
Abstract
Introduction
Detrusor overactivity is defined by the International Continence Society as a urodynamic observation characterized by spontaneous or provoked detrusor contractions during the filling phase. Idiopathic detrusor overactivity has no known cause. The term ‘idiopathic detrusor overactivity’ has replaced the term ‘detrusor instability’. 1
Idiopathic detrusor overactivity is a syndrome characterized by urinary frequency, urgency and urge incontinence. Urodynamic characteristics of idiopathic detrusor overactivity include reduced maximal cystometric capacity and detrusor contractions that are not inhibited voluntarily. Involuntary detrusor contractions cause urgency or urge incontinence. Nocturia and nocturnal enuresis may also be observed. Symptoms in these patients frequently develop very fast and affect their quality of life considerably. 2
There are various treatment methods for idiopathic detrusor overactivity including conservative approaches, such as bladder training, electrical stimulation and pelvic floor exercises, as well as medical and surgical approaches. 2,3 Medical treatment involves anticholinergic medications. However, anticholinergic medications have several side-effects, such as dry eyes and mouth as well as constipation, which are the most commonly reported side-effects, and headache and nausea. Such side-effects negatively affect patients’ compliance. Surgical treatment has a higher morbidity rate and is used in patients who have not responded to other treatment methods. Conservative methods, such as electrical stimulation, bladder training and pelvic floor exercises are easy to administer and advantageous in terms of avoiding side-effects. 4–6
Previous studies have mostly focused on the effectiveness of pharmacological methods on the treatment of idiopathic detrusor overactivity, 7–9 and the studies involving physiotherapy have investigated conservative methods independently, rather than in combination, and reported their effectiveness on some specific symptoms, such as urge incontinence. 10–13 However, idiopathic detrusor overactivity is a syndrome characterized by more than one symptom. 2 To the best of our knowledge, the literature remains limited regarding the comparison between clinical effectiveness of each treatment option alone or in combination in the treatment of idiopathic detrusor overactivity. 14 On the other hand, it was reported that most patients do not achieve complete symptom relief with therapies alone. It was also reported that there is no sufficient evidence supporting the effectiveness of combination therapies and that randomized controlled studies are needed to investigate the effects of conservative therapies combined with pharmacotherapy on clinic results. 14–16 For these reasons, this randomized trial was carried out to compare the clinical effectiveness of pharmacotherapy and physiotherapy alone, and pharmacotherapy combined with physiotherapy in the treatment of idiopathic detrusor overactivity.
Methods
The study was carried out in 45 female patients with overactive bladder symptoms who admitted to the Department of Obstetrics and Gynaecology and the Department Physiotherapy and Rehabilitation of Hacettepe University between January 2007 and June 2008. The diagnosis of idiopathic detrusor overactivity was made by a physician (the third author) based on detailed history, physical and neurological examination, and urodynamic test. Exclusion criteria were accompanying neurological disorder, neoplasm, second degree or greater pelvic organ prolapse (Baden-Walker), type III stress urinary incontinence, pregnancy, any mental disorder interfering the patient’s cooperation during the treatment, use of a pacemaker or an intrauterine device, or previous medical, surgical treatment or physiotherapy for detrusor overactivity. In addition, contraindications to trospium chloride were reasons for exclusion.
During the study period, the number of patients admitted to the Department of Obstetrics and Gynaecology with overactive bladder symptoms was 97. Sixty-eight of these patients were definitely diagnosed with urodynamic detrusor overactivity. Fifteen patients did not fulfil the criteria and seven patients refused to participate in the study. The remaining patients (n = 46) diagnosed with idiopathic detrusor overactivity were referred to Hacettepe University, Faculty of Health Sciences, Department of Physiotherapy and Rehabilitation. These patients were assessed before the treatment. Then these 46 patients were randomly assigned into 3 groups as pharmacotherapy (n = 15), physiotherapy (n = 15), and pharmacotherapy combined with physiotherapy (n = 16) using a computer-generated block randomization list created by a statistician. Physiotherapy applications were performed by the first author, and assessments were performed by the second author. Only one patient in the pharmacotherapy group did not complete the study because of blurred vision (Figure 1).
Patient flowchart. IDO, idiopathic detrusor overactivity; PT, pharmacotherapy; PR, physiotherapy; PT + PR, pharmacotherapy combined with physiotherapy.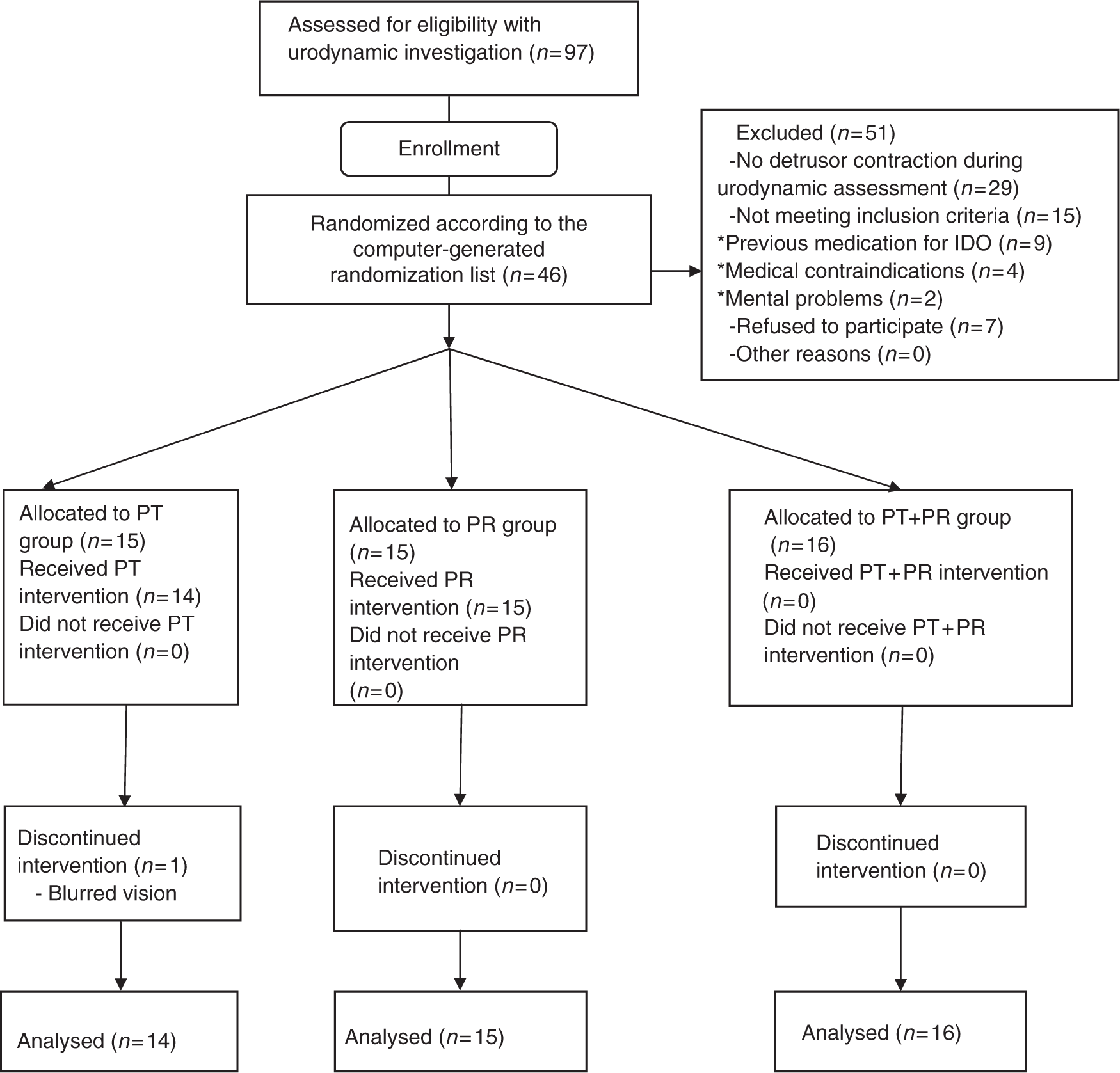
This study was approved by the ethics committee of the Faculty of Medicine, Hacettepe University. A signed informed consent form was obtained from each participant. This study was supported by the Scientific Research Unit, Hacettepe University.
Evaluation
Demographic characteristics of the patients along with their histories were obtained. All participants were evaluated objectively with filling cystometry, surface pelvic floor electromyography, and 1-hour pad test, and subjectively with 24-hour frequency–volume chart and quality of life questionnaire. All evaluations were performed at baseline and at the end of the eighth week.
Filling cystometry, which was administered before the study as part of the diagnosis process, was also administered at the end of the study to detect the maximum cystometric capacity (the bladder volume at which the patient reported that she could no longer delay micturition). Urodynamic stress incontinence was also noted during cystometry. Valsalva and cough-induced stress tests were performed at each 100-mL interval during bladder filling. Cystometry was administered with a multichannel test device (MMS UD 2000 BV Netherlands) at a medium filling rate of 70 mL/min with the patient in semi-supine position. Intravesical and abdominal pressures were measured simultaneously. Abdominal pressure was measured by placing a special catheter in the vagina. Prior to cystometry, all patients demonstrated a negative urine culture. Both cystometry measurements (pre- and post-treatment) were performed by the same researcher (the third author), who was blinded to the treatment protocol.
Electromyographic activity of pelvic floor muscles of all patients was determined in microvolts with an electromyographic biofeedback device (Myomed 932 Enraf Nonius, The Netherlands) using a vaginal surface electromyography probe. The patients lay in the supine position with knees bent, and were instructed to squeeze the vaginal probe without contracting the abdominal, hip, and thigh muscles, and also without holding breath. We did not allow any movement of the pelvis during measurement. 17 Measurements were carried out three times for each patient and the mean of these three measurements were recorded.
In order to evaluate the severity of incontinence, the standard International Continence Society 1-hour pad test was used. 18,19 Patients were instructed to wear a pre-weighed pad and drink 500 mL of plain water during the first 15 minutes. The following 30 minutes included walking and stair climbing. During the last 15 minutes, the patients performed the following provocation activities: standing up from sitting (10 times), coughing vigorously (10 times), running on the spot for 1 minute, bending to pick up a small object from floor (5 times), and washing hands in running water for one minute. At the end of the 1-hour test, pads were removed and weighed. The increase in pad weights were considered as the total weight of urine lost. A sensitive balance (Sartorius, BP 310 S, Germany) was used to measure the pad weights.
The patients completed a 24-hour frequency-volume chart for three non-consecutive days and the mean of the data in these three charts was included in the evaluation. Of these charts, the number of voids/day–night and the number of incontinence episodes/day were included in the evaluation parameters.
The impact of urinary incontinence on the patient’s quality of life was determined with a 22-item quality of life questionnaire developed by Wagner et al. A lower score indicates a better quality of life. 20–22
Finally, all side-effects of trospium chloride were recorded at the last visit.
Treatment protocols
All treatment protocols were in a structured eight-week programme.
Patients in the pharmacotherapy group were given trospium chloride (Spasmex 30 mg) orally 3 times a day (15 mg each dose and totalling 45 mg/day) for eight weeks.
In the physiotherapy group, treatment consisted of interferential current therapy, pelvic floor exercises and bladder training. Interferential current application was conducted 5 days a week for eight weeks, totalling 40 sessions. Treatment was carried out using an electrotherapy device (Elettronica Pagani, IT 20 I Roland Serie, Italy) with vacuum electrodes. Each session was 20 minutes (0–10 Hz for 10 minutes; 0–100 Hz for 10 minutes). Two vacuum electrodes were placed in the suprapubic region and the other two were placed crosswise on the medial side of the ischial tuberosity. 22,23
We opted for interferential therapy because of the ease of use and external application without giving harm to the superficial tissues. Also the use of medium-frequency interferential currents has been suggested as a means of overcoming the problem of stimulating deep-seated structures, such as pelvic floor more effectively, without using invasive methods. 23–25
The patients began the pelvic floor exercises with 5 sets a day with 10 repeats (fast and sustained contractions) and then the number of sets was increased by 5 each week. During the measurement of the electromyographic activity of pelvic floor muscles using electromyographic biofeedback device, the patients were taught how to contract the pelvic floor muscles via audio-visual feedbacks. The patients were provided a diary, in which they were asked to record their exercise sets, by which we planned to encourage them to do the exercises regularly.
In bladder training, the patients were asked to avoid bladder-irritating and diuretic beverages and return to normal fluid intake (50–70 oz (1oz = 30 mL) of liquid), and encouraged to gradually lengthen the period between micturitions. In this training, frequency–volume charts were used. 3,26 Some techniques (selective contraction of pelvic floor muscles during urgency and deep and slow breathing to combat urge feeling, trying to keep mind busy rather than concentrating on bladder) were also taught to the patients to help them in the process of lengthening the period between micturitions as well as to deal with urgency. 12,27
In the combined therapy (pharmacotherapy + physiotherapy) group the patients were administered physiotherapy (electrical stimulation, pelvic floor exercises and bladder training) and at the same time received trospium chloride (the same amount of medicine that the pharmacotherapy group received) for eight weeks.
Statistical analysis
SPSS and NCSS were used for statistical analyses. Data were checked for normality using the Shapiro–Wilk test. Data with a normal distribution were analysed with parametric tests; data with a not normal distribution were analysed with non-parametric tests. To analyse the data from more than two independent groups, one-way ANOVA and Kruskal–Wallis variance analysis were used. Data from two different periods in the same group were analysed with the paired t-test and Wilcoxon signed ranks test. Multiple comparisons after one-way ANOVA and Kruskal–Wallis variance analysis were performed with Tukey HSD test within SPSS and Dunn’s test within NCSS, respectively. Statistical significance level was considered to be 0.05.
Results
Pretreatment evaluation parameters of women, mean (standard deviation)
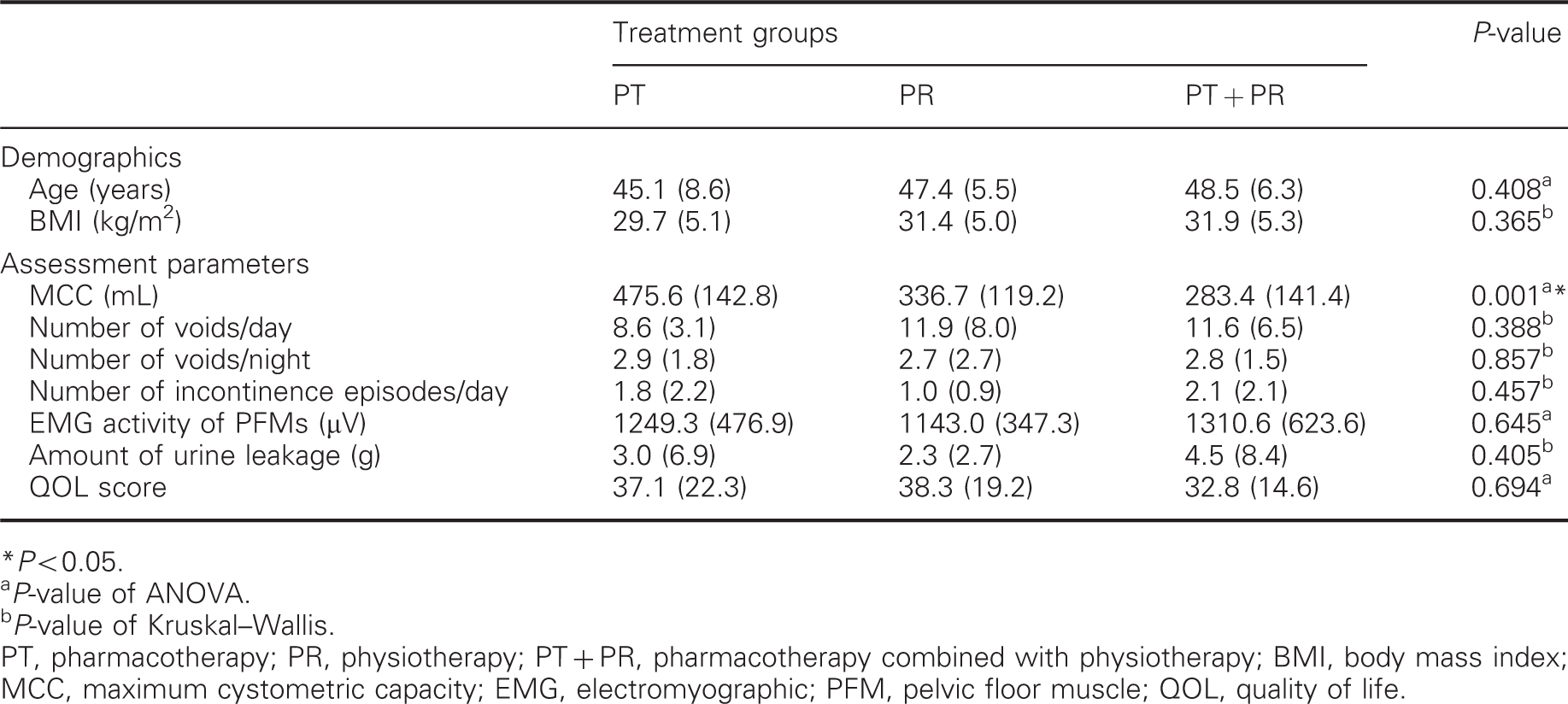
P < 0.05.
P-value of ANOVA.
P-value of Kruskal–Wallis.
PT, pharmacotherapy; PR, physiotherapy; PT + PR, pharmacotherapy combined with physiotherapy; BMI, body mass index; MCC, maximum cystometric capacity; EMG, electromyographic; PFM, pelvic floor muscle; QOL, quality of life.
Comparison of pre and post-treatment parameters in three groups
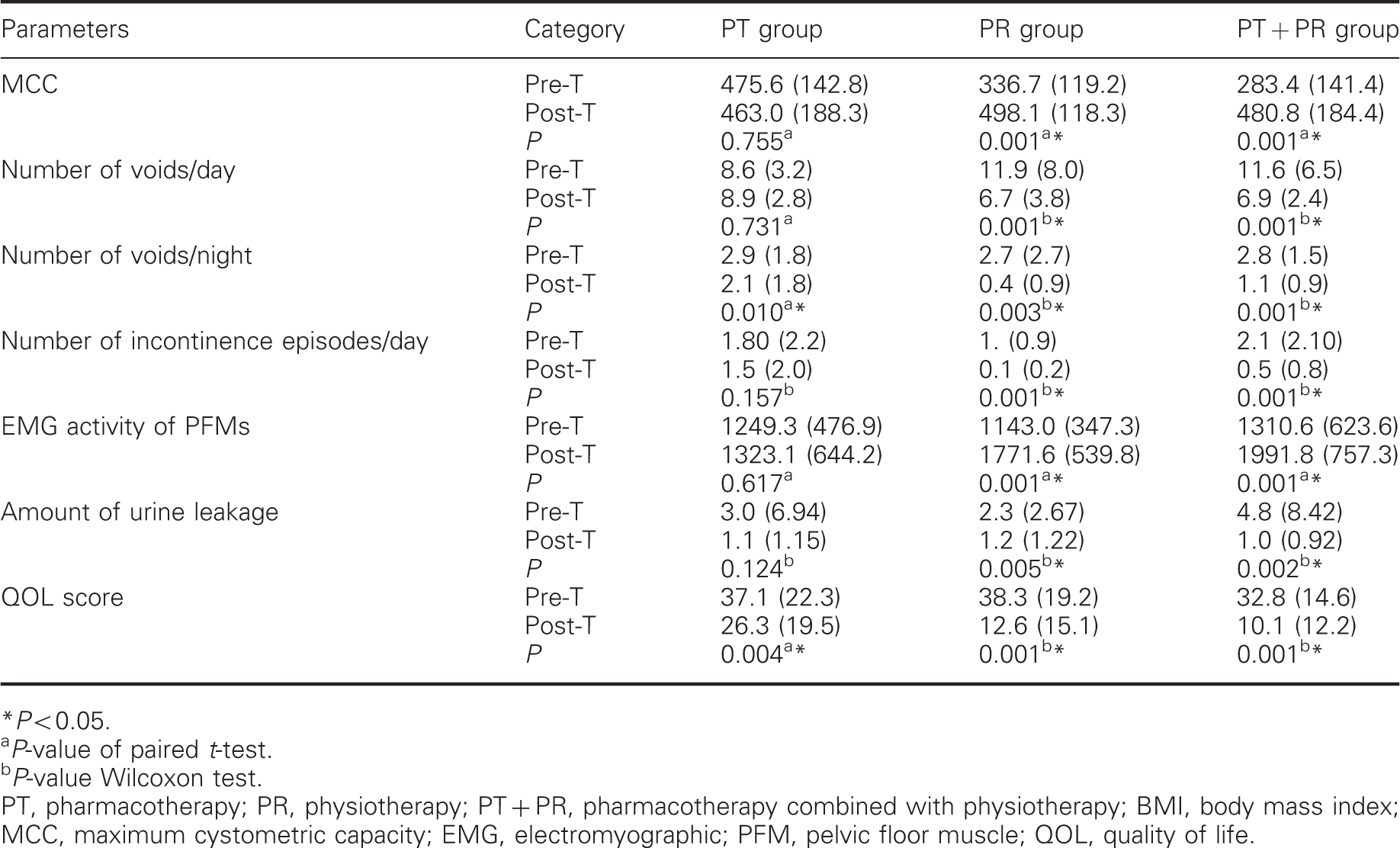
P < 0.05.
P-value of paired t-test.
P-value Wilcoxon test.
PT, pharmacotherapy; PR, physiotherapy; PT + PR, pharmacotherapy combined with physiotherapy; BMI, body mass index; MCC, maximum cystometric capacity; EMG, electromyographic; PFM, pelvic floor muscle; QOL, quality of life.
The number of voids/day, the number of incontinence episodes/day, and the amount of urine leakage declined significantly in both physiotherapy and combined treatment groups (P < 0.05), while there was no statistically significant difference in the pharmacotherapy group (P > 0.05) (Table 2).
The number of voids/night and the quality of life scores improved significantly (P < 0.05) in all groups (Table 2).
Comparison of differences between pre and post-treatment parameter values in the three groups
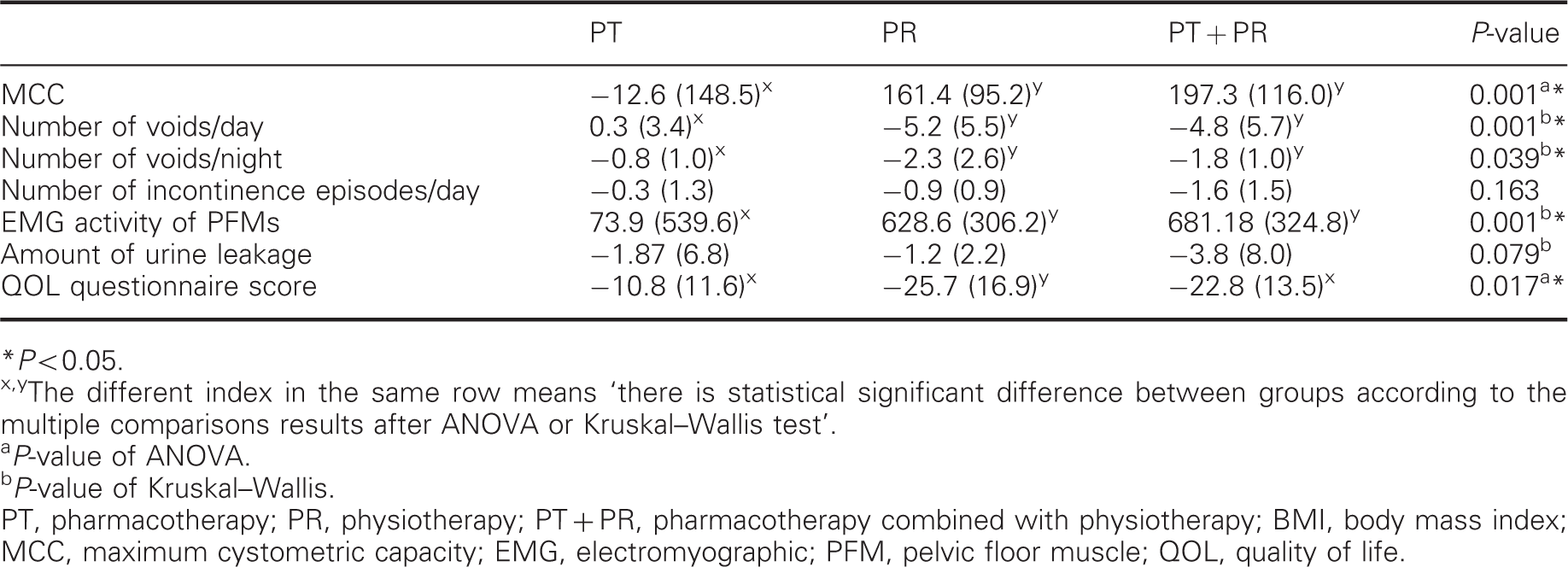
P < 0.05.
The different index in the same row means ‘there is statistical significant difference between groups according to the multiple comparisons results after ANOVA or Kruskal–Wallis test’.
P-value of ANOVA.
P-value of Kruskal–Wallis.
PT, pharmacotherapy; PR, physiotherapy; PT + PR, pharmacotherapy combined with physiotherapy; BMI, body mass index; MCC, maximum cystometric capacity; EMG, electromyographic; PFM, pelvic floor muscle; QOL, quality of life.
According to the results of multiple comparisons, there was a significant difference between the pharmacotherapy group and the other groups (P < 0.05) in terms of change in the maximum cystometric capacity, but there was no statistically significant difference between the physiotherapy and combined treatment groups (P > 0.05) (Table 3). This means that the maximum cystometric capacity showed similar improvement in physiotherapy and combined therapy groups.
In terms of changes in the number of voids/day and night and electromyographic activity of pelvic floor muscles, there was a significant difference between the pharmacotherapy group and the other groups (z > 1.96) while there was no statistically significant difference between the physiotherapy group and combined therapy group (z < 1.96). The number of voids/night showed less improvement in the pharmacotherapy group compared to the other groups. The number of voids/day–night and electromyographic activity of pelvic floor showed similar improvement in both physiotherapy and combined treatment groups.
In terms of the improvement in the quality of life scores, there was a statistically significant difference between the physiotherapy group and the other groups (P < 0.05); however, no significant difference was observed between the pharmacotherapy and combined therapy groups (P > 0.05) (Table 3). As a result, the quality of life score showed the best improvement in the physiotherapy group (P < 0.05) and a similar improvement in both pharmacotherapy and combined therapy groups were observed.
During cystometry, urodynamic stress incontinence was diagnosed in 7 patients (n = 2 in the pharmacotherapy group, n = 3 in the physiotherapy group and n = 2 in the combined therapy group), but none of these patients had type III stress urinary incontinence.
In the present study, dry mouth was the most reported side-effect (7/31, 22.58%) in the pharmacotherapy and combined therapy groups, but none of the participants dropped out because of it. Just 1 patient in the pharmacotherapy group withdrew from the study because of visual impairment. There were no other reported side-effects.
Discussion
In the present study the effects of a pharmacological agent (trospium chloride) and a physiotherapy protocol (alone and in combination) on idiopathic detrusor overactivity were investigated and compared in terms of several parameters (maximum cystometric capacity, electromyographic activity of pelvic floor muscles, voiding diary parameters, the amount of urine leakage and the quality of life score). At the end of the study, it was observed that the some study groups showed similar results in terms of some parameters and differences were observed between groups in some other parameters.
In the patient groups that received physiotherapy alone and combined therapy of trospium chloride and physiotherapy, there were significant improvements in both subjective evaluations (the number of voids/day–night and the quality of life score) and objective evaluations (the maximum cystometric capacity, electromyographic activity of pelvic floor muscles and the amount of urine leakage). Moreover, in the patient group that received just pharmacotherapy, there were significant improvements in some of the subjective evaluations (the number of voids/night and the quality of life score).
This study has some limitations. One of the limitations of the present study is the small sample size. However, in the study period, only a proportion of the patients admitted to the Department of Obstetrics and Gynaecology with overactive bladder symptoms were definitely diagnosed with urodynamic detrusor overactivity. Furthermore, the exclusion criteria, especially the one regarding the patient’s previous detrusor overactivity treatment, and some patients’ inability to attend to a two-month-long physiotherapy programme further reduced the sample size. Another limitation is the lack of long-term follow-up.
Strengths of the present study include presenting many disease-specific assessment parameters, low drop-out rate (n = 1), and the utilization of a randomized design. Moreover, a new physiotherapy protocol was performed by combining three different conservative approaches.
The main goal of treatment in overactive bladder is to inhibit detrusor overactivity and thereby to increase the functional bladder capacity. 13 Placebo-controlled studies in the literature investigating the effectiveness of trospium chloride on idiopathic detrusor overactivity reported a significant increase in the maximum cystometric capacity compared to placebo. 7,28 Several studies reported a significant improvement in the cystometric capacity of the patients with detrusor instability after only bladder training or only pelvic floor electrostimulation. 10,29,30 The number of studies comparing the effect of trospium chloride and physiotherapy is limited. 14 Ozdedeli and colleagues’ randomized controlled study reported a similar improvement in the maximum cystometric capacity with intravaginal electrical stimulation and trospium hydrochloride. 31
Unlike previous studies reporting positive effects of trospium chloride on bladder capacity, the trospium group in our study did not experience a significant improvement in bladder capacity. This finding may be attributed to the statistically significant higher level of maximum cystometric capacity values of the pharmacotherapy group (compared to the other two groups); however, an increase in bladder capacity due to the detrusor inhibitive behaviour of trospium chloride was expected (because these patients had been suffering overactive bladder symptoms and all of them were diagnosed with urodynamic detrusor overactivity). Therefore, we were not able to conclusively determine the effect of trospium chloride on bladder capacity. Further studies investigating the effect of trospium chloride on the pre-medication bladder capacity may be needed. On the other hand, the maximum cystometric capacity significantly increased in both physiotherapy and combined therapy groups, which shows that the physiotherapy protocol has a positive effect on the maximum cystometric capacity. Physiotherapy and combined therapy were able to lengthen the periods between micturitions and increased the volume of urine the patients pass each time via some mechanisms that result in a decrease in detrusor pressure and an increase in urethral pressure, 32 and thus their maximum cystometric capacity values showed an increase in urodynamics.
The voiding diary is a reliable and valid tool to assess the symptoms of overactive bladder. 33 In our study, the number of voids/day–night and the number of incontinence episodes/day were included in the evaluation parameters from diaries. Previous studies showed a reduction in the number of voids/day and night, and in the daily number of incontinence episodes using a wide range of physiotherapy applications applied for various lengths of time. 10,34–36 Zinner et al. investigated the effects of trospium chloride on voiding parameters in patients with overactive bladder syndrome and reported a statistically significant decrease in the number of voids/day–night and the number of incontinence episodes/day. 37 In the present study, the number of voids/night improved in all groups, but this improvement was less in the pharmacotherapy group compared with the other groups. This finding showed that all three treatment approaches are effective on nocturia, and physiotherapy alone may be effective in patients with symptoms of nocturia who were contraindicated for anticholinergic agents. The number of voids/day and the number of incontinence episodes/day improved significantly in the physiotherapy and combined therapy groups but not in the trospium group. This might be explained by the absence of improvement in the maximum cystometric capacity and electromyographic activity of the pelvic floor muscles in the pharmacotherapy group.
Electromyography can be used to measure the electrical activity of skeletal muscles and is a direct representation of the outflow of motoneurons in the ventral horn of the spinal cord to the muscles as a result of either voluntary or reflex pelvic floor muscle contraction. In clinical practice, surface electrodes on a vaginal probe are most commonly used due to the high sensitivity of the perineal region and the skills required for using wire or needle electrodes. One difficulty with surface electromyography is to ensure accuracy, that is, to measure the activity of only the muscle/muscles desired without interference from other muscles – so-called cross-talk. In the present study, validity was established by giving instructions to the patients and by keeping the pelvis steady during the evaluation. 17,38 The technique used in this study does not measure the strength directly, but only depicts it indirectly by measuring electromyographic activity during a muscle contraction. 39
Studies in the literature have reported the positive effect of electrical stimulation and pelvic floor exercises on pelvic floor muscle strength. 22,23 Although no study has investigated the effect of bladder training on pelvic floor muscle strength in particular, Theofrastous et al. reported that, among patients with urinary incontinence, the patient group that received pelvic floor exercises showed greater increase in pelvic floor muscle strength than the patient group that received bladder training. 40 Padda et al. reported that atropine, an anticholinergic agent, did not have an effect on vaginal and anal pressure. 41 In the present study, with regard to the electromyographic activity of pelvic floor muscles, there was a significant increase in the physiotherapy and combined therapy groups while there was no significant change in the pharmacotherapy group. This finding suggests that trospium chloride has no significant effect on the electromyographic activity of the pelvic floor muscles.
Prajsner et al. reported that 1-hour pad test is an effective evaluation method, especially in stress incontinence, and that it is less effective in patients with genuine urge continence. 42 However, several studies in the literature use the pad test to investigate the effects of different treatment approaches, such as interferential low-frequency therapy, dorsal genital nerve stimulation and intradetrusor injection with botulinum toxin A, on overactive bladder. 43–45 Also in this study, seven patients had a diagnosis of urodynamic stress incontinence as well as detrusor overactivity. Therefore, the use of pad test in this study in the assessment of clinical effectiveness of the therapies was meaningful.
Jonassan et al. applied maximal electrical stimulation 20 minutes/day for 12 weeks to a group of patients with detrusor instability and reported a significant decrease in the pad test results. 46 In the present study, we observed a significant improvement in pad test results in both physiotherapy and combined therapy groups, while there was no significant difference in the pharmacotherapy group. We think that this finding is due to the increased electromyographic activity of the pelvic floor muscles in both physiotherapy and combined therapy groups. With increasing pelvic floor muscle activity the amount of urine loss decreased. Trospium alone produced no statistically significant change in the amount of urine leakage.
Overactive bladder syndrome can have a significant negative impact on quality of life, impairing several areas, including emotional well-being, productivity at home and at work, social relationships, sexual intimacy and physical functioning. 47 Some studies in the literature have investigated the effectiveness of treatment protocols in urinary incontinence using the quality of life questionnaire developed by Wagner et al. 21,23 In the present study, the quality of life scores revealed an improvement in all groups. Pharmacotherapy and combined therapy groups showed a similar improvement, but the physiotherapy group showed a better improvement compared to the other groups. Further studies are needed to provide an explanation for this outcome.
Anticholinergic drugs have several side-effects, negatively affecting the patients’ compliance. 4 Studies that compared the effects of trospium chloride and other pharmacological agents in detrusor instability reported that trospium chloride was better in terms of central nervous system effects, side-effect profile and tolerability. 8,48 Although in the present study the side-effect profile of trospium chloride was not investigated directly, it looks relatively good based on the results. Only one patient withdrew from the study.
The physiotherapy intervention of this study is relatively rigorous. It would be clinically important to conduct new trials to determine whether similar results are achievable with a less rigorous intervention (e.g. with fewer clinical intervention sessions per week).
The three most commonly employed methods for treating newly diagnosed overactive bladder syndrome are bladder training, anticholinergic therapy and a combination of the two. 49 Song et al. reported that tolterodine alone may be instituted as a first-line therapy, but may be more effective when combined with bladder training in overactive bladder syndrome. 49 So, the inclusion of another group involving trospium chloride combined with bladder training to the present design would have been useful. If this approach is found more effective than others, this will be quite meaningful, because this approach demands little effort and requires less clinician time compared with clinical electrostimulation and pelvic floor training.
It has been reported that patients with overactive bladder syndrome do not achieve complete symptom relief with individual therapies and there are a limited number of studies in the literature reporting that combined therapies are better than individual treatments. 14,15 In the present study, we applied three conservative approaches (electrical stimulation, bladder training and pelvic floor exercises) in the physiotherapy group, and in the combined therapy group we included a pharmacological agent in the physiotherapy protocol. In the present study, although the pharmacotherapy group showed improvements in some variables, physiotherapy and combined therapy groups showed better improvements compared to the pharmacotherapy group, which means that combined treatments are more effective than pharmacotherapy alone.
In conclusion, the physiotherapy protocol (combination of electrical stimulation, pelvic floor training and bladder training) alone or in combination with trospium chloride was more effective than trospium chloride alone in the management of idiopathic detrusor overactivity. However, further studies with a larger population group and following up the patients for a longer period of time are warranted to find out if these effects are long-lasting or not.
Clinical message
Physiotherapy protocol (including electrical stimulation, bladder training, and pelvic floor training) or the combination of this physiotherapy protocol with trospium chloride is more effective than trospium chloride alone in the treatment of female patients with idiopathic detrusor overactivity.
Footnotes
Acknowledgements
We thank Hacettepe University, Scientific Research Unit for material support and Mr E Coşgun from Hacettepe University, Department of Biostatistics for his help with statistical analyses.
Author contribution
The study was carried out in collaboration between all authors. SK, TA and SB participated in the concept and design of the study. All authors were involved in the process of collecting the data and interpreted the results. SK and TA performed the statistical analyses in consultation with a statistician and drafted the manuscript. All authors read and approved the final manuscript.
Competing interest
None.
Funding
Hacettepe University, Scientific Researches Unit provided the material support (urodynamic catheters) for the present study. The authors did not receive payments or other benefits or a commitment or agreement to provide such benefits from a commercial entity. There is no conflict of interest.