
Abstract
Background
The objective of this study was to compare the efficacy and safety of endovenous microwave ablation (EMA) and high ligation and stripping (HLS) for the treatment of small saphenous vein insufficiency..
Methods
This single-center retrospective study consecutively enrolled patients with small saphenous vein insufficiency who underwent either endovenous microwave ablation (EMA) or high ligation and stripping (HLS). Clinical severity was assessed using the Clinical-Etiology-Anatomy-Pathophysiology (CEAP) classification and the Venous Clinical Severity Score (VCSS). Quality of life was evaluated using the Aberdeen Varicose Vein Questionnaire (AVVQ) and the Chronic Venous Insufficiency Questionnaire-14 (CIVIQ-14). Perioperative complications and vein closure rates were recorded. The primary outcome was technical and anatomical vein closure at 6 and 12 months postoperatively. Secondary outcomes included operative time, postoperative complications, symptom improvement, and quality-of-life changes. Propensity score matching was performed to minimize baseline confounding between groups.The objective of this study was to compare the efficacy and safety of endovenous microwave ablation (EMA) and high ligation and stripping (HLS) for the treatment of small saphenous vein insufficiency.
Results
Following propensity score matching (PSM), the baseline characteristics between the two groups were comparable. EMA demonstrated a significantly shorter operative time compared to HLS (p < 0.001). Improvements in both symptoms and clinical severity scores were significantly greater and occurred more rapidly in the EMA group (p < 0.01). Regarding postoperative complications, the incidence rates of paresthesia and numbness were significantly lower in the EMA group compared to the HLS group (p < 0.05). However, improvements in health-related quality of life and 12-months safety indicators showed no significant differences between the two groups (p > 0.05).
Conclusion
The study findings confirm that endovenous microwave ablation (EMA) significantly improves quality of life in patients with small saphenous vein (SSV) insufficiency. Compared to high ligation and stripping (HLS), EMA demonstrates superior minimally invasive characteristics, facilitates faster recovery, and provides better symptom relief within the first year post-procedure. Furthermore, its long-term safety profile is non-inferior to HLS, collectively resulting in higher patient satisfaction.
Keywords
Introduction
Lower extremity venous varicosities (LEVV) represent a prevalent manifestation of chronic venous insufficiency (CVI). The underlying pathological basis is dysfunction of venous valve closure 1 Epidemiological data indicate that approximately half of the adult population experiences mild venous insufficiency, with typical varicose veins observed in about 15% of men and 35% of women.2,3 The clinical features of this condition are significant; patients commonly report sensory symptoms such as lower limb pain, burning sensations, and pruritus, frequently accompanied by heaviness and nocturnal muscle cramps. 4 From an anatomical distribution perspective, the great saphenous vein (GSV) is the primary site involved in superficial venous insufficiency of the lower extremities. Notably, primary small saphenous vein (SSV) insufficiency is observed to play an independent pathogenic role in approximately 20% of cases. 5 The saphenopopliteal junction (SPJ) is typically located 1-2 cm proximal to the popliteal skin crease, visualized in approximately 83% of anatomical dissections, with only 62% exhibiting a normal termination pattern. A common trunk variation with the medial gastrocnemius vein is present in about 25% of cases. The SSV is accompanied along its distal course by the sural nerve. Furthermore, anatomical variations in the SPJ region – including its location, drainage pattern, and common trunk formations – render surgical treatment of the SSV significantly more complex compared to the GSV.6,7 Therefore, accurate diagnosis and management of the SSV are crucial for symptom relief.
Regarding treatment modalities, the traditional high ligation and stripping (HLS) procedure, recognized for its definitive efficacy and technical simplicity, remains a fundamental surgical approach for CVI. Currently, the application of minimally invasive endovenous techniques, such as ultrasound-guided foam sclerotherapy (UGFS), thermal ablation (including radiofrequency ablation (RFA), endovenous laser ablation (EVLA), and endovenous microwave ablation (EMA)), and non-thermal ablation (such as mechanochemical ablation (MOCA) and cyanoacrylate closure), provides options for enhanced precision and reduced invasiveness in the treatment of lower extremity venous disorders.8,9 Compared to the robust evidence base available for GSV interventions, comparative studies evaluating different treatment modalities for SSV remain relatively scarce. Notably, the European Society for Vascular Surgery (ESVS) guidelines identify EMA as one of the effective treatment options for varicose veins. 10 Therefore, this single-center retrospective cohort study aimed to compare endovenous microwave ablation (EMA) with high ligation and stripping (HLS) for the treatment of small saphenous vein incompetence, with a focus on procedural efficacy, perioperative safety, and health-related quality-of-life outcomes.
Materials and Methods
Data collection
This single-center retrospective cohort study (conducted in accordance with the STROBE statement) was carried out in the Department of Vascular Surgery, Affiliated Hospital of Chengdu University of Traditional Chinese Medicine between January 2020 and January 2024. The study protocol received approval from the Institutional Ethics Committee (Approval No.: 2024KL-249). Consecutive screening of all patients diagnosed with primary small saphenous vein (SSV) varicosities (CEAP clinical class C2-C6) undergoing intervention was performed via the hospital electronic medical record (EMR) system.
Inclusion Criteria:1.Age between 18 and 90 years. 2.Presence of at least one venous-related symptom (e.g., pain, swelling, skin changes). 3.Ultrasound confirmation of:Small saphenous vein (SSV) trunk diameter >4 mm, and SPJ reflux duration >0.5 s 4.Patent deep venous system (peak flow velocity >30 cm/s). 5.Signed informed consent obtained and completed follow-up.
Exclusion Criteria:1.History of concurrent or prior deep vein thrombosis (DVT) or pulmonary embolism (PE). 2.Patients with recurrent varicose veins. 3.Critical limb ischemia (ankle-brachial pressure index, ABPI <0.8). 4.Carriers of cardiac implantable electronic devices (e.g., pacemakers, implantable cardioverter-defibrillators (ICDs)). 5.Chronic anticoagulation therapy (e.g., warfarin, rivaroxaban). 6.Pregnant or lactating women. 7.Inability to comply with follow-up or questionnaire assessments. 8.Life expectancy <1 year (due to advanced malignancy or end-stage organ failure). 9.Active non-melanoma skin cancer or other malignancy requiring ongoing active treatment.
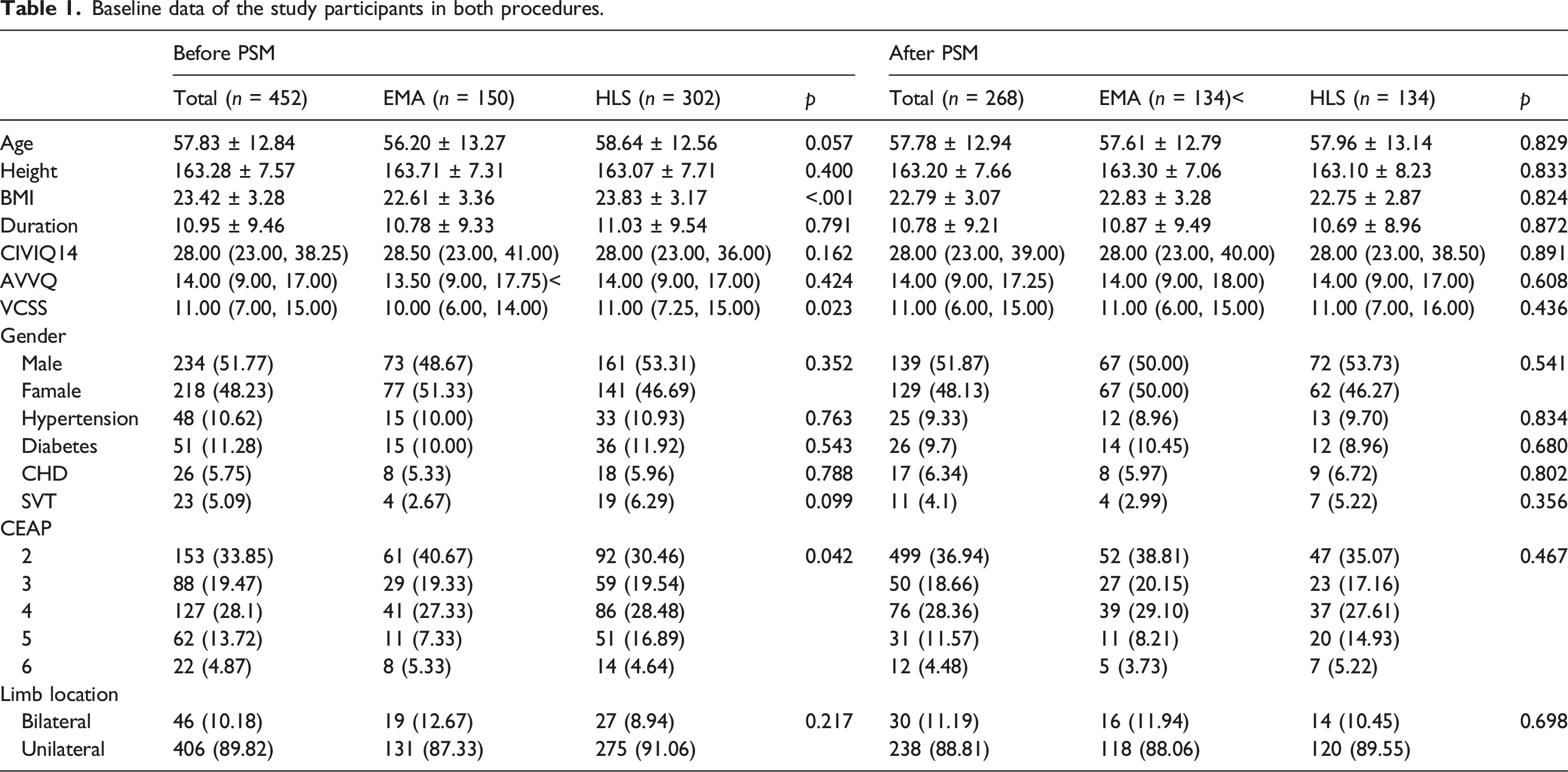
A total of 452 patients were initially enrolled, allocated to the endovenous microwave ablation group (EMA, n = 150) and the conventional high ligation with stripping group (HLS, n = 302). After propensity score matching (PSM), 134 patients were retained in each treatment cohort (EMA: n = 134; HLS: n = 134). All source data underwent blinded independent review via the Picture Archiving and Communication System (PACS) to ensure standardized extraction of imaging parameters.
Procedures
All interventions were performed under ultrasound guidance in accordance with the European Society for Vascular Surgery (ESVS) guidelines for venous treatment. 10 Preoperative duplex ultrasound mapping was performed to delineate the small saphenous vein anatomy, identify reflux sources, and plan the intervention. 11
EMA Procedure:Under real-time duplex ultrasound guidance, venous access was obtained by percutaneous puncture of the SSV trunk at the mid-to-upper calf, approximately 10–15 cm distal to the popliteal crease, selecting a straight and superficial segment while avoiding major perforators and adjacent nerves.After adequate local anesthesia, a microwave ablation catheter12,13 (Model: ECO-100F-2016, Φ2.0 × 1600 mm; Nanjing Yigao Medical Technology) was inserted via Seldinger technique at 2 cm distal to the SPJ. Tumescent anesthesia solution (500 mL normal saline +15 mL 1% lidocaine +0.5 mL epinephrine +10 mL sodium bicarbonate) was infused to establish a 10 mm perivenous fluid barrier, Tumescent volume was limited to one bottle per unilateral case and two bottles per bilateral case. Ablation was performed at 55W power in 5-s cycles using a stepwise pullback technique at 1 cm increments to achieve SSV trunk closure. Proximal 2 cm segments underwent two additional ablation cycles. Immediate post-procedural ultrasound confirmed complete luminal occlusion (absence of Doppler flow signals).
HLS Procedure:Following satisfactory anesthesia, a 1 cm longitudinal incision was made ∼2 cm inferior to the popliteal crease along the ultrasound-mapped SSV course. The SSV trunk was isolated and exposed. High ligation was performed with proximal double ligation. A stripping device was then inserted retrogradely through the distal end and advanced to the mid-calf ultrasound marker. The distal vessel was divided via a 5 mm stab incision, and the stripping device was exteriorized proximally for complete stripping of the proximal/mid SSV segment. Focused compression was applied along the venous pathway for hemostasis control.
Common Procedures:Both groups underwent intraoperative foam sclerotherapy for residual tributaries using polidocanol. 14 The foam was prepared via the Tessari method (1% solution, 1:4 liquid:air ratio), with 1 mL injected per puncture site. The maximum foam volume per limb was capped at 8 mL. 10 This was combined with mini-phlebectomy through ≤3 mm stab incisions.Postoperative protocol included:Postoperatively, patients received prophylactic-dose low-molecular-weight heparin by immediate subcutaneous injection. Compression bandaging was applied for the first 48 h, followed by the use of Class II medical compression stockings (23–32 mmHg), which were worn continuously for 4 weeks.15–17
Quality Control: Ultrasound verification confirmed complete closure of the SSV trunk (impedance value >500 Ω for the ablation group; no residual lumen for the HLS group). All operators possessed >1,000 cases of experience with the same type of procedures. Standardized equipment was used (microwave generator: ECO-100C, frequency 2450 MHz, effective thermal field 15 mm).
Follow-up and outcome measures
Patients were followed regularly for 12 months after treatment. Follow-up evaluations were scheduled immediately postoperatively, at 48 h, and at 1, 3, 6, and 12 months. At each time point, duplex ultrasound examinations and clinical assessments were performed. For patients unable to attend in-person visits, follow-up data were obtained through telephone or online communication. These patients were instructed to undergo duplex ultrasound examinations at local hospitals, and the imaging reports were subsequently collected and reviewed by the study team.
Primary Outcome Measures Assessment: complete occlusion required closure of the entire treated target vein without discrete open segments exceeding 5 cm in length; occlusion failure was defined if the cumulative length of non-closed venous segments was >3 cm (whether a single segment or multiple segments).18,19 All assessments were performed by certified vascular surgeons under double-blinded conditions to ensure objectivity.
Secondary outcomes included systematically recorded postoperative complications according to the International Union of Phlebology (UIP) criteria, 20 clinical severity assessed using the Venous Clinical Severity Score (VCSS), and health-related quality of life measured using the Aberdeen Varicose Vein Questionnaire (AVVQ) 21 and the Chronic Venous Insufficiency Questionnaire-14 (CIVIQ-14),the CIVIQ-14 score is expressed as the global index score (GIS), calculated as (total score −14)/56 × 100.22,23
All assessment timepoints were synchronized with the primary outcome evaluations (postoperative 48 h, 1, 3, 6, and 12 months), with data collection performed under blinded conditions by trained (e.g., Mann–Whitney U test) were applied otherwise. Normally distributed quantitative data are expressed as mean ± standard deviation; non-normally distributed data are described as median (interquartile range). Categorical variables were compared between groups using the chi-square test. A p value ≤0.05 was considered statistically significant.
Results
1. Baseline data
Baseline data of the study participants in both procedures.
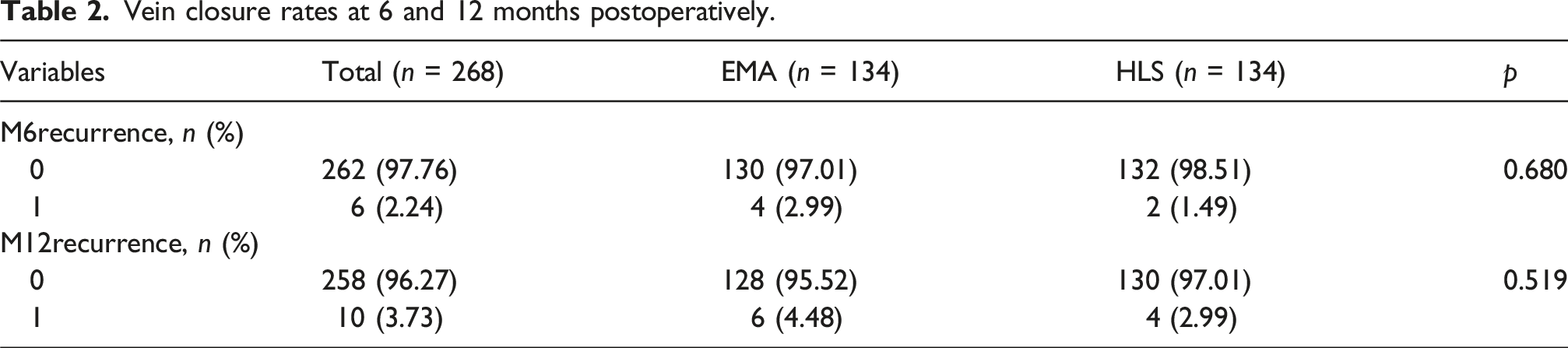
2. Primary endpoint: Vein closure rate
Vein closure rates at 6 and 12 months postoperatively.
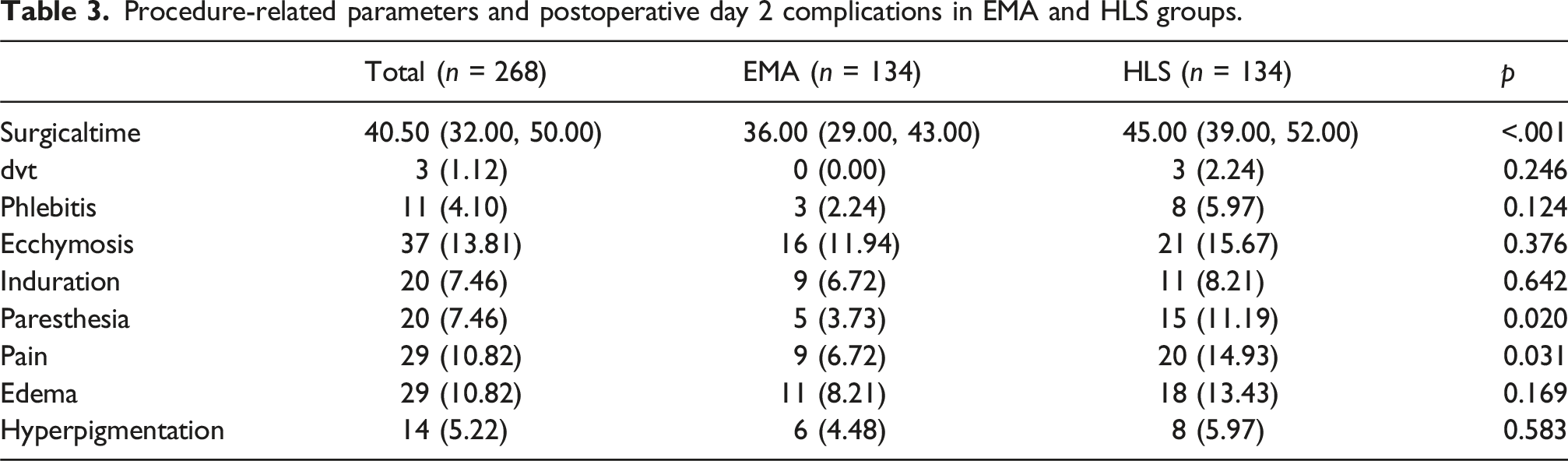
3. Perioperative Outcomes
Procedure-related parameters and postoperative day 2 complications in EMA and HLS groups.
4. Symptom and quality of life follow-up
The comparison of AVVQ,CIVIQ-14 and VCSS scores between the two groups.
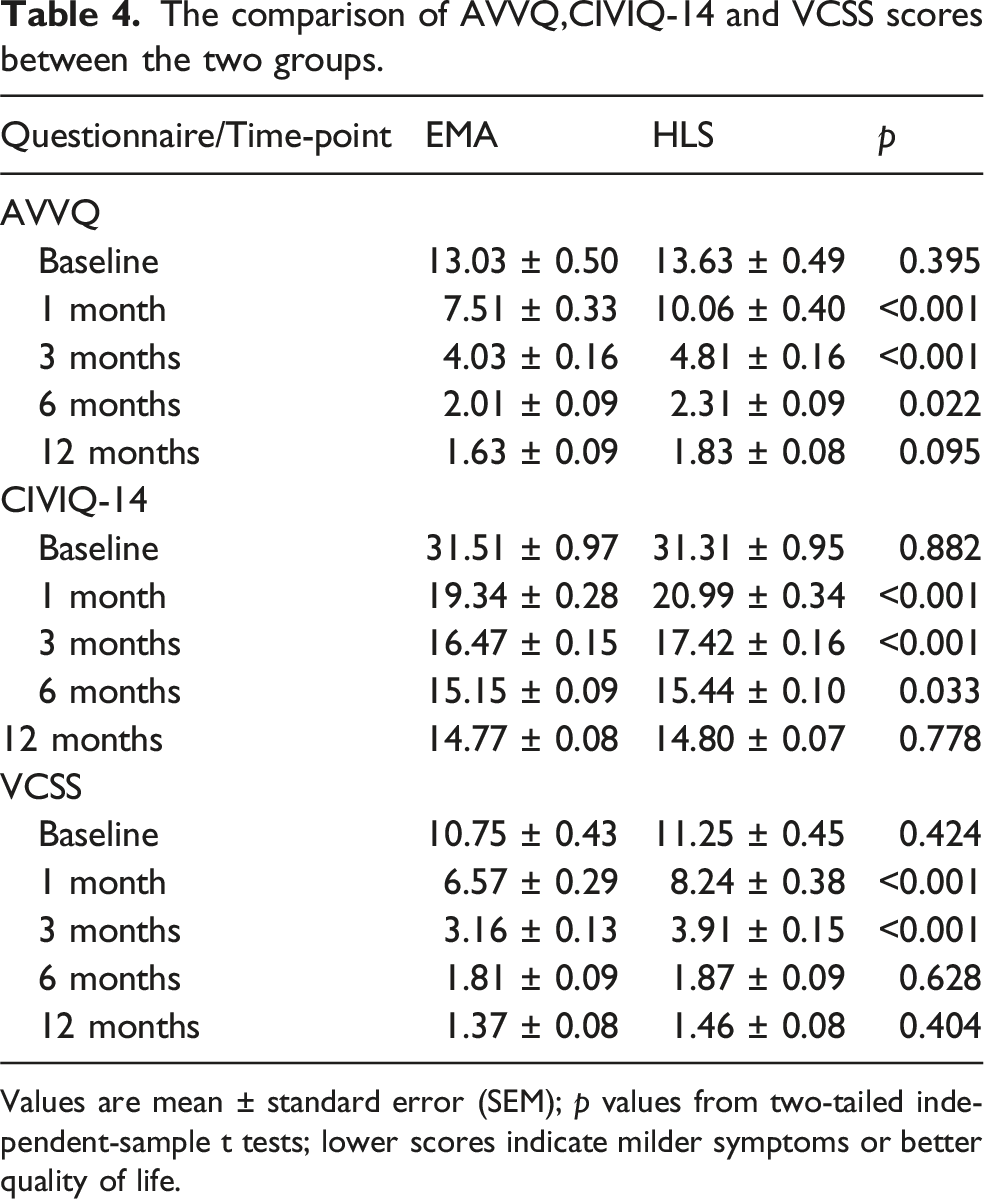
Values are mean ± standard error (SEM); p values from two-tailed independent-sample t tests; lower scores indicate milder symptoms or better quality of life.
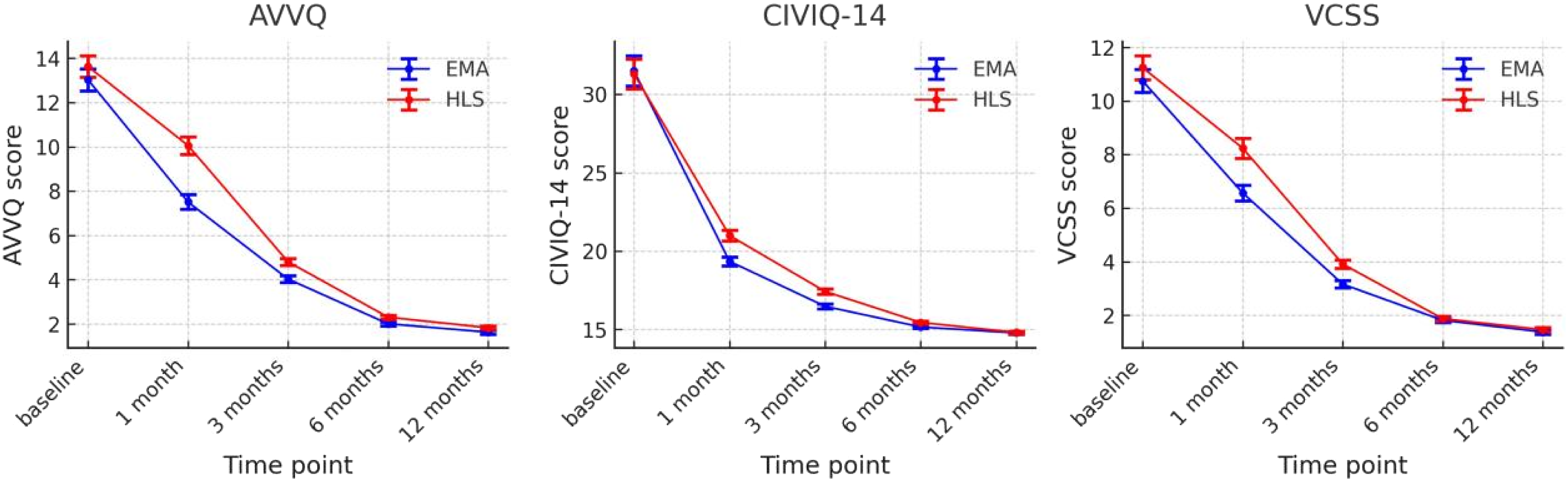
Follow-up changes in quality of life and clinical severity after percutaneous microwave ablation (EMA, blue) versus high ligation and stripping (HLS, red). (a) Aberdeen Varicose Vein Questionnaire (AVVQ) total score; (b) Chronic Venous Insufficiency Questionnaire-14 (CIVIQ-14) total score; (c) Venous Clinical Severity Score (VCSS).
Discussion
This study compared EMA with HLS for the treatment of small SSV insufficiency.The principal findings of this study indicate that EMA achieved comparable 6 and 12 months vein closure rates to HLS, was associated with a shorter operative time and lower early postoperative complication rates, and that both techniques resulted in significant improvements in symptom severity and quality of life during follow-up.
In terms of the primary endpoint, SSV closure rates at 6 and 12 months were high in both groups, with no significant differences between EMA and HLS. These findings suggest that EMA provides mid-term anatomical success comparable to conventional surgery. The closure rates observed in this study are consistent with previously reported outcomes for different treatment modalities in SSV disease. 24 For instance,a multicenter randomized trial comparing UGFS with EVLA in isolated SSV insufficiency reported similar clinical and anatomical outcomes. 25 Similarly, A randomized controlled trial comparing EVLA with conventional surgery showed that the complete elimination rate of SSV reflux was 96.2% in the EVLA group versus 71.7% in the conventional surgery group at 6 weeks. 26
With regard to nerve-related complications, the sural nerve runs in close proximity to the SSV, making it vulnerable to procedural injury. In the present study, the incidence of paresthesia was significantly lower in the EMA group compared with the HLS group, suggesting a reduced risk of nerve irritation or injury. In addition, postoperative pain was also significantly lower in the EMA group, further supporting its minimally invasive nature. These findings indicate that EMA may offer advantages in terms of early postoperative recovery and nerve-related outcomes.
In terms of symptom relief and quality of life, AVVQ, CIVIQ-14, and VCSS scores declined significantly in both groups during follow-up, reflecting marked clinical improvement. During the early postoperative period (1–3 months), scores on all three scales were lower in the EMA group than in the HLS group, indicating a faster improvement in symptoms and clinical severity with EMA. However, no significant between-group differences were observed at later follow-up time points.19,25 These results suggest that although EMA may facilitate more rapid early recovery, both treatments achieve comparable long-term improvements in overall health-related quality of life.
Both groups showed marked reductions in AVVQ, CIVIQ-14, and VCSS scores during follow-up, indicating substantial clinical improvement. Notably, AVVQ and VCSS scores were lower in the EMA group during early follow-up, suggesting a more rapid alleviation of symptoms and clinical severity. However, long-term health-related quality of life, as measured by CIVIQ-14, did not differ significantly between groups at later follow-up stages. These findings indicate that although EMA may offer faster symptomatic recovery, the long-term overall quality-of-life outcomes are comparable between the two treatment modalities.8,27,28
The potential advantages of EMA may be attributed to its mechanism of action. Microwave energy induces controlled thermal injury to the venous wall, leading to collagen contraction and irreversible occlusion while minimizing collateral tissue damage when performed under adequate tumescent protection. Standardized power settings and stepwise pullback techniques allow consistent energy delivery along the treated segment, contributing to reliable vein closure.
Advantages and limitations
This study utilized propensity score matching with standardized mean difference testing to confirm balance across baseline variables, thereby partially controlling for confounders and enhancing internal validity in intergroup comparisons. Simultaneously reporting patient-reported outcomes across three dimensions—VCSS, AVVQ, and CIVIQ-14—strengthens clinical interpretability. Limitations include: the single-center retrospective design may retain unmeasured confounders (e.g., venous diameter, operator experience); 12-months follow-up is insufficient to assess long-term recanalization and valve function recovery; exclusion of cost-benefit analyses and cosmetic appraisal; post hoc sample size estimation may lack power to detect differences in rare complications (Figure 2). Flow chart.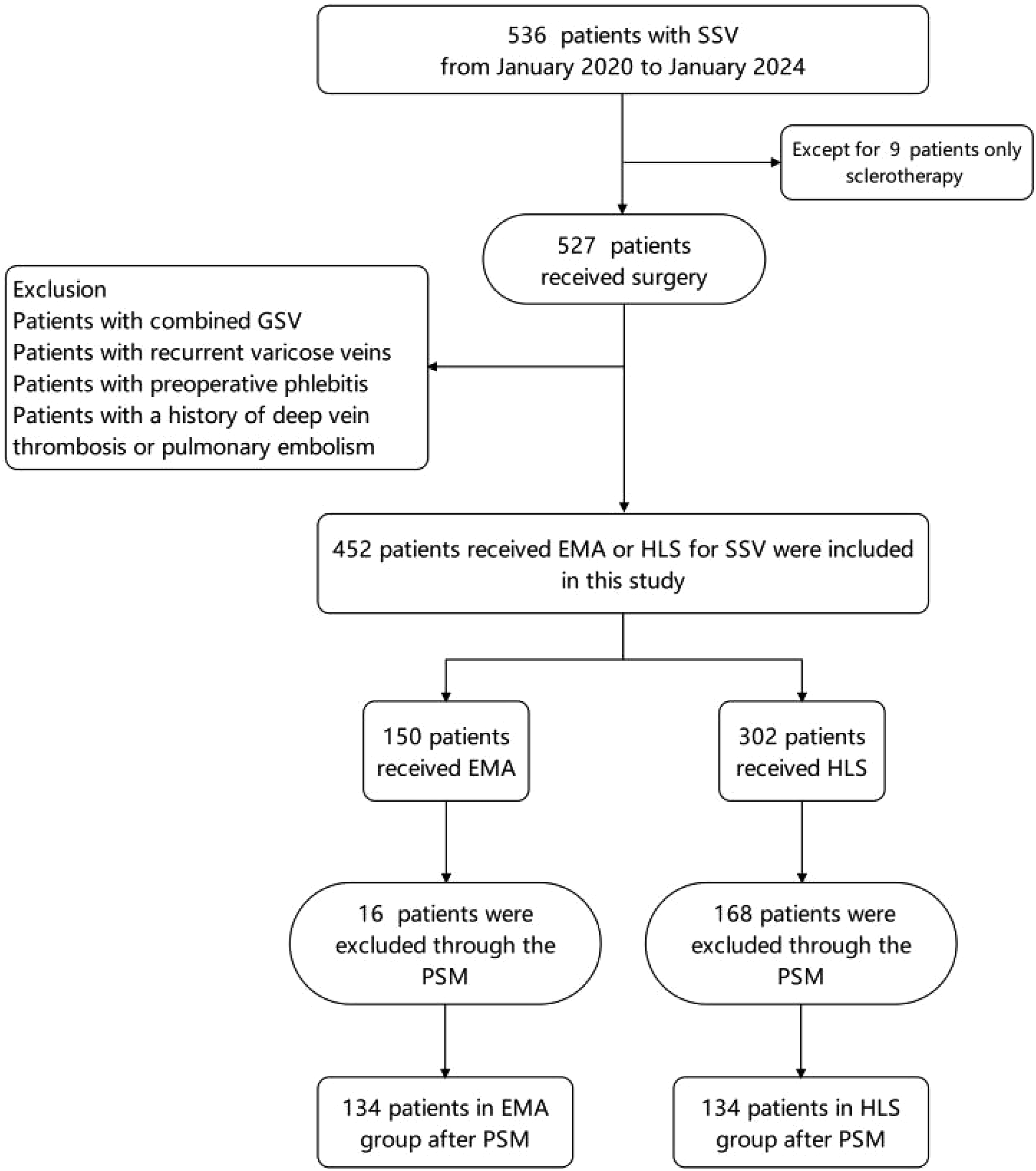
Conclusion
EMA represents an effective minimally invasive treatment option for SSV. In summary, EMA demonstrates superiority over conventional HLS in terms of symptom relief speed, operative time, and complication profile, while being not inferior to HLS in long-term health-related quality of life and safety.
Footnotes
Acknowledgements
We thank our colleagues from Vascular Surgery for their insightful discussions. Special thanks are due to Wei Zeng and Chun-shui He for their critical reading of the manuscript.
Ethical considerations
This study has been approved by the ethics committee of Hospital of ChengduUniversity of Traditional Chinese Medicine (Approval No. 2024KL-149).
Author contribution
Yao Lin and Li-feng Zhang contributed to the study conception and design. Material preparation and data collection were performed by Yu-qian Xie. Analysis was performed by Yu-qian Xie. The first draft of the manuscript was written by Yu-qian Xie and all authors commented on previous versions. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Wei Zeng and Chun-shui He are the guarantor for this work.