
Abstract
Introduction
Hemiplegic patients after stroke continue to suffer from abnormal gait and limitations to walking caused by several factors, including muscle weakness, impairment of weight bearing or balance, learned non-use, spasticity, exaggerated deep tendon reflex and co-contraction of synergic pattern muscles. 1 Most hemiplegic patients can walk independently with or without assistive devices, but several problematic factors, as mentioned above, may prevent them from achieving full functionality. Therefore, many treatment methods for the reduction of problematic factors and the improvement of balance and gait ability have been studied and developed.
There have been many conventional treatments, such as neurodevelopment treatment and sensory stimulation, designed to make patients shift their weight to the affected side. 2,3 Functional walking training methods, such as weight unloading devices and robots as well as balance training systems such as the Balance Master System and Balance Retrainer have also been used to achieve this goal. 4 – 9 Weight-bearing exercise has been regarded as essential in stroke rehabilitation, because it facilitates the contraction of antigravity muscles in the lower extremities and can help stroke patients regain balance and gait ability. 10 – 15 Constrained induced movement therapy (CIMT) has recently garnered attention in the field of stroke rehabilitation because of its ability to reduce learned non-use and improve patients’ functional state. 16 – 20
Our team therefore focused on a sliding rehabilitation machine, which has the advantage of providing both weight-bearing exercise and forced use by repetitive flexion and extension of the lower extremities. The inclination of the sliding rehabilitation machine can be controlled to adjust the burden of exercise to suit mild to severe hemiplegic stroke patients and to improve their function – especially balance and gait ability.
The aim of this study was to examine the effectiveness of the sliding rehabilitation machine in improving balance and gait ability in chronic stroke patients.
Methods
Thirty patients were recruited between June 2009 and October 2009. The patients were admitted to the hospital with a stroke and were chronic stroke patients who were over six months from the onset of disease. Only those patients who had a medium and high falling risk as determined by the Berg Balance Scale (less than 40 out of 56 points) were included in this study. Patients with severely impaired cognitive function (Mini-Mental State Examination <24), severe visual or perceptual impairment, previous musculoskeletal abnormality or damage to the lower limbs, another medical disease that could get in the way of exercise, or severe heart disease such as myocardial infarction or arrhythmia were excluded from the study. The protocol was approved by the Institutional Review Board and informed consent was obtained prior to training. As shown in Figure 1, no patients dropped out in this protocol.
Flow diagram of this study.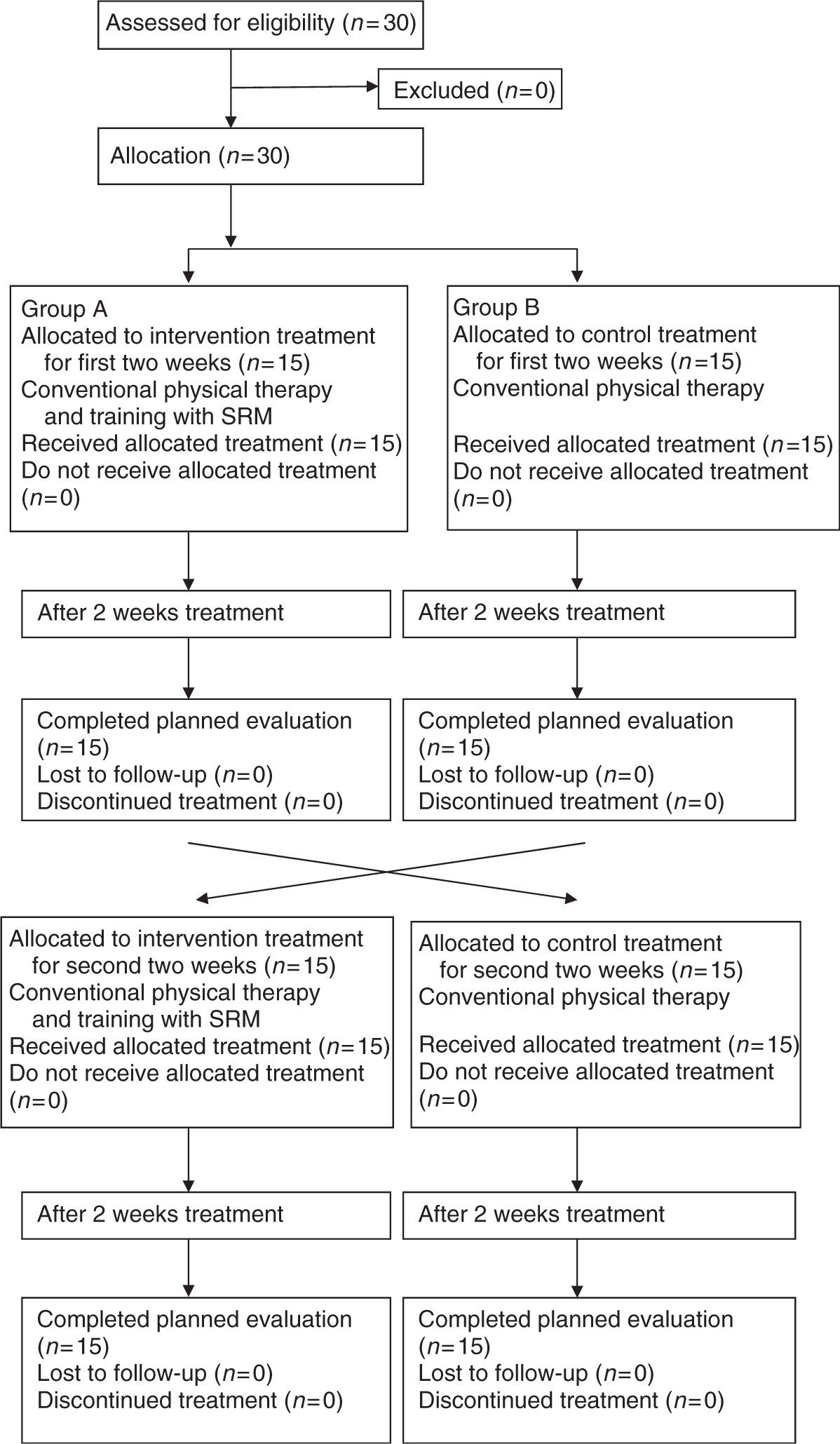
We used a sliding rehabilitation machine. This has a rail system, a patient-supporting carriage, a footplate which is moved up and down, and a leg elevation device that is connected to the patient support carriage. The footplate can be moved up and down to change the maximal angle of knee flexion. If the non-hemiplegic leg is placed on the leg elevation device connected to the patient support carriage, forced use of the hemiplegic leg is easily achieved. The goniometer shows the degree of inclination of the sliding board, and there are Velcro straps to fix the patient’s body and ankles for their safety. It is possible to change the locations of the footplates to determine the degree of knee flexion. Before and even during the 30-minute training with the sliding rehabilitation machine, we frequently changed the maximum inclination at which patients could exercise with knee flexion and extension. Therefore, we were able to gather quantitative data such as maximum inclination and maximum number of repetitions at a given inclination. In cases where the patient could not exercise the affected lower extremity individually, they were allowed to exercise both lower extremities together.
The 30 patients were divided into two groups according to the results of dice thrown by the researcher. Patients with odd numbers were assigned to group A and the others to group B. They underwent four weeks of training with different protocols. One group (group A, n = 15) underwent training with the sliding rehabilitation machine for 30 minutes per day, 5 times per week, for two weeks with concurrent conventional training based on the Bobath concept for 40 minutes per day, and subsequently underwent only the conventional training for another two weeks. The other group (group B, n = 15) underwent the same types of training in reverse order, each for two weeks. The effect of the experimental period was defined as the sum of changes during the two-week sliding rehabilitation machine training in each group (groups A and B), and the effect of the control period was defined as the sum of those during the two-week training without the sliding rehabilitation machine in each group.
All training sessions were conducted by experienced physiotherapists with certification from the Korean Society of Physical Therapy. All patients finished the four-week intervention without significant side-effects.
All 30 patients underwent objective assessment before training, and at two and four weeks of training. The Functional Ambulatory Category, 21 the Six-Minute Walk Test, 22 the Timed Up and Go Test, 23 the Berg Balance Scale 24,25 and the Korean-Modified Barthel Index 26 were used as clinical tools to measure the level of function. The Modified Ashworth Scale and a Manual Muscle Test were used to measure the spasticity and strength of knee extension, respectively. The reliability and validity of these clinical tests are well established.
Because some patients could not walk independently, external support was given when administering the Six-Minute Walk Test and the Timed Up and Go Test. The outcome assessor was not blinded.
SPSS Version 12.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. The Wilcoxon rank sum, chi-square and Fisher’s exact tests were used to compare the two groups (A and B groups) before training. A signed-rank test was used to compare the training effects between pre and post treatment in the two periods and in the experimental and control periods individually. Results were considered to be statistically significant if the P-value was less than 0.01.
Results
General characteristics of patients
General characteristics of subjects
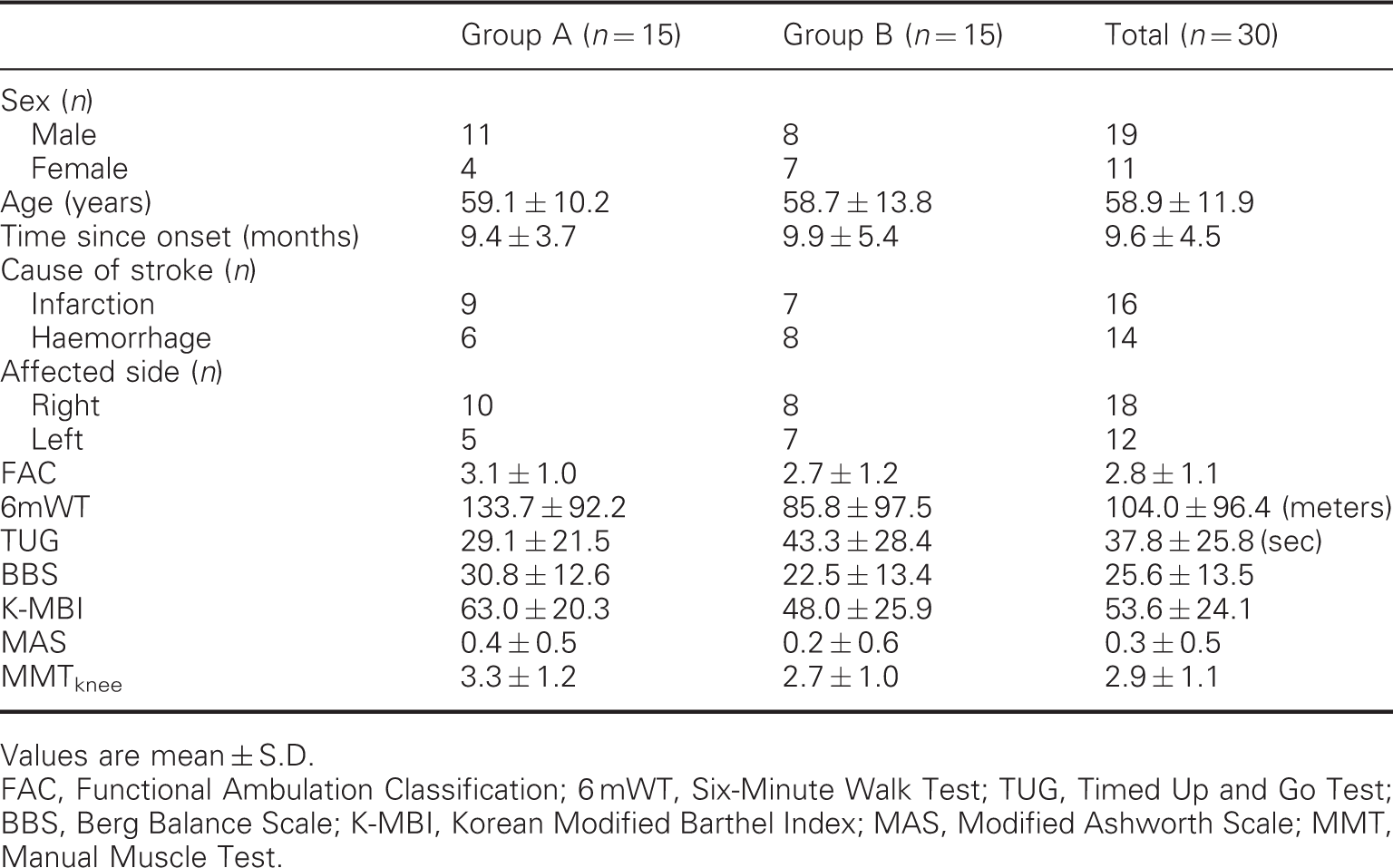
Values are mean ± S.D.
FAC, Functional Ambulation Classification; 6 mWT, Six-Minute Walk Test; TUG, Timed Up and Go Test; BBS, Berg Balance Scale; K-MBI, Korean Modified Barthel Index; MAS, Modified Ashworth Scale; MMT, Manual Muscle Test.
Training effects
Summary of treatment effects in group A and B
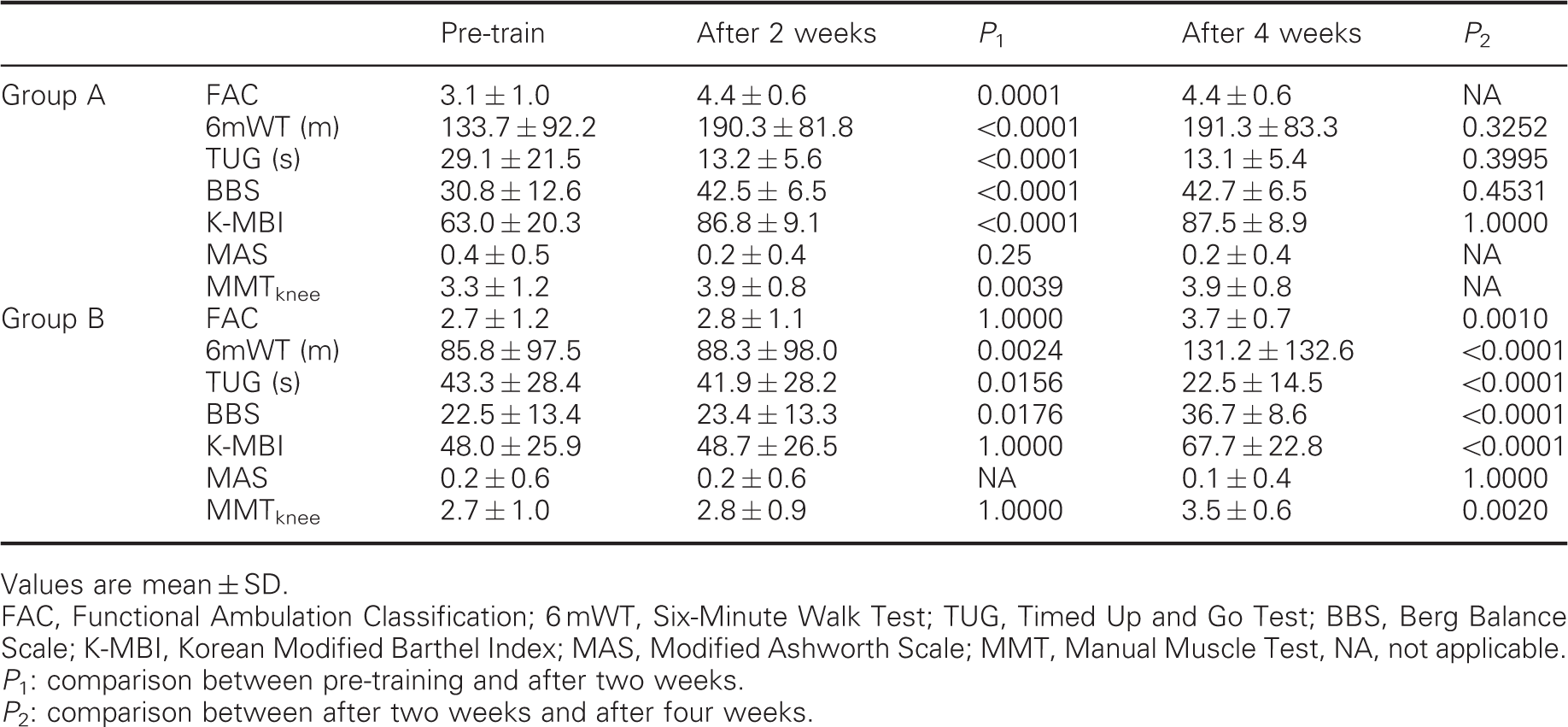
Values are mean ± SD.
FAC, Functional Ambulation Classification; 6 mWT, Six-Minute Walk Test; TUG, Timed Up and Go Test; BBS, Berg Balance Scale; K-MBI, Korean Modified Barthel Index; MAS, Modified Ashworth Scale; MMT, Manual Muscle Test, NA, not applicable.
P 1: comparison between pre-training and after two weeks.
P 2: comparison between after two weeks and after four weeks.
Comparison of changes in measurement values of clinical parameters between experimental and control periods during the training period
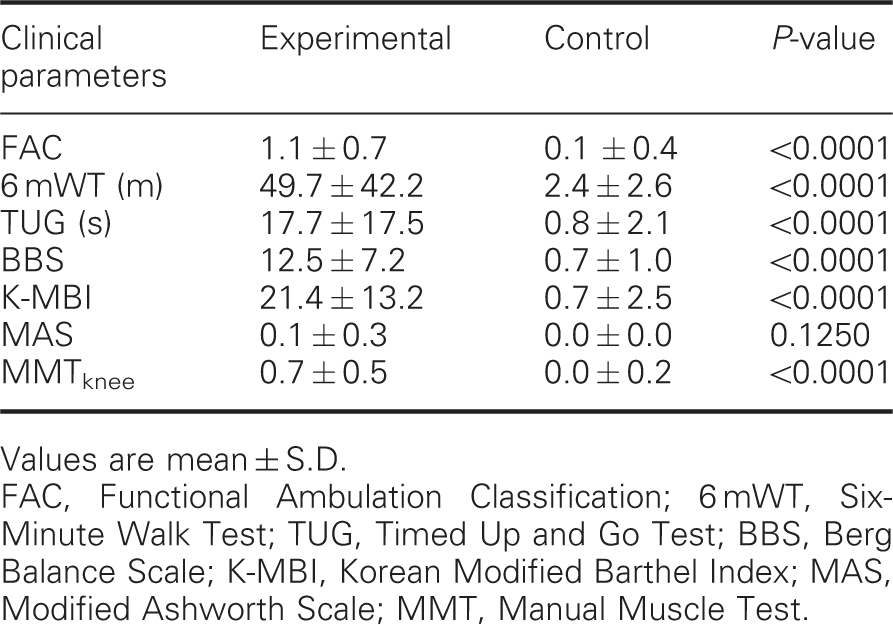
Values are mean ± S.D.
FAC, Functional Ambulation Classification; 6 mWT, Six-Minute Walk Test; TUG, Timed Up and Go Test; BBS, Berg Balance Scale; K-MBI, Korean Modified Barthel Index; MAS, Modified Ashworth Scale; MMT, Manual Muscle Test.
Discussion
Restoration of independent walking ability should be the primary goal of therapeutic efforts in rehabilitation of patients with stroke because disability on walking may reduce their ability to perform everyday activities and may exacerbate other stroke-related disabilities. 27,28 As mentioned earlier, poor prognostic factors such as muscle weakness, impairments of weight bearing or balance, learned non-use, spasticity, exaggerated deep tendon reflex and co-contraction of synergic pattern muscles could prevent stroke patients from recovering their functions. 1 Rehabilitation teams should focus on reducing these factors.
Because of this, our team developed the sliding rehabilitation machine which has the advantage of providing both weight-bearing exercise (one of the strengthening exercises) and forced use by repetitive flexion and extension of the lower extremities. Treatments using strengthening exercises and constraint-induced movement therapy in motor recovery of stroke patients are accepted in the rehabilitation field. In fact, the modified tilt table, which has a railing system and patient supporting carriage, was introduced to provide weight-bearing exercise to severe burn patients, but has not been used for stroke patients. 29 The modified tilt table is similar to the sliding rehabilitation machine, but unlike the modified tilt table, the sliding rehabilitation machine has a footplate which can be moved up and down, and a leg elevation device which is connected to the patient support carriage. The leg elevation device makes forced use of the hemiplegic lower extremity easy and the movable footplate makes control of maximal knee flexion easy.
We tried, therefore, to examine the effectiveness of the sliding rehabilitation machine in improving balance and gait ability in chronic stroke patients.
It is well known that muscle power is the most essential component of walking and mobility after stroke, and strengthening exercises should be a fundamental component of rehabilitation treatment. Ada et al. 30 reported that strengthening interventions increase strength, improve activity, do not increase spasticity and should be part of rehabilitation after stroke. Langhome et al. 31 reported that although the existing evidence is limited by poor trial designs, some treatments do show promise for improving motor recovery, particularly those that focus on high-intensity and repetitive task-specific practice.
It is also known that closed kinetic chain exercise is more effective than open kinetic chain exercise because closed kinetic chain exercise is more closely related to activities of daily life. 6,7,9,32,33 Sometimes we use the Noland-Kuckhoff table and the Cybex Dynamometer (Cybex Inc, USA) for strengthening exercise, but there are some limitations to these machines. They cannot be used in patients with poor muscle power or poor motivation and do not achieve the effects of closed kinetic chain exercise. The sliding rehabilitation machine, on the other hand, does not face these limitations and can be adapted to most stroke patients.
Although there are some limitations of scope and some debate, constraint-induced movement therapy seems to be a very effective rehabilitation treatment for the upper extremity of hemiplegic stroke patients by forced usage of the affected side to manage learned non-use. 16 – 18,20 Lin et al. 20 showed that enhanced performance of the upper extremity was found in those treated with constraint-induced movement therapy and Taub et al. 18 found that stroke patients showed large improvements in the functional use of their affected arm in their daily lives and that the changes persisted over two years after constraint-induced movement therapy. However, studies on the use of constraint-induced movement therapy for the lower extremities of patients with severe motor or balance problems are rare. 19 The sliding rehabilitation machine works by a similar principle, making patients use their lower extremity in accordance with their muscle power by changing inclinations.
Our results during treatment with sliding rehabilitation machine support and confirm the findings of previous studies that rehabilitation with repetitive and task-oriented treatment is beneficial to motor recovery in hemiplegic patients with stroke. 9,16 – 20,30 – 32 There were statistically significant improvements in all clinical parameters in the experimental period after two weeks of training with sliding rehabilitation machine in each group (groups A and B) when compared with the parameters before training (Table 2). Changes in measurement values of clinical parameters during the training period (sum of two weeks of training with sliding rehabilitation machine in each group) were statistically significantly improved in the experimental period when compared with the control period (sum of two weeks of training without sliding rehabilitation machine in each) (Table 2). There are even some improvements in the control period, although, with the exception of Six-Minute Walk Test, these are not statistically significant. This suggests that additional treatment with the sliding rehabilitation machine may be helpful to regain balance and gait ability.
This study has some limitations. First, a small number of patients and only patients in the hospital were recruited, so these data may not represent stroke patients as a whole. Second, because we thought that there was little interaction between the two treatments and because patients are usually allowed to get rehabilitation treatment for only four weeks in the hospital, we did not give our patients a resting period between the two different treatment sessions, which is considered essential in a crossover study of drugs. Third, we did not evaluate the long-term effectiveness of the treatment, and, thus, there should be ongoing follow-up beyond the completion of the treatment. Fourth, this study was done by non-randomized crossover design. Fifth, the assessor was not blinded.
Nevertheless, the patients were at the chronic stage at which spontaneous recovery is minimal and objective tests were used, so we think the findings of this study are meaningful.
Clinical messages
Weight-bearing exercise and forced used of hemiplegic lower extremity is possible with a sliding rehabilitation machine. The additional use of the sliding rehabilitation machine may be a useful tool for the improvement of balance and gait abilities in chronic stroke patients.
Footnotes
Acknowledgements
This study was supported by a grant of the Korea Healthcare technology R&D Project, Ministry for Health, Welfare and Family Affairs, Republic of Korea (A084177).
Contributions
The authors Seung-Deuk Byun and Tae-Du Jung have contributed equally to this work.