
Abstract
Background
Stasis dermatitis with hyperpigmented skin lesions is a distressing condition for patients with chronic venous hypertension. There are no randomized studies evaluating lasers for the treatment of these patients. Lasers can be an attractive option for treating hyperpigmentation associated with stasis dermatitis.
Methods
This prospective, randomized, 3-arm, open-label, vehicle-controlled study will enroll patients scheduled to undergo treatment for stasis dermatitis with hyperpigmented skin lesions. Patients will be allocated to either Q-switched Nd: YAG 1064 nm short-pulse nanoseconds, Nd: YAG 1064 nm ultra-short-pulse picoseconds, or cold cream vehicle control. All treatments are scheduled for six visits with pre-defined dates, with a final follow-up visit at 28- to 35-days intervals. Primary outcomes include colorimetry analysis, secondary outcomes pre- and post-photographic analysis, and DLQI quality-of-life assessment.
Conclusions
The results of this trial will provide high-quality evidence to guide clinical practice on optimal management of hyperpigmented skin lesions secondary to stasis dermatitis.
Introduction
Stasis dermatitis, formerly called ochre dermatitis, is a common chronic inflammatory skin disease of the lower limbs in patients with chronic venous insufficiency. It is often associated with varicose veins of the lower limbs, chronic dependent edema, hyperpigmentation, lipodermatosclerosis, and ulcerations. It is characterized by eczematous, scaly skin with watery patches and plaques on the legs and feet, with or without lichenification. 1
The prevalence of chronic venous insufficiency ranges from 1 to 40% in women and 1 to 17% in men, 3 times more frequent in women. The leading cause of chronic venous insufficiency is hereditary, and risk factors include age, family history of venous disease, female sex, standing occupation, obesity, and history of deep vein thrombosis. Heart failure and hypertension are aggravating factors. 2
Stasis dermatitis, caused by venous hypertension, usually results from dysfunction of the venous valves, obstruction of venous flow, or failure of the calf muscle “venous pump.” Venous hypertension induces microcirculatory changes in the dermis, including dilated capillaries and increased permeability, which lead to edema, accumulation, and adhesion of leukocytes to the vascular endothelium, hemosiderin deposits, and hyperplastic venules. The progression of the inflammatory process leads to lipodermatosclerosis (fibrosis of the skin and subcutaneous tissue) and the formation of ulcers. 3
Stasis dermatitis is a late manifestation of chronic venous disease (CEAP classification stage C4). Due to its severity, the medial malleolus is the most frequently and severely involved, although skin changes can extend to the knee and foot. They are intensely itchy, and sometimes there are fissures. With the chronicity of the condition, the lesions tend to become lichenified. 4
The treatment consists of correcting the cause of venous insufficiency, with surgery for varicose veins of the lower limbs using various techniques, and the use of elastic compression stockings.
Topical corticosteroids are used for acute cases and can be applied to lesions to reduce itching and inflammation. However, their long-term use is associated with local and systemic side effects. 5 Topical calcineurin inhibitors are often used and are associated with skin burns. 6 No treatment has been specifically approved for the treatment of hyperpigmentation associated with stasis dermatitis. Consequently, new and effective therapies with favorable safety profiles are needed. 7
Nd: YAG lasers are advantageous for skin rejuvenation because their short pulse width causes minimal damage to surrounding tissues. It is used to treat various conditions, including vein disorders and hyperpigmentation. 8
Stasis dermatitis is a serious health problem for patients with chronic venous hypertension with aesthetic and quality of life implications.
To our knowledge, there is no prospective, randomized study evaluating these lasers for treating stasis dermatitis in patients with chronic venous insufficiency.
Methods
Study design
This prospective, randomized, open-label, vehicle-controlled study will enroll patients at a private clinic (Clinic Ramacciotti, Santo Andre, SP, Brazil) scheduled to undergo treatment for stasis dermatitis with skin hyperpigmentation. Enrollment will occur after written informed consent is provided. This trial will be conducted following the SPIRIT guidelines. 9
All study data will be collected using a pre-established clinical case report form (CRF) within the REDCap® platform (Research Electronic Data Capture, REDCap Consortium, Vanderbilt University Medical Center, Tennessee, USA), which will capture demographic information, risk factors, and clinical characteristics related to patient comorbidities. Clinical evaluations will be conducted by a trained team member employing standardized assessments, including imaging when clinically indicated.
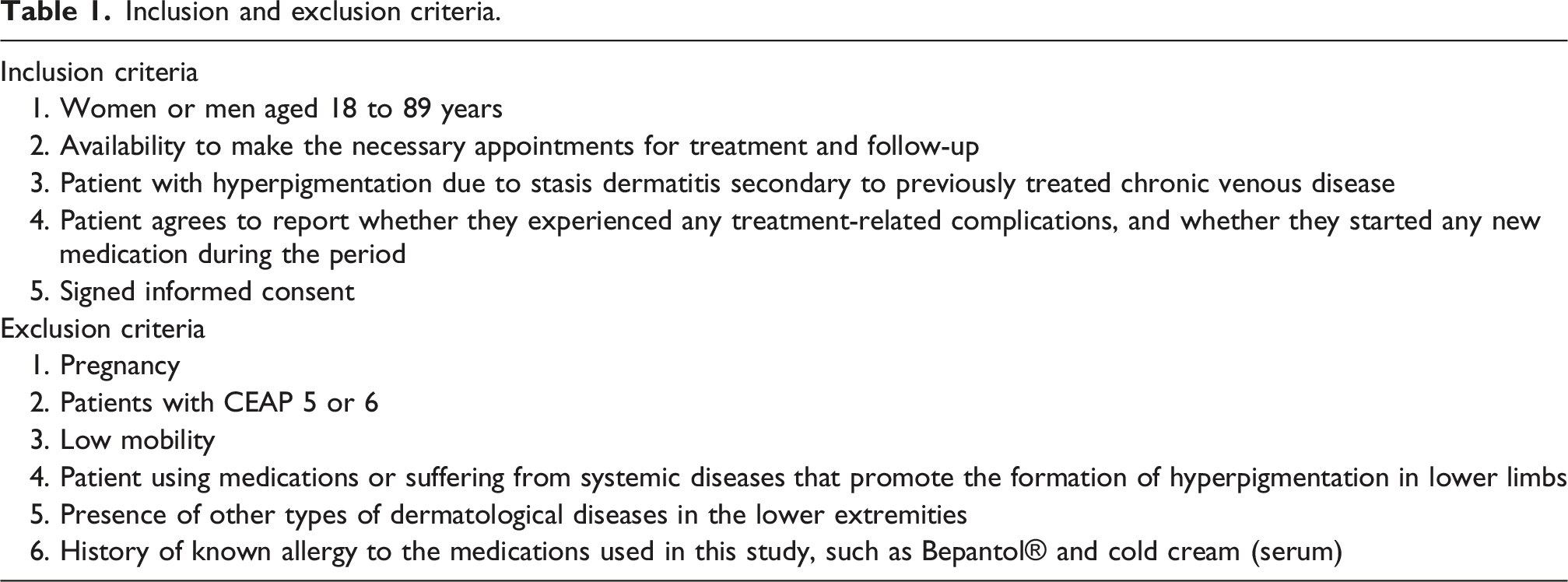
Inclusion and exclusion criteria.
Ethical approval and trial registration
This study will be conducted in compliance with the principles of the Declaration of Helsinki and applicable national regulations. The research protocol was reviewed and approved by the Research Ethics Committee (CAAE: 85824824.1.0000.5479; Approval Number: 7.375.875). The trial was registered with ClinicalTrials.gov under identifier NCT06980961.
Randomization and intervention
Randomization
Patients will be randomized into 3 Groups, using a computer-generated randomization schedule prepared before study initiation. For intervention, group 1 patients will be treated with an Nd:YAG 1064 nm Q-switched laser, and group 2 patients will be treated with an Nd:YAG 1064 nm Picosecond laser. In the Control Group (group 3), patients will receive a topical vehicle.
Baseline characteristics will be documented, and patients will be electronically randomized within the REDCap® platform (version 11.0.3) using a 3:1 allocation ratio, balanced across randomly permuted blocks of variable sizes. This study will be conducted under an open-label design.
The randomization list will be generated using validated software REDCap®, ensuring allocation concealment through variable-sized blocks. Investigators will access the trial-specific website and complete a standardized medical record form to enroll patients.
Interventions
Group 1
Nd: YAG 1064 nm Q-switched laser (5 nanoseconds), 4 mm spot size, from 100 to 1000 mJ total energy, treatment scheduled for six visits with pre-defined dates, with intervals of 28 to 35 days. The device will be Omer Smart®, a Q-Switch Laser produced by Medical San (Lajeado, RS, Brazil).
Group 2
Nd: YAG1064 nm picoseconds laser (400 picoseconds), 2 to 10 mm spot size, from 100 to 1000 mJ total energy, treatment scheduled for six visits with pre-defined dates, with intervals of 28 to 35 days. The device will be Omer Premium®, a picolaser produced by Medical San (Lajeado, RS, Brazil).
For both lasers, the initial energy will be set based on the immediate response of the treated area. It starts at 100 mJ and increases until erythema, edema, or petechiae are observed.
Group 3. (control arm)
The control vehicle is a cold cream, supplied by HERVA’S manipulation pharmacy. The composition of cold cream will be beeswax, acetyl palmitate, BHA, cetearyl alcohol, propylparaben, and water. This topical agent will be applied to patients daily throughout the treatment period. It is scheduled for six visits with pre-defined dates, spaced 28 to 35 days apart.
Study procedures
The initial assessment will be carried out by a trained team after a prior evaluation of the lesion. Baseline characteristics will be collected, and photos will be taken and uploaded electronically to the REDCap® platform. The images will be of the affected lower limbs (in a standardized lighting environment, position, and marking of the most pigmented area, in a small studio for standardized digital photographs, a dark box dedicated to photos of the lower limbs), and the measurement of the color of the lesion by digital colorimetry WR 10QC.
The most pigmented area, or the area that is most bothersome to the patient, is selected on the limb with a CEAP score of up to 4. With the patient in the supine position, the distance from the plantar surface of the heel to the lesion, relative to the malleolus, is measured with a ruler. The ruler and spirograph are positioned over the target area, and photographic documentation is then performed. A 5-cm radius circle is then drawn on the skin, within which 20 colorimeter measurements are obtained. Based on the photographic documentation, the circle is consistently repositioned over the same area in subsequent assessments.
The lower limbs will be photographed before and after the treatment using a Nikon D7500 pro digital camera. The images will be obtained under natural light, with the patient in orthostasis and a dark background in the previously described digital studio. All laser procedures and completion of clinical data will be performed by physicians previously assigned for the study.
In addition to the photos, patients will undergo color measurement of the lesions using digital colorimetry. There will be six treatment sessions, with pictures of the affected legs taken at the first visit and at the final follow-up visit (V7). Painless digital colorimetry – in a pre-defined area on the ankle (or the darkest area on the base visit) is scheduled for all visits. Patients will be discontinued by participant request, disease worsening, or severe adverse event.
The Dermatology Life Quality Index (DLQI) questionnaire will be administered at visit 1, followed by treatment initiation. This quality-of-life questionnaire will be re-applied on the last visit. Figure 1 details the study procedures. Study design.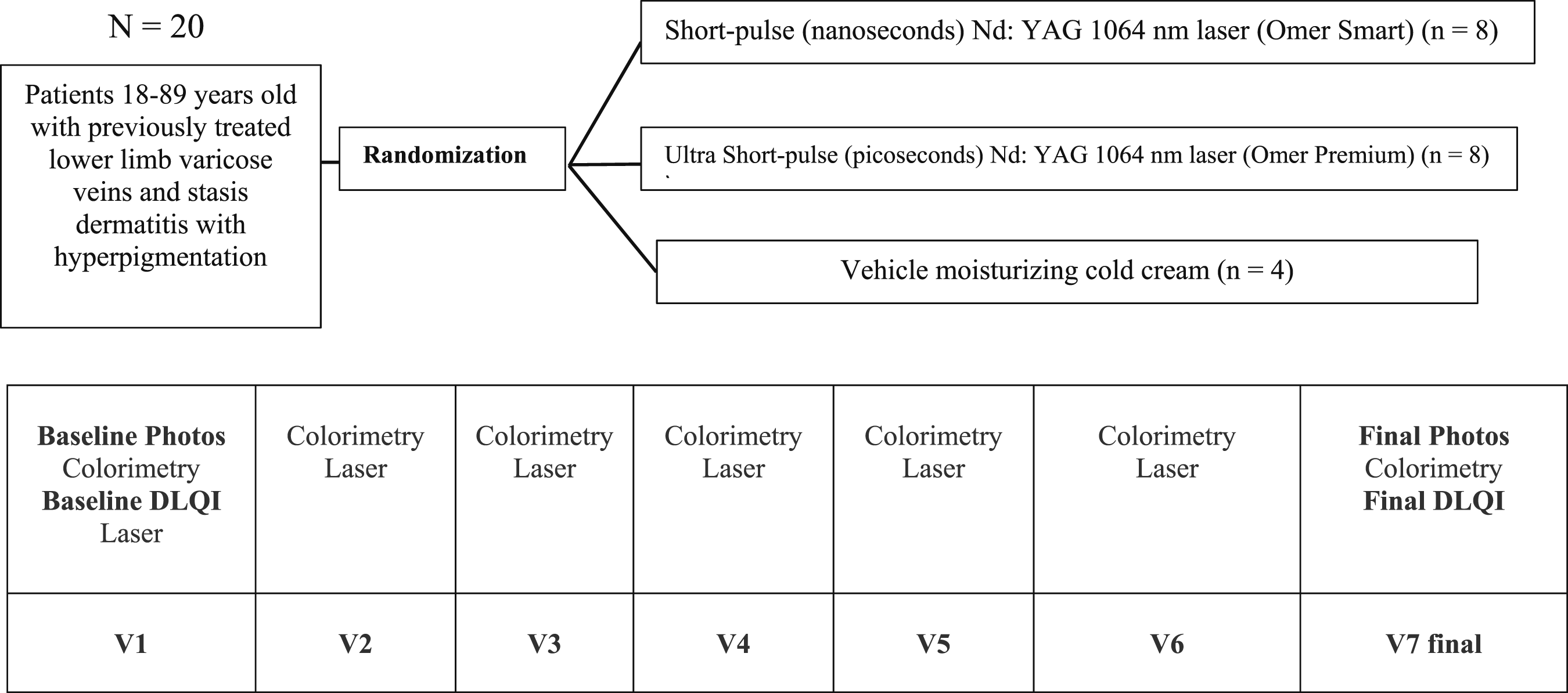
Objectives
To prospectively evaluate the efficacy and safety of the Nd: YAG 1064 nm Q-switched laser, the Omer Smart® (nanoseconds), and the Nd: YAG 1064 nm picosecond laser, the Omer Premium® (picoseconds) in the treatment of stasis dermatitis in patients with chronic venous insufficiency.
Primary objective
To test the efficacy and safety of nanoseconds and picoseconds lasers in treating skin hyperpigmentation due to stasis dermatitis in patients with treated chronic venous hypertension.
Primary efficacy outcome
Pre-, during, and post-laser treatment assessment of skin hyperpigmentation by stasis dermatitis by digital colorimetry. Final analysis comparing baseline versus final visit (after six treatment sessions and a final follow-up visit 28 to 35 days after the last treatment session).
Co-primary efficacy outcome
Pre- and post-treatment laser evaluation of skin hyperpigmentation improvement by pre- and post-treatment photography, and stasis dermatitis by blinded evaluators.
Primary safety outcome
Potential skin alterations: redness, swelling, temporary changes in skin pigmentation (hyper or hypopigmentation), petechia, scarring, or burns.
Secondary objective
Validate the evaluation criteria for stasis dermatitis skin hyperpigmentation treatment, such as the digital colorimeter and evaluation by pre- and post-treatment photographs with blind evaluators (3 experienced dermatologists and vascular surgeons) for the treatment arms.
Secondary efficacy outcome
Evaluation of a questionnaire on quality of life, Dermatology Life Quality Index (DLQI), 10 pre- and pos- post-intervention for skin hyperpigmentation secondary to stasis dermatitis.
Hypothesis
Nanosecond and picosecond lasers are superior to vehicle (cold cream) treatment in reducing hyperpigmentation associated with stasis dermatitis secondary to chronic venous hypertension.
Colorimetry analysis
The primary outcome will be the skin tone dissimilarity (expressed as ΔE) between treated and adjacent areas, measured using digital colorimetry. This method was previously described and allows precise measures of skin color differences. 11
The ΔE value is derived from differences in the International Commission on Illumination L*a*b* (CIELAB) color space, which provides a systematic way to represent color differences using three parameters: lightness (L*), red-green chromaticity (a*), and yellow-blue chromaticity (b*). Measured CIELAB color space parameters enable the unique identification of every visually distinguishable color, and their use is proposed to unambiguously communicate skin color information for clinical or scientific purposes.12,13
This metric provides a structured approach to quantifying color differences, with specific intervals indicating varying levels of perceptibility that may be translated into different intensities of pigmentation: • 0 < ΔE <1 - the difference is unnoticeable • 1 < ΔE <2 - the difference is only noticed by an experienced observer (mild), • 2 < ΔE <3.5 - the difference is also noticed by an inexperienced observer (light), • 3.5 < ΔE <5 - the difference is noticeable (moderate), • 5 < ΔE - gives the impression that these are two different colors (intense)
Patients will undergo colorimetric analysis, Δwith E representing the skin color difference between the treated and adjacent areas. Multiple colorimetric measurements (20 per circle) will be carried out from baseline and at each session. The ΔE considered for each session will be the mean ΔE obtained.
Photographic analysis
The co-primary outcome will be the improvement in post-procedure skin hyperpigmentation after six treatment sessions, evaluated using before-and-after photo documentation and analyzed by three experienced, independent, and blind observers.
All evaluators will have access to high-definition before-and-after pictures of the patient’s legs that were designated for them. Then, they will answer the question, “Do you think there’s post-treatment improvement in hyperpigmentation in the treated areas of this limb, yes or no?” for the affected limb, according to their expertise. The answers chosen by most of the evaluators will be considered for data analysis.
Quality of life questionnaire
The DLQI is the most frequently used patient-reported outcome measure in dermatology. It was the first dermatology-specific quality-of-life questionnaire, published in 1994. 10 It has 10 questions about the impact of skin disease on quality of life over the last week. The DLQI has validated score meaning bands and responsiveness and defined minimal meaningful change. It is mapped to EQ-5D to calculate utility values. 14
The DLQI covers the following areas in its 10 questions: (1) Symptoms: How itchy, sore, painful, or stinging the skin has been. (2) Embarrassment: How embarrassed or self-conscious one has been due to their skin. (3) Daily Activities: How much the skin condition has interfered with shopping, home care, or gardening. (4) Clothing: How much the skin condition has influenced the clothes worn. (5) Social/Leisure: How much the skin condition has affected social or leisure activities. (6) Sport: How much has the skin condition made it difficult to do sports? (7) Work/Study: Whether the skin condition has prevented working or studying, and if not, how much it has been a problem. (8) Personal Relationships: How much has the skin condition created problems with close relationships? (9) Sex: How much has the skin condition caused sexual difficulties? (10) Treatment: How much has the treatment for the skin condition been a problem, considering factors like time or mess?
These 10 questions will be applied to all patients at baseline visit and at the end of the six treatment visits and compared among study groups.
Safety analysis
Safety analysis will be conducted through clinical evaluation at all pre-scheduled visits. It includes clinical analysis of potential discomfort or pain and of skin alterations, such as abnormal redness, swelling, temporary changes in skin pigmentation (hyper- or hypopigmentation), petechiae, scarring, or burns. It will be reported as the number of participants with treatment-related adverse events.
Statistical analysis
Statistical analyses will be carried out using R software (RStudio®: Integrated Development for R. RStudio, PBC, Boston, 2020, version 4.2.2). Descriptive statistics will include absolute and relative frequencies for categorical variables, and measures of central tendency (mean and median) and dispersion (standard deviation, minimum, and maximum) for continuous variables.
Given the lack of data on the use of these lasers in stasis dermatitis, no sample size calculations were performed. A convenience sample of 20 patients was chosen for this study.
For the pre- and post-comparisons between the three treatment modalities, the paired Wilcoxon signed-rank test will be used for continuous variables that do not meet parametric assumptions, with a one-tailed approach.
For categorical paired outcomes, the McNemar test will be applied in its unilateral form, using a one-tailed binomial test on discordant pairs to assess the directionality of the effects. The significance level is set at 5% (p < .05).
Interrater reliability among evaluators will be calculated using kappa concordance and gross agreement tests.
For the DLQI test, Kruskal-Wallis, chi-squared, and t-tests will be used to analyze differences in DLQI scores between groups and to compare them with background variables.
Discussion
There are currently no approved treatments for skin hyperpigmentation due to stasis dermatitis, and research regarding lasers is lacking. Topical treatments were tested. One randomized controlled trial that evaluated betamethasone valerate 0.12% for stasis dermatitis and steroid-treated patients versus vehicle showed a statistically significant mean change in erythema and eczema. 15 Crisaborole® (topical agent) treated participants had significantly reduced total sign score (a score designed particularly for this trial) from baseline versus vehicle-based on in-person (nondermatologist) assessment (32.4% vs 18.1%, p = .0299) and central reader (dermatologists) assessment of photographs (52.5% vs 10.3%, p = .0004). However, no specific outcomes for hyperpigmented skin lesions were reported. 16
To our knowledge, no prospective randomized clinical trials have evaluated lasers for treating skin hyperpigmentation secondary to stasis dermatitis. Both lasers chosen for this study (Nd: YAG 1064 nm Q-switched and Nd: YAG 1064 nm picosecond) have been studied and shown to be effective for treating skin hyperpigmentation and rejuvenating the skin.17,18 Due to the lack of studies on hyperpigmentation associated with stasis dermatitis, we decided to study both lasers compared to vehicle (cold cream).
For both lasers, the initial energy will be set based on the immediate response of the treated area, depending on the laser’s ability to interact with the given hyperpigmentation skin lesion. Energy will vary from patient to patient, depending on the individual’s pigment response to the laser. In most pigments, it is challenging to reach immediate whitening, such as that observed in tattoos. We expect melasma like reactions, such as transient erythema, edema, and petechias.
Before enrollment, the patient must have the primary cause of venous hypertension treated (varicose veins, including saphenous vein reflux) by any approved technique (stripping, endolaser, radiofrequency, foam, and others). We decided to exclude patients with venous hypertension not treated to decrease the potential bias of a persistent cause for stasis dermatitis and worsening of skin hyperpigmentation. Patients with eczematous lesions were excluded.
The primary outcome chosen is objective and innovative. Variations in colorimetry analysis throughout the whole treatment period. This analysis will allow us to compare the time-effectiveness of different lasers. We decided to leave the subjective blinded photo analysis as a secondary outcome.
The DLQI is a validated quality-of-life questionnaire used in dermatology. It has been used for over 60 skin conditions in over 80 countries. It has been used in over 450 randomized controlled trials in dermatology, some of which used it as a primary outcome measure. It has served as a benchmark for validating more than 100 other quality-of-life instruments. A systematic review has identified 207 articles describing aspects of DLQI validation. 19 A patient-centered secondary outcome will bring important information regarding lasers for skin hyperpigmentation secondary to stasis dermatitis.
The proposed design has several limitations, including a small sample size that hampers generalization, as results from convenience samples typically apply only to the specific group studied. Additionally, the study’s single-center setting and the initial use of the objective method (colorimetry) for analyzing skin hyperpigmentation clearance are also constraints.
Conclusion
The results of this trial will provide high-quality evidence to guide clinical practice on optimal management of skin hyperpigmentation lesions due to stasis dermatitis. This study might serve as a pilot for larger multicenter randomized trials. If the study hypothesis is confirmed, lasers could become a cornerstone for the treatment of stasis dermatitis skin hyperpigmentation lesions, delivering superior cosmetic results compared to topical vehicles. These findings may also shape future guidelines, enhance patients’ quality of life, and improve long-term outcomes for this population.
Supplemental material
Supplemental Material - Q-switched and ultra-short-pulse Nd:YAG 1064 nm laser treatment for stasis dermatitis secondary to chronic venous hypertension: Rationale and design of the SUPERSTAR trial
Supplemental Material for Q-switched and ultra-short-pulse Nd:YAG 1064 nm laser treatment for stasis dermatitis secondary to chronic venous hypertension: Rationale and design of the SUPERSTAR trial by Valéria Cristina Resende Aguiar, Marcelo Halfen Grill, Rodrigo Kikuchi, Samantha Neves, Silvia Mathias Freitas, Maria Fernanda Portugal, Viviane da Silva Santana, Marcela Zanoni, Roberto Augusto Caffaro, Walkyria Hueb Bernardi, Giuliano Giova Volpiani, Fabrício Rodrigues Santiago and Eduardo Ramacciotti in Phlebology
Footnotes
Acknowledgements
The authors would like to thank Science Valley Research Institute for the logistical support for this academic study.
Ethical considerations
Protection of humans and animals: The authors declare that the procedures followed complied with the ethical standards of the responsible human experimentation committee and adhered to the World Medical Association and the Declaration of Helsinki. The institutional Ethics Committee approved the procedures. This study will be conducted in compliance with the principles of the Declaration of Helsinki and applicable national regulations. The research protocol was reviewed and approved by the Research Ethics Committee of the (CAAE: 85824824.1.0000.5479, Approval Number: 7.375.875).
Consent to participate
Confidentiality, informed consent, and ethical approval: The authors have obtained approval from the Ethics Committee to analyze routinely collected and anonymized clinical data, so informed consent was not required. Relevant guidelines were followed.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the author, with modest support from Science Valley Research Institute.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ER reports grants and consulting fees from Bayer and Pfizer, grants from the Brazilian Ministry of Science and Technology, and personal fees from Aché Pharma, Althaia, EMS, Novartis, and Daiichi-Sankyo outside the submitted work—no conflict of interest to disclose for the remaining authors.
Data Availability Statement
Anonymized participant data can be made available upon requests directed to the corresponding author. Proposals will be reviewed based on scientific merit. Once a proposal is approved, data can be shared via a secure online platform upon signing a data access agreement.
Contributorship
This is a study design manuscript. Enrollment is ongoing. VCRA, ER, SN, RK, MHG, and GGV researched literature and conceived the study. VCRA was involved in protocol development and obtained ethical approval. ER wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript. All authors will be involved in the clinical study procedures. Final contributorship will be disclosed when the manuscript, including the data, is submitted for publication.
Declaration on the use of artificial intelligence
During the preparation of this work, the author(s) used Grammarly to improve the text’s clarity and grammar. The authors carefully reviewed the output and are solely responsible for the manuscript’s content. After using this tool/service, the author(s) reviewed and edited the content as needed and took full responsibility for the publication’s content. No artificial intelligence tool was used.
Dissemination policy
Once the trial is completed, the results will be published in a peer-reviewed journal, and the primary target is Phlebology. Data will also be presented at medical meetings and online, in accordance with the submitted journal embargo policies.
Guarantor
The guarantor is Eduardo Ramacciotti, MD, Ph D, who is the senior author of the paper. Dr Ramacciotti holds important global publications, is a professor of Health Sciences at Santa Casa School of Medicine, and a professor of Thrombosis and Hemostasis at Loyola University Medical Center, Maywood, IL, USA. The current paper is a PhD thesis of the principal author (VCRA) under the formal mentorship of Dr Ramacciotti.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.