
Abstract
Background
Stent patency is a critical outcome after thrombolysis, thrombectomy and stenting of subacute thrombotic iliac vein lesions (TIVL) and there is currently no consensus regarding post-procedural antithrombotic therapy. This study aims to investigate the differences between anticoagulant combined with antiplatelet therapy (dual-pathway inhibitors therapy, DPI) and anticoagulant therapy alone (AC) in reducing the incidence of occlusion after stenting for subacute TIVL.
Methods
A retrospective cohort study collected data from patients treated with stent insertion for iliac vein lesion (IVL) after thrombolysis and thrombectomy from June 2018 to December 2022. 180 patients were included based on inclusion and exclusion criteria, and were divided into two groups based on their antithrombotic prophylaxis: the DPI group and the AC group. A 1:1 propensity score matching (PSM) was performed to balance confounding covariates between the groups. Risk factors for the primary stent patency were assessed with univariate and multivariate Cox regression. Kaplan-Meier analysis and log-rank tests were used to evaluate survival difference.
Results
After PSM, 45 patients were included in the DPI and in the AC groups, and baseline characteristics were comparable. Cox regression analysis indicated that DPI therapy was associated with better primary stent patency (HR = 0.363, 95% CI: 0.149∼0.881) (p = .025). Kaplan-Meier curves showed that the 2-years primary stent patency rate in DPI group was 84.4% (38/45), while the rate in AC group was 62.2% (28/45), with a significant difference in survival between the groups (log-rank test p = .017). Only minor bleeding occurred in both cohorts, and event rates did not differ significantly between groups [(9/45) versus (5/45), p = .384].
Conclusion
For patients with subacute TIVL undergoing stent insertion, anticoagulant combined with antiplatelet therapy was associated with better stent patency compared to anticoagulant alone. This novel finding may have implications for optimizing medical management following venous stenting after endovascular therapy of subacute iliofemoral deep vein thrombosis.
Introduction
The main concern after iliac vein stenting is the patency of the stent.1,2 Unlike in acute thrombotic iliac vein lesion (TIVL), the stent patency rate in subacute TIVL is lower,3,4 likely due to the incomplete thrombus removal. 5 Antithrombotic management after stenting is important for the patency. Some researches indicated that combined antiplatelet therapy can improve stent patency rate.6–8 A global survey on thrombosis prevention after stenting found that 25% of respondents supported using a combination of anticoagulant and antiplatelet drugs. 9 Although there are no definitive guidelines on how to choose anticoagulant or antiplatelet drug after iliac vein stenting,10–12 but, with reference to existing studies,7,8,13 anticoagulant combined with antiplatelet therapy may be appropriate for patients with high risk of stent occlusion, especially the subacute TIVL. Therefore, this study conducted a retrospective cohort approach to evaluate the efficacy and safety of anticoagulant combined with antiplatelet therapy for subacute TIVL, aiming to provide further evidence to inform post-stenting antithrombotic regimens.
Methods
Study population
This retrospective cohort study collected clinical data from patients in two participating centers who were performed with iliac vein stent insertion between June 2018 and December 2022. The level of care in the two centers was similar, and both reached the standard of tertiary medical center. A total of 676 patients were analyzed. The inclusion criteria were as follows: (1) The first diagnosed disease with TIVL; (2) Characteristics with subacute thrombosis, indicated by angiography (showing a rough and uneven vein wall, organized thrombus, and collateral filling), and confirmed by practicing interventional radiologists, in spite of despite symptom duration ≤14 days. The exclusion criteria were as follows: (1) Characteristics with acute thrombosis; (2) Stent insertion performed for post-thrombotic syndrome (PTS); (3) Stent insertion performed for non-thrombotic iliac vein lesion (NIVL); (4) Lacking clinical data, or with less than 2 years of follow-up.; (5) Thrombophilia-related disorders. Five authors independently participated in patient selection. For cases with disagreement, especially those involving disputed data, three additional authors performed re-evaluation and made the final decision. The institutional review board of both participating centers evaluated and approved the present study. Informed consent was deemed unnecessary in view of the retrospective nature of the investigation.
A total of 496 patients were excluded from subsequent analysis for the following reasons: acute thrombosis (n = 285), with PTS (n = 52), with NIVL (n = 134), with incomplete data (n = 25). Therefore, 180 patients with iliac vein stenting for subacute TIVL were included in the analysis. The study flow diagram was shown in Figure 1. Flow chart of the study. After the inclusion and exclusion criteria, 180 patients met the criteria were enrolled in the study. NIVL: non-thrombotic iliac vein lesion; PTS: post-thrombotic syndrome; PSM: propensity score matching.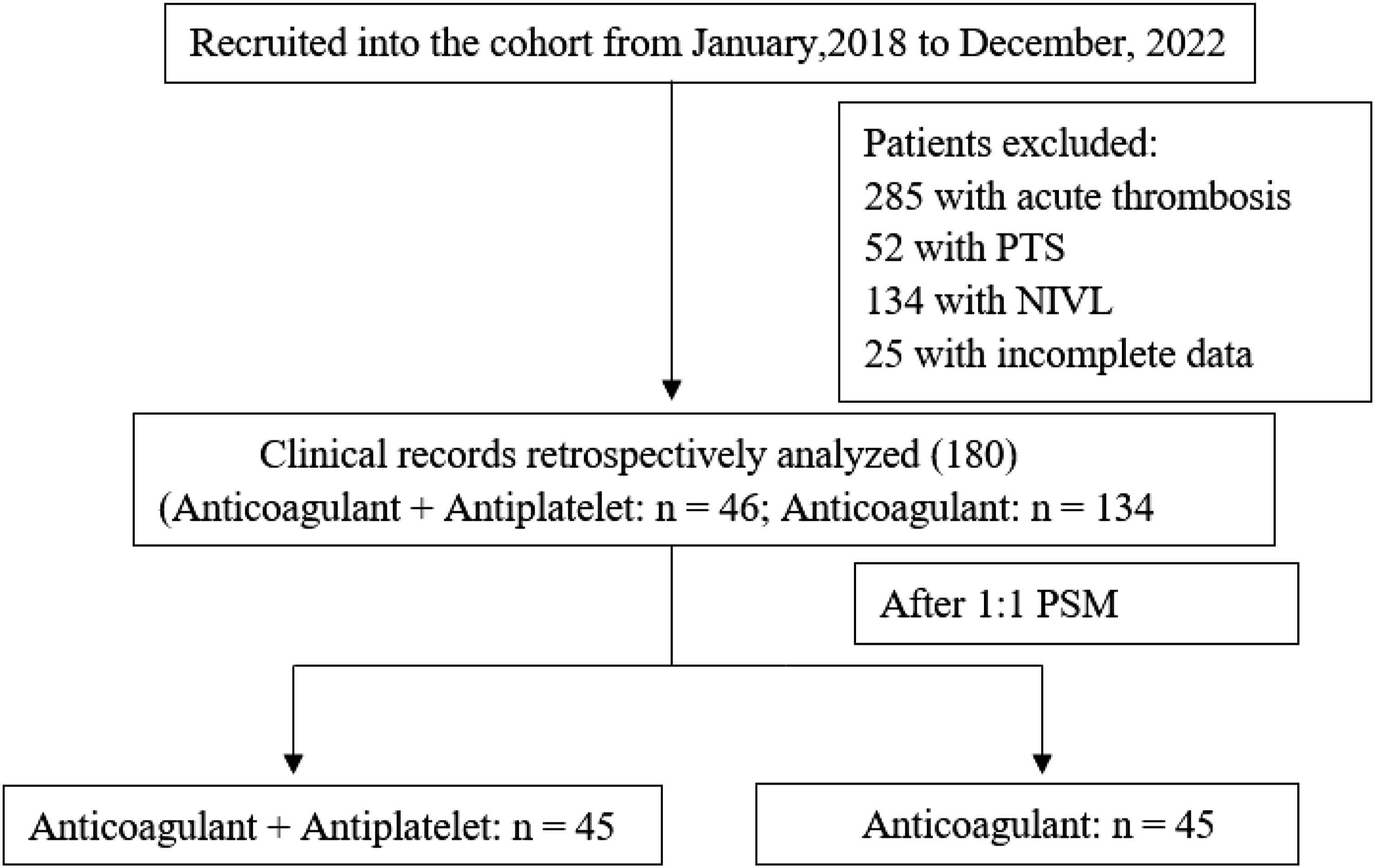
Stent insertion
The procedure was usually performed under local anesthesia. The access was obtained via ultrasound-guided puncture of the ipsilateral femoral vein or popliteal vein. A suitable length of the thrombolysis catheter was then introduced for continuous urokinase infusion (3 × 105 IU/12 h), with regular coagulation function checks. When the fibrinogen level was below 1.5, urokinase treatment was reduced, and if fibrinogen levels were below 1.0, thrombolysis was halted. AngioJet rheolytic thrombectomy (6F Solent catheter, Boston Scientific Corporation, Marlborough, MA, USA)—which utilizes high-velocity saline jets to create a Bernoulli effect for thrombus aspiration—was recommended for patients meeting ≥2 of the following criteria: (1) large thrombus burden; (2) preserved renal function; (3) acceptable cost coverage. After the catheter-directed thrombolysis (CDT), lesions pre-dilation was performed using balloon catheters (Mustang balloon, Boston Scientific, Marlborough, MA, USA) or (Armada balloon, Abbott Vascular, Lake Bluff, IL, USA) under fluoroscopic guidance. For lesions demonstrating ≥50% diameter stenosis of the iliac vein, stenting was performed with oversizing by 10%–20% relative to the adjacent normal venous diameter. The stent was positioned to ensure complete lesion coverage with <1 cm protrusion into the inferior vena cava. The multiple stents could be placed at the operator’s discretion based on the length of lesion. Similarly, stent type selection was also left to the operator’s discretion. (one case shown in Figure 2). A 67-year-old male patient with a 16-days history of left lower-limb swelling. (a, b) Venography showed the signs of thrombus, rough vessel wall and fine lumen. (c) Thrombectomy was performed with AngioJet and CDT was administered subsequently. (d) A 10 mm balloon was used for dilation and >50% narrowing was observed. (e) The post-procedure venography demonstrated the iliac vein remained obstructed. (f) After iliac vein stent insertion, venography demonstrated an improved luminal caliber, which demonstrated brisk flow real time.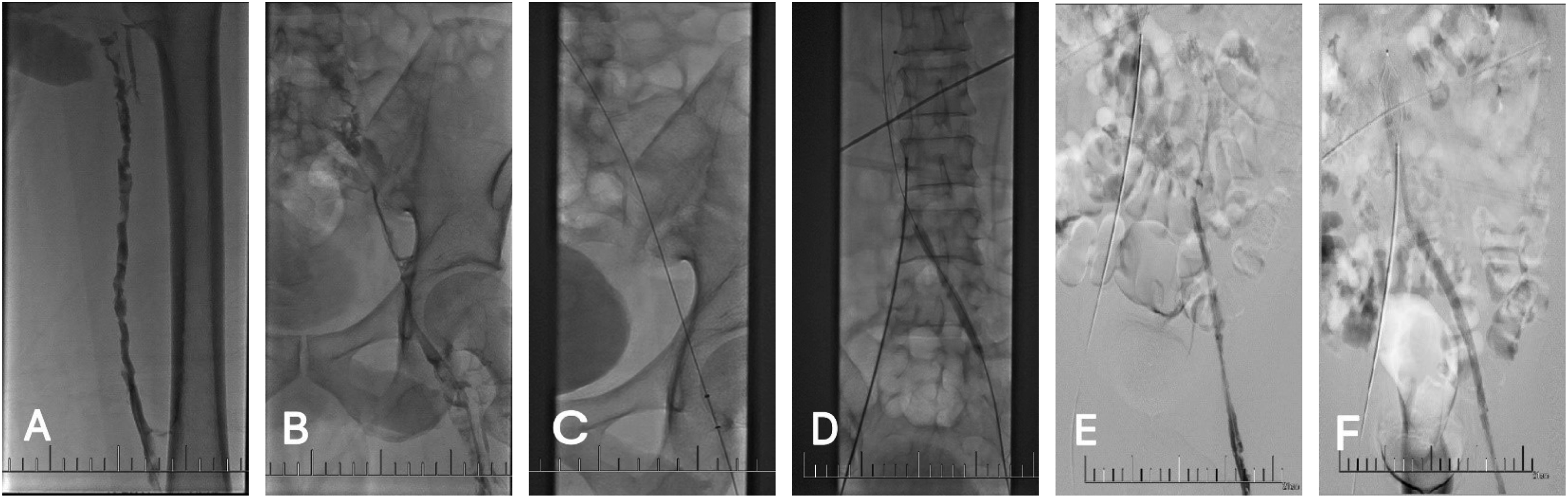
Outcomes and definitions
The primary outcome was the 2-years primary stent patency rate calculating from the date of surgery to the date of stents malfunction, which defined occlusion or stenosis more than 50%. The secondary outcome was the incidence of any major or minor bleeding according to the ISTH definitions. 14 The degree of thrombus removal was graded by calculating the percentage reduction in total thrombus score (difference of the baseline and post-procedural thrombus scores divided by the baseline scores), which was measured according to the Venous Registry Index and classified as follows: grade I (<50% reduction), grade II (50%∼90% reduction), and grade III (>90% reduction).
Antithrombotic therapy
In DPI group, rivaroxaban was administered (20 mg/d) for at least 6 months, combined with antiplatelet medication for at least 3 months (aspirin, 100 mg/d, or clopidogrel, 75 mg/d). Those who received a different Direct Oral Anticoagulant (DOAC) or Low Molecular Weight Heparins (LMWH) were still enrolled in DPI group. Those whose antiplatelet therapy did not meet the criteria described above, or who received anticoagulant therapy followed by antiplatelet therapy, were enrolled in the AC group. In AC group, rivaroxaban was also administered (20 mg/d) for at least 6 months. For patients with minor bleeding, the anticoagulant dose in both groups was reduced to (10 mg or 15 mg/d).
Follow-up observations
All patients were followed up by outpatient examination or telephone consultation at 3 months, 6 months, 1 year and 2 years after discharge. Ultrasound was routinely used to assess stent patency, and venography was often strongly recommended at 1 and 2 years after discharge. If symptoms worsened or stent failure was suspected at any time, patients were immediately hospitalized for further evaluation.
Statistical analysis
Data were analyzed by SPSS statistical software (Version 22.0). The PSM was conducted to match the potential bias of confounding covariates between the two groups. The following factors were used for matching: age, the duration of symptom, sex, hypertension, diabetes, the affected limb, BMI, combined pulmonary embolism, stenting timing, the diameter of stent, the number of stents, the thrombus clearance rate and the leg circumference difference during perioperative period (admission to discharge). To maximize the utilization of data, 1:1 nearest neighbor caliper matching without replacement was performed with a caliper value of 0.02. Chi-square test was used to compare categorical variables between DPI and AC group, with the x2-value reflecting the overall deviation between the observed and expected frequencies. Meanwhile, the student’s t-test was used for continuous variables, with the t-value reflecting the degree of difference between the means of samples. The primary stent patency curve was generated using Kaplan-Meier (K-M) estimates. The log-rank test was used to compare survival differences between groups. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using Cox proportional hazards regression models. Univariate Cox regression analysis and multivariate Cox regression analysis were conducted to assess factors associated with the primary stent patency. Variables with p value less than 0.1 in the univariate Cox analysis and the variables with clinical value (the duration of symptom, stenting timing, the number of stents, the thrombus clearance rate) were included in the multivariate Cox analysis.
Results
The general characteristics of involved patients before and after PSM.
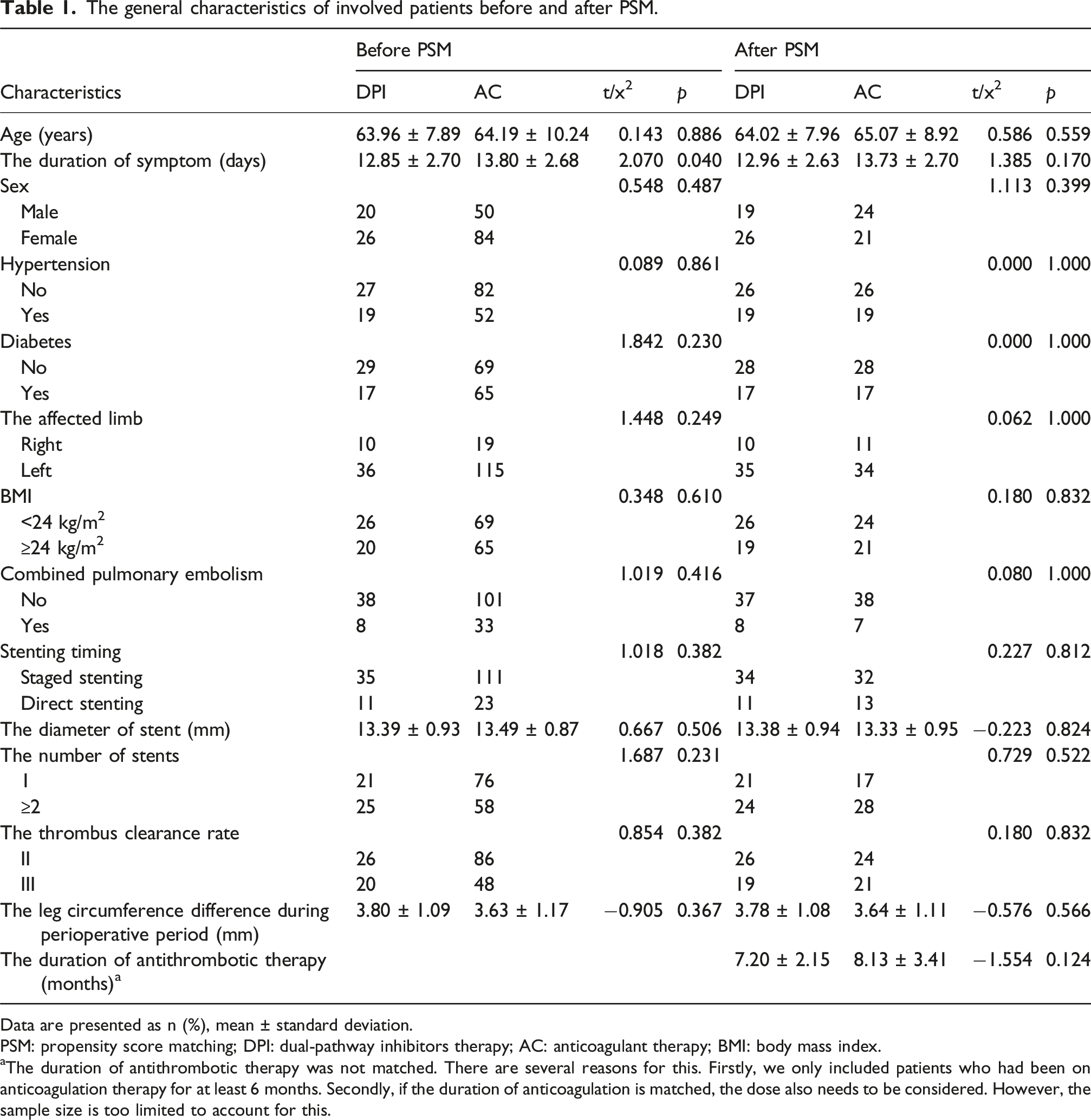
Data are presented as n (%), mean ± standard deviation.
PSM: propensity score matching; DPI: dual-pathway inhibitors therapy; AC: anticoagulant therapy; BMI: body mass index.
aThe duration of antithrombotic therapy was not matched. There are several reasons for this. Firstly, we only included patients who had been on anticoagulation therapy for at least 6 months. Secondly, if the duration of anticoagulation is matched, the dose also needs to be considered. However, the sample size is too limited to account for this.
Univariate and multivariate cox regression
Risk factors for 2-years primary stent patency before PSM.
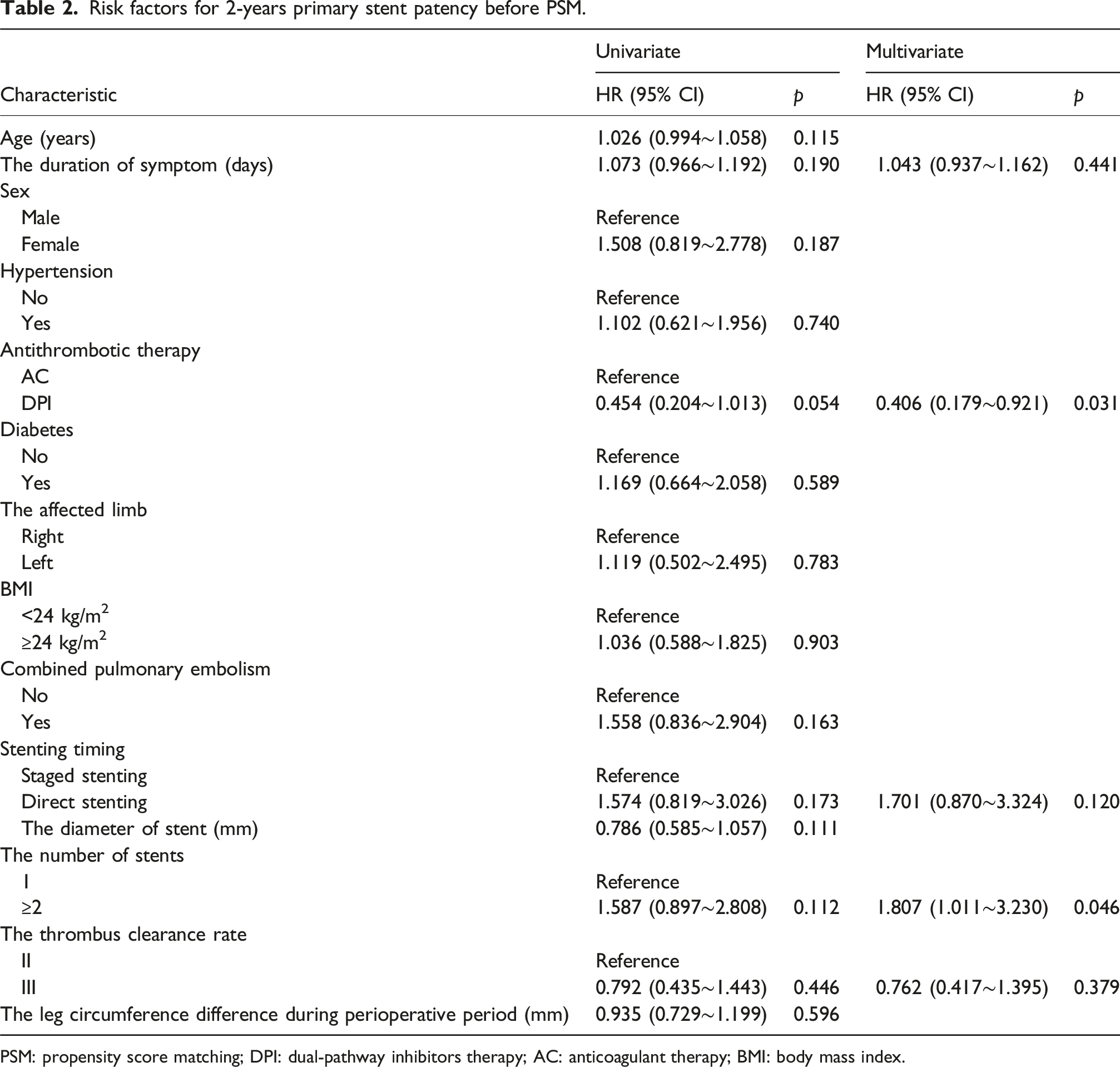
PSM: propensity score matching; DPI: dual-pathway inhibitors therapy; AC: anticoagulant therapy; BMI: body mass index.
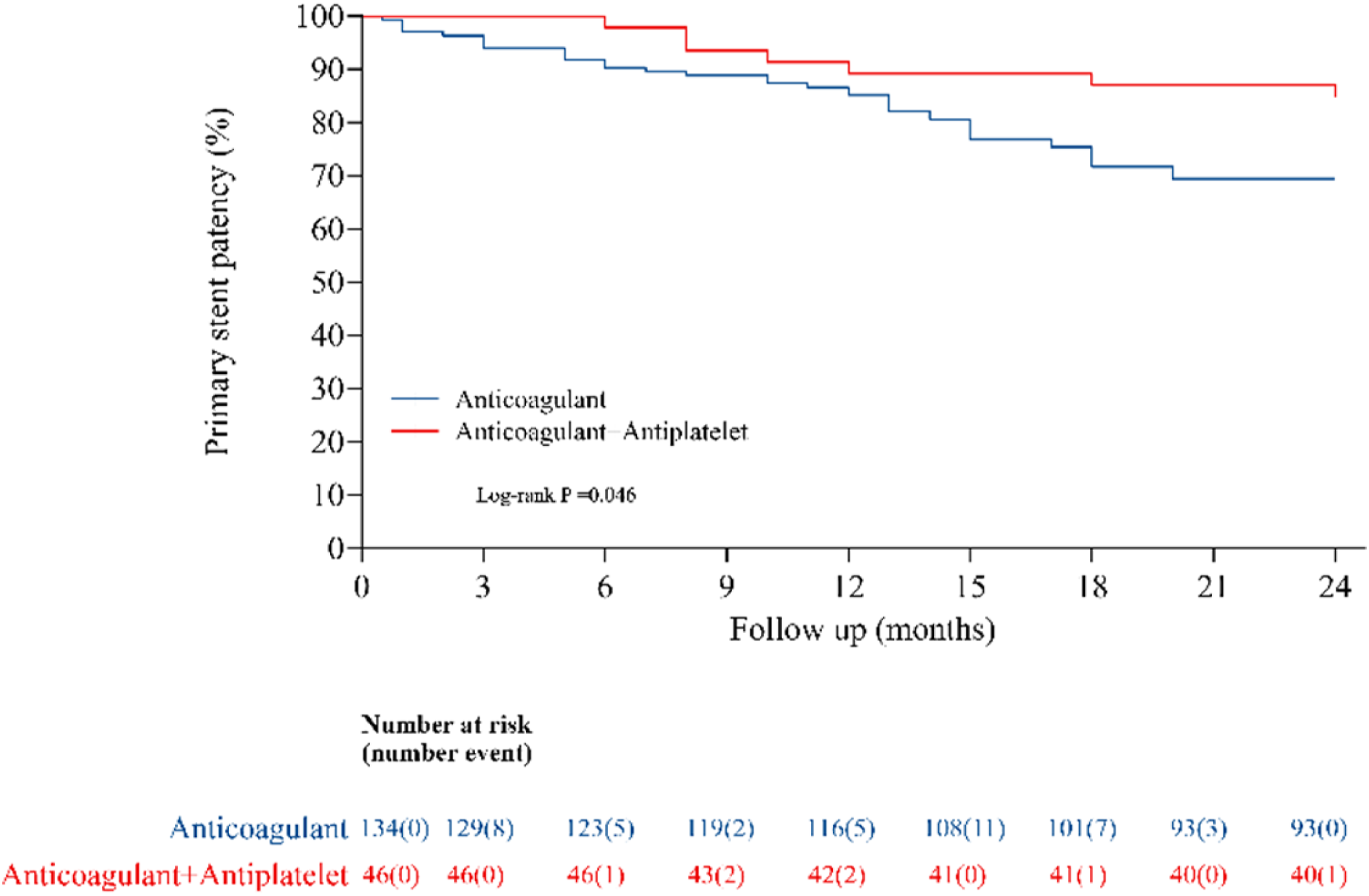
Before PSM, Cumulative Kaplan–Meier estimates of the primary stent patency (%) following different antithrombotic therapy after stenting in subacute thrombotic iliac vein lesion. The cumulative incidence during 2 years significantly reduced in anticoagulant + antiplatelet.
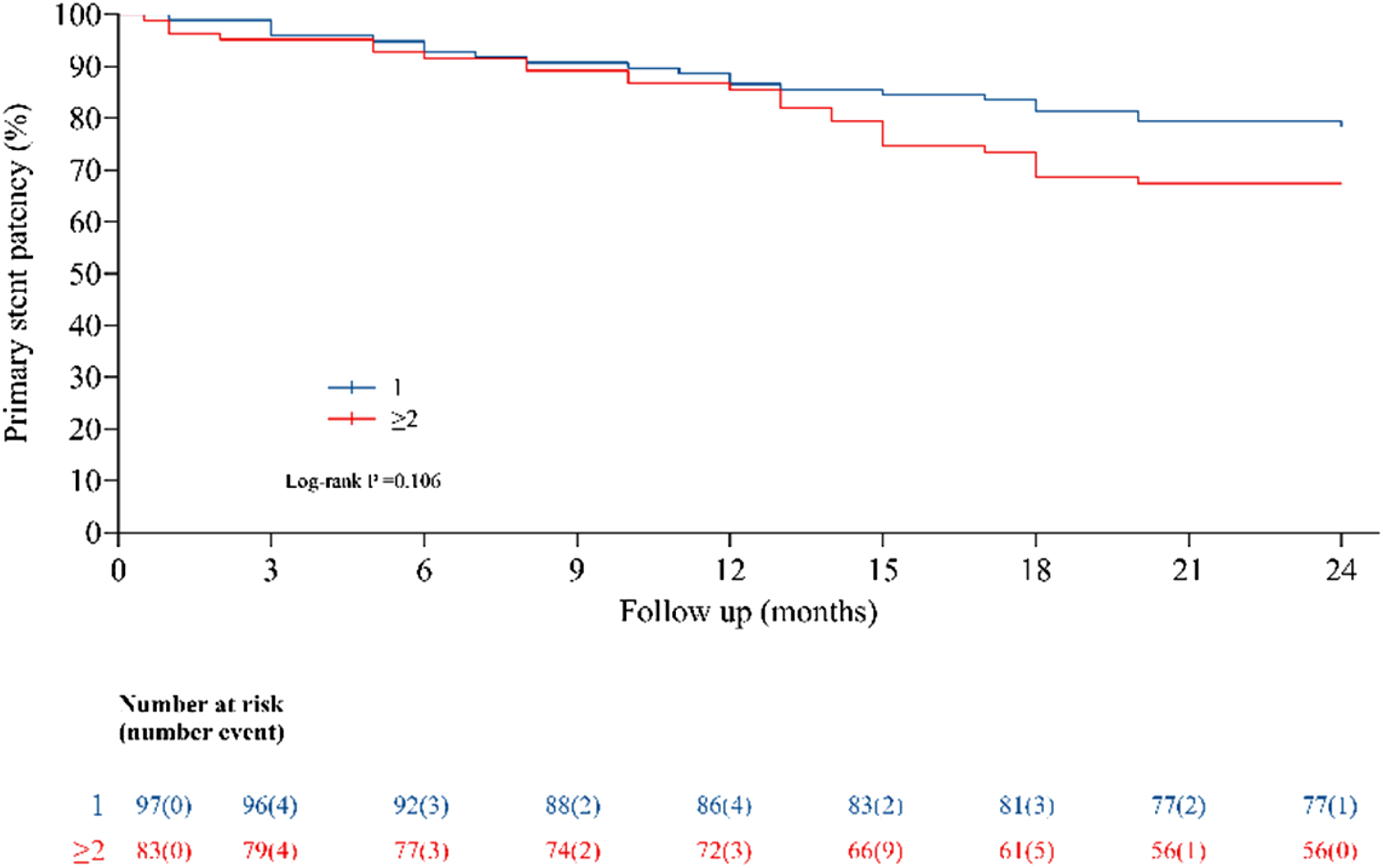
Before PSM, Cumulative Kaplan–Meier estimates of the primary stent patency (%) following the number of stents in subacute thrombotic iliac vein lesion. The cumulative incidence during 2 years was no significantly difference.
Risk factors for 2-years primary stent patency after PSM.
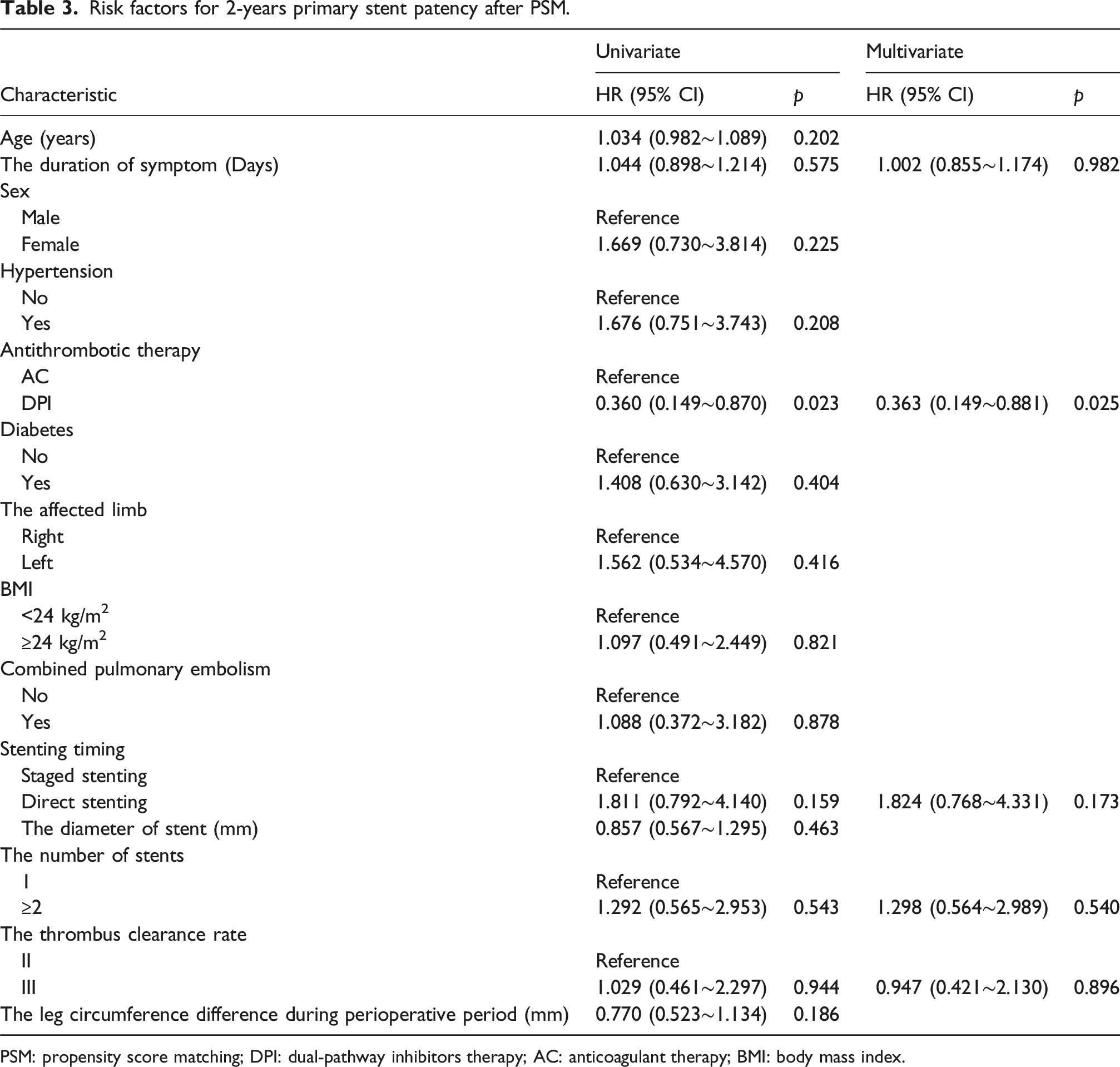
PSM: propensity score matching; DPI: dual-pathway inhibitors therapy; AC: anticoagulant therapy; BMI: body mass index.
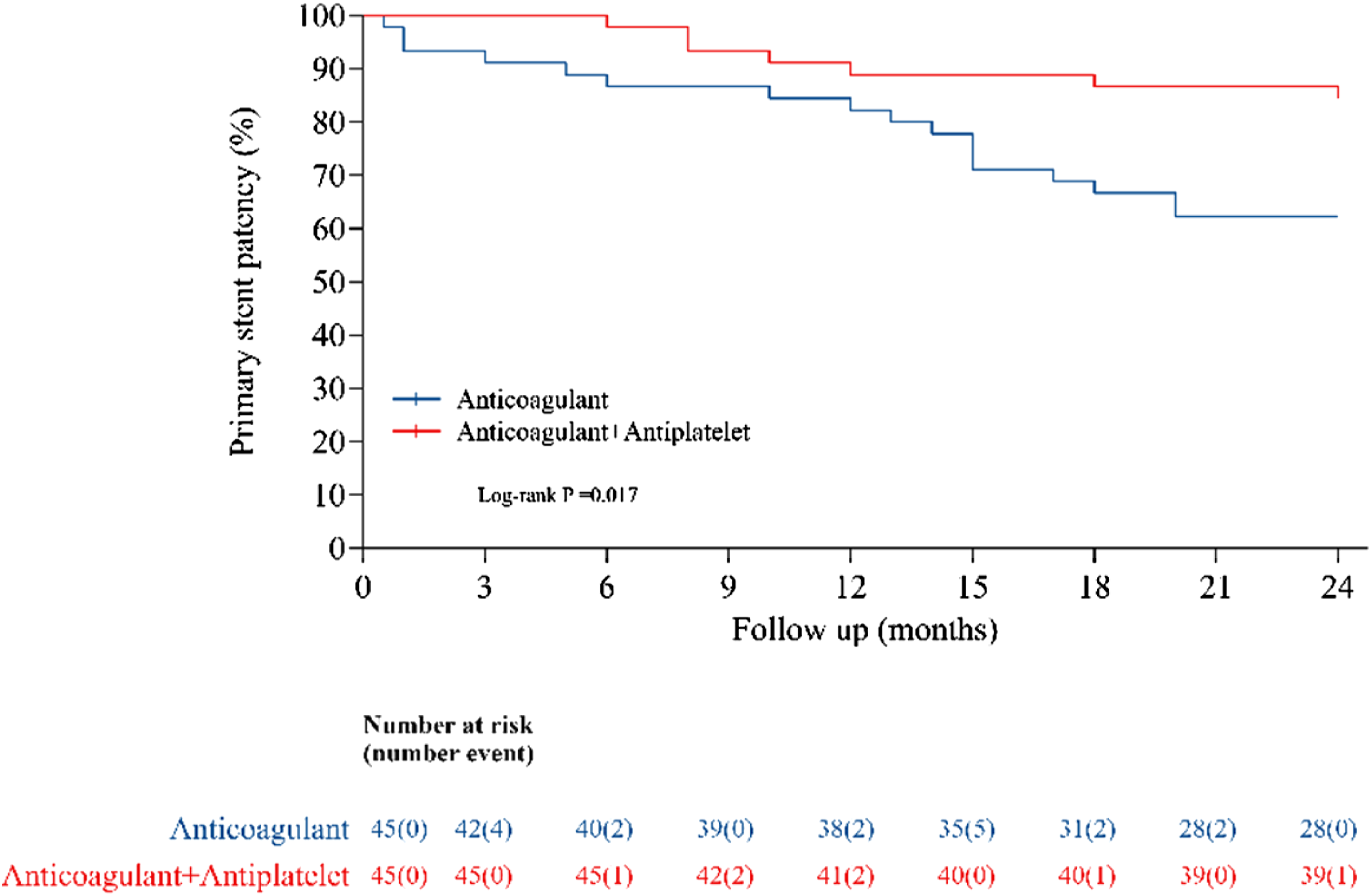
After PSM, Cumulative Kaplan–Meier estimates of the primary stent patency (%) following different antithrombotic therapy after stenting in subacute thrombotic iliac vein lesion. The cumulative incidence during 2 years significantly reduced in anticoagulant + antiplatelet.
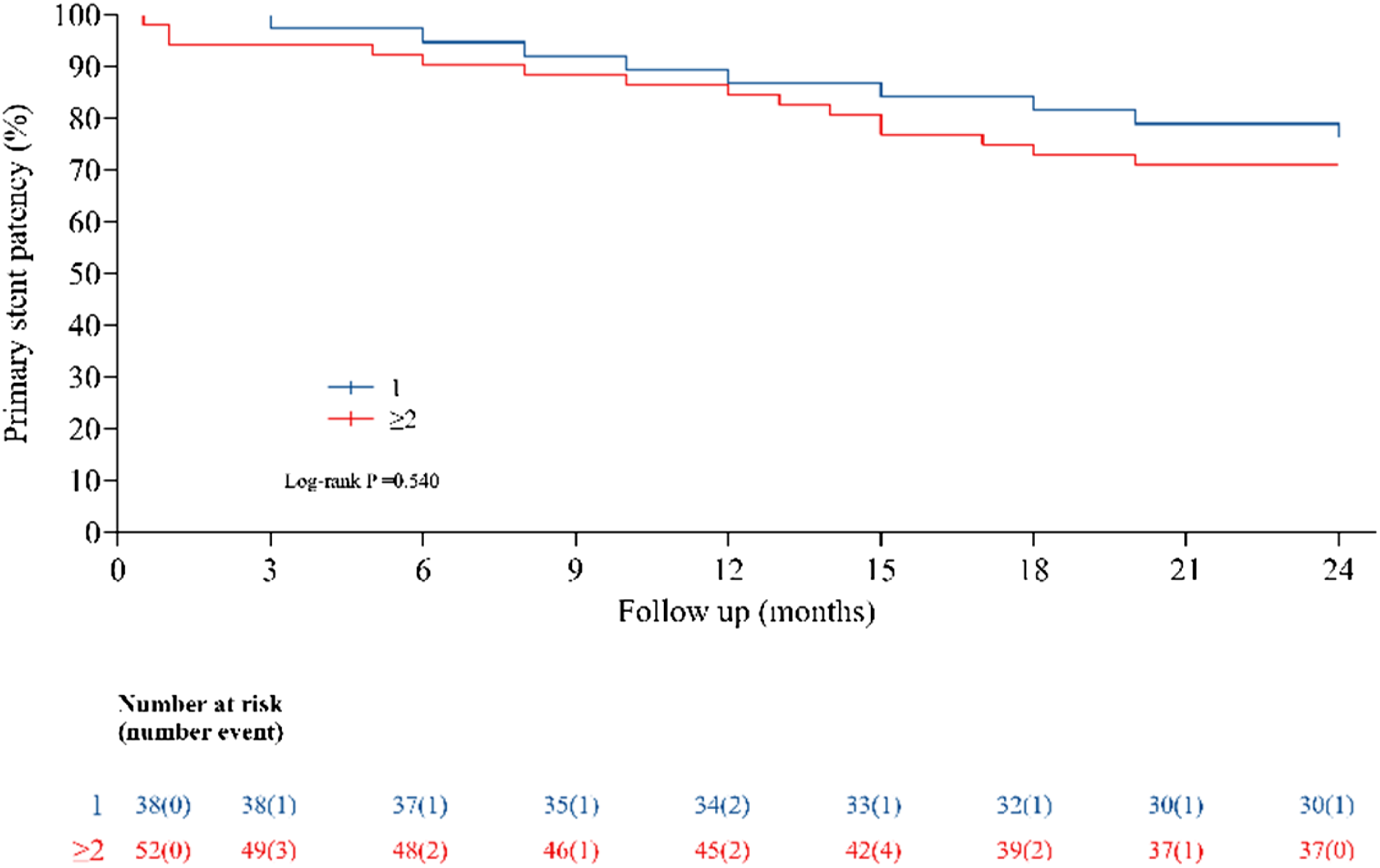
After PSM, Cumulative Kaplan–Meier estimates of the primary stent patency (%) following the number of stents in subacute thrombotic iliac vein lesion. The cumulative incidence during 2 years was no significantly difference.
There were 9 cases of minor bleeding (6 gingival, three urinary system) in DPI therapy group and 5 cases of minor bleeding (4 gingival, one rhinorrhagia) in AC group [(9/45) versus (5/45), P = .384]. All of them continued to receive anticoagulant at a reduced dose, and the bleeding improved. No major bleeding was reported.
Discussion
TIVL is a common lower extremity venous disease. However, many patients do not receive timely treatment during the acute phase, leading to partial thrombus organization and progression to the subacute phase. Few studies have examined whether antithrombotic strategies to maintain stent patency in acute TIVL should differ from strategies used for subacute TIVL. So, given the lack of institutional guidelines on the management with DPI or AC, we conducted this study. Our findings demonstrated that DPI therapy was associated with a higher primary patency rate compared to AC alone for subacute TIVL, even achieving a patency rate (84.44%) similar to that reported in the acute phase (85.2%). 15 This may underscore a critical gap in clinical practice, where delayed diagnosis of TIVL often leads to suboptimal outcomes.
One study conducted an immunological study on the thrombus formatted in iliac vein stenting in pigs, 16 revealing that the content of platelet at both the head and tail of the thrombus exceeded expectations, which may suggest a pharmacological backing to the findings from the present study. Another study identified two primary tissue types in stent-related stenosis 17 : thrombosis and diffuse intimal thickening (DIT). DIT was usually triggered by endothelial injury which initiated platelet aggregation. A recent review showed that activated platelets play a significant role in driving inflammation, thrombosis, and intimal hyperplasia through their surface receptors and secretory functions. 18 All of these findings provide potential theoretical support for the use of antiplatelet medications. But in clinical practice, evidence guiding post-procedural antithrombotic management is limited. 19 The decision to combine antiplatelet therapy relies on clinical judgment due to the lack of formal guidelines, particularly for subacute TIVL case.
Recently, the application of DPI in artery disease suggested that low-dose anticoagulant combined with antiplatelet therapy was associated with a lower rate of ischemic events, indicating the potential benefits of DPI. 20 However, this benefit hasn’t been extended to acute TIVL in which DPI therapy did not significantly increase long term patency.4,21 Meanwhile, in the treatment of PTS, one study found that DPI therapy for 6 months had a higher 5-years primary patency rate of 72%, without any major bleeding events. 22 Another study reported that patients who received DPI for at least 1 year, with clopidogrel discontinued after 2 months and aspirin continued indefinitely, had a 1-year primary patency rate of 88% and a 2-years primary patency rate of 62%, with no severe bleeding. 23 The DPI therapy did not seem to significantly improve patency rate in PTS patients, which was likely due to the poor inflow tract (anatomical classification Type 4). 24 In contrast, patients undergoing stenting for subacute TIVL typically had adequate inflow tracts, making antithrombotic prophylaxis in the stent outflow tract particularly crucial. In our study, the DPI group demonstrated significantly a higher 2-years primary stent patency rate compared to the AC group, indicating superior clinical efficacy. In terms of safety, there were no life-threatening bleeding events occurred and overall bleeding rates showed no statistical difference between groups.
In spite of the introduction of specialized iliac vein stents, there are still no clear consensus on the efficacy of specialized versus non-specialized iliac vein stenting in the subacute TIVL.25,26 In our study, the non-specialized stents were predominantly used, with only a limited number of specialized stents employed. The sample size will be expanded in future studies to enhance statistical power. Regarding the effect of direct versus staged iliofemoral stenting on stent patency, a cohort study reported 1-year primary patency rate of 93.5% in the direct group and 97.8% in the staged group (p = .323), showing no significant difference. 27 Our finding was consistent with this result. The multivariate Cox regression analysis showed no significant association between stenting timing and primary patency (HR = 1.824, p = .173). However, higher-quality studies with extended follow-up are still needed to evaluate the impact of stenting timing on stent patency, particularly in subacute TIVL.
On the other hand, the relationship between stent number (the greater the number, the longer the length) and patency rate warrants further investigation. Unlike in arterial disease, there is a consensus that longer stent length increases occlusion risk. Therefore, a “leave nothing behind” approach is recommended. In venous disease, one study suggested a potential association between stent length (particularly those extending into the common femoral vein) and stent occlusion, though this difference was not statistically significant. 28 However, another study involving patients with NIVL, PTS, and acute TIVL found that stent length did not increase the risk of in-stent thrombosis, though its 6-months follow-up period may limit the generalizability of the finding. 29 A clinical practice guideline on the management of chronic venous disease showed that good inflow and outflow tracts were important factors for stent patency. 30 In our study, the multivariate Cox regression analysis of pre-PSM indicated that the stent number was an influencing factor, but Kaplan-Meier survival analysis did not show statistical significance. After PSM, multivariate Cox regression analysis and Kaplan-Meier survival analysis did not suggest that the number of stents was an influencing factor. We believe that the importance of our results is to suggest that it may be safe to place a stent in a longer segment to cover the diseased segment without fear of sacrificing patency.
The link between inflammation and thrombosis has received increasing attention. 31 Meanwhile, the multifaceted role of platelets in inflammation is increasingly recognized, 32 these may also explain the higher patency rate in the DPI group. Because the patients in our study did not have relevant inflammatory measures, there is no evidence to prove this theory at this time and this may be a critical area for future research.
As depicted in the paper, the current standard of care for treatment of subacute TIVL is variable in terms of antithrombotic therapies, stent types, techniques (direct vs staged stenting), the stent number and the influence of inflammation. While the present study does come with limitations, it sheds light on the possible beneficial effects of DPI therapy without significant risks in bleeding.
There were some limitations in this study that need to be highlighted. First, it was a retrospective study with a small sample size. Second, potential selection bias—due to the multi-center nature of this study and the lack of a standardized protocol—may affect the reliability of the conclusion. Third, the assessment of duration of use of antithrombotic agents, dosage schedule of antithrombotic agents, the use of other medications and possible drug interactions were not evaluated due to the limitations in data availability. Fourth, due to limited use of intravascular ultrasound (IVUS) in China, we only assessed residual thrombus and positioning of stents by venography at present. Fifth, at present, it is impossible to precisely define subacute TIVL, we used angiography to make the distinction between acute and subacute TIVL, which we acknowledge is not precise. In future studies, MRI or IVUS may be considered for a more precise assessment.
Conclusion
Anticoagulant combined with antiplatelet therapy may be superior to anticoagulation alone in maintaining 24-months stent patency in patients with subacute TIVL.
Supplemental Material
Supplemental Material - Anticoagulant combined with antiplatelet therapy is associated with improved iliac vein stent patency following thrombolysis and thrombectomy of subacute iliofemoral deep vein thrombosis: A retrospective propensity score matching cohort study
Supplemental Material for Anticoagulant combined with antiplatelet therapy is associated with improved iliac vein stent patency following thrombolysis and thrombectomy of subacute iliofemoral deep vein thrombosis: A retrospective propensity score matching cohort study by Huang Tianan, Yu Yin, Lihua Huang, Yong Lu, Jun Yang, Xiaodong Jiang, Chen Zhuo, Hong Xin in Phlebology
Footnotes
Acknowledgements
We would like to thank Kaiwen Chen for her kind help in the preparation of manuscript.
Ethical considerations
The study was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committees of the The Affiliated Hospital two of Nantong University (2024KT363).
Author contributions
Tianan Huang: Methodology, Formal analysis, Software, Visualization, Writing-original draft. Yu Yin and Lihua Huang: Methodology, Supervision, Writing-review & editing. Yong Lu: Methodology, Supervision, Writing-review & editing, Project administration. Jun Yang and Xiaodong Jiang: Investigation, Supervision, Project administration. Zhuo Chen: Investigation, Formal analysis, Validation. Xin Hong: Conceptualization, Writing-review & editing, Supervision, Validation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Nantong City Health Commission’s scientific research Project (QN2024018, MS2024037), the Nantong University Special Research Fund For Clinical Medicine (Grant No. 2024LQ015). the Nantong Municipal Bureau of Science and Technology Project (No. MSZ2023156).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Xin Hong.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.