
Abstract
Introduction
The recovery of walking capacity has been recognized as one of the major goals for the functional rehabilitation of patients with post-stroke hemiparesis, and the reintegration of walking function into their community life is the final aim of their rehabilitation. 1,2 It is reported that 60–80% of patients with stroke can walk independently, in spite of chronic physical disability. 3 However, another study reported that only approximately 7% of patients capable of walking independently could provide an assurance of walking independently in the community again. 4 Community ambulation requires the ability to integrate walking with a variety of tasks in a complex and changing environment and the ability to successfully navigate in the community. 1 Recently, therapeutic concerns for patients have been increasingly emphasized with respect to the recovery of skills required for walking in the community. 2,5,6 The results of some advanced studies on enhancing the functional walking of patients with stroke suggest that goal-directed varying ambulation training that takes the actual environment into account should be used for such patients. 1,6
Numerous therapeutic approaches have been used clinically to improve ambulation capacity and to overcome physical problems that may be secondary to walking impairment. A task-oriented approach to walking training of the patients has been specifically established to encourage functional rehabilitation with the aim of improving physical conditioning. 7 To improve the walking function of patients with chronic stroke, strengthening training has also been incorporated into physical conditioning programmes in the clinical setting. 8 In addition, treadmill training with or without body weight support has been commonly accepted with regard to enhancing the walking function of patients. 9 The underlying problems caused by stroke may limit the engagement of the walking components related to environmental adaptation in the community; however, previously published studies had not been designed to investigate the effect of treadmill training on recovering the ambulation ability of patients in various community situations. 10
Previously published studies have also not investigated the effect of treatment on the recovery of the community ambulation ability of post-stroke patients. In most cases, the application of walking training and its evaluation is based on therapeutic indoor settings. However, although the mobility and walking function of chronic stroke patients have often been assessed by using clinical assessment tools that involved some items related to community activities, it is difficult to assess walking function in uncontrolled environments of community despite improved indoor activities. 5 Consequently, the therapeutic evidence obtained to date for community ambulation ability is not sufficient for applying a specific neurological treatment. Furthermore, to the best of our knowledge, there are only a limited number of studies on improving walking ability in actual community situations, which is the ultimate rehabilitation goal of patients with stroke. Therefore, this study aimed to investigate the effect of functional ambulation training performed in a real community environment for patients with post-stroke hemiparesis.
Methods
This study used a randomized controlled pilot design. The study population comprised 25 patients who had post-stroke hemiparesis and were receiving inpatient management service in a rehabilitation hospital; these patients had volunteered to participate in this study. The patients were randomly segregated into two groups: the experimental group (13 patients) and the control group (12 patients). The inclusion criteria for participation in this study were as follows: (1) the first stroke had occurred six months to five years before the study; (2) a walking speed of <0.7 m/s, which indicates unsafe community ambulation 11 ; (3) no auditory or visual deficits; (4) no orthopaedic or cardiovascular conditions that may interfere with the study; (5) no cognitive impairment (>25 in Mini-Mental State Examination). 12 All the subjects signed an informed consent form before participating in the study.
Outcome measurements
In this study, the walking function of the subjects were assessed by using three clinical walk tests (10-m walk test, 6-minute walk test, and community walk test with a 300-m walking route) and two questionnaires (walking ability questionnaire and activities-specific balance confidence scale).
For the 10-m walk test, the subjects were instructed to walk as fast as possible on a 12-m indoor walkway. Walking aids and/or foot orthoses were used, if required. To avoid the effects of acceleration and deceleration, measurements were obtained for the middle 10-m stretch of the walkway. 2 The time taken for walking at a self-adopted maximum speed was measured using a stopwatch (AST, KK-5898, USA). The 10-m walk test has high test–retest reliability in patients with stroke (intraclass coefficient (ICC) = 0.87). 13 The 6-minute walk test is a useful assessment tool for exercise tolerance in deconditioned individuals 14 and is reported to have high test–retest reliability with regard to measuring the distance travelled by individuals with neurological deficits (ICC = 0.94). 15 The subjects were instructed to walk repeatedly along a 20-m walkway for 6 minutes, with or without a walking aid. 16 Rest periods were allowed at the subjects’ request. The assessor did not encourage the subjects. The maximum distance walked in 6 minutes was recorded. The community walk test was performed on a walking route that involved crossing the street, stepping up and down the ramp/kerb, and stepping over some street obstacles. The walking path for testing was newly established to avoid the learning effect with respect to training routes that may have been used for subjects from the experimental group during community ambulation training aimed to evaluate walking function in an actual community situation. In accordance with suggestions made with respect to community ambulation in a study performed by Lerner-Frankiel et al., 17 the subjects were instructed to walk at a comfortable pace for 300-m in a community near our hospital. The time taken to walk 300-m was measured and multiplied by a factor corresponding to the level of walking aid used (no aid, ×1; ankle foot orthosis, ×2; mono cane, ×3; quadruped cane, ×4; ankle foot orthosis and mono cane, ×5; and ankle foot orthosis and quadruped cane, ×6). 18
The walking ability questionnaire was used to rate the subjects’ mobility with regard to certain aspects of 19 ambulatory tasks commonly performed indoor (8 activities) and outdoor (11 activities). 19 In the walking ability questionnaire, mobility was categorized on the basis of a 5-point scale (0, unable; 1, wheelchair; 2, assisted; 3, supervised; and 4, independent). The total walking ability questionnaire score possible is 76, and a high score implies excellent walking ability. The activities-specific balance confidence scale was used to assess the confidence levels of the subjects in executing 16 balance and mobility tasks, including outdoor activities. The activities-specific balance confidence scale is a numerical rating scale with scores ranging from 0 (no confidence) to 100 (compete confidence). 20 It has acceptable test–retest reliability (ICC = 0.86). 21 The scores were averaged across the 16 tasks, and the average value was used for subsequent analyses.
Procedures
The subjects were randomly allocated to the experimental group or control group. Each subject was given an envelope containing two cards and was instructed to blindly draw one card on each occasion. This study was single blinded: the person undertaking the assessment and data analysis was unaware of the group of each patient while the subjects and their therapist were not blinded to the treatment group. The experimental and control groups received a functional training based on the Bobath concept 22 daily for an hour, according to the routine schedule of the rehabilitation unit. The functional training consisted of standing up from a sitting position, therapist-guided movement of the trunk and lower limb to simulate normal walking pattern, forward and backward stepping of affected and unaffected lower limb, and stair climbing. In addition, the subjects from the experimental group underwent 1-hour sessions of community-based ambulation training; these sessions were conducted three times per week for a four-week period (i.e. a total of 12 sessions). The subjects in the control group did not receive specific walking training, other than daily rehabilitation training. To ensure the safety of the patients during training, a physical therapist followed the patients while they were undergoing the walking training. The outcomes were measured before and after the four-week training.
Community-based ambulation training
The community-based ambulation training programme consisted of four-phase walking training performed in various community situations, which were differently applied according to a weekly schedule. In accordance with the suggestions made in a study performed by Shumway-Cook et al., 6 the difficulty level of the walking training was increased every week, with different environmental demands in each session. During the four-week training period, walking training was conducted at various locations (e.g. in the foyer of a hospital, a pavement, stairs, a ramp, a car park, a pedestrian crossing, and a shopping centre), with progressive changes in the environmental demands (Appendix 1). Although it was planned that the subjects would progress to the next phase at the end of a week, they were allowed to proceed to the next phase if they could walk for 300-m of the given walking route of each phase without a rest interval. 17 In this study, five subjects did not meet the criteria for progression to the fourth phase from the third phase; therefore, these subjects underwent one more session on the walking route for the third week and only two sessions in the final fourth week phase.
Data analysis
The data obtained for the subjects were analysed using the SPSS 12.0 software (SPSS Inc., Chicago, IL, USA). The data for the two groups were expressed in terms of mean and standard deviation. Independent t-test was used to compare the two groups with respect to the demographic characteristics (age and stroke onset time) of the subjects. In each group, the differences between the pre-test and post-test data were analysed using the paired t-test. All variables between the groups and the difference in values of each variable within the groups were compared using independent t-test. The significance level was set at 0.05 for all analyses.
Results
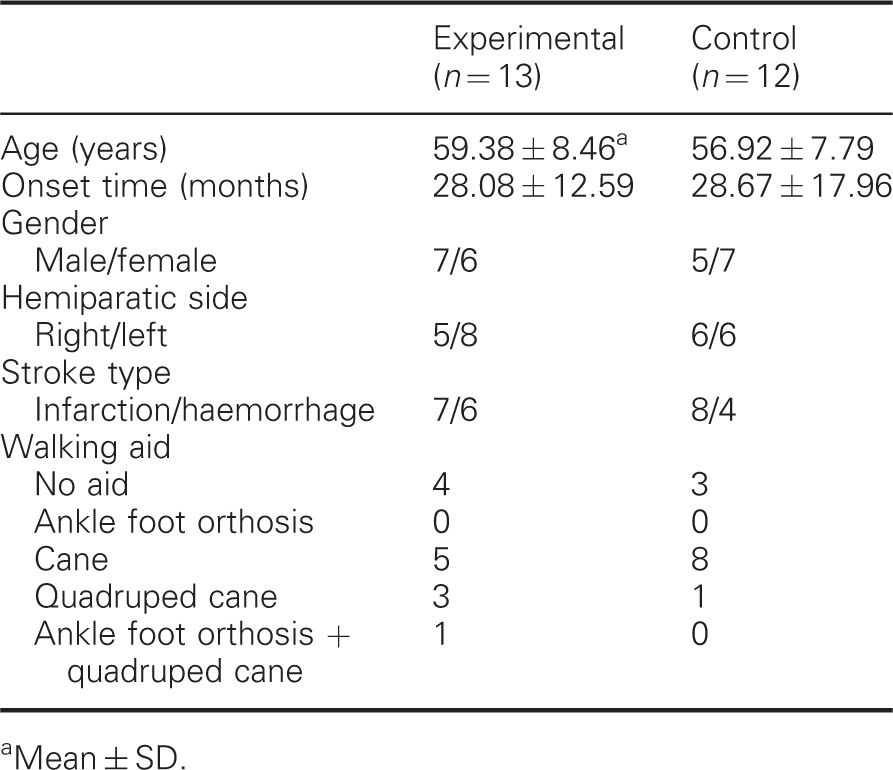
Although 27 patients were initially included in the study, 2 patients (1 from each group) were excluded because they did not regularly participate in the treatment sessions. Therefore, data for 25 patients were used for the analysis. Figure 1 shows a flowchart of the study. The demographic data of the subjects are summarized in Table 1. No statistically significant differences were observed between the two groups with respect to age (t = 0.76, P = 0.46) and onset time (t = −0.94, P = 0.93).
Flowchart of the study. Demographic information of the subjects Mean ± SD.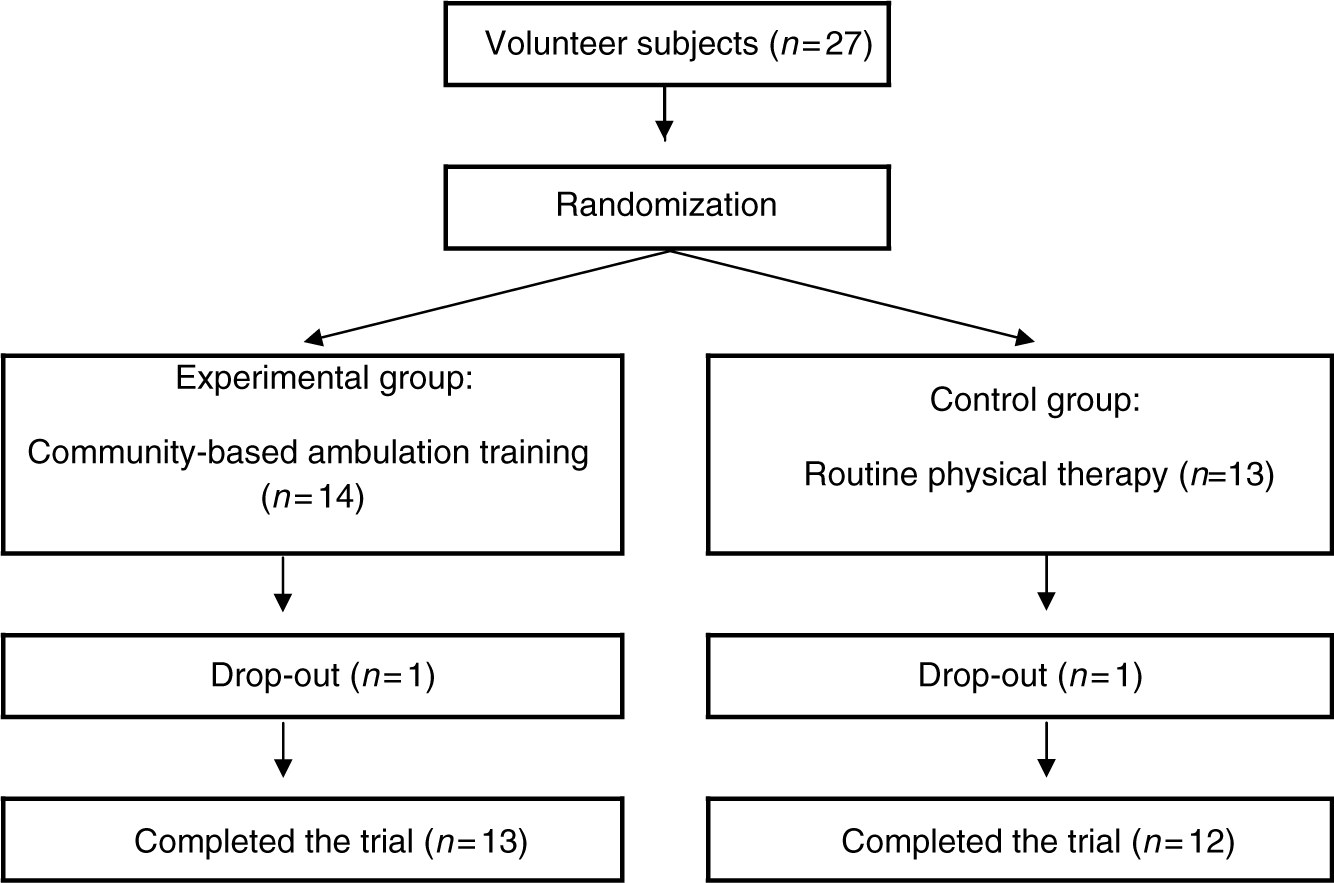
Comparison of the outcome measures within groups and between groups
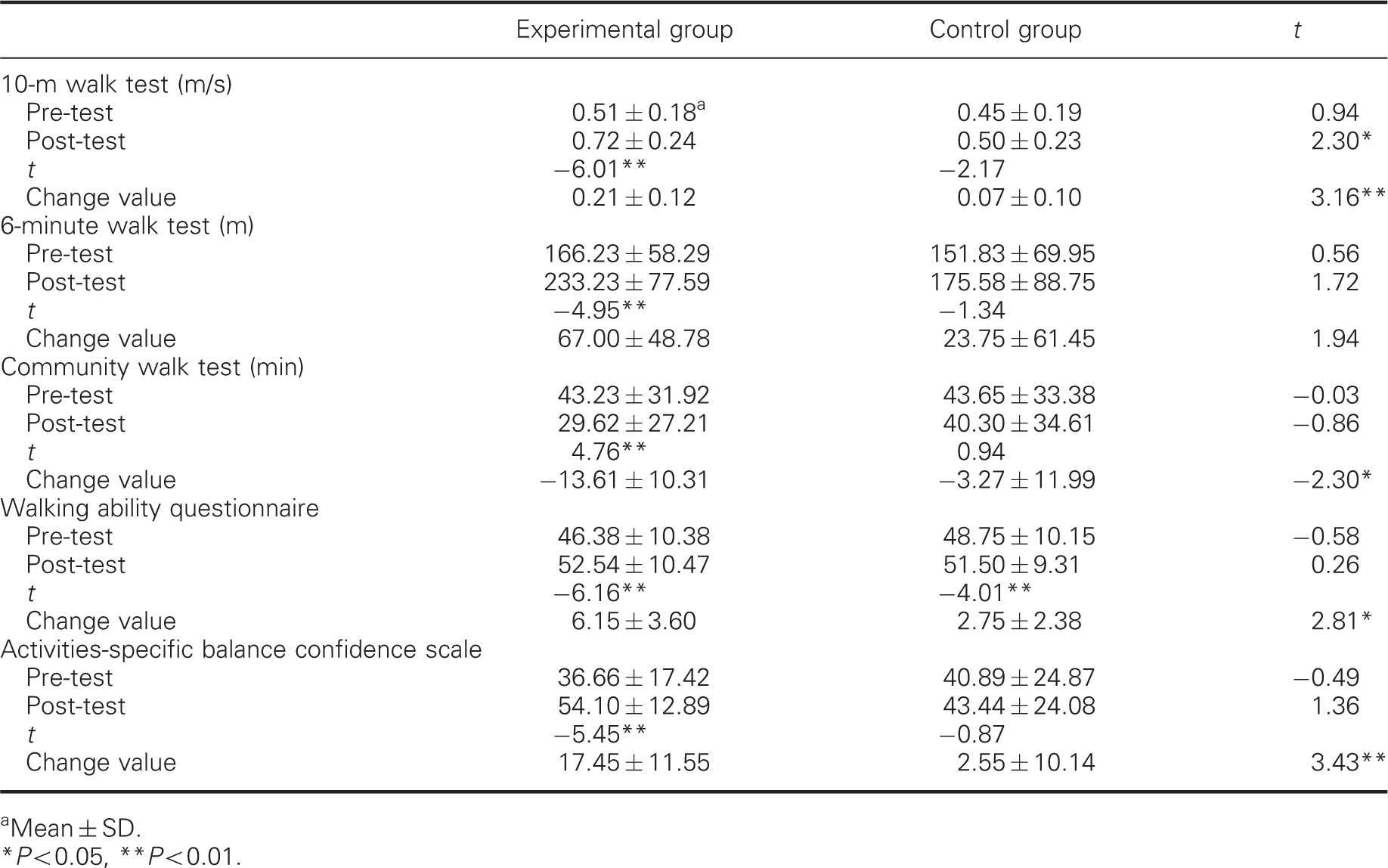
Mean ± SD.
P < 0.05, **P < 0.01.
Discussion
This study was performed to identify the effect of community-based ambulation training in patients with post-stroke hemiparesis. We found that if community-based ambulation training is integrated with routine functional training for patients with post-stroke hemiparesis, then it may provide additional benefits.
In general, walking training for most patients with post-stroke hemiparesis is conducted indoors, which is a predictable and controlled environment. It cannot be assumed that the skills required for walking under these conditions will suffice while walking outdoors. 1 Shumway-Cook et al. 6 suggested that eight environmental dimensions contribute to mobility and physical disability: distance, temporal factors, ambient conditions, physical load, terrain, attentional demands, postural transitions, and traffic density. Our training programme was scheduled such that there was a sequential increase in these environmental dimensions. The training during the first and second weeks involved a relatively simply designed walking route in order to enhance the adaptation of the patients to community ambulation training. At the beginning of the third week, the training involved more dimensions than in the previous phases, with the aim of reinforcing the community ambulation ability. In particular, this phase involved a pedestrian crossing, which may pose difficulties with respect to time limitations for post-stroke patients who walk slowly. 5 The inclusion of a pedestrian crossing in the walking route may be an important reason why some subjects did not meet specific criteria for progression to the next phase and experienced delay in advancing to the next phase.
In aspects of completing all training courses, the training in the final week was focused on walking practice for performing actual tasks and on supporting community participation, according to the recommendations of Shumway-Cook et al. 6 Although it is difficult to include all environmental dimensions, we tried to design the training route such that it met the requirements for community-based daily activities.
We found that the subjects from the experimental group experienced greater improvements in walking speed measured with the 10-m walk test at post-test than did the subjects from the control group. In addition, on comparing the pre- and post-test scores, we observed a significant improvement in all walking function-associated variables in the subjects from the experimental group, while the subjects from the control group exhibited improvements only in the walking ability questionnaire scores. Post-stroke walking is characterized by reduced walking speed, cadence, stride length and gait symmetry, with prolonged stance duration on the unaffected side and reduced step length of the affected limb. 23 Walking speed is an important factor related to community walking 24 and reflects the levels of walking ability, balance function, and overall physical condition. After ambulation training, significant improvement in 10-m walk test and community walk test scores, which represent indoor and outdoor walking capacities, respectively, may be directly associated with the walking ability questionnaire scores, which indicate the level of mobility for indoor and outdoor ambulatory activities. 19 The walking ability questionnaire scores for the subjects from the control group may be related to the effect of routine scheduled rehabilitation therapy that was performed during the study period. The Bobath concept-based therapy, which was routinely used in this study, may help in improving the proximal movement of the pelvis, with subsequent positive changes in the movement of distal parts such as the knee and foot. 22
It is frequently reported that patients with post-stroke hemiparesis do not experience complete satisfaction with their levels of outdoor mobility and community reintegration and perceive difficulties in community ambulation and community participation. 25 In this study, the community walk test scores significantly improved after community ambulation training, although the testing was performed using a new walking route that the subjects from the experimental group had not walked on during the training. This finding suggests that the ambulation training performed in this study can be used in various community situations. The results of this study indicate that community ambulation training, which is readily available in the clinical setting, may be used as an additional therapeutic option in order to provide patients with post-stroke hemiparesis a better opportunity for returning to community life.
Most studies on the walking rehabilitation of patients with post-stroke hemiparesis do not assess cognitive and psychological processes, such as fear, fatigue, depression, 17 and lack of confidence. The loss of independent ambulation – especially outdoors – is the most debilitating aspect of stroke sequelae and can cause frustration about not being able to leave the house. 25 However, in this study, the activities-specific balance confidence scale scores indicate that the confidence levels related to mobility and activity 20 significantly improved after the intervention. We believe that an improved level of walking confidence may influence the recovery of indoor and outdoor walking capacity and that this improved confidence level should be strongly associated with the quality of life of such patients. 3
The findings of this study are supported by those of some recent studies that involved community-based activity training; these studies reported that a community-based physical activity programme comprising mobility and environmental options is a safe, feasible and efficacious training method for patients with post-stroke hemiparesis. 26 Moreover, Lord et al. 27 suggested that a community-based walking programme is a practical alternative to routine rehabilitation therapy.
In recent times, virtual reality-based training that involves some community environments, including walking and crossing streets, stepping over obstacles, and walking in a car park, has been considered an efficient method to enhance the competency of such patients with respect to walking in the community. 2 Access to training is considered essential for managing patients with post-stroke hemiparesis in that it increases the patient’s participation and motivation to follow through with a given course of walking training. Virtual reality-based training may not be easily accessible to most patients because it requires specific apparatus for simulating various community environments.
Our study has some limitations, which can be improved in future studies. First, this study was a small pilot study. The sample size was determined by the number of subjects enrolled for training rather than power analysis. The small sample size of this study may be a major factor that limits the generalization of our results to the entire hemiparetic population. However, despite this limitation, many of the between-group and within-group comparisons were strongly in favour of the experimental group. These findings must be verified in a larger sample. Second, because of the absence of a long-term follow-up, we could not determine whether the community ambulation training would have a long-term effect. Finally, extra therapy time was provided to the subjects of the experimental group as part of the study design. The benefits of additional treatment rather than the specific therapeutic option cannot be entirely ruled out. Therefore, further controlled clinical studies with a larger study population and longer interventions are required to verify the clinical benefits of community-based ambulation training.
Clinical messages
Walking training may provide additional clinical benefits when designed by taking into account environmental barriers that patients with post-stroke hemiparesis can experience in their community life, and such a training may be more effective than inpatient training. Community-based ambulation training, which is readily available in the clinical setting, may be used as an additional therapeutic option for patients with post-stroke hemiparesis in order to give these patients a better chance of returning to community life.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Appendix 1 – Community-based ambulation training
The walking training in the first week was conducted on a 150-m route that comprised a hospital’s foyer, even ground near the hospital and low-rise stairs. To encourage subsequent adaptation for community ambulation training, the training in the early phase was initiated on a route that involved relatively simple environmental demands. The subjects were asked to walk through a crowd in one area; this is a task that has more attentional demands than treadmill walking.
The walking path for the training in the second week was 200-m long and included uneven ground outside the hospital and a pavement in a public place, which was used by many people. This training environment had more attentional demands than the first week’s training environment, and the subjects could not help walking on uneven outdoor surfaces.
For the third week, the subjects from the experimental group underwent walking training on a 300-m route, which is the minimum distance for successful community ambulation, in order to overcome some spatial and temporal barriers and promote confidence levels with regard to community ambulation. The route consisted of a low slope, a pedestrian crossing and a pavement, with some obstacles such as street trees and architectural barriers.
The walking training in the fourth week involved visiting a shopping centre near the hospital. To increase the difficulty level of the walking training, the 500-m walking route included a pavement, a pedestrian crossing and a car park in a shopping centre. In the shopping centre, the subjects were asked to ascend and descend stairs and to push a trolley. The final task involved the most complicated environmental changes, including changes in distance, temporal factors, physical load, terrain, attentional demands, postural transitions and traffic density.