
Abstract
Introduction
Down’s syndrome is a genetic disorder attributed to chromosomal abnormality (Trisomy 21). Global estimation of the incidence of the condition is 1 in 1,000 to 1 in 1,200 live births. 1 Down’s syndrome is characterized by several clinical symptoms which include orthopaedic, cardiovascular, neuromuscular, visual, cognitive and perceptual impairments. It is the most common genetic cause of developmental disability and affects both the gross motor and fine motor skills of children. Several studies have demonstrated that individuals with Down’s syndrome have deficits in eye–hand coordination, laterality, visual motor control, reaction time, strength and balance. 2 – 9
Children with Down’s syndrome have been noted to have reduced strength of the hip abductor and knee extensors as compared to children without Down’s syndrome. 3 Cioni et al. concluded that children and adolescents with the condition have reduced quadriceps strength when compared to children without mental retardation and with mental retardation without Down’s syndrome. They also reported that adolescents did not demonstrate the physiological increase in muscle strength that typically occurs by 14 years of age. 4 Muscle strength, especially the lower-extremity strength of individuals with mental retardation, including Down’s syndrome, is of fundamental importance to their overall health and their ability to perform daily activities. 5 Thus the preservation of muscle strength at a satisfactory level is necessary for the activities of daily living.
Studies done to determine the effect of strength training in Down’s syndrome are few and have been done in the adult population (24–26 years). 10,11 The study done by Tsimaras and Fotiadou 10 documented a significant improvement in leg strength following a 12-week intervention as measured using a isokinetic dynamomter. However, in a recent study performed by Taylor et al. 11 the intervention group showed an improvement in the upper limb endurance but no difference in the lower limb muscle performance as measured using 1RM. A case study has been carried out to determine the combined effects of strength and aerobic conditioning in a 10.5-year-old child with Down’s syndrome, showing improvements in strength after a six-week exercise protocol. 12 Strength training has shown positive results in children with cerebral palsy without any documented adverse effects. 13 – 16 However, literature for the same in children with Down’s syndrome is lacking.
Additionally, postural deficits have been identified in children with Down’s syndrome. Shumway-Cook and Woollacott 7 found that postural responses to loss of balance were slow in young children with Down’s syndrome, and they concluded that these responses were inefficient for maintaining stability.They also suggested that balance problems in these children occur not due to hypotonia but from defects within higher level postural mechanisms. Conolly et al. 9 compared the motor skills of children with and without Down’s syndrome using Bruininks Osteresky Test of Motor Proficiency (BOTMP), and found that children with Down’s syndrome scored significantly lower in the balance subset than the comparison group.
Balance training in children with Down’s syndrome has been studied by Wang et al. 17 who implemented a programme of vertical and horizontal jump training for 14 children with Down’s syndrome and children with mental retardation without Down’s syndrome for six weeks and noted significant improvement in the balance scores as measured by balance sub-test in the BOTMP. However, this study was not done exclusively on children with Down’s syndrome so the results cannot be generalized since other studies show that children with Down’s syndrome score lower than children with mental retardation without Down’s syndrome in the balance subset of BOTMP. 9 There is no conclusive evidence on the effect of strength and balance training in children with Down’s syndrome. So, the aim of this study was to determine the effect of a strength and balance training programme in these children
Methods
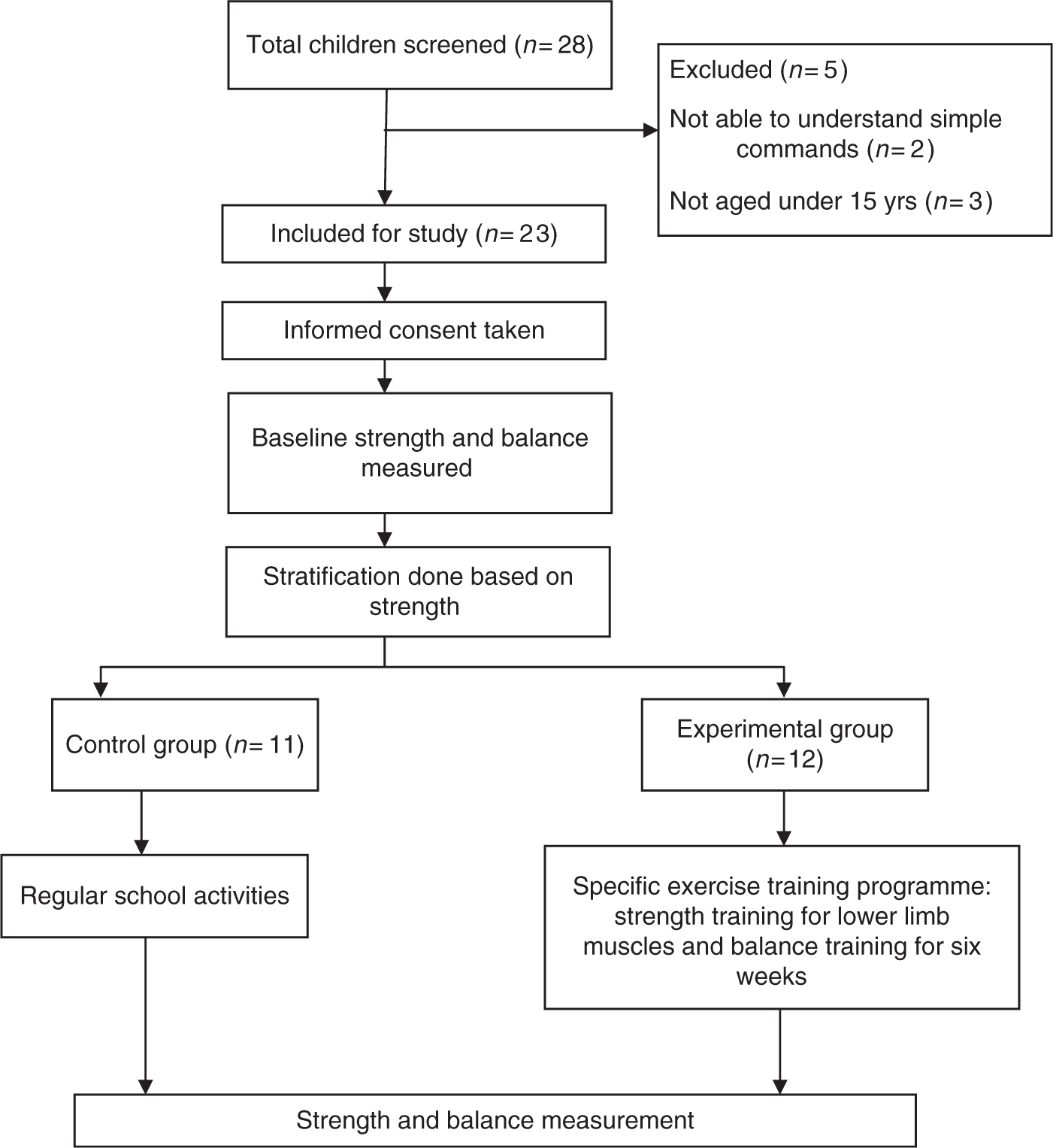
Children (n = 28) with a medical diagnosis of Down’s syndrome were recruited from two schools. The inclusion criteria were: children between the age of 7 to 15 years, ability to understand simple instructions and ability to stand and walk independently. The exclusion criteria were: associated cardiovascular condition and loss of functional vision and hearing. Out of the 28 children, 23 met the study criteria. The study was approved by the ethical committee. Informed consent was taken from all parents/guardians.
The anthropometric details (height and weight) were recorded. Height was measured with the shoes removed using a metal tape measure. Weighing scale was used to measure the weight. The IQ level was determined using the Binet kamat test 18 administered by a clinical psychologist. This test is the Indian adaptation of the 1934 version of the Stanford–Binet Scale test and has been used in Down’s syndrome. 19
Handheld dynamometer (HHD) was used to measure the strength of hip flexors, hip abductors, hip extensors, knee flexors, knee extensors and ankle plantarflexors as per the instruction manual of the instrument. The intra-rater reliability of the instrument was tested prior to collecting baseline data. The reliability ranged between 0.73–0.90 (ICC values). The procedure was explained and demonstrated to the children. Three test trials were performed for each muscle group for both lower limbs. The best performance of the right lower limb was used in the data analysis. The children were allowed a minimum rest period of 30 seconds between the trials. Balance was measured using the balance subscale of the BOTMP, a standardized test which was administered as per the guidelines in the manual.
After collecting the baseline measurements, the children were randomly divided into the experimental and control group using stratified random sampling. Stratification was done based on the average lower limb extension strength (average of hip extensor, knee extensor and ankle plantarflexor strength).This was done to ensure homogeneity in both the groups. Within each strata, random sampling was done using chit method. Experimental or control group was written on a sheet of paper, placed inside an envelope and sealed. The children within each strata were asked to pick a envelope to randomize them into two groups.
Participants in the intervention group underwent a specific exercise training programme which included progressive resistance exercises for the lower limb and exercises for balance training over a period of six weeks, three times a week. Strength training was started at 50% of 1RM. Resistance exercises using sandbags were given for hip flexors, abductors, extensors, knee flexors and extensors and ankle plantarflexors. For each muscle group two sets of 10 repetitions were given, the resistance was increased by half a kilogramme (1.1 lbs) when the child was able to complete the sets with ease and without undue stress. The following activities were selected for balance training: horizontal jumps, vertical jumps, one leg stance with eye open, tandem stance, walking on line, walking on balance beam and jumping on a trampoline. Each activity was given initially for 10 repetitions; it was increased by five repetitions when the child was able to do it with ease.
Instructional procedures were based on demonstration and a total communication approach. Each exercise was demonstrated before its execution to familiarize each subject. Instructions were repeated until the subject knew what was expected. Subjects were positively reinforced during the entire training programme to ensure their maximum effort during each training session. The control group received no special intervention, but continued their activities that were being followed in the school which included classroom studying and play activities. Following the six-week intervention, strength and balance were measured. Strength was measured using the HHD and the balance subset of BOTMP was used to measure balance.
Data analysis was done using the SPSS software version 11.5. Mann–Whitney U test was used to analyze between group variables. Non-parametric tests were used since the sample size was small and the data was skewed. P-values of <0.05 were considered significant.
Results
A total of 28 children were screened, of which 23 met the inclusion criteria and were included in the study. The anthropometric details of the children are described in Table 1. Twelve children were randomly allocated to the experimental group and 11 were in the control group. Figure 1 demonstrates the progress through trial. All the participants in the intervention group completed the exercise protocol successfully.
Flow diagram. Baseline characteristics mean (range).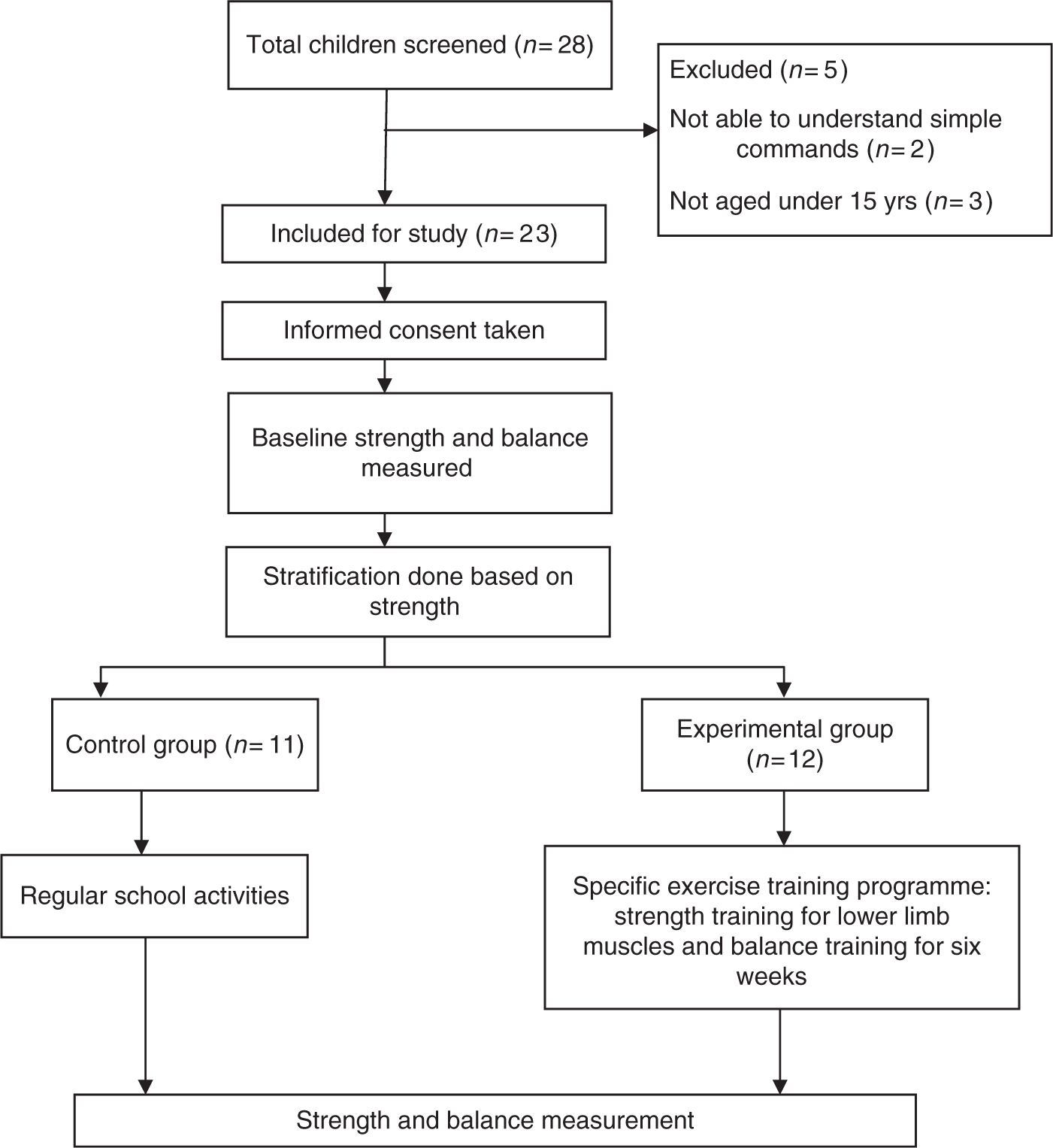
Strength
Pre-post values and change in the strength of lower limb muscles in the experimental and control group
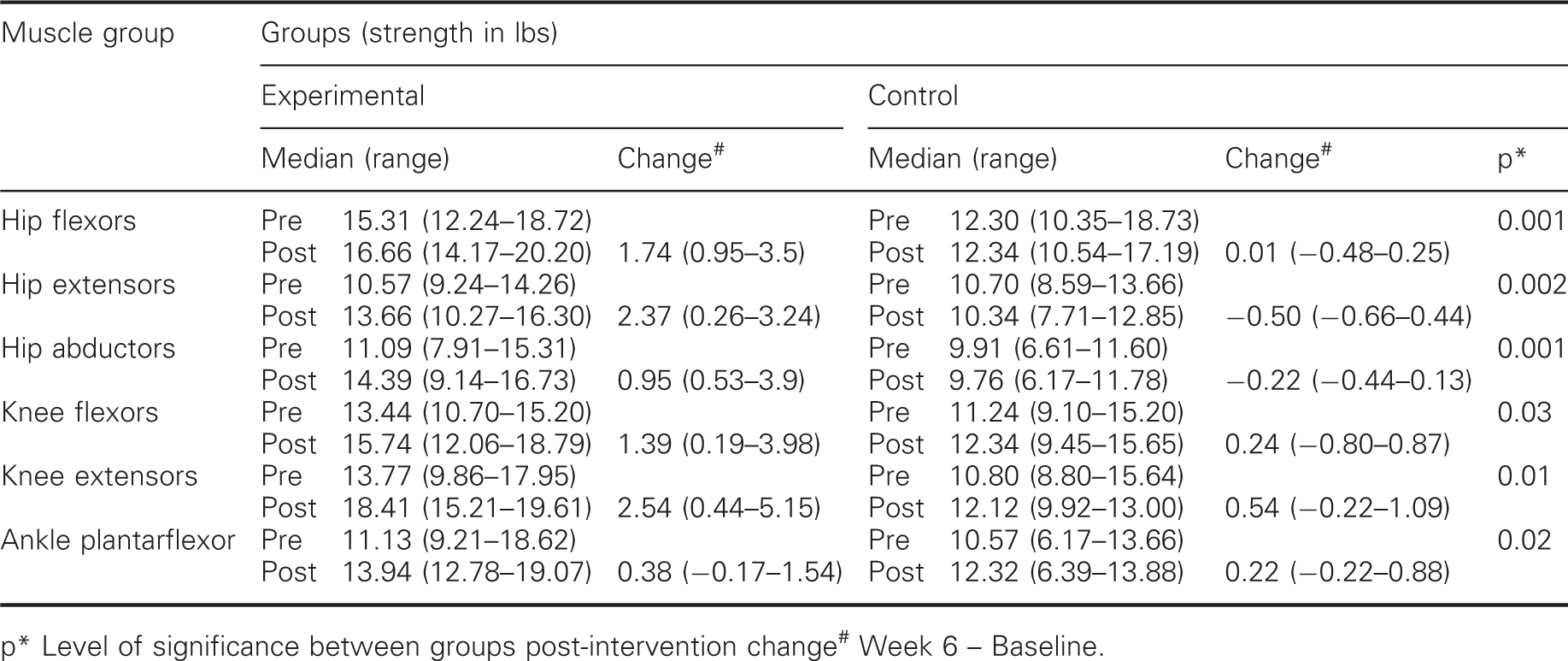
p* Level of significance between groups post-intervention change# Week 6 – Baseline.
Balance
Pre-post values and change in the balance subset of BOTMP in the experimental and control group
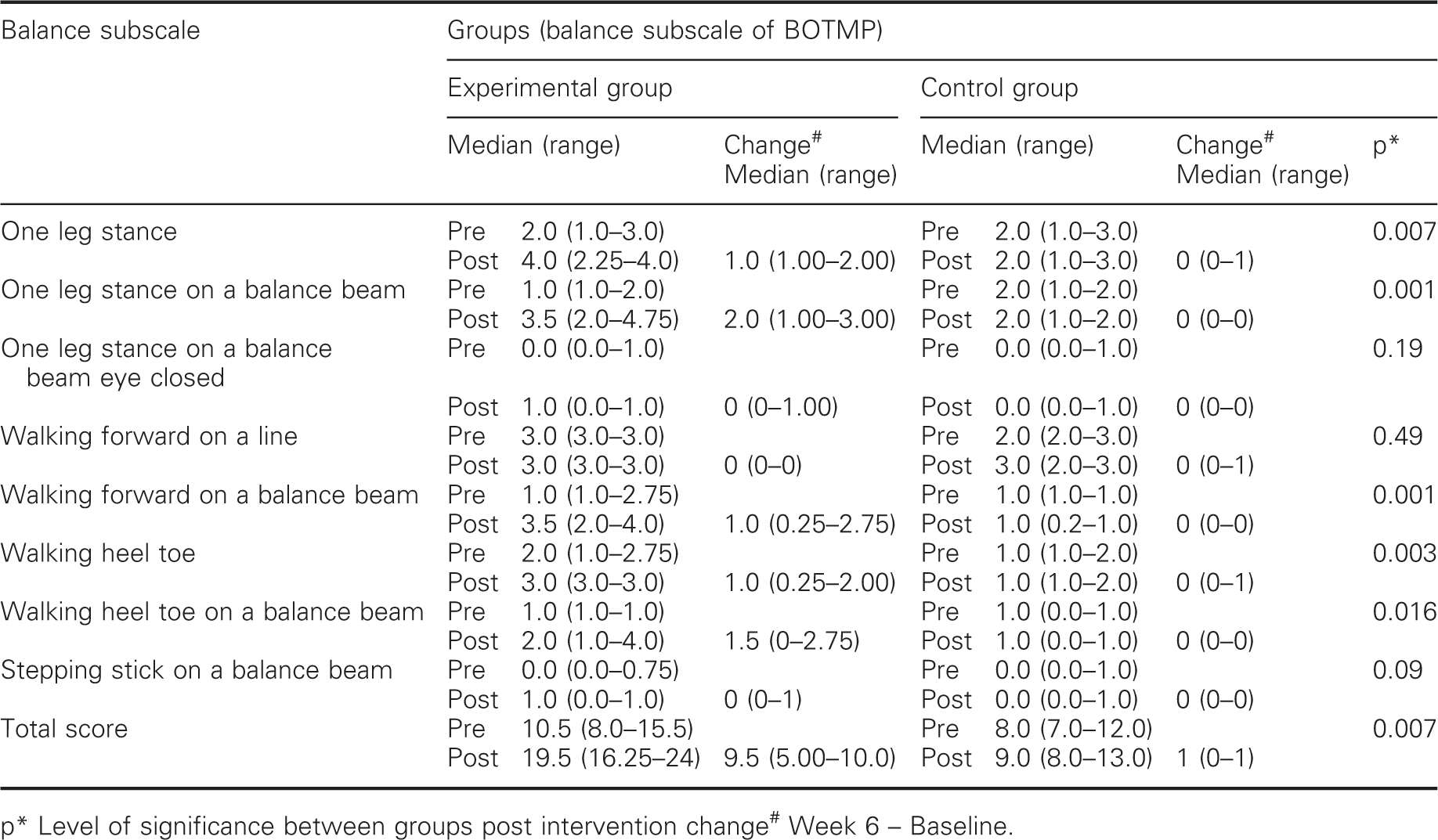
p* Level of significance between groups post intervention change# Week 6 – Baseline.
Discussion
The main finding of this study is that following six weeks of an exercise training programme the children with Down’s syndrome were able to improve the strength of the lower limb muscles and overall balance when compared to the control group. Following the intervention, the strength of all the muscle groups measured improved. This indicates that a six week protocol was sufficient to produce a statistically significant difference. However, clinically the improvement in strength was 1.74 (0.53–3.61) lbs. This low difference can be due to a number of reasons. Firstly, that the strength training was started at 50% of 1RM and progressed gradually. It has been documented that resistance should be started at 70–80% of 1RM to obtain the effects of strength training. 20,21 However, we started at a lower resistance because children with Down’s syndrome have skeletal muscle hypotonia and ligamentous laxity, hence high loads can increase the risk of musculoskeletal injury. 20 Secondly, the training programme was given for six weeks as compared to the 10/12 week programme given in the previous studies. 10,11 Since the programme was shorter, the changes in muscle strength can be attributed to enhanced neural recruitment rather than changes in increased muscle fibre size which requires a minimum of 12 weeks’ training. 22 It has also been documented that prepubescent children do not demonstrate changes in muscle fibre size, and increased strength results from enhanced neural recruitment and timing. 23
Strength training in children with cerebral palsy has been a recent subject of interest among researchers. A number of studies have reported that training benefits these children. Strength training programmes have been documented to improve the lower limb strength, 14 gross motor function scores 14 and gait 16 and that they also have psychological benefits, such as feeling of increased well-being and improved participation in school. 13 Thus, the need is to apply similar strength training protocols in children with other disabilities.
Among children with Down’s syndrome, a case study was done on a 10.5-year-old girl, which included lower limb strengthening in the protocol. This study showed that the subject improved her 10RM significantly following the six week intervention and no adverse effects were reported. More studies on this population are required so that the benefits can be documented and training programmes can be incorporated for all children with Down’s syndrome. The results of our study add evidence to effects of strength training.
The children also benefited from the balance training and the scores on the balance subscale of BOTMP improved from 10.50 to 19.50 in the experimental group which was statistically significant. However, some individual components did not show any difference as compared to the control group post-intervention. Ceiling effect was seen in the component of walking on a straight line. In this component the child is supposed to walk forward six steps on a line to achieve the maximum score of 3. The median score at baseline itself was 3, hence there was no difference seen post-intervention (P = 0.49).
The other component that did not show improvement was standing on a balance beam with eyes closed. This is the only test in the scale that checked balance with vision occluded. None of the exercises in the balance training included activities with eyes closed, this could be the reason why there was no difference in the scores of this component.
The last component was stepping over a response stick on a balance beam. In this component the child is given a score of 0 if they are unable to perform the activity and a score of 1 if they are able to do it. Although, the children in our study found it difficult to perform this task, the score improved from 0.00 (0.00–1.00) to 1.00 (0.00–1.00) in the intervention group. However, it was not statistically significant.
Overall, majority of participants in this trial had a moderate level IQ, yet they were all capable of taking part in the programme and experienced benefits from doing so despite their intellectual disability. Adequate demonstration was given for each exercise. This was done to make sure that the children were able to understand and perform the exercises in the correct manner. Compliance to the intervention was excellent with no drop-outs. Hence we can safely say that the training programme implemented in this study was feasible for children with Down’s syndrome.
One of the limitations of the study was that blinding was not done as the assessor knew which group the patient was in. Also, the control group was not given any intervention; hence no attention was given to them. The improvement in the experimental group could have arisen from attention. Lastly, the sample size was small. Future studies can be done with a larger sample size to enhance the applicability of the results. Also, studies can be done using a more objective measure of balance like force platform and the balance exercises which include components that occlude vision can be added. The long-term effect of such training programmes can be documented by doing follow-up studies. It would also be interesting to see the effect of such interventions on activity levels and physical function.
Clinical messages
Strength and balance improves in children with Down’s syndrome following a six week intervention. Such programmes are feasible.
Footnotes
Acknowledgement
The authors wish to thank the children who participated in the study.