
Abstract
Objectives
This study aimed to analyze the patients with saphenous vein aneurysm (SVA) close to the junction treated with endovenous vacuum-assisted laser ablation (VALA).
Methods
This was a retrospective analysis the patients with great saphenous vein aneurysm close to the junction involving a terminal valve and varicose veins who underwent VALA from March 2021 to October 2025. Sclerotherapy of the tributaries were performed during the same treatment session. All patients were examined clinically and with duplex ultrasound (DUS) in the standing position.
Results
Ten patients with a median diameter of the great SVA 23.8 mm (IQR 21.6 – 28.9) were included in the study. At 6 months follow up saphenous aneurysms were absent and clinical outcome was improved in all of the patients. At the early postoperative visits there were no patients with symptoms of pulmonary embolism (PE), two cases of endothermal heat-induced thrombosis (EHIT) 1, and one case EHIT 2, which required the prescription of an anticoagulant therapeutic dose. No other adverse events were observed.
Conclusion
Sonographic and clinical 6-months follow-up showed that VALA is an effective procedure with excellent technical result for the treatment of great SVA close to the Junction. However, the best thromboprophylaxis strategy in this case remains to be debatable.
Introduction
A saphenous vein aneurysm (SVA) has been defined as a local dilatation of the vein of at least three times the upper limit of the average diameter, or >20 mm, if close to the saphenofemoral junction (SFJ), or >15 mm, if close to the saphenopopliteal junction (SPJ). 1 The Pascarella’s anatomical classifications establishes great saphenous vein (GSV) aneurysm located in the proximal third portion as Type I, Type II distal third portion, Type III as a combination of Type I and II SVA, and Type IV small saphenous vein (SSV) aneurysm. 2 Type I has the most clinical importance due to the increased risk of local thrombosis of the aneurysm and subsequent venous thromboembolism (VTE) including pulmonary embolism (PE) and difficulty of open surgery.3–5 According to the clinical practice guidelines for patients with superficial truncal vein aneurysm, located within 3 cm of the SFJ or SPJ, open surgical excision, with high proximal and distal ligations should be performed. 6 However, there are small prospective studies, in which endovenous thermal ablation (EVTA) was used alone or combined with high ligation if the diameter of the SVA close to the SFJ exceeded 30 mm, and was efficacious and safe.7,8 In case of SVA more than 30 mm it is difficult to remove the intraluminal blood from vein using only tumescent anesthesia. So, we combined endovenous laser ablation (EVLA) with vacuum evacuation of the remaining intraluminal blood to make the procedure more effective and safer. We retrospectively analyzed of the patients who presented with aneurysm close to the junction, treated with endovenous vacuum-assisted laser ablation (VALA) and followed-up for 6 months.
Methods
It was a retrospective analysis as one part of the research work “Endovenous vacuum-assisted laser ablation (VALA) in the treatment of large saphenous veins (>15 mm)”. This study protocol was approved by the regional Ethics Committee of the Ryazan State Medical University named after academician I.P. Pavlov (N0. 10, 06.03.2025). The study was registered in the clinical trials register of the Russian Phlebological Association (RPA) ID: CVD.030.01.09032025 and ClinicalTrials.gov ID: NCT06971068.
The retrospective analysis included patients with great saphenous vein aneurysm close to the junction and chronic venous disease who underwent VALA. Patients at two phlebology centers in Russia and Kyrgyzstan who were examined from March 2021 to October 2025 clinically and with duplex ultrasound (DUS) in the standing position were included in the analysis. Superficial and deep veins were assessed according to Clinical Etiological Anatomical Pathological (CEAP) classification. The type aneurysm was defined by Pascarella’s classification. 2 The inclusion criteria were set as age over 18 years, a great saphenous vein aneurysm ≥20 mm in diameter involving terminal valve, varicose veins of the lower extremities with clinical class C2-C6.
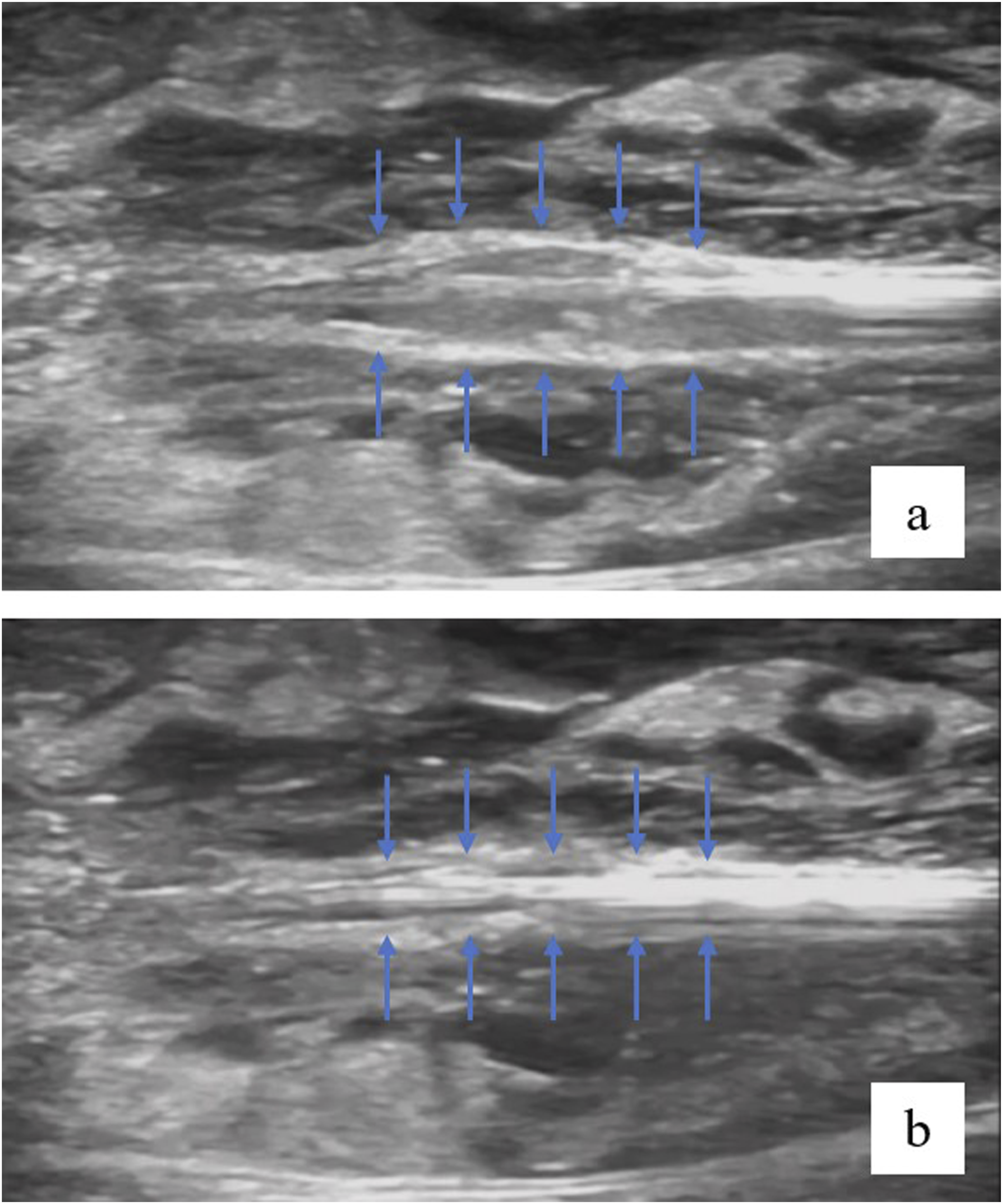
The VALA procedure was performed using a 1470-nm diode laser and a radial 2-ring Pro fiber. The design of this fiber was distinguished by the presence of an additional catheter around the laser fiber, through which a solution could be supplied into the vein lumen during EVLA to straighten the tortuous vein and wash out the remaining blood from the lumen. The fiber was positioned near the terminal valve. After tumescent anesthesia and before laser ablation was performed evacuation of residual blood from the sac of the aneurysm that led to a closer wall location of the treated vein to the surface of the light guide lens (Fig. 1, 2). All of the patients underwent concomitant foam sclerotherapy of the tributaries. Patients received preventive doses of low-molecular-weight heparin (LMWH) before and after the procedure for 10 days. Compression stockings were administered after the procedure (23–32 mmHg at the ankle) for 1 month. The posttreatment visits were the next day, after 14 days, 2 and 6 months and included DUS examination and clinical estimation. Evacuation (a) of blood through a catheter and accumulation (b) in the evacuation container. Wall location of the treated vein in relation with the surface of the light guide lens before (a) and after (b) the evacuation.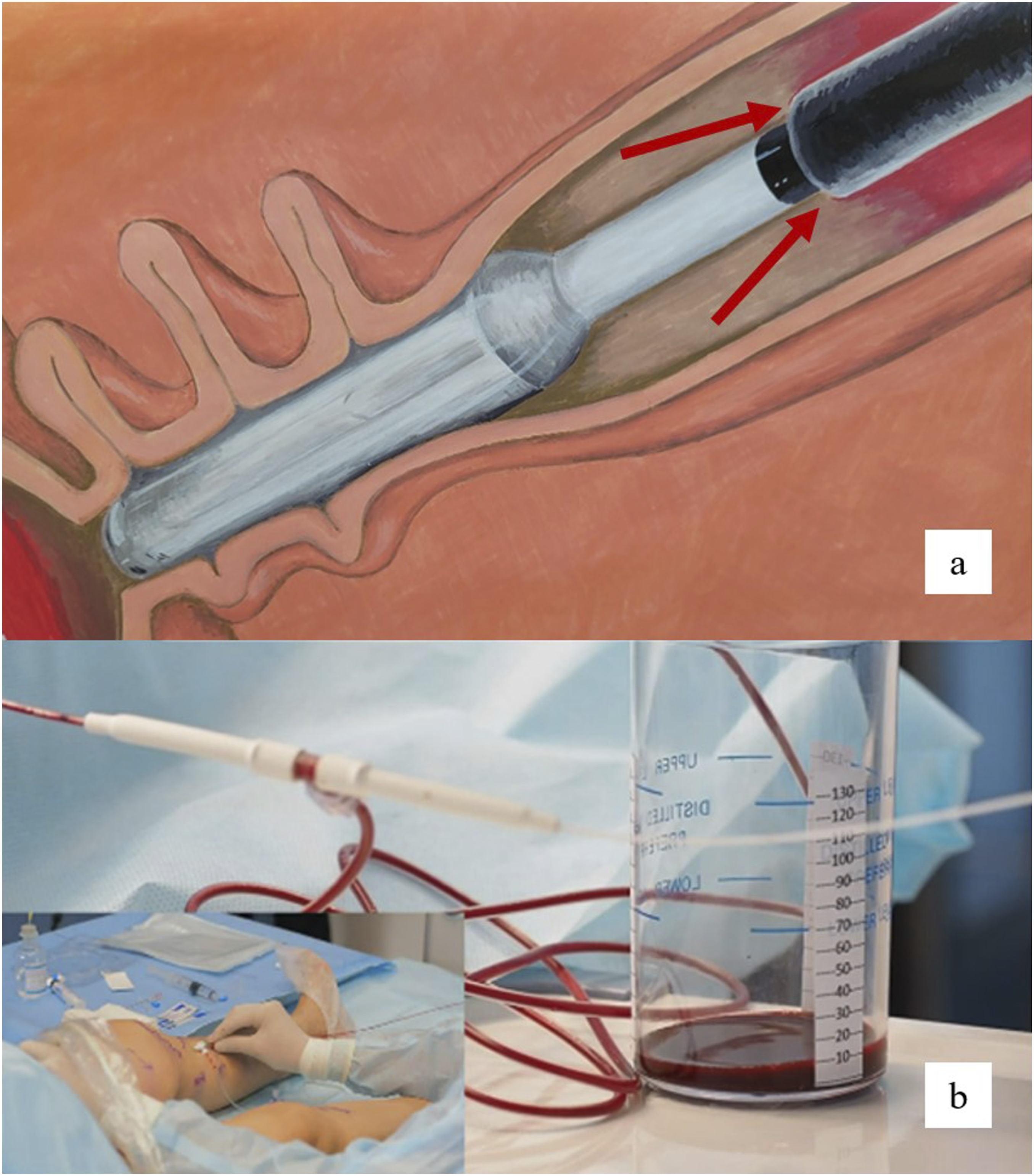
Statistical analysis
Continuous variables are expressed as the median and interquartile range (IQR), and categorical variables are expressed as absolute and relative frequencies. To test improvement of the CEAP before and after treatment, the Wilcoxon sign ranked test was used. Analysis was performed using the website “Social Science Statistics”, https://www.socscistatistics.com/tests/. A p-value <.05 was considered statistically significant.
Results
Baseline characteristics of the study participants.
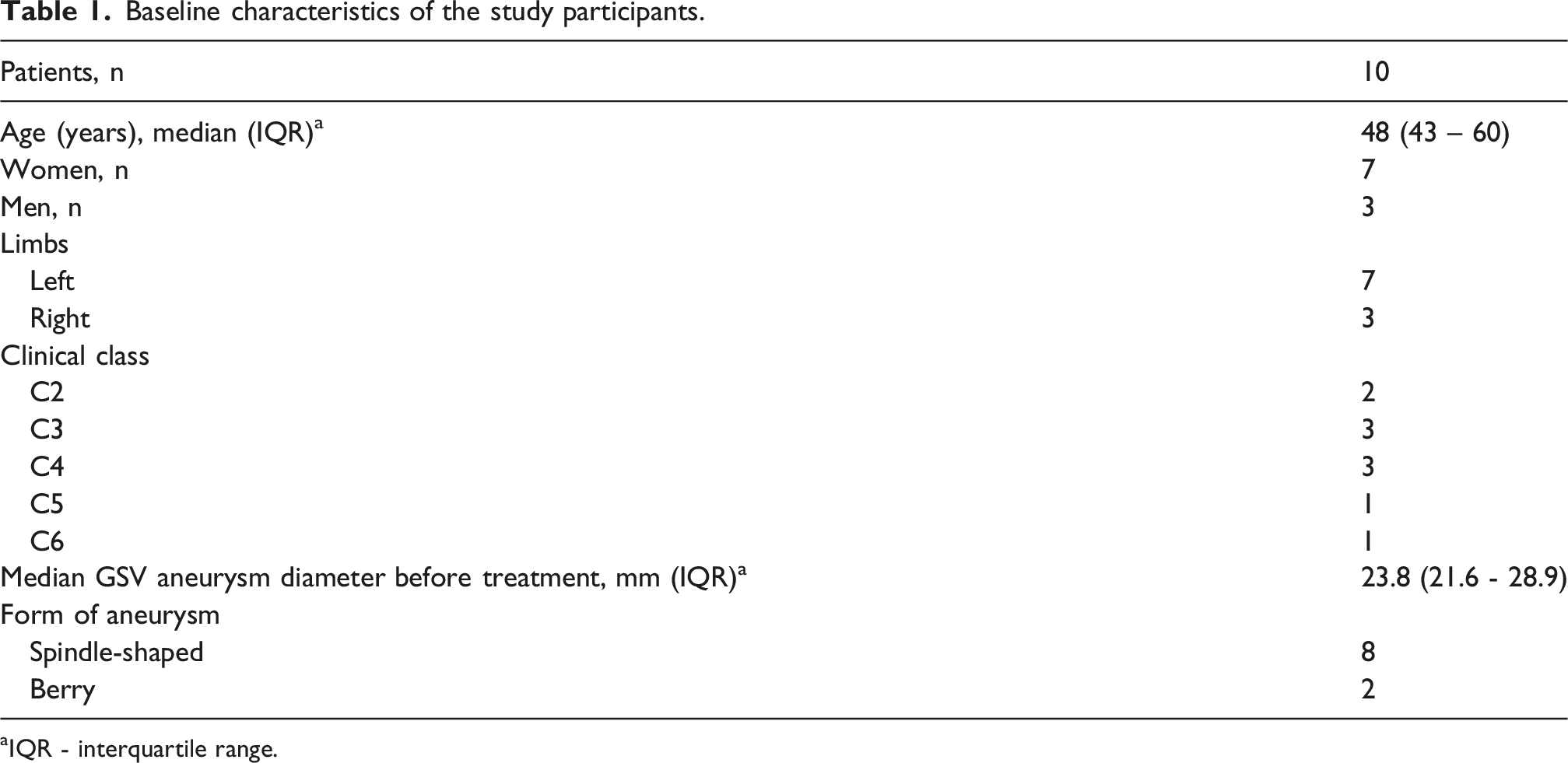
aIQR - interquartile range.
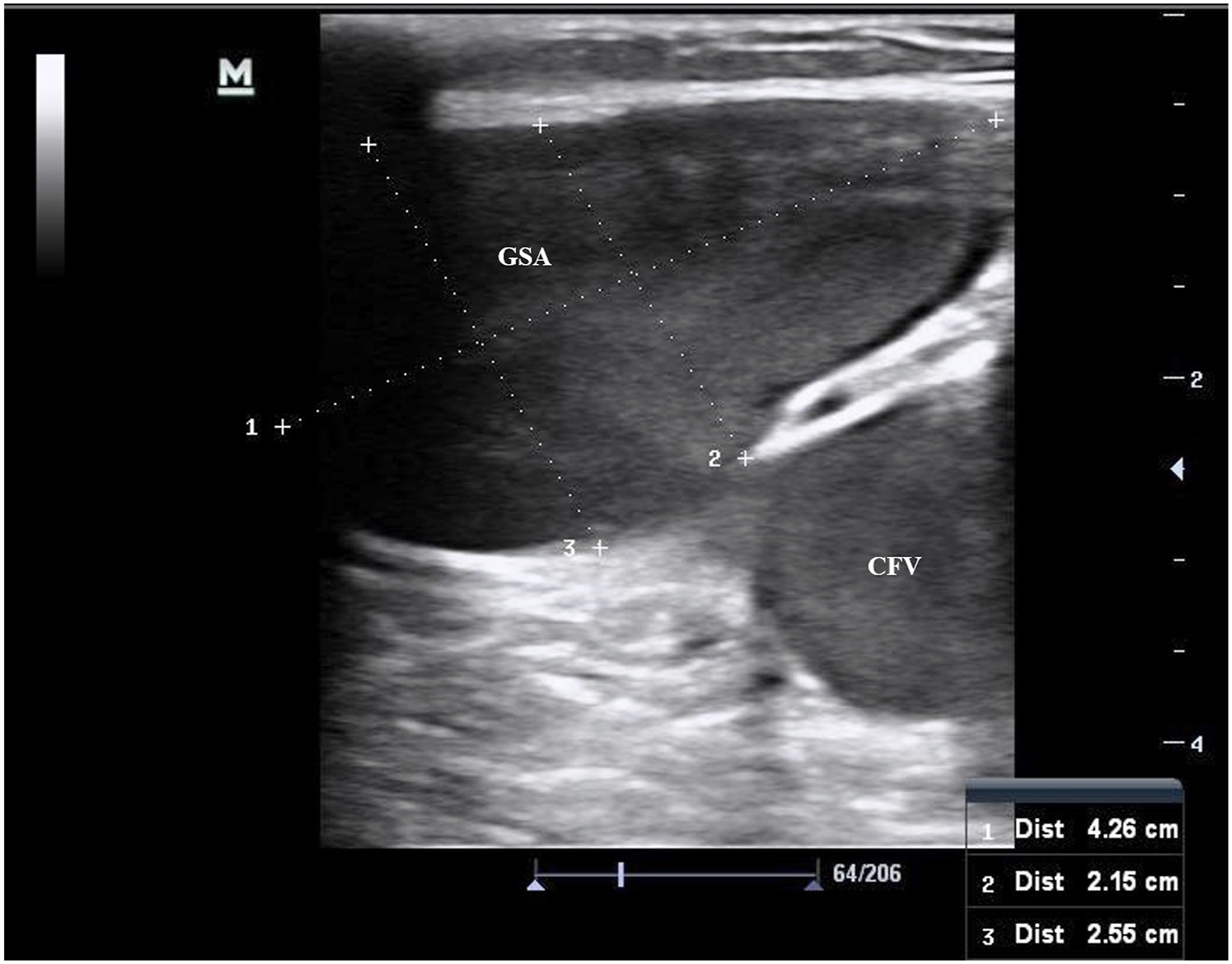
The next day after the procedure the diameter of the GSAs was reduced by half. No blood flow was detected in the treated area in nine patients. In one case we found free lumen of aneurysm with treated vein walls. At 2 weeks follow up all of the treated areas were closed, the diameters were insignificantly larger than after 1 day. At 6 months follow up saphenous aneurysms were absent in all of the patients (Figure 3). DUS image of the saphenous vein aneurysm at the SFJ level before (a), within 1 month (b) and within 6 months after treatment (c). GSA, great saphenous aneurysm. CFV, common femoral vein.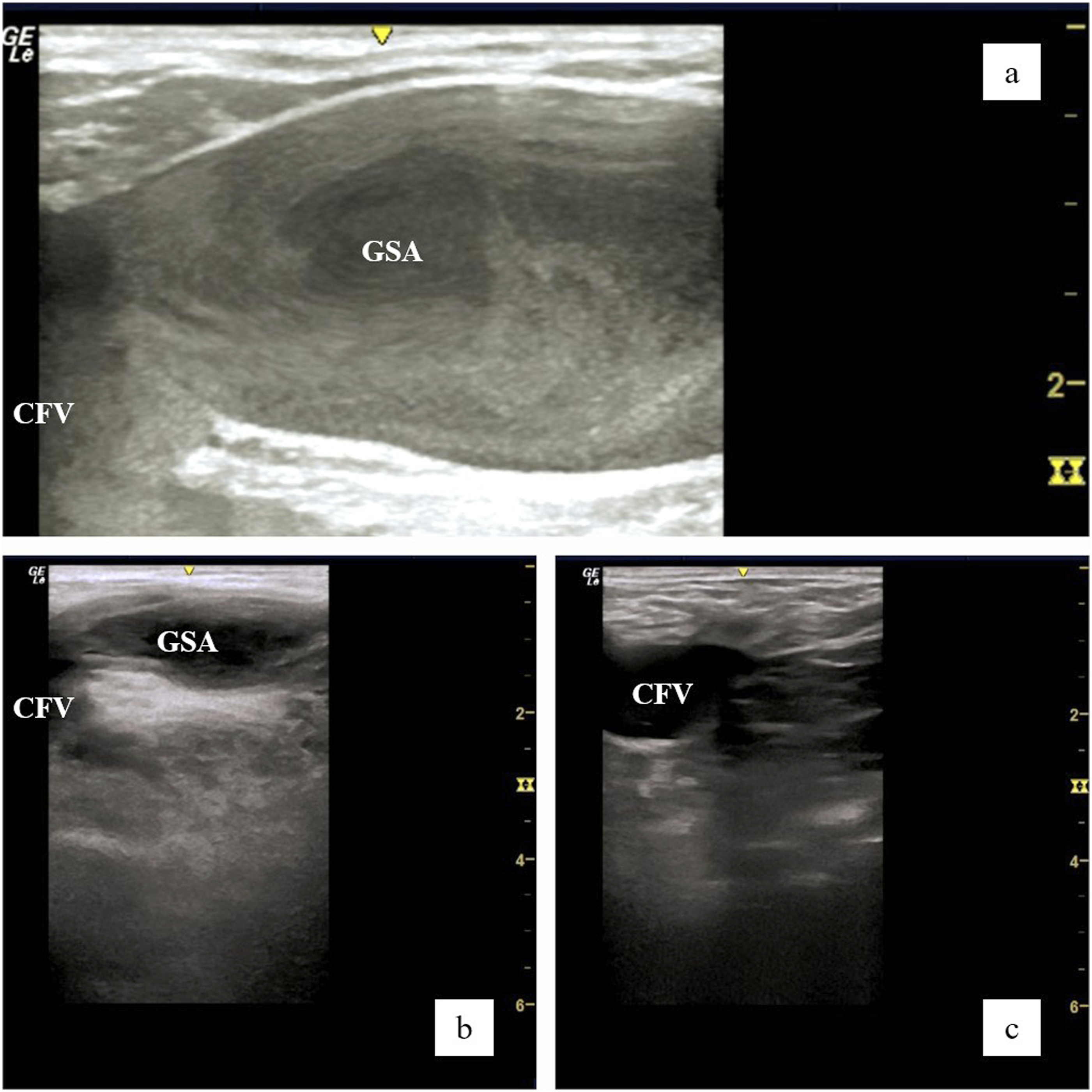
The efficacy end points achieved during the follow-up period.
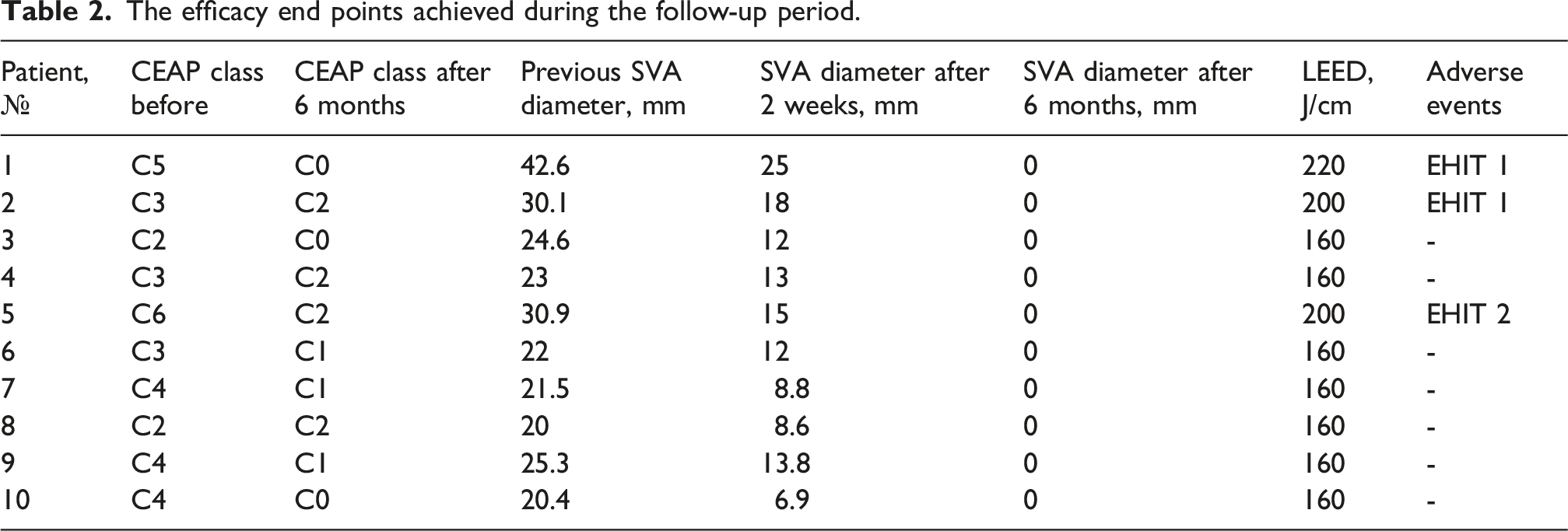
At the early post-operative visits there were no patients with symptoms of PE, two cases of EHIT 1, and one case EHIT 2. We noticed that EHIT appeared at different times (next day after the procedure and after 2 weeks) in patients with aneurysms more than 30 mm in diameter and it required the prescription of an anticoagulant therapeutic dose. No other adverse events were observed.
Discussion
There are enough studies about saphenous vein aneurysms. But many of them observed not only aneurysms. Moreno O. et al. found that the mean diameter of groin SVA was 1.9 ± 0.4 cm, Pascarella L. et al. measured the average diameter as 1.48 ± 0.53 cm · 1.8 ± 0.59 cm, Pavlovi MD. et al. calculated the median GSV aneurysm diameter as 21 (17.2 – 23.4) mm.2,8,9 However, the GSV diameter more than 20 mm is considered to be aneurysm. Furthermore, a configuration of SVA is important. Treatment of a spindle-shaped expansion (Figure 4) with EVTA is not a very difficult task.10,11 A complicated case is a berry aneurysm especially if it involves terminal valve (Figure 5). Bush RG and Bush P. consider that the aneurysmal dilation proximal or distal to the subterminal valve should be classified separately since treatment is different. The authors propose that aneurysmal dilations of the SFJ (includes junctional branches) be classified as Type Ia. Aneurysmal dilatation distal to the subterminal valve should be classified as Type Ib.
12
We believe that aneurysm Type Ia is the main reason for refusing EVTA and preference to open surgery. DUS image of the spindle-shaped great saphenous vein aneurysm. DUS image of the berry great saphenous vein aneurysm.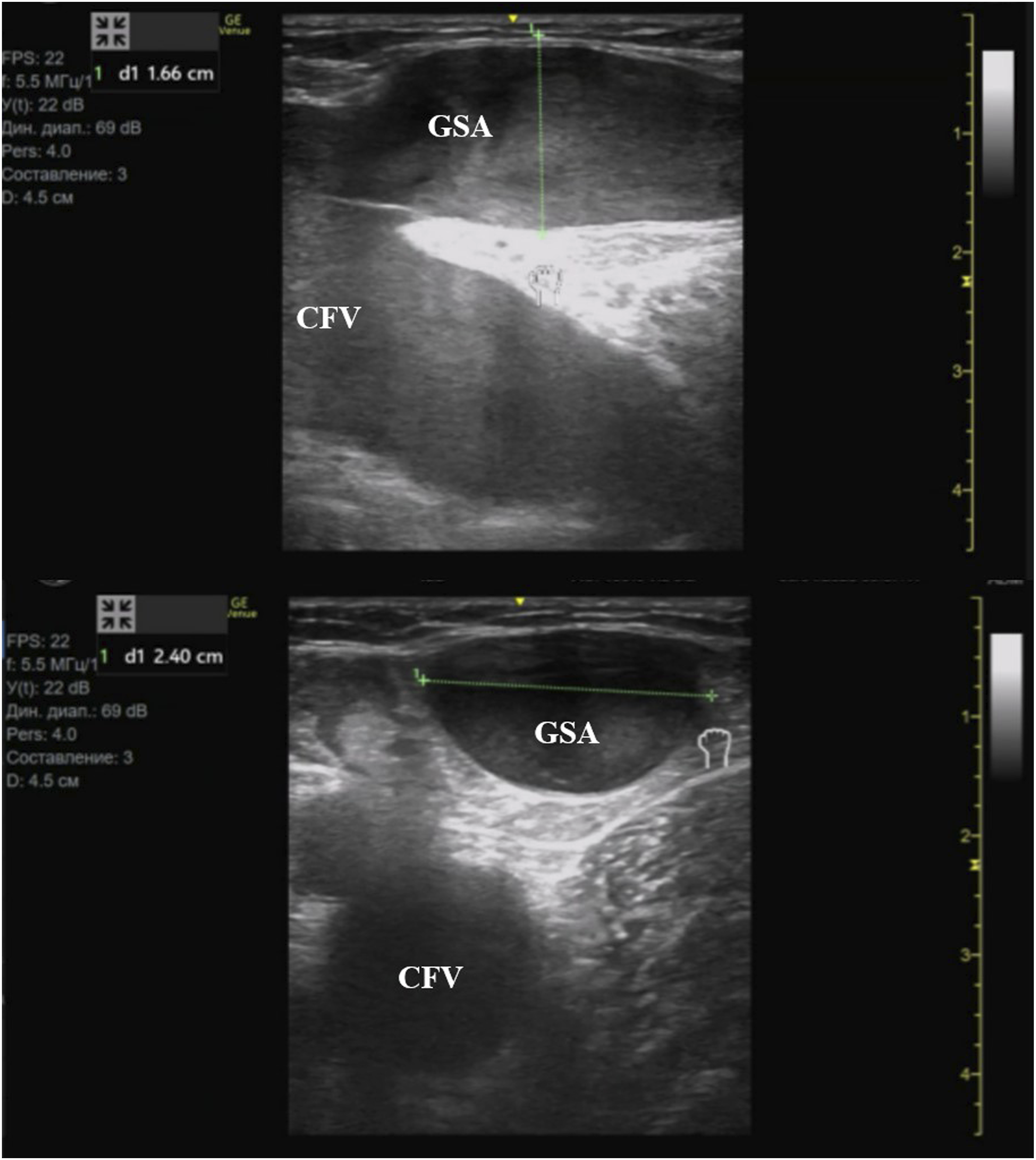
Based on histologic studies by Bush RG and Bush P. of both extrafascial varicose vein and venous aneurysm segments, the histologic findings are very similar. In both segments, there is smooth muscle hypertrophy to varying degrees. The intima is thickened as well as the adventitia with collagen infiltration. These findings are consistent with the end results of persistent venous hypertension; muscle hypertrophy and collagen breakdown with abnormal synthesis of proteins. 12 So, we can use the same methods for treatment of GSA as varicose vein with the difference that we should remove the intraluminal blood and make the aneurysm sac wall closer to the surface of the light guide lens to avoid the resorption of laser energy by blood. But it is difficult to remove the intraluminal blood from an aneurysm using only tumescent anesthesia. Dabbs EB. et al. suggested using a multi-pass technique. 13 They noticed that no colour flow was observed and successful complete fibrotic occlusion of the entire length of the treated GSV was confirmed in all cases. However, the authors did not actively follow-up on these patients over time for the purpose of this study. All the patients returned approximately 8 weeks after EVLA for a follow-up. So, the eventual condition of the veins remained unknown. We also do not possess the information about EHIT occurrence during 8 weeks. In our study all cases of EHITs disappeared at 4 weeks. In addition, it is not always possible to use a multi-pass technique in GSA especially in obese patients. Trendelenburg position also does not allow to evacuate all of remaining blood.
We evacuated the blood remaining in the lumen of the vein after tumescent anesthesia by using the new ELVeS 2ring Pro fiber (Biolitec AG, Ceram Optec). In our opinion, it allowed laser radiation to act directly on the aneurysmal wall, avoid the risk of carbonization of the fiber lens and achieve a good result of treatment. We used Radial 2ring fiber instead of Radial fiber since in the previous study it was established that carbonization and sticking during EVLA caused by excess temperature rise can be minimized by using Radial 2ring fiber compared with Radial fiber, coupled with the 1470 nm wavelength. 14
Despite the fact that we prescribed pre- and postprocedural thromboprophylaxis in patients with GSV aneurysms, we had tree cases of class 1-2 EHIT. It may well be true that this duration of thromboprophylaxis does not prevent EHIT and we need to use thromboprophylaxis for up to 2 weeks or more.
Limitations
Our study has some weaknesses. It has a non-comparative design and the study sample was small.
Conclusion
Sonographic and clinical 6-months follow-up showed that VALA is an effective procedure with an excellent technical result for the treatment of GSV aneurysm close to the junction (Type I). However, the best thromboprophylaxis strategy in this case remains to be debatable.
Footnotes
Ethical considerations
This study protocol was approved by the regional Ethics Committee of the Ryazan State Medical University (N0. 10, 06.03.2025).
Funding
This research was not funded by anyone.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
OB.
Contributorship
OB and DA researched literature and conceived the study. OB and DA were involved in protocol development, gaining ethical approval and data analysis. OB and DA were involved in patient recruitment. OB wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.