
Abstract
Objectives
Endovenous radiofrequency ablation (RFA) is an established minimally invasive treatment for saphenous vein insufficiency. This study evaluated 1-year clinical and anatomical outcomes of RFA in a real-world cohort, including staged adjunctive interventions when indicated.
Methods
This retrospective study initially evaluated 99 patients with symptomatic saphenous vein insufficiency. Of these, 84 patients, corresponding to 90 treated limbs, completed follow-up and were included in the final analysis. Among these, 74 patients underwent great saphenous vein (GSV) ablation (including 6 bilateral procedures, totaling 80 limbs), and 10 patients underwent small saphenous vein (SSV) ablation. Clinical outcomes were assessed using the Venous Clinical Severity Score (VCSS), while Clinical-Etiology-Anatomy-Pathophysiology (CEAP) classification was used to describe baseline disease severity.
Results
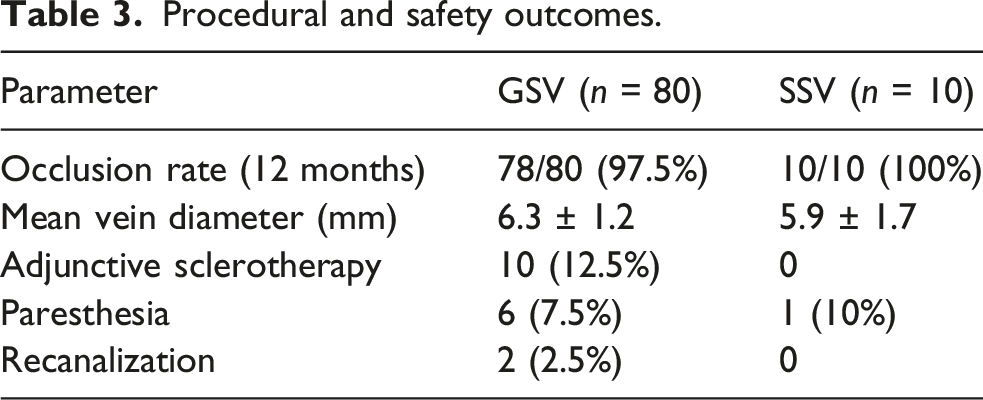
The overall occlusion rate across all treated limbs was 88/90 (97.7%). In the GSV subgroup, mean VCSS decreased significantly from 6.0 ± 1.5 at baseline to 2.2 ± 1.2 at 12 months (p < .001). In the SSV subgroup, mean VCSS decreased from 5.5 ± 0.5 to 2.0 ± 1.0, demonstrating comparable clinical improvement. Ten limbs (12.5% of the GSV limbs) required adjunctive sclerotherapy for symptomatic residual tributaries. Minor complications included transient paresthesia in 7 limbs (7.7%), all of which resolved during follow-up. One patient (1.2%) developed Ablation-Related Thrombus Extension (ARTE), which was managed conservatively without sequelae.
Conclusion
Endovenous RFA provided high occlusion rates, significant clinical improvement, and a favorable safety profile at 1 year. These findings support RFA as an effective treatment option for both GSV and SSV insufficiency in routine clinical practice.
Keywords
Introduction
Chronic venous disease (CVD) is a highly prevalent global health concern, affecting between 10% and 30% of the adult population. The global prevalence is projected to rise significantly due to an aging population and the increasing incidence of obesity.1–3 While the great saphenous vein (GSV) remains the primary focus of most clinical research, small saphenous vein (SSV) insufficiency is common and clinically significant, occurring in approximately 15% of patients. 4 The vast majority of clinical presentations involve symptomatic varicose veins (Clinical-Etiology-Anatomy-Pathophysiology (CEAP) C2–C3), which markedly reduce patient-reported quality of life and productivity.5,6
Historically, open surgical high ligation and stripping (HL/S) was the definitive therapeutic standard but is associated with greater postoperative morbidity and longer recovery compared with endovenous techniques. Consequently, minimally invasive endovenous thermal ablation methods, including radiofrequency ablation, have largely replaced surgery as first-line treatment in contemporary clinical practice.3,7,8
The introduction of minimally invasive endovenous thermal ablation techniques has fundamentally transformed the management of saphenous vein insufficiency over the last two decades. 9 Radiofrequency ablation (RFA), particularly second-generation segmental thermal ablation systems like ClosureFast, provides effective truncal occlusion through percutaneous access under ultrasound (US) guidance.3,8,9 Clinical trials have consistently demonstrated that RFA offers superior early patient-centered outcomes compared to surgery, including significantly reduced post-procedural pain and a faster return to routine activities. 7 Standardized reporting of these clinical outcomes relies on the updated CEAP classification to describe cross-sectional disease status and the revised Venous Clinical Severity Score (VCSS) as a dynamic, evaluative tool responsive to longitudinal changes following intervention.6,10,11
In addition to truncal thermal interventions, ultrasound-guided foam sclerotherapy (UGFS) using polidocanol serves as a well-tolerated and effective adjunct for managing symptomatic residual tributaries.5,11 This minimally invasive technique ensures enhanced endothelial contact and treatment accuracy, allowing for the comprehensive elimination of complex venous patterns in an ambulatory setting.5,9,11
Although the effectiveness of endovenous radiofrequency ablation (RFA) has been demonstrated in previous studies, real-world data evaluating both anatomical and clinical outcomes remain valuable.5,9,12 There is a continuous need for research that incorporates both anatomical occlusion rates and patient-reported clinical severity scores to assess the efficacy of thermal ablation across different saphenous trunks. Therefore, this study aimed to evaluate the 1-year anatomical and clinical outcomes of endovenous radiofrequency ablation in patients with great and small saphenous vein insufficiency, including the use of staged ultrasound-guided foam sclerotherapy for symptomatic residual tributary veins when indicated.
Materials and methods
Study design and patient selection
This retrospective study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board. Between 2024 and 2026, a total of 99 patients were evaluated. Of these, 84 patients, corresponding to 90 treated limbs, completed follow-up and were included in the final analysis. Fifteen patients were excluded because of loss to follow-up. Among these, 74 patients underwent GSV ablation (including 6 bilateral procedures, totaling 80 limbs), and 10 patients underwent SSV ablation. All outcome analyses were performed on a limb-based basis. Inclusion criteria were truncal reflux lasting >500 ms on duplex US in the standing position. Patients with acute deep vein thrombosis, non-ambulatory status, or a history of previous intervention on the target vein were excluded (Figure 1). CONSORT-style flow diagram of patient inclusion, treatment allocation, and adjunctive intervention. UGFS: Ultrasound-guided foam sclerotherapy; GSV: Great saphenous vein; SSV: Small saphenous vein.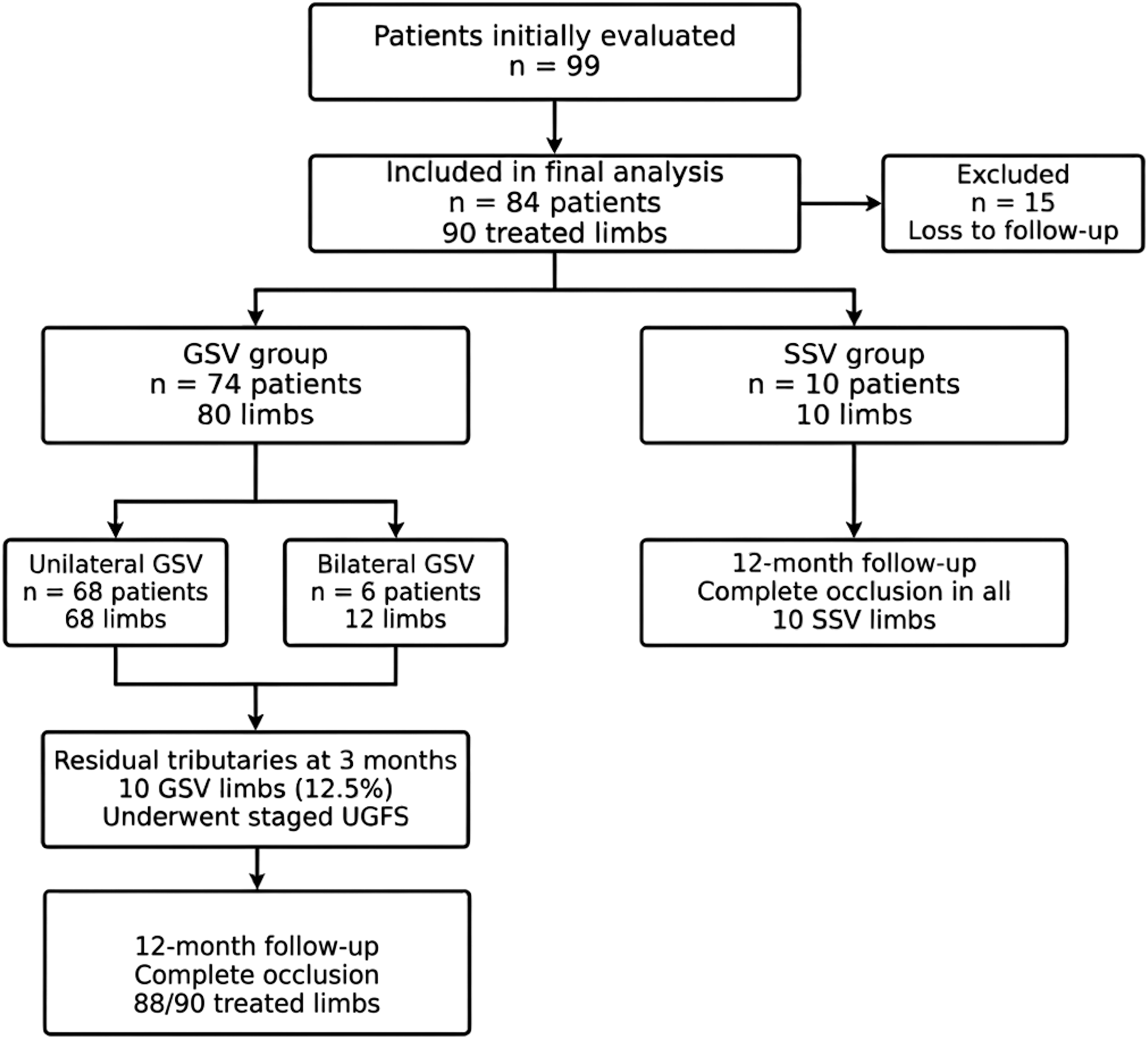
Procedure and follow-up
RFA was performed using a segmental thermal ablation system (ClosureFast, Medtronic) under ultrasound guidance and local tumescent anesthesia. Following local infiltration with prilocaine at the access site, a 7F vascular sheath was introduced, and the appropriate ablation catheter was advanced through the sheath into the target vein segment under ultrasound guidance. In the GSV subgroup, a catheter with a 7-cm heating element was used, whereas in the SSV subgroup, a catheter with a 3-cm heating element was preferred to allow for more controlled ablation in anatomically sensitive regions. Tumescent anesthesia was administered along the entire target vein segment prior to ablation. A solution consisting of 500 mL of normal saline combined with 20 mL of 2% prilocaine was infiltrated perivenously under US guidance using a pressurized infusion system. This technique provided effective analgesia, vein compression, and thermal protection of surrounding tissues. No procedural sedation was required. In the GSV subgroup, ablation was performed from the saphenofemoral junction (SFJ) to the most distal straight segment of the vein, typically at the level of the knee or mid-calf. Ablation below the mid-calf level was intentionally avoided to reduce the risk of saphenous nerve injury. In the SSV subgroup, ablation was performed from the saphenopopliteal junction (SPJ) to the mid-calf level to minimize the risk of sural nerve injury. At the SFJ and SPJ levels, three ablation cycles were applied to ensure adequate proximal closure. In the subsequent proximal segments, two cycles were delivered, followed by a single cycle per segment along the remaining treated vein. Although the manufacturer’s instructions for use (IFU) recommend two treatment cycles at the junctional segment, our institutional protocol incorporated an additional proximal ablation cycle, resulting in three treatment cycles at the SFJ/SPJ level throughout the study period. The rationale for this modification was to maximize proximal vein closure and reduce the risk of residual reflux or early recanalization at the junctional segment.
Following the procedure, compression therapy was applied using thigh-length graduated compression stockings. Patients were encouraged to ambulate immediately after the procedure and were discharged on the same day after approximately 1 h of observation. Analgesics were prescribed on an as-needed basis. At the 3-months follow-up, 10 limbs (12.5% of GSV limbs), all from the GSV subgroup, were identified with symptomatic residual tributary veins and underwent staged UGFS. Polidocanol was used as the primary detergent sclerosing agent in either 1% or 3% concentrations, depending on the diameter of the target tributary. For all cases, physician-compounded foam was prepared using the Tessari technique, which involves agitating the liquid sclerosant with room air at a 1:4 ratio using two interconnected syringes via a three-way stopcock until a cohesive microfoam is produced. All injections were performed under continuous US guidance to ensure intraluminal placement and to monitor foam dispersal, thereby minimizing the risk of inadvertent intra-arterial injection or deep venous extension. Baseline duplex US assessment included confirmation of truncal reflux and standardized measurement of target vein diameter. In the GSV subgroup, vein diameter was measured at the mid-thigh level, whereas in the SSV subgroup, measurements were obtained 2 cm distal to the SPJ. The mean preprocedural vein diameter was 6.3 ± 1.2 mm in the GSV subgroup and 5.9 ± 1.7 mm in the SSV subgroup. For SSV cases, particular care was taken regarding the access site (mid-calf or above) to minimize sural nerve injury. Clinical outcomes were evaluated using the revised VCSS at baseline and during follow-up. The CEAP classification was recorded at baseline only to characterize disease severity. Anatomical success was defined as complete occlusion of the treated segment with no evidence of flow or recanalization >5 cm on duplex US.
Statistical analysis
Statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD). The normality of continuous variables was evaluated using the Shapiro-Wilk test. Changes in VCSS over time (baseline vs 12 months) were analyzed using the paired samples t-test for normally distributed data. For data not meeting the normality assumption, the Wilcoxon signed-rank test was utilized as a non-parametric alternative. Technical success, occlusion rates, and the frequency of complications were reported using descriptive statistics as absolute numbers and percentages. A p-value < .05 was considered statistically significant.
Results
Baseline characteristics
Baseline demographic and clinical characteristics (patient- and limb-based data).
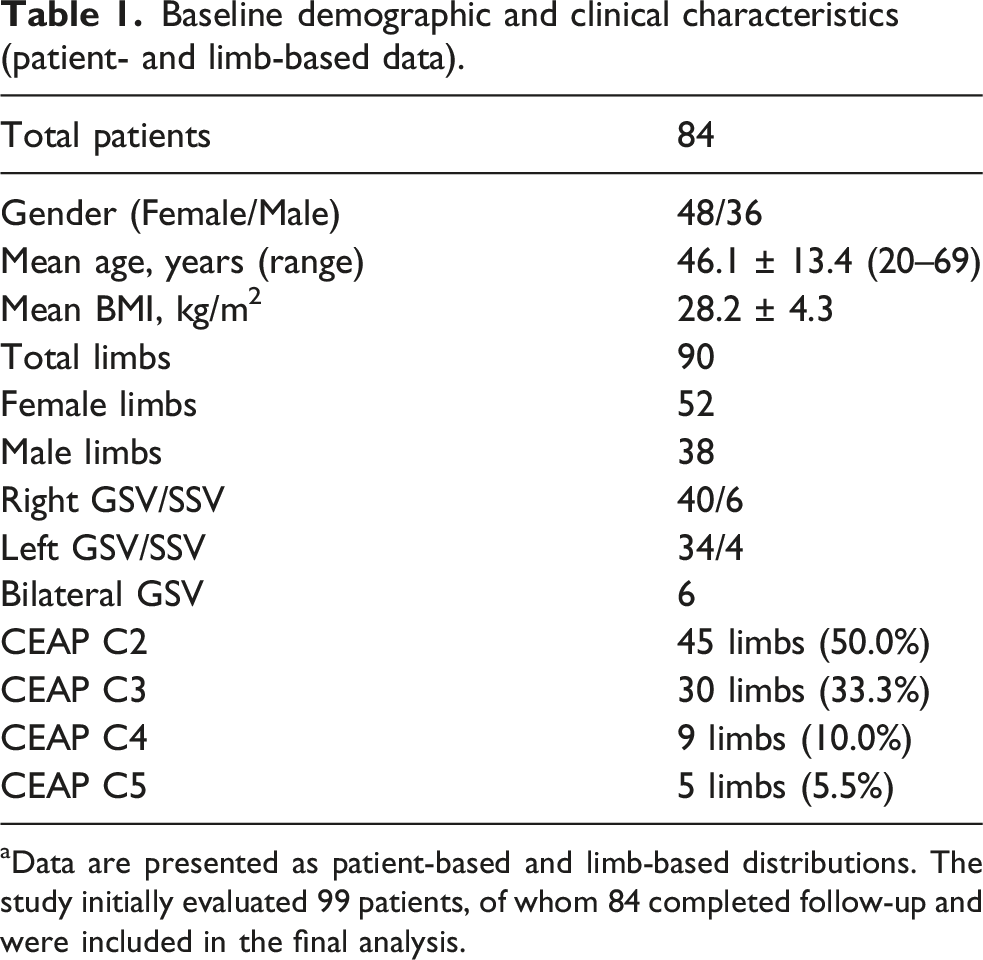
aData are presented as patient-based and limb-based distributions. The study initially evaluated 99 patients, of whom 84 completed follow-up and were included in the final analysis.
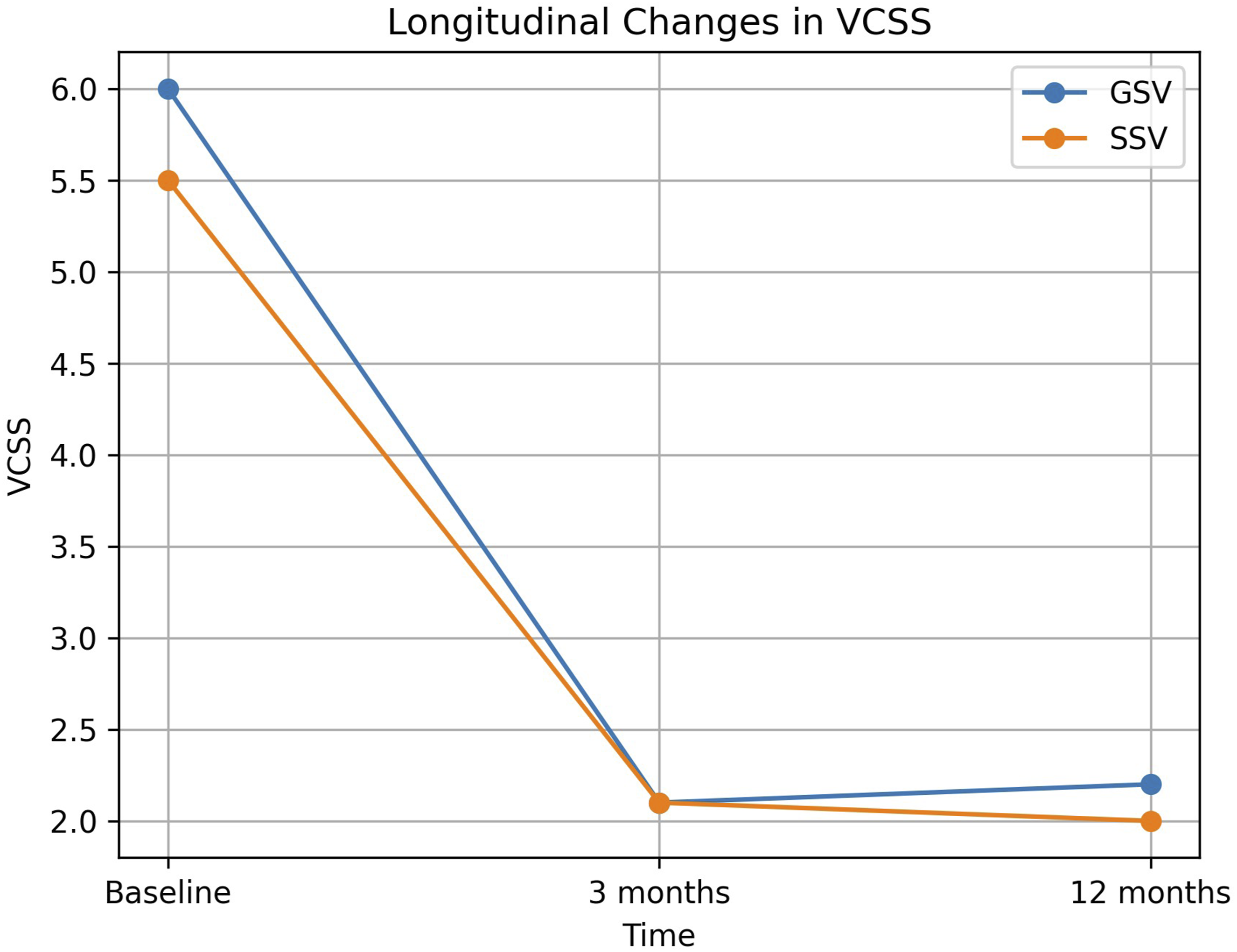
Longitudinal changes in VCSS in GSV and SSV subgroups over the 12-months follow-up period. VCSS: Venous Clinical Severity Score; GSV: Great saphenous vein; SSV: Small saphenous vein.
Procedural and anatomical outcomes
The overall occlusion rate across all treated limbs was 88/90 (97.7%). Anatomical success, defined as complete truncal occlusion confirmed by duplex US, was achieved at the 12-months follow-up. Partial recanalization at the SFJ was detected in 2 limbs (2.2%) during the 1-year study period; however, these cases remained clinically asymptomatic with sustained improvement in VCSS. A subgroup analysis of patients with SSV insufficiency (n = 10) demonstrated a 100% anatomical success rate, with complete occlusion confirmed by duplex US at the 12-months follow-up. At the 3-months follow-up, clinical and duplex US evaluation identified 10 limbs (12.5% of GSV limbs) with symptomatic residual tributaries underwent staged UGFS with polidocanol.
Clinical improvement
Longitudinal changes in venous clinical severity score (VCSS).

ap-values represent comparisons between baseline and each follow-up time point within the GSV subgroup using paired samples t-test. No statistical comparison was performed for SSV due to small sample size.
Complication rates
Procedural and safety outcomes.
Discussion
The present study demonstrates that endovenous RFA is a highly effective and safe treatment for saphenous vein insufficiency, achieving a 97.7% anatomical occlusion rate at 1 year. Our findings are consistent with current European guidelines, which recommend endovenous thermal ablation as the first-line treatment for GSV insufficiency, preferred over both surgery and foam sclerotherapy. 5 Our results are in agreement with previous reports, including the European ClosureFast study group (96.9% occlusion at 1 year), Sanrı et al. (97.6% occlusion at 12 months), and Choi et al. (94.6% and 94.5% occlusion rates for the GSV and SSV, respectively).3,8,14
The updated CEAP classification and VCSS remain widely accepted tools in the evaluation of CVD.6,12 In the present study, CEAP classification was used to characterize baseline disease severity, whereas VCSS served as the primary measure of longitudinal clinical response. The substantial improvement in VCSS observed during follow-up is likely driven by successful elimination of truncal reflux and the resulting reduction in venous hypertension and related symptoms.9,12 However, since 10 limbs underwent staged sclerotherapy for symptomatic residual tributaries at 3 months, these favorable 1-year outcomes should be interpreted within the context of a combined treatment strategy rather than truncal thermal ablation alone.
In the SSV subgroup, a 100% occlusion rate was achieved at 1 year. Given the limited number of SSV cases (n = 10), these findings should be interpreted as descriptive and hypothesis-generating rather than definitive evidence of treatment efficacy. No permanent nerve injury was observed, which may be attributable to the standardized technique used in our cohort, whereby ablation was limited to the mid-calf level to minimize the risk of sural nerve injury.4,5 The low incidence and transient nature of paresthesia further support the safety of this approach.
The safety profile of RFA in the present study was highly favorable. The low incidence of ARTE observed in our cohort (1.2%) is well within the generally accepted safety limits reported in the literature, which typically range from 1.3% to 1.7%.5,9,12 Most minor complications, including focal paresthesia, were transient and resolved completely during follow-up. These findings support the safety of RFA when performed with appropriate patient selection and standardized procedural technique.
This study has several limitations. Its retrospective design, the predominance of GSV cases, and the limited number of SSV cases may restrict the generalizability of the findings, particularly for SSV insufficiency. The absence of a comparative control group precludes direct comparisons with surgical or non-thermal treatment modalities. In addition, the 1-year follow-up period does not fully capture late recanalization or recurrence patterns. Approximately 15.2% of patients were lost to follow-up. However, the baseline CEAP classification and VCSS scores of excluded patients were comparable to those of the analyzed cohort, suggesting that attrition bias is unlikely to have materially influenced the study outcomes. Nevertheless, the effect of unmeasured confounders cannot be completely excluded. Finally, longitudinal CEAP reassessment was not performed, although VCSS was used as the primary outcome measure because of its greater responsiveness to clinical change following intervention.
Endovenous RFA is a highly effective treatment for saphenous vein reflux, achieving a 97.7% anatomical occlusion rate and a significant reduction in clinical severity as assessed by VCSS at 1-year follow-up. The procedure demonstrated a favorable safety profile characterized by a low incidence of major complications and only transient minor adverse events.
Footnotes
Ethical considerations
This study was approved by the Institutional Review Board and conducted in accordance with the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this work, the authors used Gemini (Google) and ChatGPT (OpenAI) to improve the English language and editing of the manuscript, as well as to assist in the creation of the graphical abstract. After using these tools, the authors reviewed and edited the content as needed and take full responsibility for the final version of the manuscript and its visual components.
Guarantor
Ömer Faruk Topaloğlu is the guarantor of this study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.