TAEs were reported in 6 cases on one limb and in 1 case on both limbs, with the total lesion on 8 of 40 limbs (20%; 95% CI, 10.3-35.1%). No significant difference in the occurrence of new TAEs was found between patients with bilateral and unilateral disease (p = 1.0).
Discussion
Despite physicians observing the appearance of secondary TAEs on the medial aspect of the thigh following endovenous thermal ablation of GSV, Pavlovič MD et al. were the only ones who accurately described this phenomenon. 9 Also, several papers have reported the appearance of thigh TAEs after GSV laser ablation. However, they contain anecdotal findings or do not provide specific numbers on its incidence or risk factors.10,11 Maeso J et al. reported the presence of major (without clear definition) TAEs in 9% and 66% of patients 3 years after saphenous sparing strategy (CHIVA approach) and GSV stripping, respectively. 16 Meanwhile, this study was not randomized, with significant differences between the groups, and did not properly report TAE’s assessment and precise localization on the medial aspect of the thigh.
The current study was designed to overcome these limitations and provide the actual incidence of secondary TAE development on the medial aspect of the thigh at 3 months after GSV laser ablation of 21.1%. At the same time, in most cases (17.9%), the amount of new TAEs was low, while a moderate to high amount was detected in only 3.2% of cases.
Hence, in 96.8% of patients after EVLA, secondary TAEs are either absent or can be found in a low amount that does not represent a severe cosmetic problem. Moreover, older patients are more predisposed to developing such a phenomenon but usually have lower aesthetic expectations.
The underlying mechanism of the observed phenomenon is of particular interest. Pavlovič MD et al. advanced the hypothesis that the occurrence of TAE was attributable to obstructed outflow through the feeding vein. 9
At the same time, most of the skin and subcutaneous tissues of the human lower extremity are supplied by blood via cutaneous arteries that do not originate directly from the main axial arteries. Instead, these tissues receive blood through musculocutaneous, or fasciocutaneous, arteries that pierce the deep fascia, forming the subcutaneous arterial plexus.17,18 However, two regions demonstrate an exception to this pattern. One of them is the anteromedial aspect of the mid-distal thigh. This region is supplied with blood by the saphenous artery, a branch of the descending genicular artery originating from the femoral artery in the adductor canal. Two veins and the saphenous nerve accompany it.17,19–21 Consequently, this region exhibits a dual venous drainage system comprising the concomitant veins of the saphenous artery and GSV trunk. 20 Recent studies have demonstrated that during locomotion (walking or running), when there is a significant increase in arterial blood flow, the primary venous drainage route is facilitated by perforating veins. This outflow is synchronized with muscle pump action. 22 Thus, it can be postulated that the concomitant veins of the saphenous artery constitute the primary conduit of venous outflow in exercise hyperemia. However, it is noteworthy that in 5% to 25% of cases, the saphenous artery system may be absent, thus rendering the GSV a significant pathway for blood outflow, at least from the distal to mid-thigh regions, where substantial perforating veins are present.17,19,20 Consequently, in the absence of the saphenous artery system, obliteration of the GSV may lead to cutaneous vasculature expansion and visible TAE formation.
What about the natural history of matting, there is evidence of its spontaneous resolving over time. Also, treatment with microsclerotherapy was discussed, considering that it may lead to even smaller matting. 9 In the current study, patients were not followed for more than 3 months so no conclusions could be drawn about the spontaneous resolution of secondary TAEs.
The study’s main limitation is the small sample size reflected in large confidence intervals and the limited possibility of finding significant risk factors. The number of limbs with moderate to high amounts of new TAEs was low, and a separate analysis of predictors was not allowed. Also, the demographic and clinical data limited the possible risk factors of mating, so no specific predictors, except age, were detected. The other possible anatomical and procedure-related risk factors, such as limb size, the depth of the GSV from the skin surface, the tumescent anesthesia technique, including the number of skin punctures along the line of the treated vein, the total volume of tumescent solution were not available for the analysis. The short follow-up period of 3 months restricted the evaluation of the natural history of this phenomenon. Also, the study is limited by the subjective assessment of the TAE by photos. Along with that, an almost perfect inter-rater agreement was detected. Finally, the study had a pilot nature without preliminary sample size calculations due to the absence of actual data on secondary TAE development after EVLA in the current literature.
Conclusions
Secondary TAEs on the medial aspect of the thigh after GSV laser ablation could be detected in 21.1% of lower limbs. Their amount is low in 17.9% of cases, moderate in 2.4%, and high in 0.8%. Older age is the only risk factor for its development.
Footnotes
Author contributorship
DB, VK, AF, RT and KL researched literature and conceived the study. DB and RT collected the data. MG made a statistical analysis. DB, VK, AF, RT and KL wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Denis Borsuk.