
Abstract
Objective
To analyze outcomes of initial combined arterial and venous interventions (AVI) compared with isolated venous interventions (VI) alone in patients with mixed arterial-venous ulcer (MAVLU).
Methods
Between 2012 and 2022, all patients presenting with MAVLU, defined as having a venous ulcer with a Toe Brachial Index <0.7 or an absolute toe pressure <60 mmHg. Two groups were identified: VI and AVI. The primary outcomes assessed were ulcer healing at 12 weeks and freedom from ulcer recurrence within 1 year.
Results
303 patients (57% female; mean age 59 ± 11 years) presented with active MAVLU; 44% underwent VI, and 56% underwent AVI. The Wound Bed Score was more severe in the AVI group compared to the VI group. In addition to medical and wound care therapies used across the entire cohort, venous ablation with thermal or nonthermal modalities was performed in 93% of cases, sclerotherapy in 61%, stab phlebectomy in 39%, and iliac vein stenting in 4%. In the AVI group, 76% of patients underwent endovascular arterial intervention, while 24% had open bypass procedures. All arterial procedures were successful and resulted in an increased TBI. Ulcer healing rates at 12 weeks were 9% for the VI group and 28% for the AVI group (mean; p = .01). At 1 year, freedom from ulcer recurrence was higher in the AVI group (87 ± 3%) compared to the VI group (64 ± 3%; mean ± SEM p = .01).
Conclusion
Compared to isolated venous interventions, combined arterial and venous interventions accelerate initial ulcer healing and reduce ulcer recurrence in MAVLU.
Introduction
The development of venous ulceration remains a significant public health issue, with up to 1% of the population suffering from a venous leg ulcer (VLU).1,2 Current treatment shows that healing rates in patients with a VLU and normal arterial perfusion range from 63% at 10 weeks retrospectively to 33% at 12 weeks prospectively.3–5 Clinical trials have demonstrated that early venous intervention can enhance ulcer healing or prolong the time to recurrence. 6 However, clinical trials on venous interventions have excluded patients with decreased arterial perfusion to ensure a more homogeneous population. Mixed arterial-venous disease can be present in up to 26% of patients with VLUs. 7 Evidence of concomitant arterial insufficiency (ankle-brachial index; ABI of <0.8) affects healing metrics for VLUs. 4 Limbs with a VLU and an ABI of <0.8 can take up to 19 weeks to heal, compared with 9 weeks for VLUs with an ABI of > 0.8. 4 This may be due to a lack of compression therapy because of the fear of compounding arterial malperfusion or due to the underlying arterial disease. Several authors have shown that a tailored compression regimen in patients with diabetes and arterial disease is effective without resorting to an arterial intervention.8,9 There is evidence to suggest that in the setting of a venous ulcer with an ABI of <0.5, the arterial disease should be addressed, which generally entails treating iliac and femoral artery disease. 10 There are differing views on whether to adopt a venous-only approach or a staged approach with an arterial intervention followed by a venous intervention for patients with MAVLU. 7 This study aims to analyze the outcomes of combined arterial and venous interventions compared to venous interventions alone among patients with MAVLU at a single center.
Patients and methods
Study design
This was a retrospective study. Between 2012 and 2022, all patients presenting with a de novo active VLU were surveyed. From this cohort, two groups were identified: those who had initial venous interventions (VI) only and those who had staged arterial and venous interventions (AVI). Arterial interventions were performed before venous interventions. Demographics, comorbidities, prior interventions, pathophysiology, pathology, Interventions, and adverse events were recorded. Consent was waived because patients were not directly studied, and the data collection was retrospective and de-identified. The study was approved by the institutional review board. The study conformed with the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines (https://www.strobe-statement.org/).
Setting
Patients were drawn from a single urban tertiary referral, level 1 trauma center in San Antonio associated with two urban wound care clinics.
Selection
Inclusion criteria were all patients with a de novo active VLU, in the presence of superficial truncal venous reflux (great saphenous vein - GSV; small saphenous vein - SSV and perforator - PERF) and without evidence of deep venous reflux on duplex imaging, and a Toe Brachial index (TBI) <0.7 or absolute toe pressure <60 mmHg. Patients with iliac venous obstructive disease and/or superficial reflux were also included. Criteria for superficial venous reflux were defined as retrograde flow duration >500 ms, and criteria for deep venous reflux were defined as retrograde flow duration >1000 ms in the femoral or popliteal segments. Patients with a history of deep venous thrombosis (DVT) were confirmed to have a normal deep venous system. Ulcers with atypical features were also excluded. Additionally, patients with recurrent venous ulcers were also excluded. Only one ulcer on the index leg per patient was included in this review to maintain the independence of observations and avoid bias based on patients presenting with bilateral ulcers.
Ulcer evaluation
The patients were clinically assessed using the Revised Venous Clinical Severity Score (rVCSS), which can be used to measure the disease severity of the venous disease. 11 Photographs of the wounds were obtained at the initial visit and at 4-weeks intervals/Prior to taking the digital images, the wound was cleansed with 0.9% saline solution. The lower limb with the ulcer was placed against a white background for the photograph. A ruler in cm was placed close to the ulcer and used as the reference object. The photograph was taken with a standard camera that had automatic white balance, high sharpness, and flash disabled. The camera was kept perpendicular to the wound (90°) and 50 cm away, moving closer or farther as necessary. Wound area measurements were obtained from the digital photographs using NIH ImageJ 1.53i software. 12 All wound tracings were subsequently verified by a blinded wound expert at the end of data collection. Based on these images, the ulcer was assessed by the Wound Bed Score 13 and the Margolis Score. 14 The Wound Bed Score (WBS) is based on nine criteria: Black Eschar (% wound area), Eczema/Dermatitis, Depth. Granulation tissue, Scarring, Color of wound bed (pink/red), Edema/Swelling, Resurfacing Epithelium, Exudate Amount. Each wound can have a maximum score of 16 (the best score), to a minimum score of 0 (the worst score) (see e-Appendix). 13 The Margolis Score is based on two criteria: Each wound was assessed by Ulcer Area (cm2) and Ulcer Duration (weeks), and each variable was scored from 0 to 2 and summed together, with the larger number reflecting a harder-to-heal wound (see e-Appendix). 14
Management
Diagnostic imaging
All patients presenting with a de novo venous ulcer underwent venous and arterial imaging. To determine the presence of venous disease, all patients underwent superficial and deep venous duplex ultrasound scanning to evaluate the limb for reflux. If there were abnormal findings in the common femoral vein or significant above-knee swelling, a concomitant iliac vein duplex was performed. To evaluate for arterial disease, all patients underwent an initial noninvasive evaluation on presentation, including ankle-brachial index (ABI) and/or toe-brachial index (TBI). In the presence of a low ABI or TBI, a vascular non-invasive or contrast study (duplex scan, arteriogram, or CT angiography) was obtained to define the anatomy.
Wound algorithm
Compression of the VLU was achieved with an Unna boot in accordance with current societal guidelines.1,15 Compression protocols were not altered after arterial intervention. Standard and PCR-based wound culture data were obtained in most cases, and appropriate antimicrobial therapy was used only in the presence of a positive culture. Skin substitutes were used after 4 weeks of compression, and in cases where the wound was not progressing, and there was an absence of an active infection. A maximum of 10 placements was performed on each wound over a 6-month period.
Venous algorithm
Following identification of superficial venous incompetence, great saphenous and small saphenous ablation was performed where there was >500 ms of reflux and appropriate anatomic criteria. In the presence of residual perforator reflux, perforator ablation was performed where there was a reversal of flow from the deep system to the superficial system of >500 ms, and where there was a diameter of more than 3.5 mm.
Arterial algorithm
Following identification of occlusive lesions in the lower extremity, endovascular or open intervention was performed at the discretion of the individual attending to attain maximal revascularization. • Endovascular Intervention: Following diagnostic angiography, intervention (angioplasty stenting or atherectomy) on femoral, tibial, and pedal vessels was performed whenever possible at the same setting with the patient receiving systemic heparin to ensure an activated clotting time (ACT) of 250 s, and completion angiography was performed to assess the final technical result. An attempt was made to intervene on as many vessels as possible during the first intervention. Attempts were made to secure two tibial vessel runoff to the foot with particular attention to the vessels associated with the appropriate angiosomes. Both antegrade and pedal access techniques were used during an endovascular intervention.16–23 • Open Procedures: Common femoral endarterectomy was performed using established techniques and vessels were patched with a bovine pericardial patch. Vein bypass using standard techniques was employed in patients with a suitable target vessel, acceptable venous conduit, and good pedal runoff. Both reversed, in situ, and non-reversed configurations were performed under general anesthesia.16–18,21–23 Prosthetic bypass was used where the vein was considered unsuitable in diameter <3.0 mm or length
Follow-up
After discharge, patients attended wound care and podiatric surgery to manage their foot wounds as frequently as necessary to ensure wound healing and renewed ambulation. Patients were followed by the vascular clinic and underwent routine duplex ultrasound follow-ups at 1, 3, and every 6 months following their procedure using criteria previously described. 21 During follow-up, angiography was only performed if non-invasive studies suggested restenosis/occlusion (positive duplex scan with a drop in toe-brachial index (TBI) of >0.1 and/or if the patient had recurrent symptoms (worsening ischemia and/or poor wound healing); angiography was performed as appropriate.16,21,24,25
Date variables
The definition of the variables used in the study are shown in the e-appendix.
Definition of outcomes
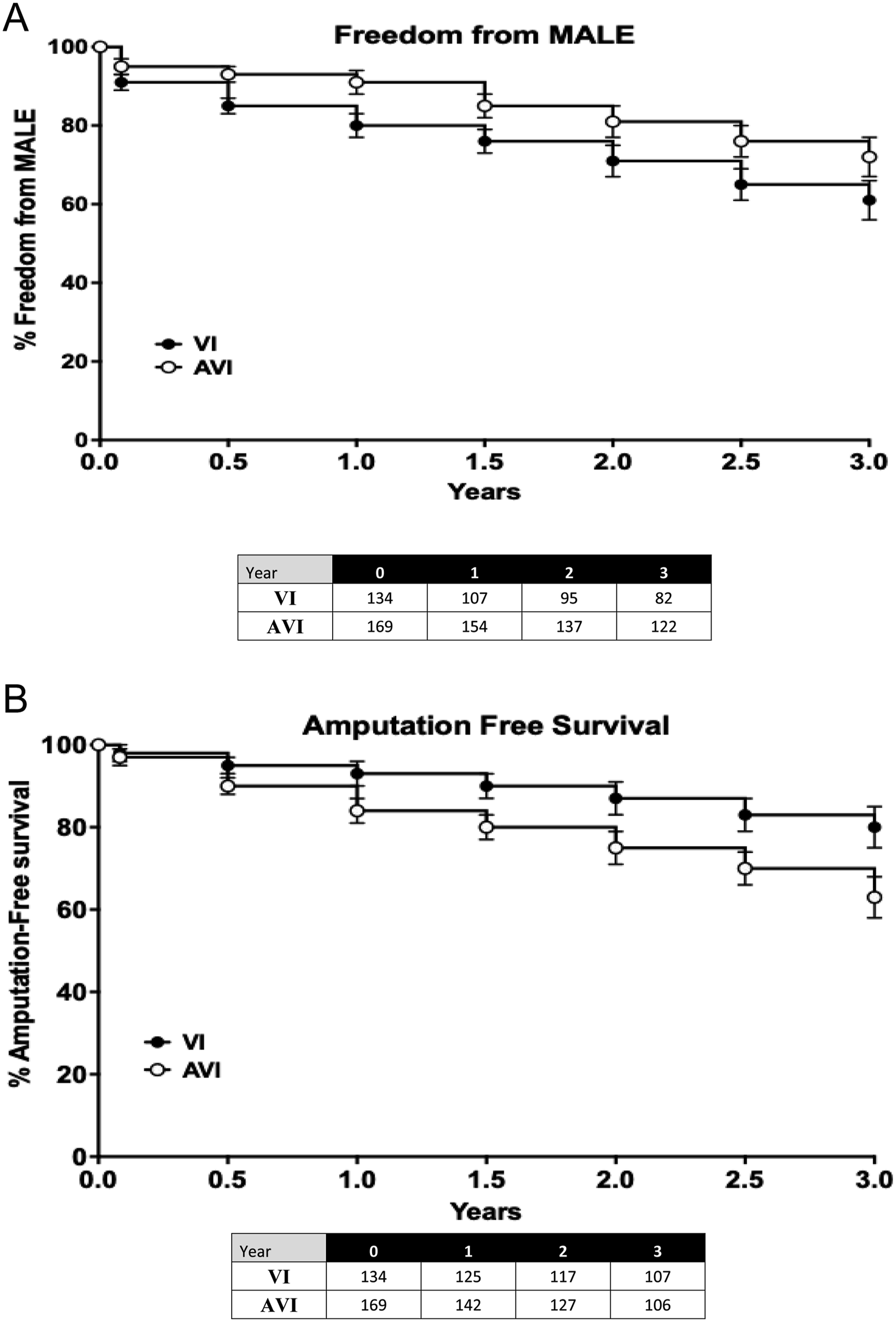
The primary outcomes were initial VLU healing at 12 weeks and freedom from recurrence of VLU within 1 year. A VLU was defined as a full-thickness defect of skin, most frequently in the ankle region, that fails to heal spontaneously and is sustained by chronic venous disease, based on venous duplex ultrasound testing, Initial healing was defined as complete epithelialization of the VLU, with no scab formation or drainage, sustained for at least two consecutive assessments over 4 week period, Recurrence was defined as the return of the VLU after it was deemed as initially healed. The secondary outcomes were Amputation-free survival (AFS) and Freedom from modified major adverse limb events (MALE). Amputation-free survival is defined as the duration of time a patient remains alive without undergoing a major limb amputation. Modified major adverse limb events is defined as major amputation (amputation above the ankle) or any venous or arterial open or percutaneous reintervention on the index leg.
Statistical analysis
Measured values are reported as percentages or mean ± SD. Non-parametric ANOVA or χ2 testing or Fisher exact test was used to analyze individual variables and significance compared to the VI group (Control group). Rates of initial Ulcer healing and Ulcer recurrence, Amputation-free survival, and freedom from modified MALE were calculated using life table analyses and presented as mean ± SEM. The log-rank test was used to determine differences between cohorts on life tables, with significance compared to the VI group. Univariate and multivariate analyses were performed to define factors impacting categorical outcomes. Univariate and multivariate Cox proportional hazard analysis was performed to determine factors affecting time-dependent outcomes. The models included all variables with a p = .05 in covariate analysis. A backward elimination procedure using a p = .2 was used to reduce each model. The results are expressed as an adjusted hazard ratio (HR) or an odds ratio (OR) as appropriate, with a corresponding set of 95th percent confidence intervals (CI). The VI group was used as the control group in these multivariable analyses. Analyses were performed using JMP software (version 9.0; SAS Institute, Cary, NC) and RStudio (version 1.2.5001; RStudio, Inc., Boston, MA).
Results
Patient population
Demographics, venous pathology and ulcer characteristics.
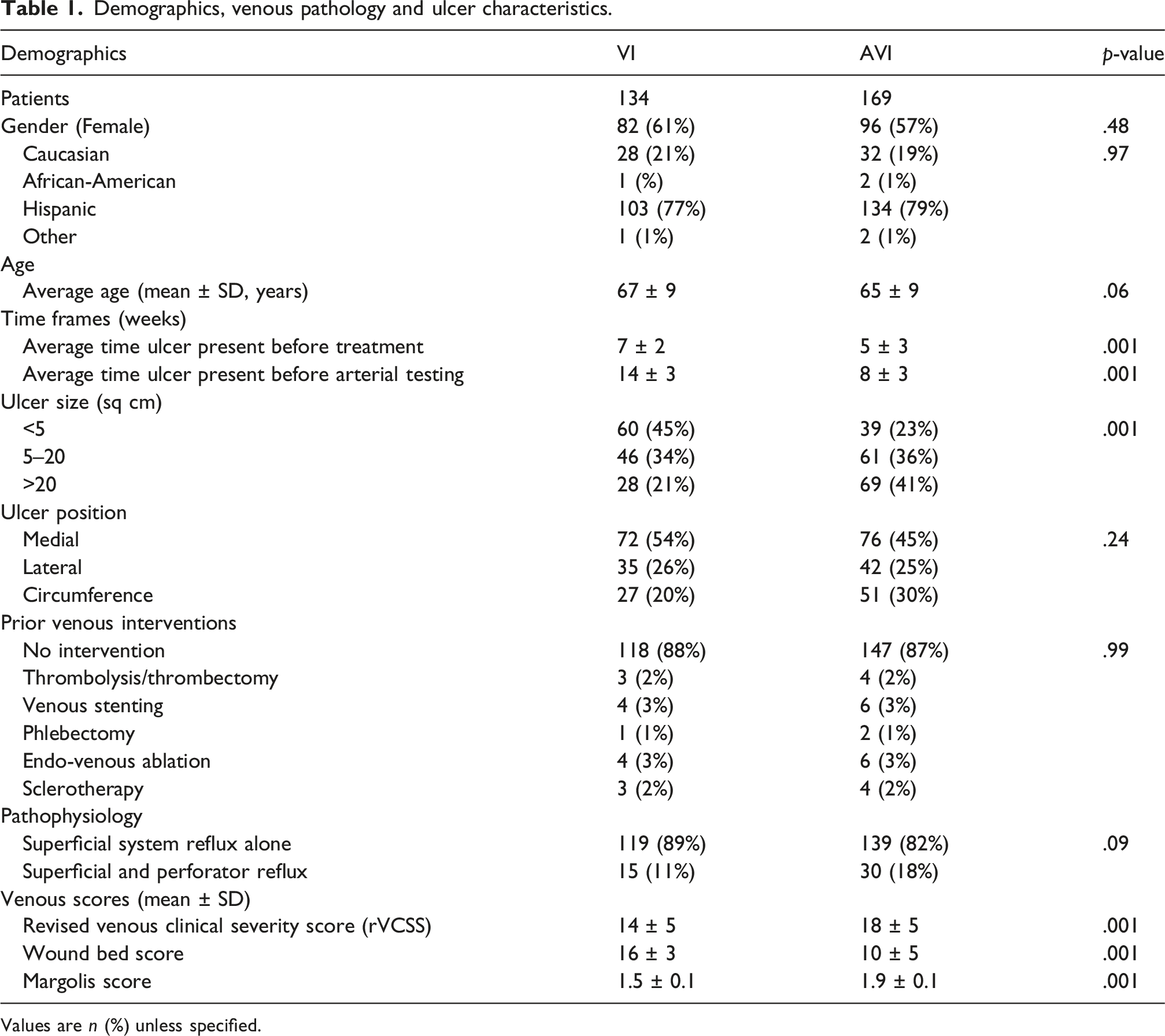
Values are n (%) unless specified.
Comorbidities.
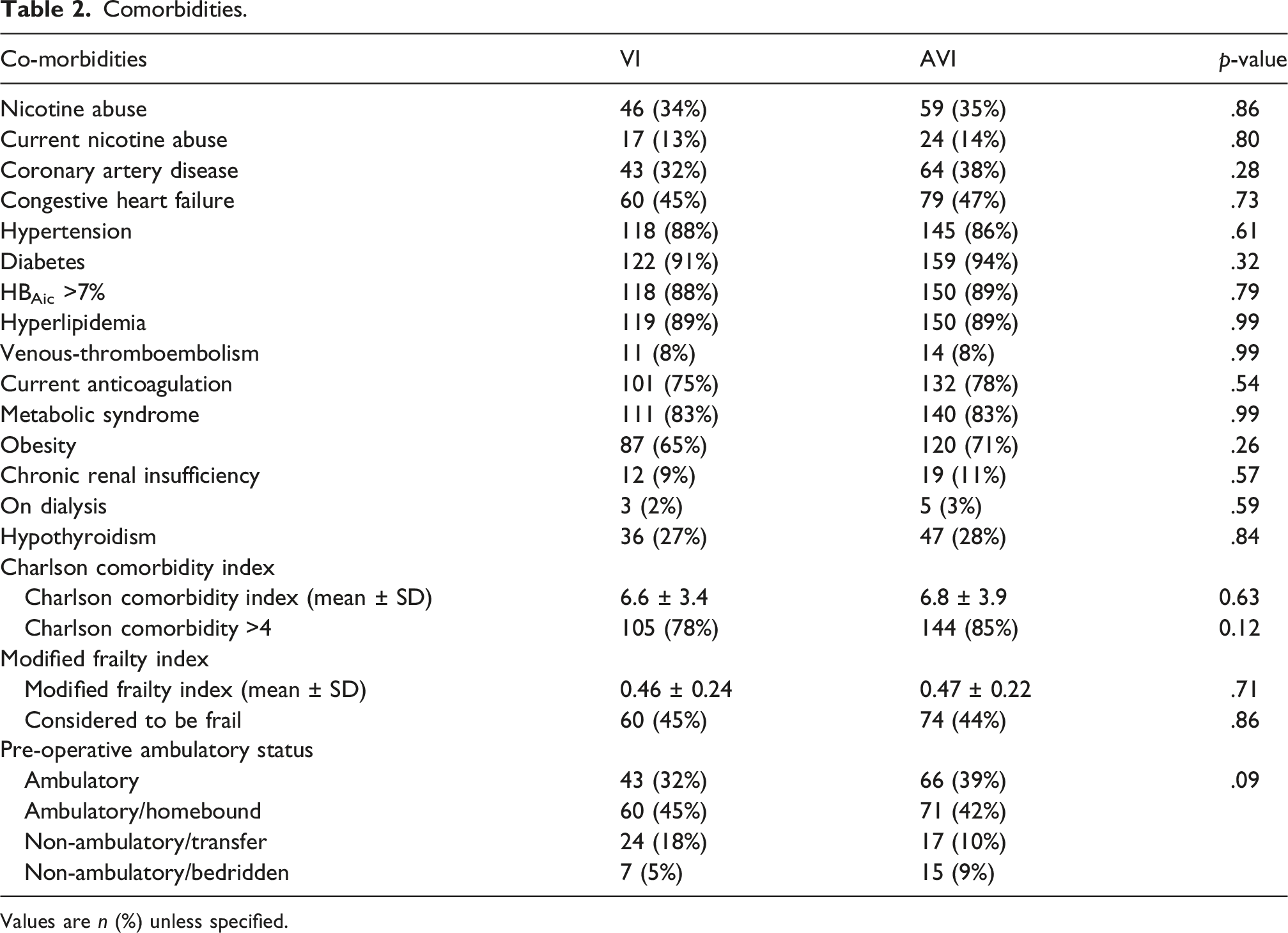
Values are n (%) unless specified.
Anatomic and hemodynamic presentation
The ulcerations in the AVI group were noted to be significantly larger than those in the VI group, but their locations on the leg were equivalent. Among the 303 patients, 100% had GSV incompetence, 33% had SSV incompetence, and 11% had perforator incompetence. Of the patients undergoing arterial intervention, 9% had significant iliac disease, 44% had superficial femoral arterial disease, 23% had tibial arterial disease, and 24% had multi-level disease. There were no differences in venous pathology between the groups, and prior venous or arterial interventions were equivalent (Table 1 and Appendix Table 1). The rVCSS, Wound Bed Score, and Margolis score were higher in the AVI group compared to the VI group (Table 1). Absolute toe pressures were significantly lower in the AVI group compared to the VI group on initial presentation (Appendix Table 1). When ABIs of the index limb were stratified across the entire cohort, 34% had an ABI <0.5, and 66% had an ABI of 0.5–0.8. In the AVI group, 47% had an ABI of <0.5 and 53% had an ABI of 0.5–0.8, and in the VI group, 18% had an ABI of <0.5 and 82% had an ABI of 0.5–0.8 (AVI vs VI; P = .001). The distribution by Trans-Atlantic Inter-Society Consensus (TASC)-II for iliac disease and by Global Limb Anatomic Staging System (GLASS) category for the femoro-popliteal and infra-popliteal segments in the AVI group are shown in Appendix Table 1.
Interventions
Venous and Ulcer interventions.
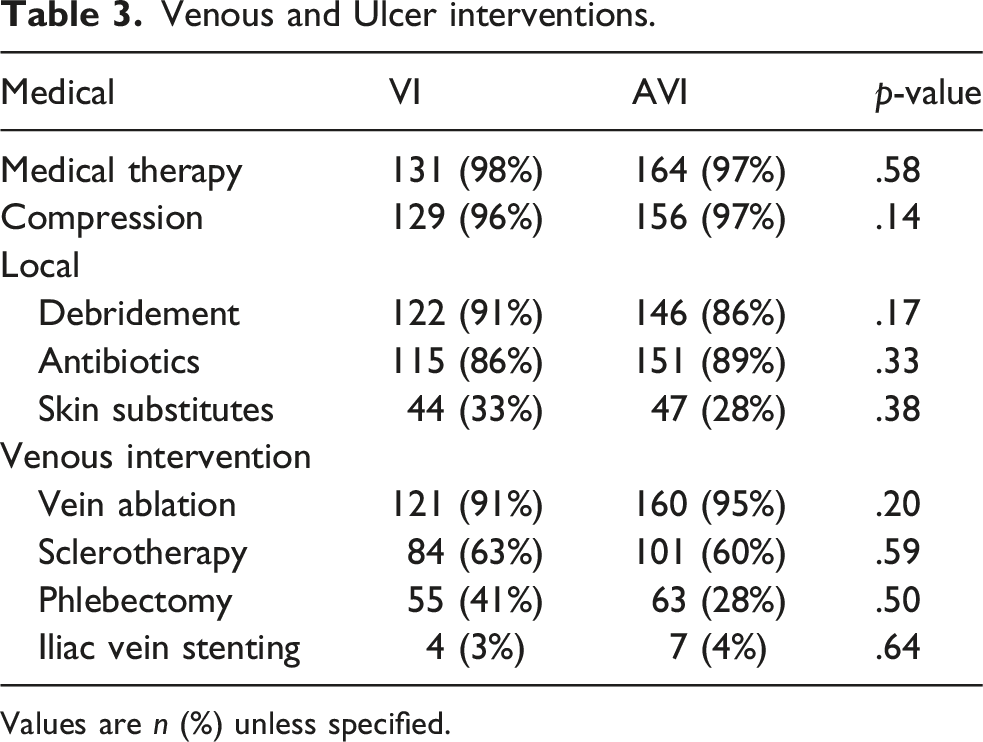
Values are n (%) unless specified.
Venous interventions were performed in the majority of patients with superficial and perforator incompetence. Venous ablation using either thermal or nonthermal modalities was performed in 93% of the cases, sclerotherapy in 61%, stab phlebectomy in 39%, and iliac vein stenting in 4%. The groups were equivalent regarding venous interventions (Table 3).
Of those undergoing arterial intervention followed by venous interventions, 76% of patients underwent endovascular intervention, and the remainder underwent bypass surgery (all were femoropopliteal bypasses). Endovascular interventions were performed in 76% of the patients: 26% had an iliac intervention, 24% had a femoropopliteal intervention, and 15% had a proximal tibial intervention. Multilevel endovascular interventions were performed in 11% of the patients. Open procedures were performed in 24%: 12% were femoropopliteal bypasses (87% of vein and 13% with prosthetic), while the remainder (15%) were common femoral artery endarterectomies. Hybrid procedures consisted of common femoral artery endarterectomies with ipsilateral iliac stenting in 5%. There was an average 0.20 ± 0.13 mmHg increase in TBI after arterial intervention, with 77% of the patients achieving an increase of >0.1 in TBI at 1 month. Following arterial intervention in the AVI group, 7% had an ABI of <0.5, 11% had an ABI of 0.5–0.8, and 82% had an ABI >0.8. The median time between arterial intervention was 3 weeks (range 2–6 weeks) for endovascular interventions and 9 weeks (range 5–12 weeks for open surgical interventions. Median follow-up was 38 months (15–41 months), with 11% of patients lost to follow-up.
Early outcomes
Immediate outcomes.
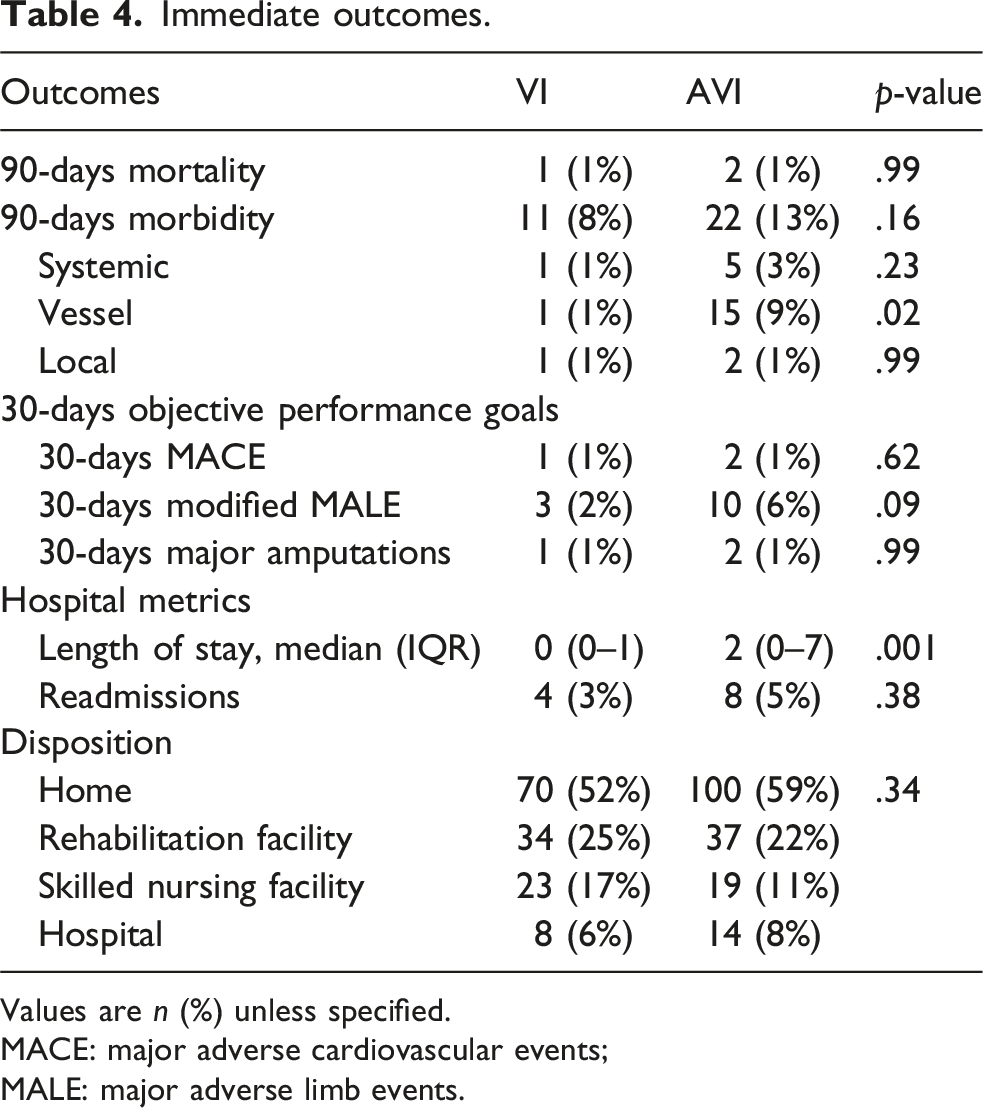
Values are n (%) unless specified.
MACE: major adverse cardiovascular events; MALE: major adverse limb events.
Crossover late interventions in VI group
In the VI group, 31% of patients with a primary VLU had an unplanned arterial intervention after their venous intervention during follow-up to facilitate wound healing. The median time to arterial intervention was 11 weeks (range 7–16 weeks). Indications for the crossover were slow healing, prompting arterial studies, and early recurrence or the development of arterial symptoms. These cases were considered major adverse limb events and censored from the initial healing and VLU recurrence analysis of the VI group. By multivariate analysis, a longer time before presentation (p = .04), wound size >20 sq cm (p = .02), increasing wound bed scores (p = .01), a Charlson Comorbidity Index >4 (p = .01) and ABI <0.5 (p = .01) were associated with crossover.
Late outcomes
Initial ulcer healing was 9 ± 2% (mean ± SEM) and 29 ± 2% at 12 weeks (p = .001) and 46 ± 4% and 65 ± 4% at 24 weeks for VI and AVI, respectively (p = .03; Figure 1(A)). By Cox proportional hazard analysis, wound size >20 sq cm (p = .03), wound bed severity (p = .03), Charlson Comorbidity Index >4 (p = .02), presence of frailty (p = .02), increasing wound bed scores (p = .01), and venous intervention alone (p = .01) were associated with poorer initial ulcer healing. At 3 years, freedom from ulcer recurrence was 64 ± 3% (mean ± SEM) and 87 ± 3% at 1 year (p = .01) and 32 ± 5% and 58 ± 5% for VI and AVI, respectively (p = .02; Figure 1(B)). By Cox proportional hazards analysis, a Charlson Comorbidity Index greater than 4 (p = .02), the presence of frailty (p = .02), and the occurrence of an arterial MALE or venous intervention alone (p = .01) were associated with ulcer recurrence. In the AVI group, limb-based patency was 68 ± 4% (mean ± SEM) at 3 years. By Cox proportional hazard analysis, lower limb-based patency was associated with diabetes (p = .04), chronic renal insufficiency (p = .03), Charlson Comorbidity Index >4 (p = .04), and presence of frailty (p = .02). Freedom from modified MALE was 61 ± 5% (mean ± SEM) and 72 ± 5% for VI and AVI, respectively (p = .04; Figure 2(a)). Events that contributed to the loss of freedom from modified MALE were endovascular reintervention, arterial intervention after a venous intervention, and major amputation. In Cox proportional hazard analysis, no factor indicated a need for intervention for MALE. Amputation-free survival was 80 ± 6% and 63 ± 5% for VI and AVI groups at 3 years, respectively (p = .01; Figure 2(a)). By Cox proportional hazard analysis, a Charlson Comorbidity Index greater than 4 (p = .02), the presence of frailty (p = .02), and ulcer recurrence (p = .03) were associated with lower amputation-free survival. The life table curves for time to initial healing (A), and freedom from recurrence (B) are shown for the two intervention groups: Venous intervention - VI (•) and arterial and venous intervention - AVI (○). Data are the mean ± standard error of the mean (SEM) and number at risk shown in the table where appropriate. No error bars are displayed if the standard error of the mean is >10%, and the data set terminates if the number at risk is <10. The log-rank test was used to determine differences between groups on life tables. The life table curves for freedom from MALE (A), and amputation free survival (B) are shown for the two intervention groups: venous intervention - VI (•) and arterial and venous intervention - AVI (○). Data are the mean ± standard error of the mean (SEM) and number at risk shown in the table where appropriate. No error bars are displayed if the standard error of the mean is >10%, and the data set terminates if the number at risk is <10. The log-rank test was used to determine differences between groups on life tables.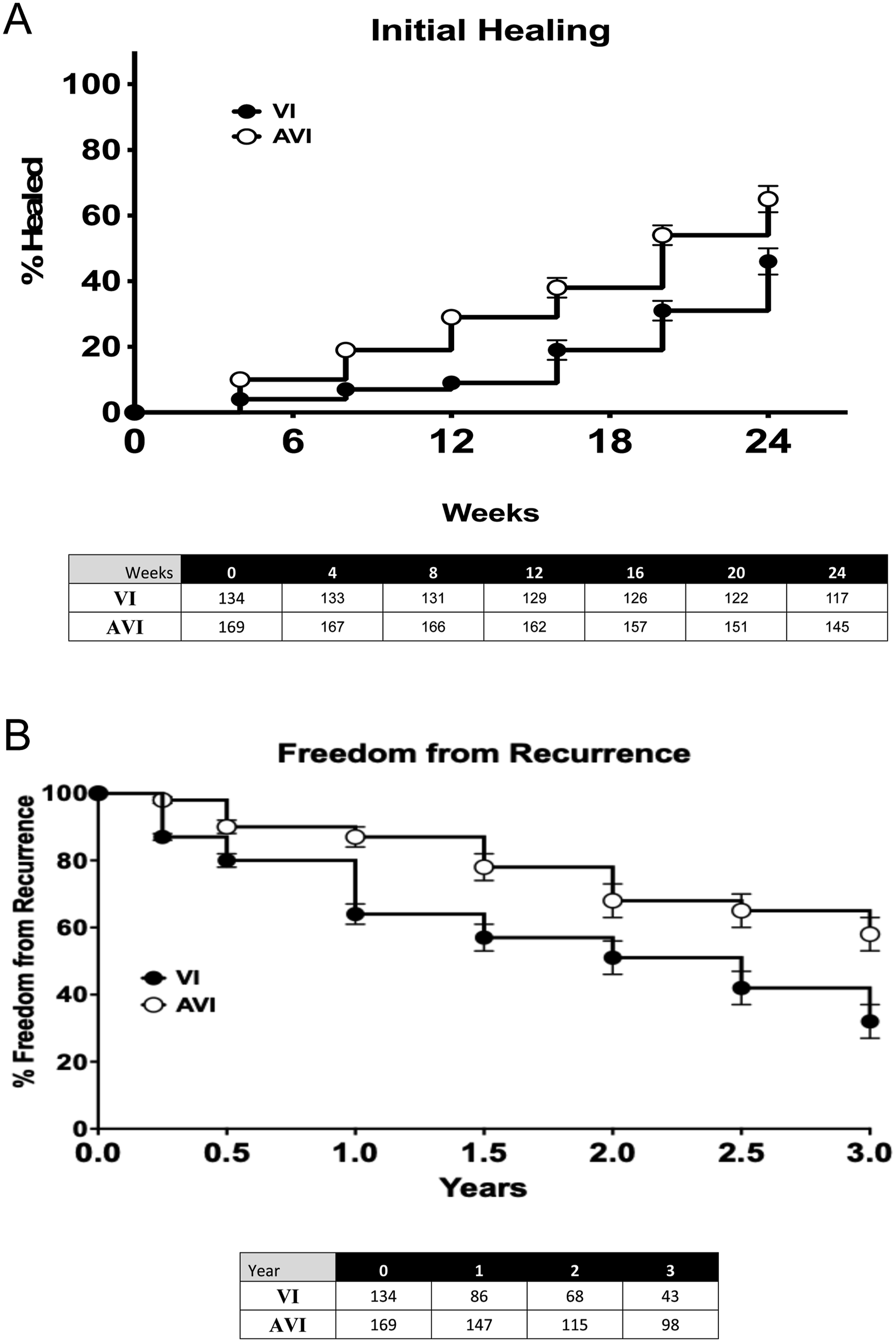
Discussion
In this current single-center retrospective study, approximately 27% of patients presenting with a VLU had evidence of arterial insufficiency as determined by TBI. In those patients with MAVLU, those who underwent VI had similar venous pathophysiology on duplex imaging as the AVI group. There was a significant increase in presentation time before intervention in patients who underwent VI compared to those who underwent AVI. Furthermore, the time to obtain arterial testing was also longer in those who underwent VI. The initial ulcer sizes were larger, and the wound bed scores were more severe in the AVI group than in the VI group. An initial larger ulcer size and higher wound bed scores correlated with reduced time to presentation and earlier arterial testing. The TBI was significantly lower in the AVI group compared to the VI group. Both groups had a similar treatment profile for their venous disease, and those initially treated for arterial disease predominantly had iliac and femoropopliteal interventions. Patients in the AVI group had an accelerated initial wound healing rate compared to the VI group and a lower VLU recurrence rate. However, those undergoing AVI had a higher MALE rate and a lower AFS in the longer term compared to those who underwent VI, which was related to the severity of the underlying arterial disease.
Marin et al., 26 compared clinical presentation and ulcer characteristics between patients presenting with MAVLU and those with a VLU. In their report, the authors did find that the surface areas of the MAVLU and the VLU were similar, but the MAVLU were considered to be deeper and have a greater eschar burden. This would support our data that wound bed scores are worse in MAVLU treated by AVI. Patients with MAVLU tended to present more rapidly to medical attention, usually having a shorter ulcer duration at initial assessment. 26 Furthermore, in another study on chronic leg ulcers with arterial insufficiency, the only risk factor associated with slower wound closure was initial wound size on presentation, 27 The current study expands on these findings and shows that in a population of patients with a MAVLU, those who undergo an arterial intervention followed by a venous intervention present faster, have more rapid arterial testing, and have larger, more complex wounds compared to those MAVLU that undergo venous interventions alone. It shows that there is a correlation between the size and complexity of the wound and the pattern of clinical interventions performed.
The mainstay of care for a VLU is compression therapy and local wound care. Multiple reports have demonstrated that initial healing of the VLU with intact arterial perfusion can be achieved in approximately 10 weeks. In addition to compression and wound care for VLU, there is sufficient evidence to show that the interruption or ablation of incompetent superficial veins will result in improved healing of VLUs and lead to increased intervals for ulcer recurrence.28–31 In a scoping review of clinical practice guidelines for venous leg ulcer (VLU) management, all recommend below-knee compression to improve healing outcomes after calculating the ankle-brachial index to rule out significant arterial disease. However, there is a lack of consensus and a lack of clear guidance in relation to the specific ABI range where standard compression therapy can be used and where modified compression can be used. 8 A recent systematic review suggested that modified compression therapy (MCT) has a role in selected cases of MAVLU in those with moderate PVD (ABI 0.5–0.8) 32 There is a consensus that an ankle-brachial index of less than 0.5 or an ankle pressure of <60 mmHg, necessitates revascularization first, and compression therapy is contraindicated prior to that. 33 In the current study, patients were offered standard compression or modified compression based on their presenting TBI during the efforts to obtain initial healing of the VLU in the MAVLU population. After a systematic review, Alagha et al. found that there were no direct comparisons of a strategy of venous interventions first (either modified compression, surgery, or ablation) compared to arterial intervention first in patients with MAVLU. 34 In addition, there is little data on the use of therapies stratified by the baseline ABI of 0.5 to 0.85 and ABI <0.5. 34
Several reports have demonstrated that arterial revascularization can expedite MAVLU healing and improve quality of life.10,35 Open surgical revascularization heals about 60% of MAVLU patients, although subsequent venous intervention may be needed in a staged manner. 36 Karkos and associates support the use of combined arterial and venous interventions in a small study by demonstrating in their series that there was a higher healing rate with concomitant revascularization and venous intervention. 37 Early reports suggested that in patients with MAVLU and moderate arterial disease (ABI 0.5–0.8), revascularization should be reserved for those who failed conservative management with supervised modified compression therapy (ulcers increasing in size, new ulcers developing, and increased pain).10,33,38 The progress in endovascular techniques and outcomes has shifted this approach to a more aggressive interventional strategy. Lantis JC and colleagues 35 performed only percutaneous transluminal angioplasty (PTA) for 27 patients with MAVLU and ABI <0.7, subsequently followed by medical management, including compression therapy initiated 6–10 days after the endovascular intervention. No venous interventions were performed. This revascularization strategy, combined with medical therapy, resulted in an initial healing rate of 75% at 10 weeks, which increased to 100% at 22 weeks after the endovascular intervention. Georgopoulos et al. reported that successful revascularization in MAVLU patients, as demonstrated by normalization of ABI post-operatively, was followed by compression therapy. The arterial intervention combined with the best medical management, including compression, significantly shortened healing time compared to those patients who received compression-only (16.6 ± 2.6 weeks vs 24.7 ± 3.2 weeks, p < .001). 10 In the current study, arterial interventions, when coupled with a venous intervention, did accelerate both initial VLU healing and recurrence. Importantly, those patients in the AVI group experienced higher MALE rates and lower amputation-free survival than those in the VI group. This likely reflects a greater arterial burden in the patients than in those in the VI group as was indicated by the lower hemodynamic parameters at presentation.
This study is the first to report crossover events in the MAVLU patients. Among patients with a primary VLU who underwent VI initially, 31% underwent an unplanned arterial intervention during follow-up to facilitate wound healing. The crossover was associated with a longer time before the presentation of VLU, which may indicate poorer access to healthcare and health insurance or poorer health literacy. Patients also had more comorbidities as determined by Charlson comorbidity scores >4. Furthermore, an initial lower ABI (<0.5) was associated with a crossover event. Upon presentation, the size and severity of the VLU were also important findings consistent with the findings of Marin et al., 26 and led to crossover from VI group to a delayed arterial intervention.
This study has limitations. It is retrospective; the treatment protocols were not driven by a standard protocol but rather by individual attending decision-making, which may have created inherent bias and may not make the two treatment groups fully comparable. It is also from a specific region with a distinct population, and thus, the results may not be generalizable. It is also important to note that both scientific information and technology evolved over the study period.
In conclusion, approximately 27% of patients presenting with active venous leg ulcers (VLUs) demonstrate arterial insufficiency. On presentation, MAVLUs are larger and have more severe wound severity. Initial ulcer healing and freedom from ulcer recurrence are superior in AVI relative to VI. Up to one-third of patients will crossover during follow-up to receive arterial interventions in the VI group. In the presence of impaired arterial perfusion, combined venous and arterial interventions accelerate wound healing and decrease ulcer recurrence in MAVLU.
Supplemental material
Supplemental Material - Current outcomes of interventions to treat mixed arterial-venous ulcers
Supplemental Material for Current outcomes of interventions to treat mixed arterial-venous ulcers by Joseph P. Hart, Mona Li and Mark G. Davies in Phlebology.
Footnotes
Author’s note
Presented at the International Venous Congress (Miami, FL; April 18 - 20, 2024).
Author contributions
Study design: all authors. Obtain data: all authors. Statistical analysis: all authors. Data interpretation: all authors. Manuscript draft: all authors. Critical revision: all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Mark G Davies.
Supplemental material
Supplemental material for this article is available online.
Appendix
Hemodynamics and GLASS disease grading. Values are n (%) unless specified. TASC II: Trans Atlantic Societal Consensus II; GLASS: Global Limb Anatomic Staging System.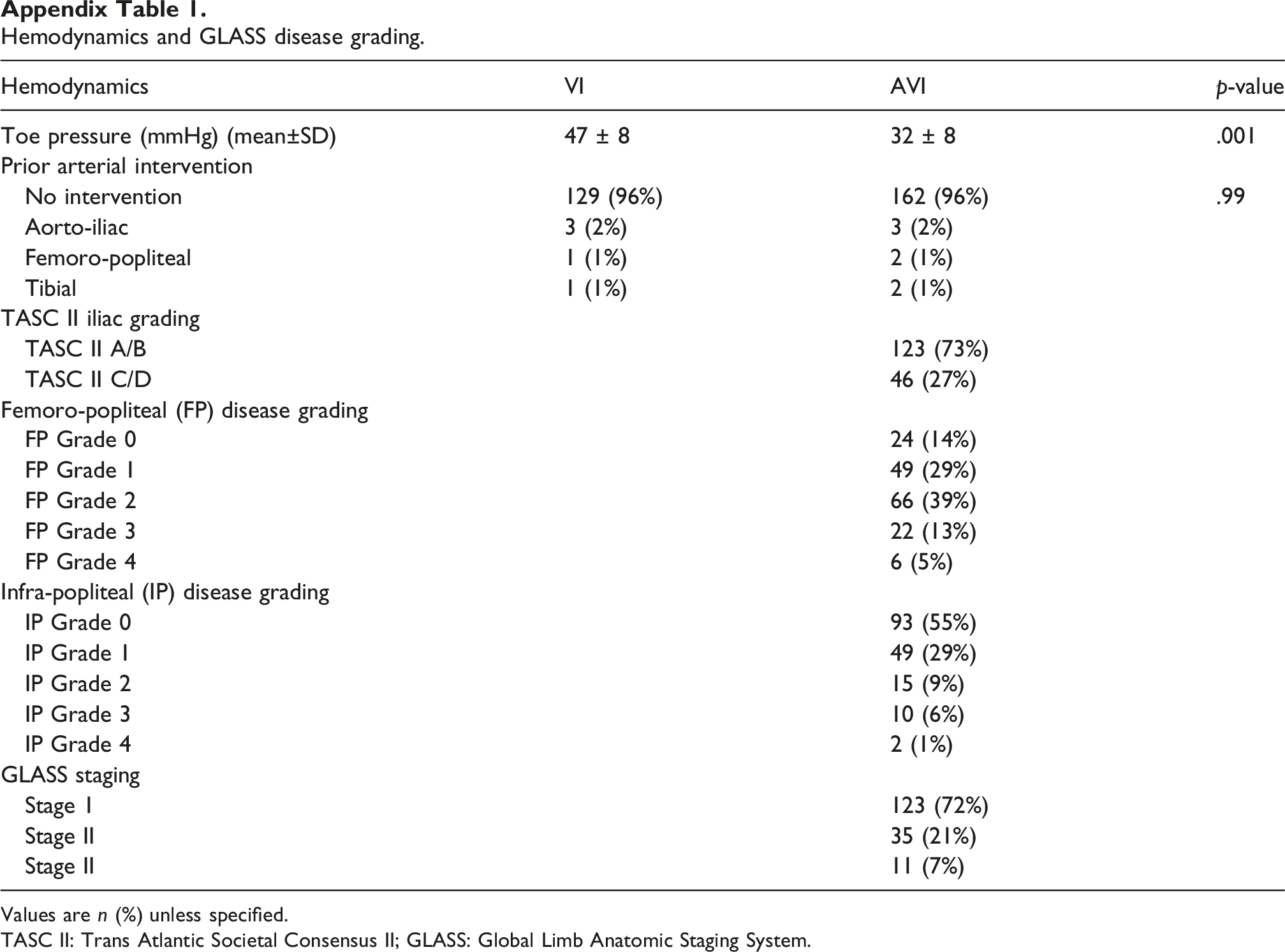
Hemodynamics
VI
AVI
p-value
Toe pressure (mmHg) (mean±SD)
47 ± 8
32 ± 8
.001
Prior arterial intervention
No intervention
129 (96%)
162 (96%)
.99
Aorto-iliac
3 (2%)
3 (2%)
Femoro-popliteal
1 (1%)
2 (1%)
Tibial
1 (1%)
2 (1%)
TASC II iliac grading
TASC II A/B
123 (73%)
TASC II C/D
46 (27%)
Femoro-popliteal (FP) disease grading
FP Grade 0
24 (14%)
FP Grade 1
49 (29%)
FP Grade 2
66 (39%)
FP Grade 3
22 (13%)
FP Grade 4
6 (5%)
Infra-popliteal (IP) disease grading
IP Grade 0
93 (55%)
IP Grade 1
49 (29%)
IP Grade 2
15 (9%)
IP Grade 3
10 (6%)
IP Grade 4
2 (1%)
GLASS staging
Stage 1
123 (72%)
Stage II
35 (21%)
Stage II
11 (7%)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.