
Abstract
Introduction
Stroke is the major cause of disability in adults. 1 If the upper limb is affected, only 5–20% of stroke patients will regain full arm and hand function, 2 leaving the majority with severe impairment or complete loss of function in the long term. 3 – 5 Stroke survivors with persistent functional loss have only a minimal chance of regaining further function 6 which emphasizes the need for valuable and effective treatment regimens focusing on arm and hand function. Existing evidence for the efficacy of widely used treatment concepts to improve arm and hand function such as conventional neurological therapy and constraint induced therapy is limited. 7 A new treatment approach, called ‘therapeutic climbing’, 8 is increasingly propagated, however, without any controlled data.
Conventional neurological therapy is based on neurophysiological theories proposing that spasticity prevents economic and effective movement and therefore must be controlled in order to achieve efficient movement strategies. The classical aspects symmetry, posture and inhibition of ineffective synergistic movements characterize this treatment approach. Conventional neurological therapy is nowadays generally complemented by functional task-orientated strategies. 9 A recent systematic review showed no significant differences between a neurophysiological approach and other treatment strategies. 10
Constraint induced therapy as described by Taub et al. 11 requires the wearing of a restraining mitt on the less-affected hand for 14 hours a day and repetitive task training with the affected hand, constraining inhibitory overactivity of the non-affected brain hemisphere, thus allowing reorganization of the affected cerebral cortex with functional recovery and preventing learned non-use. Due to these high time demands compliance rates have been reported to be low. 12 Further limitations are the 6 hours of individual treatment per day, requiring high therapist resources and consequently causing high costs. The efficacy of constraint induced therapy for arm management in hemiparetic patients was assessed in two systematic reviews,13,14 finding a moderate reduction of disability assessed at the end of treatment which was not maintained in the long term. The benefit of constraint induced therapy in individuals with minimal to moderate arm and hand function remains unclear.
Therapeutic climbing has been developed from sports climbing. Rationales for its use are based on results of studies indicating an improved recovery of arm and hand function by bilateral arm training.15,16 Using shaping techniques, repetitions and motivational aspects motor relearning and functional recovery is promoted. Experiences showed promising results indicating therapeutic climbing to be a safe treatment option with generally good acceptance by stroke patients. Adaptations for patients with minimal to moderate arm and hand function are possible; however, the functional gain is not clear. Controlled data are required also with a focus on adverse effects such as shoulder pain.
In view of the lack of evidence for the effectiveness of these three treatment approaches to improve minimal to moderate arm and hand function after stroke as well as the possibility of adverse effects we considered further research to be urgently needed. The aims of this study were therefore twofold: first, to test a study design investigating the effects of these three treatment approaches on minimal to moderate arm and hand function in patients after stroke, and second, to explore the feasibility and potential effects of these three treatment approaches within this patient group.
Methods
This pilot randomized clinical trial with blinded assessment at baseline, post intervention and six months follow-up was conducted in the Neurorehabilitation Center Valens, Switzerland, and was approved by the ethical committee of the Canton of St. Gallen.
Patients suffering from acute, subacute and chronic stroke referred for inpatient rehabilitation were included in the study if the following criteria were fulfilled: (a) improvement of arm and hand function as the primary rehabilitation goal, (b) minimal to moderate arm and hand function (stage 2–6 on the Chedoke-McMaster Impairment Inventory subscales arm and hand control 17 ), (c) no shoulder pain (Chedoke-McMaster Impairment Inventory subscale shoulder pain at least stage 5 17 ), (d) capable of walking a minimum of 20 m with assistance or walking aids, (e) capable of understanding treatment instructions and providing informed consent, and (f) written informed consent. Patients were excluded if there were other neurological disorders or other serious comorbidities.
The primary goal of all interventions was to improve arm and hand function. As the intensity of treatment for restoring arm and hand function after stroke was considered to be crucial, it was an important prerequisite of this study to provide a high amount of therapy in all three intervention groups. Therefore, in addition to individual treatment sessions resource-friendly group therapies were included in the treatment programme.
Conventional neurological therapy included individual physiotherapy (5 hours) and occupational therapy (2.5 hours) per week, including postural control during task performance, inhibition of uneconomic and therefore ineffective synergistic movements and facilitation of economic movements to relearn efficient movement strategies for functional task performance. In addition, participants received general activation in a group setting for 5 hours per week and, depending on their motor skills, either 3 hours of garden group or wood-workshop group or 2 hours of fine motor dexterity group. If required, patients were instructed or assisted while washing and grooming in the morning and while eating with the affected hand. Total treatment time was 15–20 hours per week.
In the constraint induced therapy individual physiotherapy and occupational therapy were each performed for 2.5 hours per week, focusing on constraint training. The 5 hours of group therapy consisted of specific arm and hand function training with individual task-oriented exercises. To enable patients with minimal function to perform their task-oriented exercises, adaptations such as hand fixation with a bandage to the object, use of magnets or hooks attached to objects to imitate grasping activities while enhancing shoulder and elbow movements, or choice of positions requiring less strain against gravity were used. Participants trained their arm and hand function while washing, grooming and eating with assistance. In addition to the same total of 15–20 hours per week, the constraint induced therapy group performed 5 hours of self-training (30 minutes after every physiotherapy and occupational therapy session), continuing their repetitive task-oriented training. During the therapies participants wore a constraining mitt, and they were also encouraged to wear it outside the sessions depending on their functional skills.
Therapeutic climbing consisted of the same treatment protocol and the same amount of therapies as the conventional neurological therapy group except that at least 80% of the individual physiotherapy sessions consisted of climbing-specific exercises performed at the climbing wall inside the clinic. Depending on their motor skills, participants were asked to hold, reach, grasp different sized grips, to lean or push on them or to pin small objects to the wall with either hand, maintaining the position with the other hand. Participants were standing on the floor or, with increased function, climbing horizontally or vertically on the wall.
At baseline, the severity of the stroke was assessed by the European Stroke Scale, 18 and ADL by the Extended Barthel Index. 19 – 21 The primary endpoint was arm and hand function, assessed using the Wolf Motor Function Test and the Motor Activity Log at baseline, at discharge, and at six months follow-up. The Wolf Motor Function Test is a 17-item test of arm and hand function and impairment. Its reliability and validity as an outcome measure for patients with hemiparesis has been established. 22 – 25 Time and quality for task completion is measured with 15 items of the Wolf Motor Function Test, while the two remaining items grade strength. The Motor Activity Log is a reliable semi-structured interview concerning the use of the involved arm and hand in 30 ADLs and for satisfaction with arm and hand function.26,27
Secondary outcomes were shoulder pain evaluated by the subscale for shoulder pain of the Chedoke-McMaster Impairment Inventory (ordinal scale from 1 to 7, 1 = constant violent pain in shoulder and arm, 2 = intermittent violent pain in shoulder and arm, 3 = constant pain in shoulder, 4 = intermittent pain in shoulder, 5 = no pain in activities of daily life, but pain during testing, 6 = no pain, but with risk factors, 7 = no pain, no risk factors), 17 active range of motion in shoulder flexion measured in a standing position with a goniometer and isometric strength for shoulder flexion and extension as well as elbow flexion and extension determined with a hand-held dynamometer. 28
We stratified the three treatment groups based on age, time since acute event, and amount of arm and hand function. An independent and blinded research assistant performed concealed randomization using a randomization schedule with blocks of three generated by the primary researcher. The participants could not be blinded to treatment but were unaware of the exact content of the other two alternative treatments. Treating therapists were not involved in the outcome measurements. The same independent and blinded assessor performed all outcome measurements. She had been trained in advance and the results of five test patients did reliably correspond with those of a second assessor.
For statistical analysis we used Anova or Kruskal–Wallis tests as appropriate to detect differences between the groups at baseline and follow-up. To evaluate changes within the treatment groups at the different times of follow-up we used the Wilcoxon signed rank test. Change scores were calculated by subtracting the baseline score from the follow-up scores. To assess change differences between the treatment groups we applied the Mann–Whitney test. Alpha was set at 0.05. Effect sizes were calculated to estimate the magnitude of the observed effects and were according to Cohen defined as small (0.2–0.5), moderate (0.5–0.8) and large (>0.8). 29 Effect sizes for changes within the treatment groups were computed by dividing the mean change score by the pooled standard deviations and for change differences between the treatment groups by dividing the mean difference of the change scores by the pooled standard deviations of the change scores. We used SPSS version 11.5 for statistical analysis.
Results
Baseline characteristics of study subjects
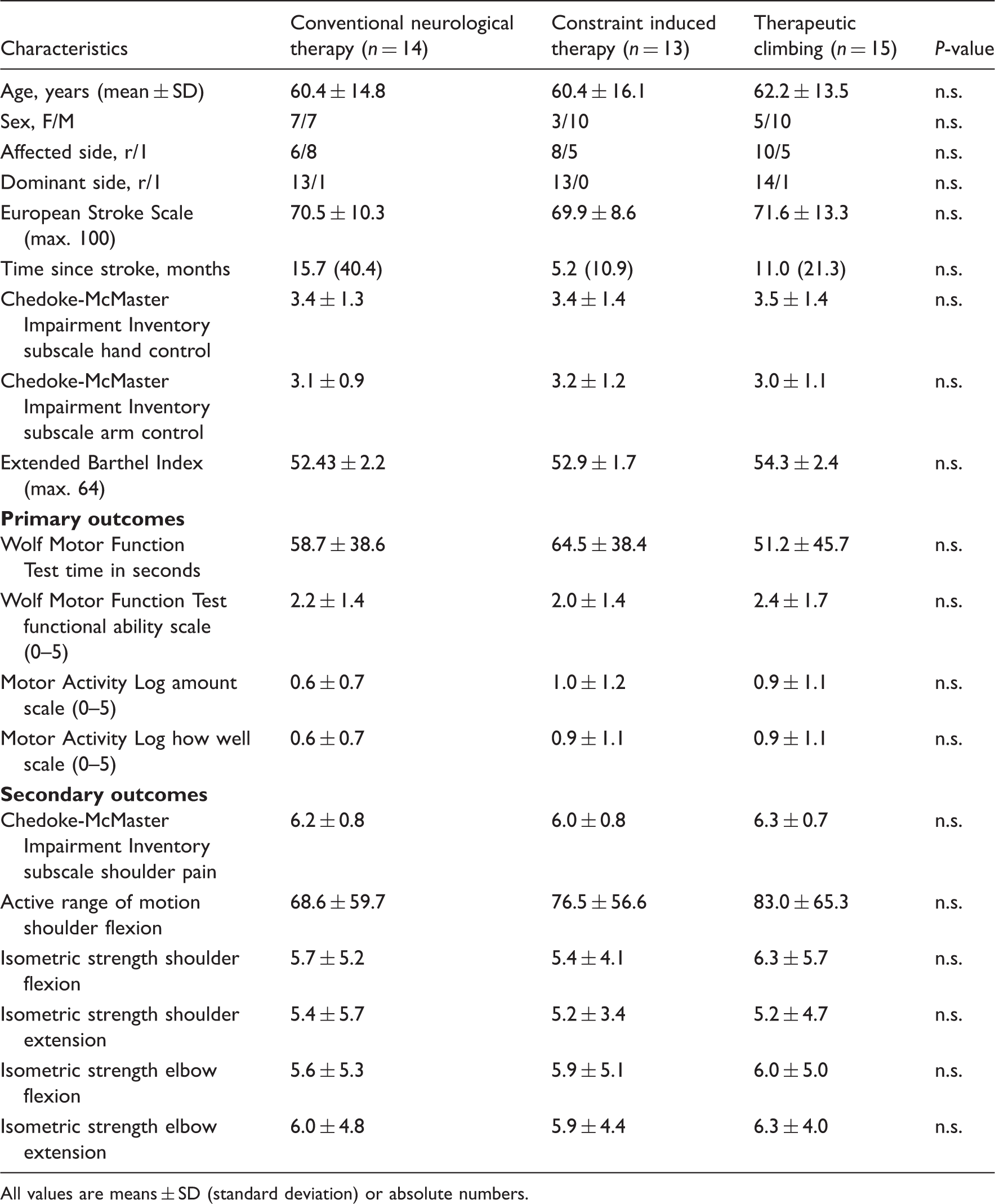
All values are means ± SD (standard deviation) or absolute numbers.
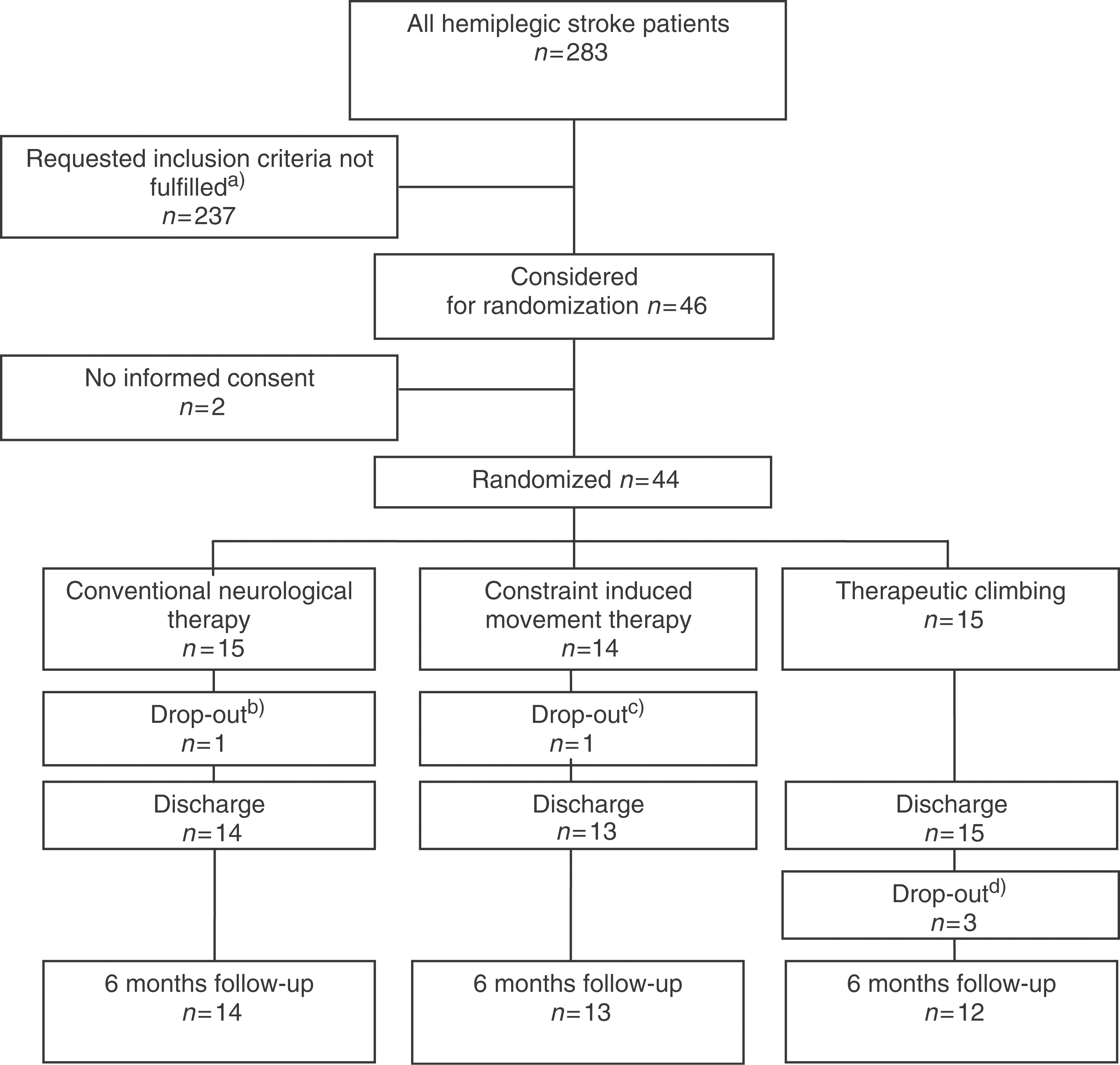
a) One or multiple inclusion criteria were not fulfilled such as: Primary rehabilitation goal was not improvement of arm and hand function but bed-mobility/transfer bed - chair (n=97) and/or standing-balance/walking ability (n=155); better than stage 6 on Chedoke-McMaster Impairment Inventory subscales arm and hand control (n=76); not capable of understanding treatment instructions and providing informed consent due to impaired cognition (n=55) or language (n=56); co-morbidity (n=41). b) 1 patient with complication (thrombosis). c) 1 patient with premature discharge (homesickness). d) 1 patient died, 1 suffered another stroke, 1 refused to turn up.
Improvements of Wolf Motor Function Test, Motor Activity Log and shoulder pain in the three groups
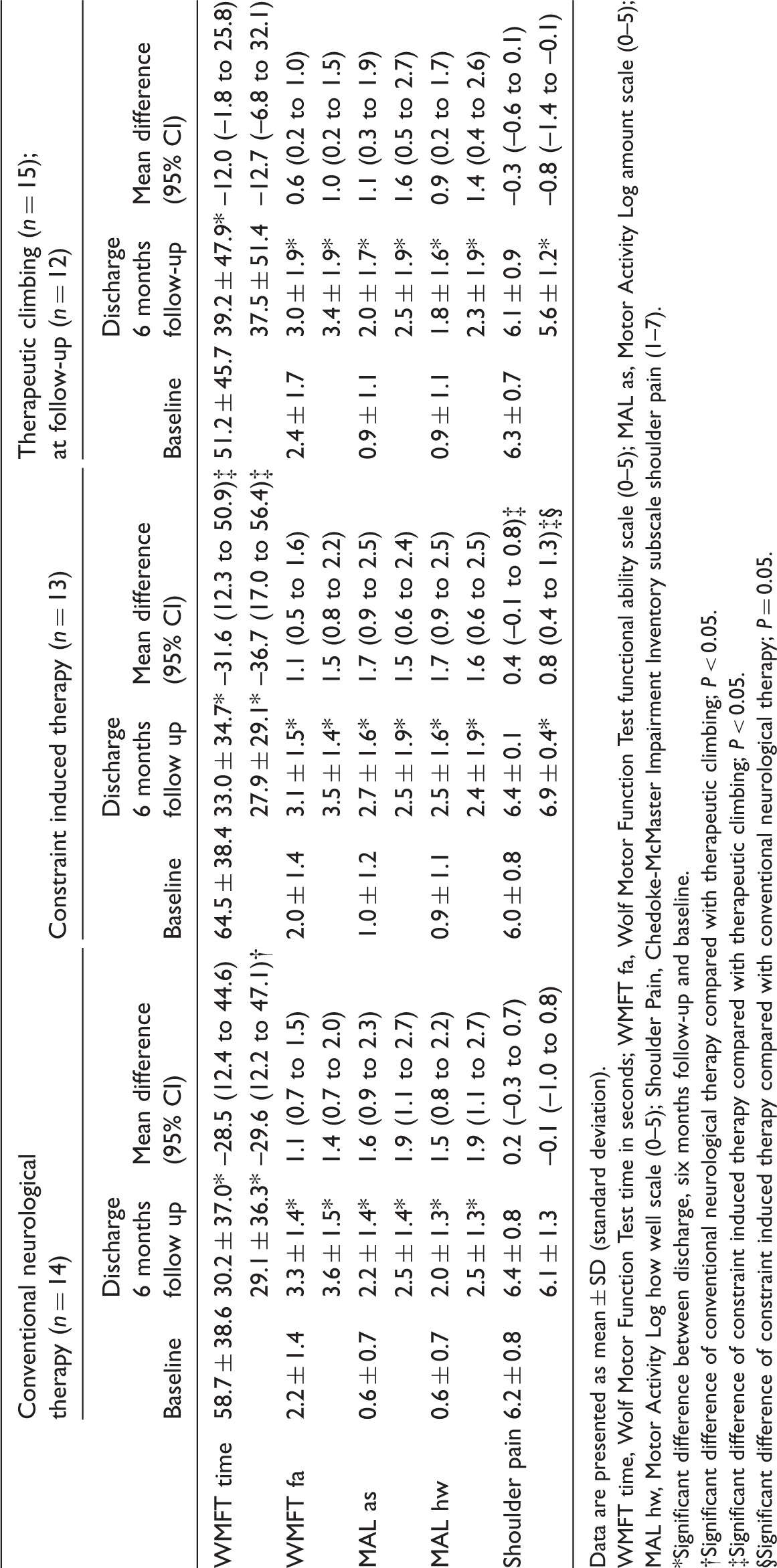
Data are presented as mean ± SD (standard deviation).
WMFT time, Wolf Motor Function Test time in seconds; WMFT fa, Wolf Motor Function Test functional ability scale (0–5); MAL as, Motor Activity Log amount scale (0–5); MAL hw, Motor Activity Log how well scale (0–5); Shoulder Pain, Chedoke-McMaster Impairment Inventory subscale shoulder pain (1–7).
Significant difference between discharge, six months follow-up and baseline.
Significant difference of conventional neurological therapy compared with therapeutic climbing; P < 0.05.
Significant difference of constraint induced therapy compared with therapeutic climbing; P < 0.05.
Significant difference of constraint induced therapy compared with conventional neurological therapy; P = 0.05.
All groups showed significant improvements from entry to discharge in all primary outcome variables, and further improvements in all outcomes at six months follow-up, with the exception of the therapeutic climbing group where the Wolf Motor Function Test time score remained unchanged from discharge to six months follow-up. The secondary outcomes – isometric strength and active range of motion of shoulder flexion – improved in all three groups significantly from entry to discharge and further improved until six months follow-up without significant differences between the groups.
Discussion
In this pilot randomized clinical trial three different treatment approaches focusing on recovery of arm and hand function in stroke patients were evaluated. All patients could be treated according to the protocol and none were lost to follow-up in relation to the response to treatment. Constraint induced therapy and conventional neurological therapy were found to be equivalent in respect of amelioration of arm and hand function in the short and intermediate term, a finding which is consistent with the results of two other dose-matched studies.7,30 Effect sizes in both groups were moderate to large, and the 50% reduction in Wolf Motor Function Test time from entry to discharge can be considered as clinically important.
Therapeutic climbing, in contrast, had a significantly lower impact on arm and hand function, indicating that the constraint and functional-orientated approaches of constraint induced therapy and conventional neurological therapy might be superior in this respect. Therapeutic climbing aims at activating all four extremities as well as the trunk. Within this study, depending on the arm and hand function, the exercises, size, distance and height of the climbing grips were chosen. This was a motivating challenge for patients with some arm and hand function but if there was minimal function only, patients needed major assistance and exercise options were limited to purely concentric and eccentric movements via the arm while holding on to the climbing grip. Everyday life activities, however, require different movement strategies and could not have been exercised in approximately 50% of the climbing therapy patients. This high percentage of patients with minimal arm and hand function resulted from the inclusion criteria and was also true for constraint induced patients. Those with low arm and hand function were able to participate in these therapy sessions but were not able to wear the constraining mitt outside therapies as suggested by the original study by Taub and co-workers. 11 However, the performance of everyday life activities or parts of them were possible during the therapy session as well as in the group therapy. This might, from our point of view, be an explanation for the observed higher impact of constraint induced therapy on arm and hand function.
Another important finding of our study was the decrease of risk factors to develop shoulder pain in the different treatment groups. Shoulder pain is a common secondary problem in patients following stroke, often impeding effective training and limiting treatment effect. 31 At entry, participants of all three treatment groups were free of shoulder pain in ADL but showed risk factors for a possible development of pain such as very low arm and hand control scores (1 or 2 on the Chedoke-McMaster Impairment Inventory subscales arm and hand control), asymmetry of scapula position on trunk or limited passive range of motion of external rotation or flexion/abduction in glenohumeral joint. Constraint induced therapy participants showed a lower risk than therapeutic climbing participants at discharge and at six months, and a lower risk than conventional neurological therapy participants at six months. These results could reflect a better prevention of misuse and an improved stabilization of the shoulder girdle in the constraint induced therapy group.
Even though there was a significant increase in the Motor Activity Log, the strength and range of motion in all groups, we could not find statistical differences between the different treatment groups. This finding supports the hypothesis that strength and range of motion are not the main determinants in functional recovery. Central adaptation and compensatory mechanisms might be more important in this respect. The Motor Activity Log might not be an appropriate measure for stroke patients with minimal arm and hand function.
The major weakness of this study is the small sample size. No final conclusions on the effectiveness of these three treatment approaches can be drawn. The reasons for the small sample size were the very stringent inclusion criteria. Two hundred and 37 out of 283 patients were admitted for rehabilitation to improve general mobility, walking, balance, cognitive and speech skills and were therefore not included in this study. From our point of view these goals are of prime importance in the rehabilitation of patients with stroke, allowing independent living. For ethical reasons we therefore included in this trial only patients who already had some mobility and balance, which allowed us to focus on treatment strategies for the affected arm and hand. We feel also further studies investigating the effect of different treatment approaches on arm and hand function must apply these inclusion criteria. This means that to achieve an adequate sample size for a study investigating treatment strategies for arm and hand function a multi-site trial should be performed.
We recommend further research investigating the effects of constraint induced therapy and conventional neurologic therapy in a larger population of stroke patients with minimal to moderate arm and hand function. We base the required sample size on the results of a recent meta-analysis assessing the efficacy of constraint induced therapy for arm management in hemiparetic patients: The authors report an effect size of 0.64 favouring constraint induced therapy compared with usual care. 14 For the recommended study we assume a moderate effect size of 0.5 and calculate a required sample size of 86 patients per treatment group (power 0.90; alpha 0.05). Based on the experiences generated through therapeutic climbing in this study we recommend further research about its impact only in patients with moderate to good arm and hand function.
Clinical messages
Conventional neurological therapy and constraint induced therapy are feasible and potentially effective treatment approaches to improve minimal to moderate arm and hand function after stroke. Constraint induced therapy seems to have the biggest potential in preventing shoulder pain. Therapeutic climbing might be a treatment option for patients with moderate to good arm and hand function.
Footnotes
Acknowledgements
We would like to thank participating patients and Elisabeth Gamper who performed all assessments.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.