
Abstract
Introduction
Fibromyalgia is a syndrome of widespread chronic pain associated with persistent fatigue, generalized morning rigidity, non-reparative sleep, cephalea, irritable bladder, dysmenorrhoea, extreme sensitivity to cold, restless legs, undefined pattern of numbness, tingling and intolerance to exercise.1,2 The condition may affect peripheral and/or central mechanisms of postural control, and is associated with balance problems and an increased frequency of falls. 3
According to Chaitow, 4 the dysfunction model in fibromyalgia syndrome has three aetiological factors (biochemical, biomechanical and psychosocial) that interact with innate and acquired characteristics to determine the vulnerability and susceptibility of an individual. The following interactions among these factors have been proposed: (1) a negative emotional state may produce specific biochemical changes, weakened immunological function and alteration of muscle tone; (2) hyperventilation modifies blood oxygenation at neuronal level, generating a state of anxiety/apprehension and having a direct impact on structural components of the thoracic and cervical region; and (3) chemical changes in blood flow may produce mood and structural changes. 4
Although fibromyalgia is not a musculoskeletal disease, most of the symptoms manifest at this level. Bialosky et al. 5 introduced the term ‘facilitation phenomenon’ to explain some events in musculoskeletal pain, especially myofascial pain, stating that neuronal structures may become hyperreactive at spinal or paraspinal tissue level (‘segmental facilitation’). Points of hyperreactivity are designated ‘trigger points’ when detected in ligament, tendon or periosteal tissue and ‘myofascial trigger points’ when in muscle or fascia.
Central sensitization is well documented in fibromyalgia but its cause remains unclear. It occurs when persistent nociceptive input leads to increased excitability in the dorsal horn neurons of the spinal cord. 6 In this hyperexcited state, spinal cord neurons produce an enhanced responsiveness to noxious stimulations and even to formerly innocuous stimulations. There is some evidence of dysfunction of the intramuscular connective tissue or fascia in fibromyalgia. 6
Vleeming et al. 7 highlighted that the posterior oblique system of functional stability involves thoracolumbar fascia and paravertebral, latissimus dorsi, trapezius and gluteus maximus muscles, being closely related to the psoas muscle. Alterations in this system are related to psoas weakness, with a direct influence on sacroiliac articulation. Hence, adipose thickening of the thoracolumbar fascia may be related to alteration of the fascial functional system, generating one of the most frequent localizations of primary fascial entrapment in fibromyalgia patients. Based on this theory, Schleip8 developed a map of ‘hypersensitivity points’ in the most frequent areas of fascial plane entrapment. These hypersensitivity points coincide with the points described by the American College of Rheumatology. 8
Liptan 6 proposed inflammation of the fascia as the source of peripheral nociceptive input that leads to central sensitization in fibromyalgia, attributing the fascial dysfunction to inadequate growth hormone production and hypothalamic pituitary adrenal axis dysfunction in fibromyalgia. The main cell of the richly innervated fascia, the fibroblast, secretes proinflammatory cytokines in response to strain, and immunohistochemical studies of biopsies have revealed elevated levels of collagen and inflammatory mediators in the connective tissue surrounding muscle cells in fibromyalgia patients. 6 According to Liptan, if it is confirmed that inflammation and dysfunction of the fascia can lead to central sensitization in fibromyalgia, treatment options could be expanded to include manual therapies directed at the fascia, such as myofascial release. While various studies have demonstrated the efficacy of different complementary therapies, 8 – 16 effective and readily available methods of manual therapy could be valuable in the treatment of fibromyalgia.
In a study on fibromyalgia and balance disorders and falls, Jones et al. 17 found that fibromyalgia symptoms of fatigue, stiffness, pain, sleep, anxiety and feeling depressed were associated with difficulties in knowing how far one can lean from a seated position, accurately attaining vertical realignment, maintaining balance while standing with eyes closed, and reaching laterally or forward while keeping heels on the ground. Their findings suggest that the totality of fibromyalgia symptoms rather than pain alone may be responsible for the poor balance demonstrated in the study. 18 A previous study by our group on the efficacy of myofascial therapy in fibromyalgia patients found that one weekly session produced a significant improvement in anxiety, sleep and quality of life. 19 The aim in the present study was to explore whether a more intensive therapeutic protocol (two sessions/week) could achieve an improvement in physical function and postural stability in these patients.
The objective of this study was to evaluate the usefulness of myofascial therapy to improve pain, physical function, and postural stability in fibromyalgia patients, based on the fascial connection between the rectus capitis posticus minor muscle and the dura mater at the level of the atlanto-occipital joint. 20 Numerous researchers have postulated that a lesion or stressful event in this area may trigger the chronic pain of fibromyalgia syndrome.10,20– 22
Methods
This single-blind clinical trial was nested in an experimental study. Intragroup and intergroup differences (experimental group and placebo group) were evaluated at baseline (pre-test), immediately after the 20-week intervention, and again at six months and one year. The experimental period was from 15 November 2007 to 15 March 2009. Before enrollment, all subjects signed informed consent to participate in the study, which was approved by the ethics committee of the University of Almeria. Participants were told they could leave the study at any time. Written informed consent was obtained from all patients before their participation in the study, which complied with the ethical criteria established in the Helsinki Declaration (2008 modification) on research projects and with current Spanish legislation on clinical trials (Royal Decree 223/2004 February 6) and biomedical research (Law 14/2007 of July 3). The confidentiality of study material was in accordance Spanish legislation on personal data protection (Law 15/1999 of December 13).
The target population consisted of patients diagnosed with fibromyalgia syndrome by physicians at the Torrecardenas Hospital Complex, and the accessible population comprised those with computerized clinical records held by the Fibromyalgia Association of Almeria (Spain) and receiving pharmacology therapy: 32 patients treated with anxiolytics, 41 with antidepressants, 86 with anti-inflammatories, 43 with corticoids, 26 with antibiotics, 64 with sleep inducers, and 79 with muscle relaxants.
Inclusion criteria were: age 40–65 years, agreement to attend evening therapy sessions, limitation of usual activities due to pain on at least 1 day in the previous 30 days, and/or moderate or worse average pain level (≤4 on 10-point scale). 23 Exclusion criteria were: receipt of non-pharmaceutical therapies; presence of infection, fever, hypotension, treatment-limiting respiratory disorders; and alterations in cutaneous integrity. 24 The theoretical sample, recruited by consecutive sampling, was formed by 155 patients. Out of 155 patients in the accessible population, 61 were excluded, and the remaining 94 patients were randomly assigned by means of a balanced stratified assignment to an experimental (n = 47) or placebo (n = 47) group. The groups were balanced for type of medication received, sex and age by using a stratification system that generates a sequence of letters (from a table of correlatively ordered permutations) for each category and combination of categories. The sequences assigned to patients were placed in envelopes containing the allocation to each study group.
Researchers telephoned selected patients and invited them to the laboratory for initial interview; for females of childbearing age, the appointment was on the day after the expected end of the menstrual period. At this interview, demographic characteristics were recorded and baseline outcome data were gathered. All determinations were obtained at least 3 hours after the last food intake and 4 hours after the last medication dose. 25 After the initial interview, patients were randomly assigned to the experimental or placebo group. Both groups underwent their corresponding intervention for 20 weeks. Assessments were repeated immediately after the final treatment session and at six months and one year. Outcomes were determined by another researcher, who was blinded to the study group of patients. However, the physiotherapist (specialist in myofascial therapy) who administered both intervention protocols and the patients themselves were not blinded to their status.
Intervention protocol
Patients in the experimental group underwent a myofascial therapy protocol, administered in the following order:20,26– 29 deep fascia release in temporal region, suboccipital release, compression–decompression of temporomandibular joint, global release of cervicodorsal fascia, release of pectoral region, diaphragm release (transverse slide), transverse diaphragmatic plane, lumbosacral decompression, release of psoas fascia and release of fascia of the lumbar square (Appendix 1).
Twice-weekly for 20 weeks, the experimental group received a 1-hour session of 10 myofascial release modalities. The placebo group received sham short-wave and ultrasound treatment for 30 minutes twice-weekly for 20 weeks. Both electrotherapy procedures were applied with disconnected equipment on cervical, dorsal and lumbar regions for 10 minutes on each region. Patients were unaware that the equipment was disconnected and that this was a sham treatment.
Outcome measures
Data on demographic characteristics were collected at baseline. Primary outcome variables were number of tender points, pain and postural stability. Secondary outcome variables were physical function, clinical severity and global clinical assessment of improvement.
Assessment of tender points
Eighteen tender points were evaluated using a pressure algometer (at 4 kg of pressure) that measures pressure (applied with a rubber tip) in 0.5 kg intervals from 0 to 5 kg (Wagner FPI 10-USA). Tender points were bilateral at: lower back of head at insertion of occipital muscles; anterior sides of intertransverse spaces, from cervical vertebra C5 to C7; medium area of upper trapezius muscle; origin of supraspinal muscle above scapulae close to their internal margin; insertion of second ribs above sternum; bony prominence of humerus at the origin of forearm extensor muscle; upper external quadrants of buttock in anterior fold of gluteal muscle; crest of greater trochanter of femur at insertion of piriform muscles; subcutaneous tissue of internal side of knee above joint line.30,31
Pain
The McGill Pain Questionnaire (MPQ) was used to assess pain levels. It is based on a multidimensional perception of pain: sensory–discriminative, motivational–affective, and cognitive–evaluative. 32 It includes: (1) 62 descriptors distributed among 15 classes and the three dimensions, with scores ranging from 0 to 33 for the sensory dimension, 0 to 12 for the affective dimension, and 0 to 45 for the evaluative (sensory + affective) dimension; (2) a visual analogue scale (VAS) to assess pain intensity and relief experienced by the patient (0 = no pain, 10 = unbearable pain); and (3) a representation of the human figure on which patients indicate the exact localization of pain. 32
Postural stability
Postural stability was determined by studying the balance of patients with a stabilometer platform (Biodex Medical System, USA), used for the diagnosis and proprioceptive treatment of patients with balance disorders. 33 Patients were asked to find the most stable foot placement on the platform, since this position was maintained throughout all three trials. This was the reference point from which the centre of pressure was measured. Patients were instructed to maintain the platform as stable as possible. The stabilometer setting was at level 8 during all tests. Patients were instructed to cross their arms at chest level to minimize their use to attain balance. Each lower extremity was tested three times, as in previous studies using the Biodex Stabilometer for assessment postural stability. 33 The mean of three trials was determined. A higher score indicates lesser postural stability.
Physical function
The Spanish version of the 10-item Fibromyalgia Impact Questionnaire was used to measure the impact of fibromyalgia symptoms on the physical and mental health of patients. 34 It explores physical, psychological, social and well-being dimensions and includes six visual analogue scales to evaluate fatigue, pain, rigidity, morning tiredness, anxiety and depression components. It assesses well-being, physical function, loss of working days and capacity for work. The Spanish version was validated in a sample of 102 females from the city of Madrid, obtaining high degrees of test–retest stability for almost all scales, except for scales of sleep disturbance, rigidity and anxiety, which showed moderate stability degrees, similar to the findings of the English version of the questionnaire. The authors recorded a high degree of internal consistency, although the relationship of the questionnaire with the currently most objective test (number of painful tender points) was discrete. Nonetheless, the authors demonstrated that the Fibromyalgia Impact Questionnaire is a good instrument to detect sensitivity to therapeutic change. 34
Clinical severity
The Clinical Global Impression Severity Scale was used to assess the physical state of the patient. Patients rated themselves on a Likert scale (1 = disease-free to 7 = extremely ill). 35
Global Clinical Assessment of Improvement
The Clinical Global Impression Improvement Scale was used to assess the overall clinical improvement as perceived by patients, who responded on a Likert scale (1 = much better to 7 = extremely ill). 36
All quantitative data were entered in a SPSS 17.0 database. The reliability and validity of the model was studied by analysing residual independence, normality and variance homogeneity. Residual independence was analysed by plotting the values obtained against residues, resulting in randomly distributed points showing no specific trend and therefore verifying the residual independence assumption. Residual normality was studied by using a Q-Q graph, finding the dots to be located close to the line and therefore confirming the residual normality assumption. Variance homogeneity was tested with the Levene test, obtaining a 95% confidence level and P-value > 0.05, confirming variance equality.
Frequency distributions were generated to examine missing data, out of range scores and the logical distribution of response options, and all measures were scored. We calculated an imputed score for standardized scales missing ≤ 10% of responses. Independent t-tests were used to compare baseline demographic characteristics between participants and drop-outs and between experimental and placebo groups. Within-group changes in painful points, physical function, pain, postural stability, clinical severity and severity improvement were analysed by using a 2 (groups: experimental and placebo) × 4 (time points: baseline, immediately post intervention, at six months and one year) repeated-measures analysis of variance (ANOVA). A 95% confidence interval (CI) (α = 0.05) was considered in all tests.
Results
Figure 1 depicts the flow of participants through the trial. Out of 155 patients screened for eligibility, 94 were enrolled and randomly assigned to intervention (n = 47) and placebo (n = 47) groups. The study was fully completed by 45 in the experimental group and 41 in the placebo group (see Figure 1 for drop-out details).
Flow of participants through the randomized trial. None of the 94 participants reported adverse effects.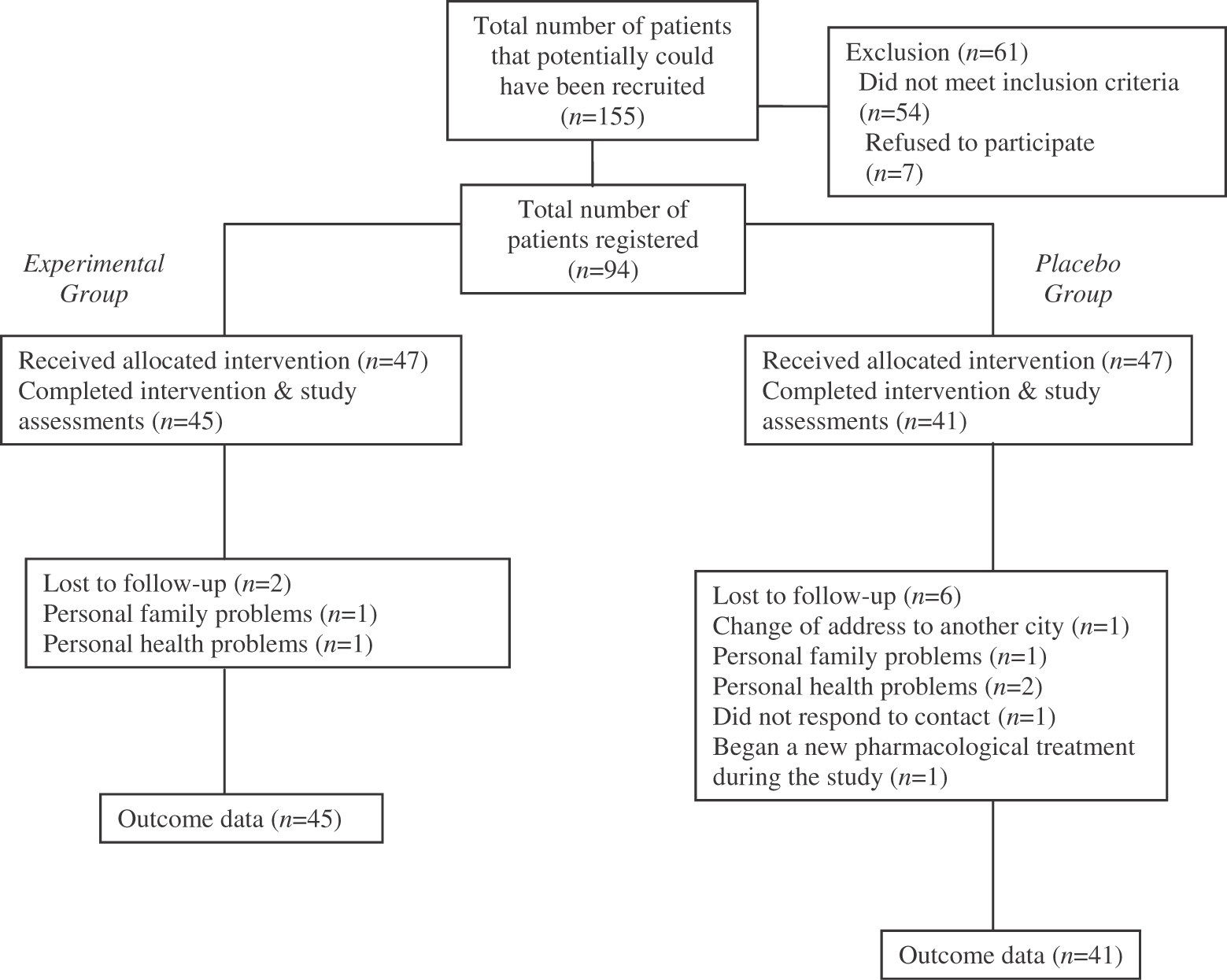
Patient characteristics
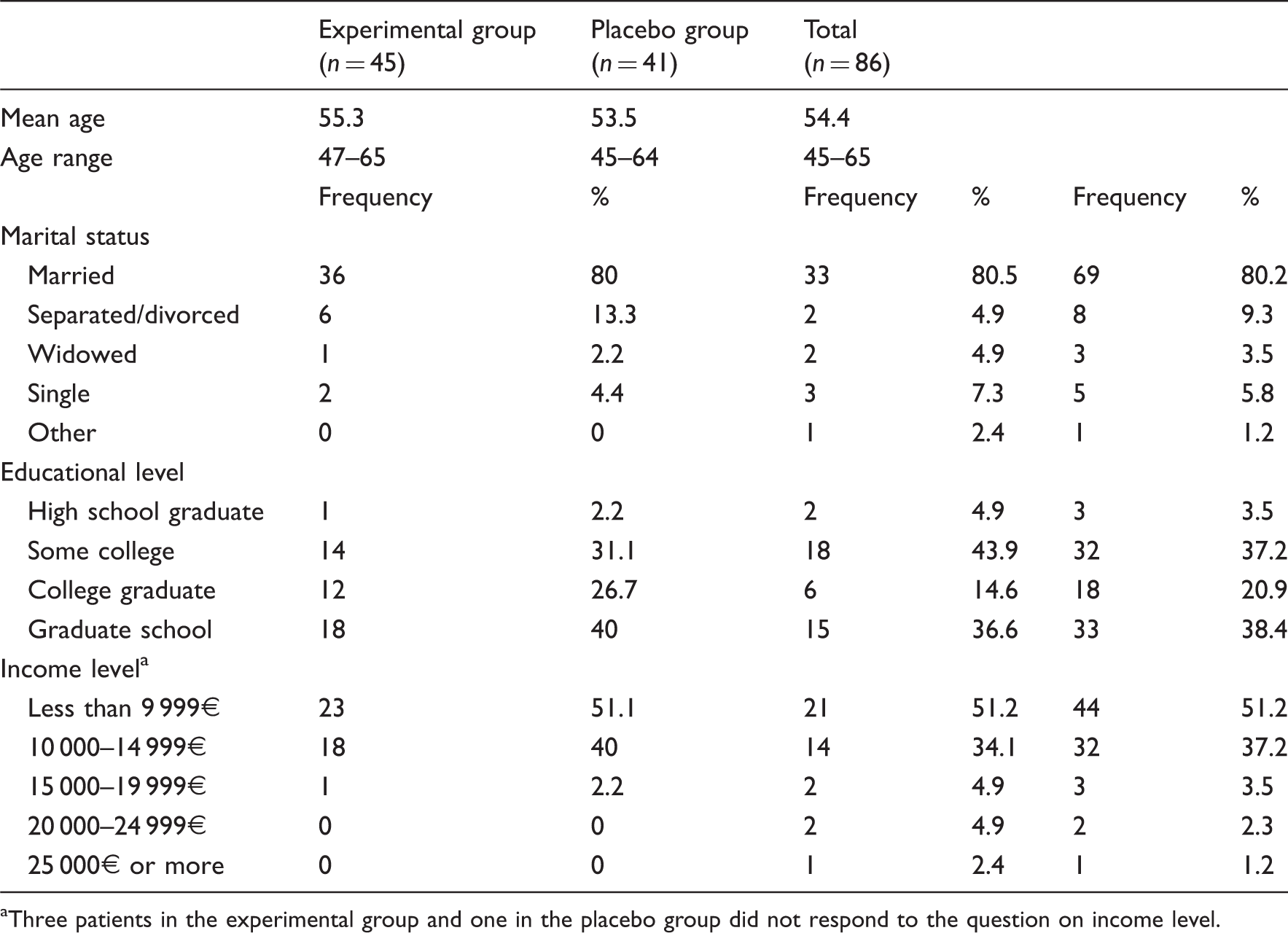
Three patients in the experimental group and one in the placebo group did not respond to the question on income level.
Significant differences between groups in numbers of patients with painful tender points (9 tender points I)
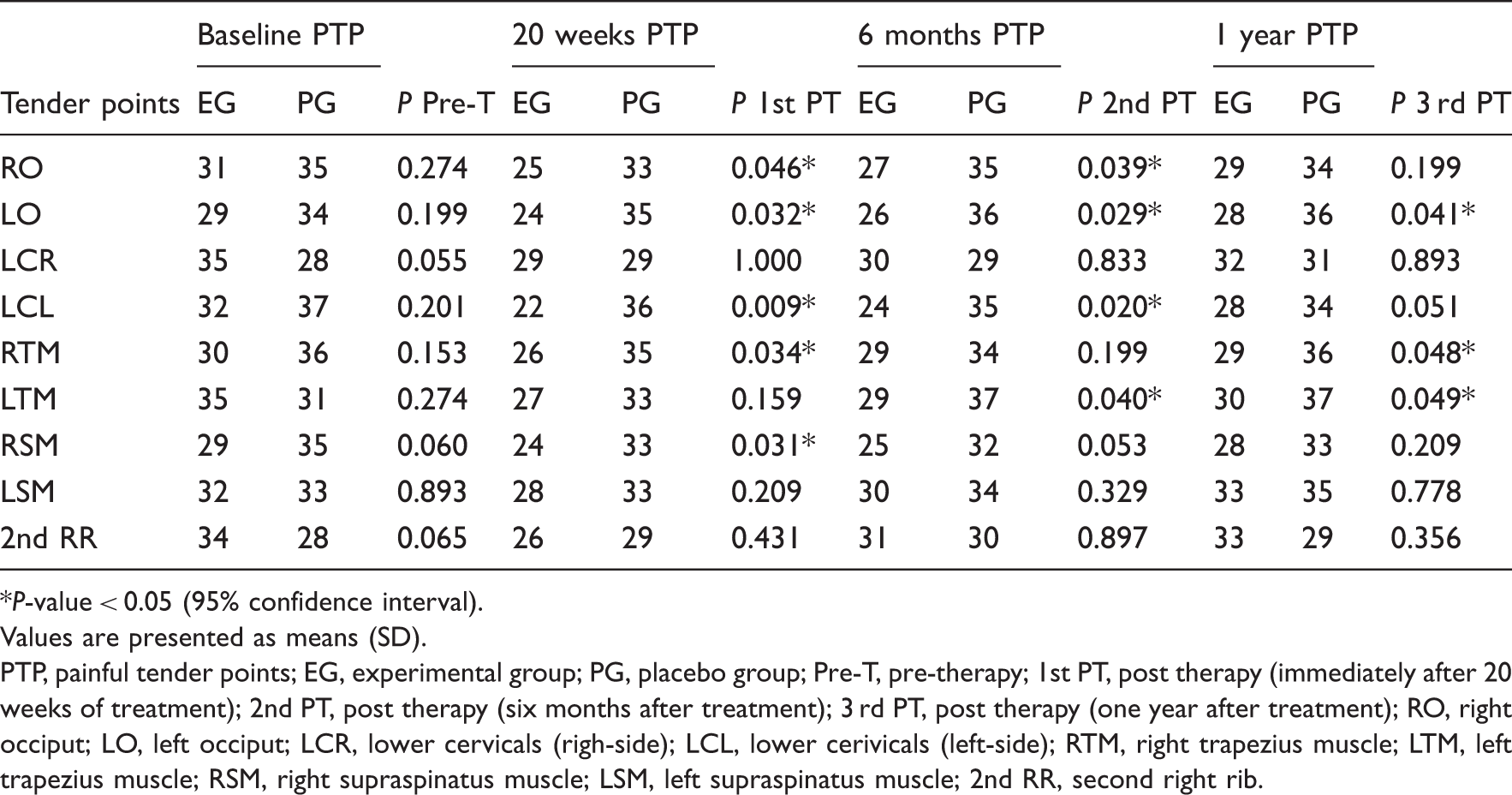
P-value < 0.05 (95% confidence interval).
Values are presented as means (SD).
PTP, painful tender points; EG, experimental group; PG, placebo group; Pre-T, pre-therapy; 1st PT, post therapy (immediately after 20 weeks of treatment); 2nd PT, post therapy (six months after treatment); 3 rd PT, post therapy (one year after treatment); RO, right occiput; LO, left occiput; LCR, lower cervicals (righ-side); LCL, lower cerivicals (left-side); RTM, right trapezius muscle; LTM, left trapezius muscle; RSM, right supraspinatus muscle; LSM, left supraspinatus muscle; 2nd RR, second right rib.
Significant differences between groups in numbers of patients with painful tender points (9 tender points II)
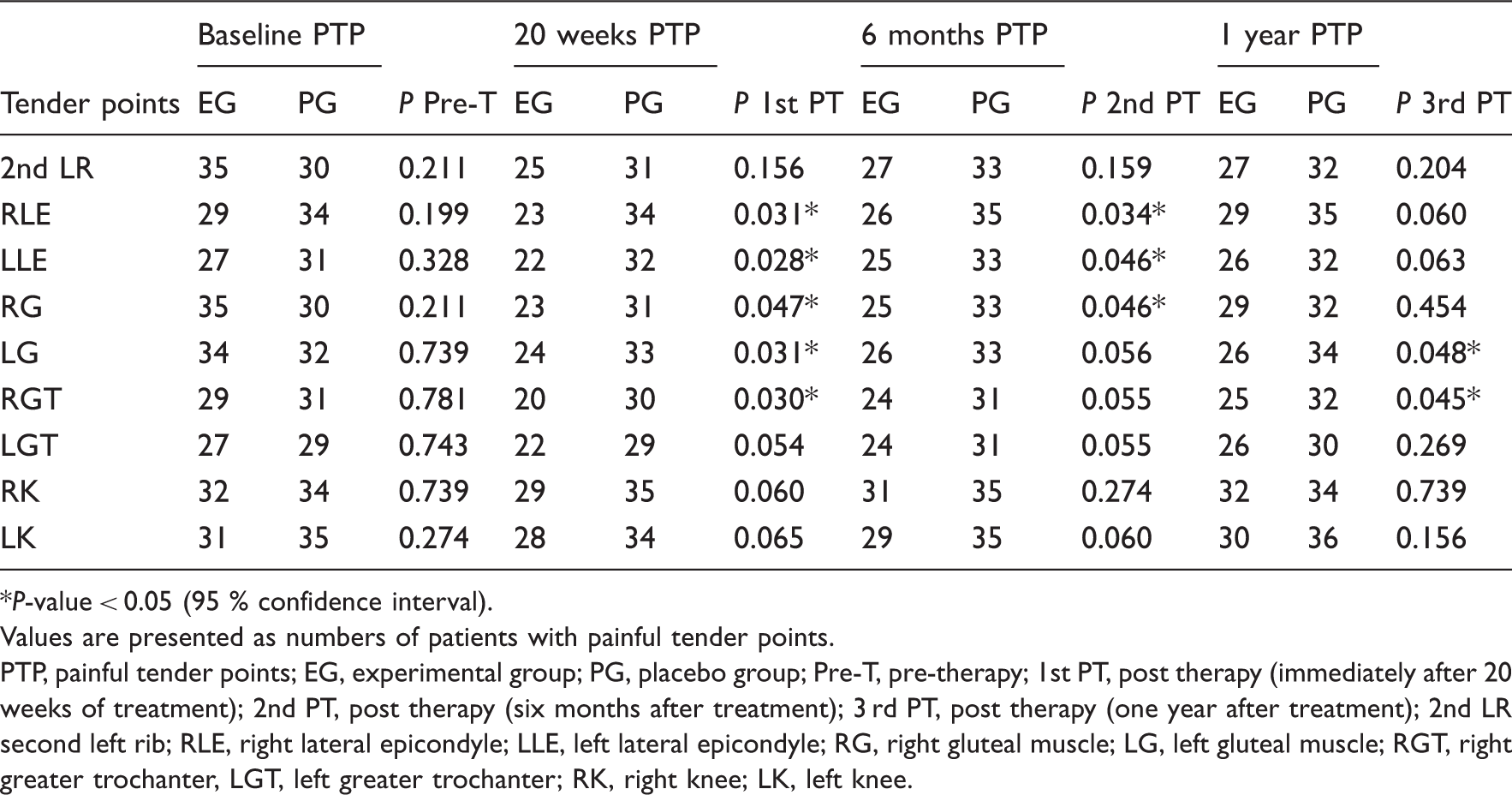
P-value < 0.05 (95 % confidence interval).
Values are presented as numbers of patients with painful tender points.
PTP, painful tender points; EG, experimental group; PG, placebo group; Pre-T, pre-therapy; 1st PT, post therapy (immediately after 20 weeks of treatment); 2nd PT, post therapy (six months after treatment); 3 rd PT, post therapy (one year after treatment); 2nd LR second left rib; RLE, right lateral epicondyle; LLE, left lateral epicondyle; RG, right gluteal muscle; LG, left gluteal muscle; RGT, right greater trochanter, LGT, left greater trochanter; RK, right knee; LK, left knee.
Differences between groups in Fibromyalgia Impact Questionnaire score, McGill Pain Score, Clinical Global Impression Severity Scale, Clinical Global Impression Improvement Scale and postural stability
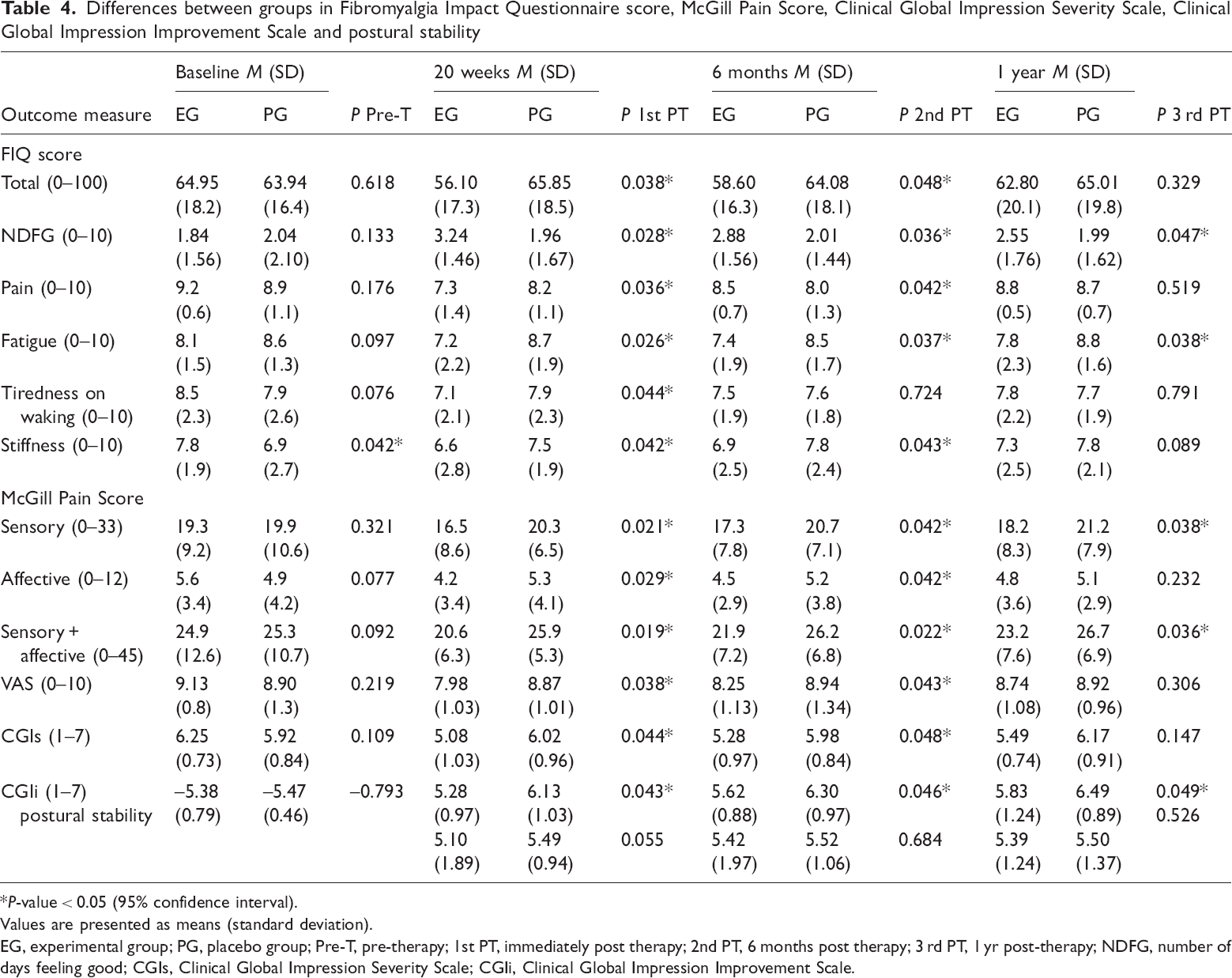
P-value < 0.05 (95% confidence interval).
Values are presented as means (standard deviation).
EG, experimental group; PG, placebo group; Pre-T, pre-therapy; 1st PT, immediately post therapy; 2nd PT, 6 months post therapy; 3 rd PT, 1 yr post-therapy; NDFG, number of days feeling good; CGIs, Clinical Global Impression Severity Scale; CGIi, Clinical Global Impression Improvement Scale.
No significant difference in postural stability was found between groups at any time, and there were no significant changes in either group among the different time points (Table 4).
At baseline, patients had an elevated global Fibromyalgia Impact Questionnaire score, with a mean of 64.95 (SD 18.2) for the experimental group and 63.94 (SD 16.4) for the placebo group. After 20 weeks of therapy, the experimental group showed a significant improvement in total Fibromyalgia Impact Questionnaire score (F = 6.54, P < 0.029), number of days feeling good (F = 6.81, P < 0.022), pain (F = 6.95, P < 0.021), fatigue (F = 5.02, P < 0.038), tiredness on waking (F = 5.24, P < 0.032) and stiffness (F = 4.96, P < 0.038). At six months post intervention, improvements persisted in total score (F = 2.71, P < 0.049), number of days feeling good (F = 5.32, P < 0.032), pain (F = 5.07, P < 0.037), fatigue (F = 3.36, P < 0.045), tiredness on waking (F = 3.51, P < 0.041) and stiffness (F = 3.29, P < 0.043). At one year, only number of days feeling good (F = 3.02, P < 0.044) showed a significant improvement. No significant improvements in any dimension were shown by the placebo group at any time point. Table 4 shows the significant differences between the groups.
Mean (SD) baseline clinical severity scores did not significantly differ (P < 0.109) between the experimental (6.25 (SD 0.73)) and placebo (5.92 (SD 0.84)) groups. The experiment group showed significant differences at the three post-therapy assessments: immediate (F = 5.02, P < 0.039), six months (F = 3.29, P < 0.043), and one year (F = 3.36, P < 0.045). The placebo group showed no significant differences at any time. Table 4 shows the differences between study groups.
Clinical improvement was not recorded at baseline. The groups differed in this parameter immediately, six months and one year after the intervention (Table 4). Neither group showed significant differences between the score immediately after the intervention and those recorded at six months and one year.
Discussion
After a 20-week weekly programme of myofascial therapy, fibromyalgia patients showed a significant reduction in pain according to pressure algometry results and McGill Pain Questionnaire, Clinical Global Impression Severity Scale and Fibromyalgia Impact Questionnaire scores. However, there was no significant decrease in postural stability as a result of this treatment.
We found that sociodemographic variables (e.g. age, previous duration of disorder, academic level, profession) had no influence on the intensity of the impact of fibromyalgia as measured by the Fibromyalgia Impact Questionnaire, in agreement with results of the original questionnaire validation study. 34 Lindberg 37 considers that variables related to instrumental quality of life should be analysed separately from those related to well-being, but the Spanish version of this questionnaire does not make this distinction. Other authors used the Fibromyalgia Impact Questionnaire to assess the outcomes of manual lymph drainage therapy and connective tissue massage and found significant improvements in a lower number of items than in our study, although they studied a sample of women for only three weeks, and the persistence of these effects was not recorded. 38
Significant improvements in physical function and pain, similar to the present results, were reported after a programme of connective tissue manipulation in patients with fibromyalgia. 39 Our group previously reported an improvement in 8 out of 18 painful tender points by the once-weekly application of myofascial therapy. 19 In the present study, with two-weekly sessions, a significant improvement was obtained in 10 painful tender points and in the sensitive, affective and sensitive + affective dimensions of the McGill Pain Score.
In countries such as Sweden, Holland, Denmark, Norway and the United States, the ‘Mesendieck System’ is one of the first therapies applied to patients with musculoskeletal problems due to muscle balance alterations; it encourages patients to understand the causes of their muscular pain in order to internalize the life habits that must be modified to improve their body functions. A study 40 of 90 fibromyalgia patients reported that they still showed significant improvements in physical function and pain at 18 months after application of the Mesendieck System.
Fatigue, stiffness, pain, sleep, anxiety and feeling depressed were associated with difficulty in maintaining balance. 17 In a previous study, 19 myofascial therapy significantly improved pain, sleep duration, anxiety and physical role in fibromyalgia patients. In the present study, a more intensive protocol of myofascial therapy failed to achieve a significant improvement in postural stability. However, a significant improvement was found in fatigue, tiredness on walking, stiffness, and number of days feeling good immediately after the therapy. A more prolonged course may be required to significantly improve the postural stability of these patients by obtaining greater and longer lasting benefits in terms of pain, physical function, anxiety, fatigue, stiffness and quality of sleep.
Authors who adopted multiple approaches in fibromyalgia patients (pharmacological therapy, physical exercise and cognitive education techniques) obtained significant improvements in almost all Fibromyalgia Impact Questionnaire items.40,41 There were no changes in the pharmacological therapy of the patients during the present study. Other authors 42 who used a multimodal approach (physical, educational and pharmacological measures) in fibromyalgia patients obtained significant differences in 9 of the 13 items in the Fibromyalgia Impact Questionnaire, although they stressed that the presence of depression is a key factor influencing Fibromyalgia Impact Questionnaire results. Another study that applied myofascial therapy in combination with aerobic exercise proposed myofascial pain treatment within a programme of multidimensional rehabilitation for patients with generalized chronic pain. 43
The lack of a postural stability test with a higher level of difficulty is a study limitation. However, the decision was taken not to exceed level 8 due to the loss of stability shown by patients in a preliminary pilot study. Another limitation is that the therapist who administered both intervention protocols and the patients themselves could not be blinded. A further study weakness is the absence of a ‘hands-on’ component in the sham treatment with disconnected electrotherapy equipment. Further research is warranted to compare outcomes obtained with our protocol with those of other manual therapies.
This study has demonstrated that fibromyalgia patients can benefit from myofascial techniques. In these patients, the decrease in muscular tension secondary to the release of myofascial restrictions improves physical function, fatigue, number of days feeling good, tiredness on walking and stiffness. Myofascial therapy significantly improves several clinical dimensions of the fibromyalgia syndrome, with an important and consistent improvement in pain, sensory, and affective dimensions.
Clinical messages
Myofascial therapy can contribute to improving physical function, fatigue, number of days feeling good, tiredness on walking, and stiffness in fibromyalgia patients. Myofascial therapy improves pain and other clinical, sensory and affective dimensions of fibromyalgia syndrome. However, a programme of 40 treatment sessions produces no significant improvement in the postural stability of these patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.