
Abstract
Introduction
About 20–30% of people who have a stroke1,2 experience weakness, in-coordination or paralysis of the muscles required to produce speech. This results in one of a group of motor speech disorders, collectively known as dysarthria. 3 With a rapidly aging population and developments in acute stroke care contributing to increased survival rates, the number of people experiencing stroke and dysarthria is likely to remain high. Together with the global impact of financial restrictions and the increasing need for cost effective use of healthcare resources, effective rehabilitation interventions have never been more essential.
There has been a recent and rapid expansion in the generation of evidence relating to stroke rehabilitation strategies 4 and this expansion has been particularly evident in the field of motor recovery. Evidence is emerging of the link between the characteristics of a rehabilitation activity and its effectiveness in motor recovery. Early, intensive, task specific intervention with an appropriate patient group, undertaking progressively challenging activities is most likely to result in effective motor recovery.5,6,7 A holistic approach to stroke rehabilitation and management is also needed, incorporating both the medical components of the condition and the psychological consequences of stroke.7,8 Such an intervention may also require alternative models of therapy delivery including group-based therapy, self-management approaches or technology-supported therapy.6,7,9
Though this evidence has originated from work relating to upper and lower limb motor recovery there is little indication that this knowledge has been applied to the rehabilitation of other motor-related disorders, such as dysarthria. 10 Two recent surveys of UK speech and language therapists indicated that the use of non-speech oromotor exercises in speech and language therapy is common.11,12 The wide prevalence of these non-speech exercises for the articulators (for example, tongue movements, internal and external to the mouth – side to side; up and down) is unsurprising as the literature to date has focused predominantly on the disease and diagnosis and related symptoms and signs of the disorder. 10
Guidelines for the management of dysarthria reflect the lack of evidence to support interventions with this population group. The most prescriptive 13 recommends educational, physiological, compensatory and augmentative approaches, though most of the evidence was based on a patient group with progressive dysarthria. Others have encouraged a holistic approach to dysarthria rehabilitation 13 but the nature of this approach is unclear. Efforts have been made to begin to develop an understanding of the psychosocial impacts of dysarthria itself. 14 – 16 For example, recent work has highlighted the complex association between the severity of dysarthria experienced by an individual and the impact on their social participation, while the coping strategies participants described may further compound social isolation.14,15
Prior to using a randomized controlled trial to evaluate the effectiveness of interventions designed to address the psychosocial impacts of dysarthria there is a recognized need for a preclinical phase to fully understand the components within, between and surrounding such a complex intervention. 17 It is important to understand how elements of patients’ values, environment, family and home setting potentially moderate outcomes and reactions to the intervention. These developments all point to the necessity of understanding the psychosocial impact(s) of dysarthria not only objectively, but also subjectively from the perspective of the patient and their family. This includes understanding how patients and their carers view dysarthria and its psychosocial consequences, the values they bring to the rehabilitation processes and how their perception of rehabilitation activities may differ from those of health professionals.
Not only is this knowledge of patient and carer approaches to rehabilitation (and what affects these) ethically important but these perspectives are also likely to influence the effectiveness of rehabilitation via the reactions and behaviours of patients and carers during rehabilitation and their subsequent use of health services. 18 In addition, exploration of the management and rehabilitation strategies reported by individuals living with dysarthria is likely to allow identification of activities (or characteristics of activities) that people with dysarthria have found to be beneficial. Such pre-clinical work 17 will inform our understanding of patients’ dysarthria rehabilitation needs and the development of therapist-led and self-management approaches. As part of a larger study investigating the beliefs and experiences of people with dysarthria following stroke,14,15 we explored participants’ perceptions of dysarthria management and rehabilitation.
Methods
Speech and language therapists from 12 clinical settings (community or hospital clinics) across Scotland approached people with stroke-related dysarthria as potential study participants following relevant ethical and administrative approvals. All referred for speech and language therapy over the preceding three years with a diagnosis of dysarthria following stroke were eligible for inclusion. Those with a co-existing diagnosis of dysarthria and a diagnosis of aphasia, cognitive impairment or dyspraxia were excluded.
We adopted a purposive sampling approach to include a range of people with diverse experiences of dysarthria. The participants’ own speech and language therapists provided them with information on the study and its purpose, followed by postage of a consent form and further information. Upon receipt of a signed consent form the research team contacted participants to confirm their interest and then formally screened for the presence of aphasia, 19 a clinically relevant depression score 20 and cognitive impairment. 21 We also recorded additional demographic data on each participant including socio-economic grouping, 22 informal carer status, severity of stroke 23 and age.
We adopted a qualitative research design to explore patients’ views on the management of dysarthria, the components of meaningful rehabilitation, and the types of rehabilitation activities that they perceived to be (or not to be) functionally relevant. In-depth semi-structured interviews were carried out with participants by one of the research team (SD), digitally recorded and then orthographically transcribed by the interviewer. An experienced speech and language therapist, a member of the research team (GP), provided confirmation or clarification as required.
All participants were interviewed in their own home using an interview schedule 14 to guide the interview. We employed a software package (NVivo) to aid organization of the qualitative research analysis, to support the thematic coding and data retrieval in a systematic manner. A constant comparative approach (grounded theory) to analysis of the data was used 24 and an early coding framework was collaboratively reviewed by the research team. Amendments were made to these frameworks in response to the research team’s collaborative reviewing activities and further refined with the continued input of the team. The findings on the psychosocial impacts related to dysarthria have been published elsewhere.14,15 In this paper we report the participants’ perceptions of communication management and rehabilitation activities following stroke-related dysarthria.
Results
A total of 33 individuals returned signed consent forms to the research team. Three participants subsequently withdrew their consent and two participants died. We screened the remaining 28 individuals and while none were excluded because of cognitive or language impairment, three participants were found to have significant depression and were excluded from the study. A total of 25 participants were interviewed but one recording failed. The results presented within this paper relate to data from interviews with 24 people that had experienced stroke-related dysarthria.
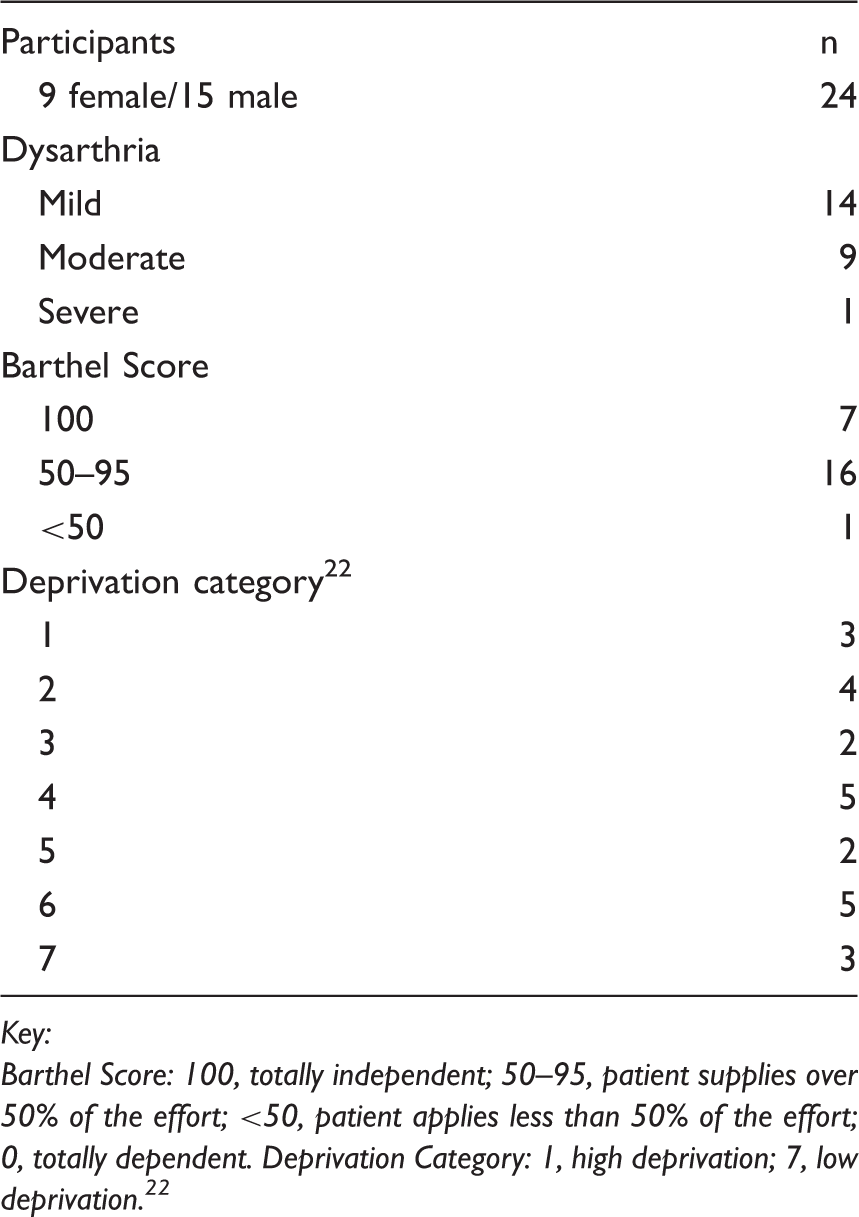
The participants had a mean age of 63.5 (SD 12; range 34–86) years. The severity of participants’ dysarthria was based on an evaluation at the time of recruitment by one of the research team (GP) and ranged from mild (n = 14), moderate (n = 9) and severe (n = 1). Participants came from a wide range of socio-economic backgrounds
22
and stroke severity (Table 1). We report below the themes arising from the semi-structured interviews as they relate to the participants’ perception of the management and rehabilitation of their dysarthria following a stroke. These are presented within the over arching themes of Maximizing Communication and Rehabilitation. A diagrammatic overview is presented in Figure 1.
Overview of main themes and findings. Participants
Key:
Barthel Score: 100, totally independent; 50–95, patient supplies over 50% of the effort; <50, patient applies less than 50% of the effort; 0, totally dependent. Deprivation Category: 1, high deprivation; 7, low deprivation.
22
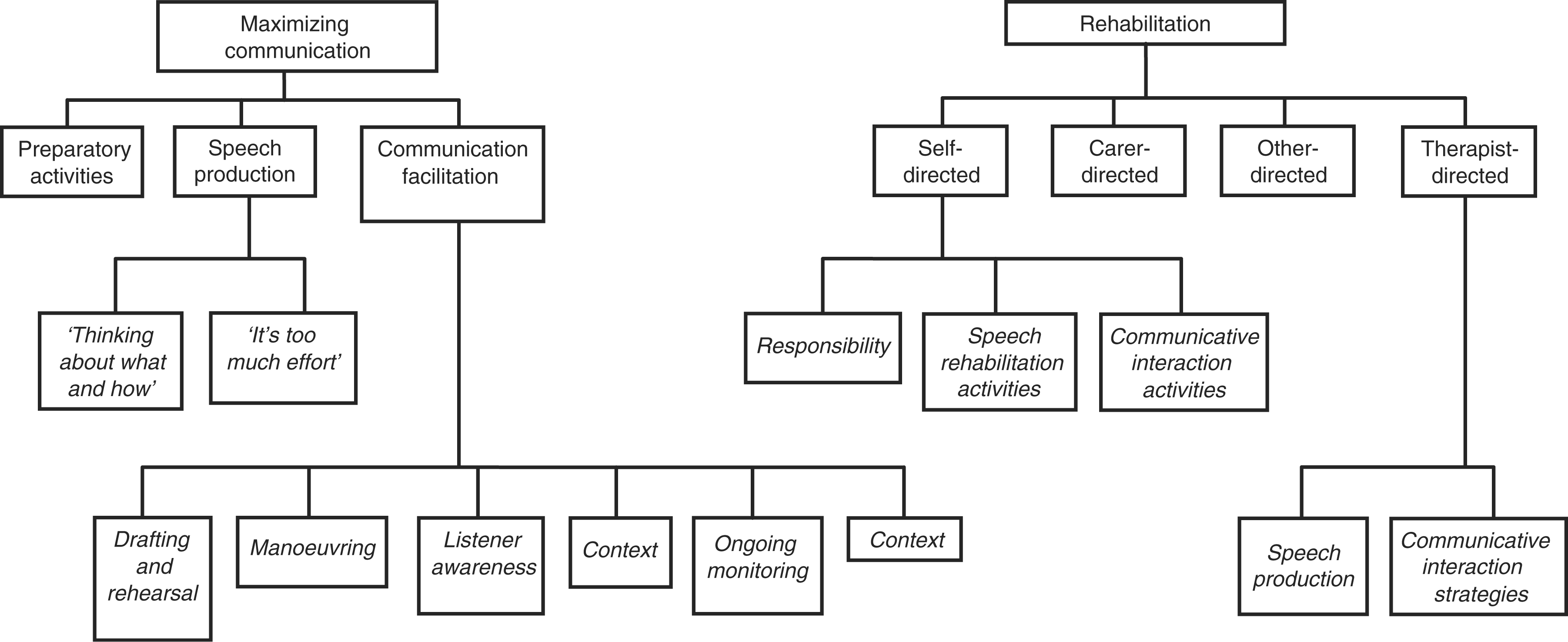
Maximizing communication
Participants described an extensive range of communication strategies they used to maximize the quality of their speech production and their communicative interactions. We report the participants’ perception of the worth of the strategies in improving their communicative success, in particular – preparatory activities, speech production activities and strategies to facilitate the communicative interaction.
Preparatory activities
Participants described a number of strategies they employed in preparation for speaking. Some were inconspicuous, cognitive strategies that might go unobserved by others, such as ‘taking precautions’ and conserving their capacity to communicate.
‘I think before I open my mouth. I think about what I’m going to say. I won’t do it as spontaneously as much as I used to … not because of what I’m going to say. It’s just how I want to say it. You know just make sure it comes out ok.’ Gender (M): Severity (Mild) – Time since onset of dysarthria (5 mths)
‘I still have to think and form the words and sometimes think of a replacement word for something.’ F: Mild – 4 mths
Other participants described a need to stay active but within the confines of their personal energy limitations. These people described pacing their communication and conceptualized their capacity for successful communication as a ‘vocal battery’. Some felt a period of time spent not conversing then left them with more reserves to participate in communication more effectively when required. Conversely, others felt that a period of non-communication had a detrimental effect on their speech.
‘I think the longer you can go without speaking helps you the next day …. Because you kind of charge up your vocal battery and then you can talk, talk, talk.’ M: Mild – 5 mths
‘I can sit here all day myself and never speak to anybody and the result is that when I go to speak to anybody it doesn’t come out.’ F: Moderate – 12 mths
Speech production
Participants also described strategies to maximize the quality of their speech. Again, activities could be divided into those that might be observed by others and those that occurred internally. Conspicuous strategies included aspects of articulation (e.g. ‘slow down’, ‘speak clearly’, ‘speak slower and politer’) and vocal projection (e.g. ‘shout louder’). Inconspicuous activities included extreme care in articulator placement, internalized rehearsal and effortful cognitive activities. Further description and examples of these are given below.
Thinking about what and how
Internalized strategies primarily seemed to relate to a heightened consciousness relating to the placement of articulators, an automatic process for most speakers.
‘It’s always taking care, placing your tongue so that the words come out as near to what they should be as I can achieve.’ F: Mild – 4 mths
Other participants described monitoring the quality of their intonation and prosody. As a consequence of dysarthria, speech at times lacked intonation and the resultant expressionless speech adversely impacted upon the interpretation of what was said. For example, one participant described the need to plan her interactions with this in mind.
‘Then you would say, “I’ve just upset her now because actually I didn’t mean to say that. I wanted to say it more softly or more caring” …. you still have to think about how you are going to approach the subject and what you are going to say so you are not offending her.’ F: Mild – 23 mths
‘I think about what I am saying and how I am saying it. Which, I always thought about what I was saying but I didn’t need to think about how I (was) saying it.’ F: Mild – 8 mths
Another participant described an extension of this process into an internalized rehearsal activity where the communication would be planned and reviewed before it was said aloud.
‘I’ve got to think about it [what I’m saying] and then I’ve got to say it to my head before I can say it out.’ M: Mild – 9 mths
Though such adjustments to speech production resulted in improved speech quality, participants did not always welcome the need to consciously undertake such activities, nor the characteristics of the resulting speech. Slow speech was identified as a stigmatizing marker, drawing comparisons with intellectual ability and a child learning to speak. Participants tried to balance the need to speak slowly to ensure quality but at an acceptable pace of speech.
‘I don’t like speaking as slow as this. It’s terrible. It’s just like a wee baby learning to speak all over again.’ M: Mild – 4 mths
‘If I spoke really slowly and tried to pronounce the words properly I could probably speak better but I don’t want to speak so slowly. I want to speak.’ M: Mild – 4 mths
It’s too much of an effort
In addition, many participants described focused, effortful concentration when producing speech. Participants described focusing on the placement of articulators, producing the sounds, intonation, breath support but also included reducing external distractions and altering their initial choice of words (or restructuring of utterances) to maximize their speech production abilities. If some sounds or words were perceived as troublesome the word was avoided or substituted. Such cognitive strategies are internalized, extremely effortful and drain the individual’s energy, which in turn hinders their spontaneity and enjoyment of communicative interactions.
‘Even thinking on another word to say is part of the therapy … not to use a combination of words. I’ve learned to do that …. It’s a nuisance at the beginning because you like to use your own language that you’re used to, but now I do it (a) thoughtfully and (b) more often without getting annoyed.’ F: Mild – 8 mths
‘I
Interestingly, this participant spoke about these preparatory activities in the past (see bold), reflecting that these strategies were no longer regularly employed.
Communication facilitation
Other strategies described by the participants related to their efforts to maximize or preserve the quality of communicative interactions with others. These included descriptions of drafting and rehearsal, manoeuvring, listener awareness, confidence, context, ongoing monitoring and conversational repair activities.
Drafting and rehearsal
Some strategies to maximize the effectiveness of communicative interactions were implemented long before the actual interaction occurred. These strategies related to planned, well defined communication activities, such as making a telephone call or delivering a report at a meeting. For such predictable structured communication situations participants described drafting and rehearsal of what they wanted to say.
‘… a meeting and if I’ve got something to say I’ll write it down on my minutes.’ M: Mild - 9 mths
Manoeuvring
Participants described other preparatory activities that occurred more immediate to the communicative interaction including descriptions of non-verbal ‘manoeuvring’ into position before they began to speak or ensuring the listener knows they intend to speak (for example, by raising a hand) and so the listeners are ready to listen.
‘You manoeuvre yourself ready to talk. Well I do. They know when I’m wanting to speak so then they listen.’ M: Mild – 5 mths
Not all participants were as successful in ensuring that they had an opportunity to contribute, which had significant consequences for their participation.
‘I’m not quick at getting my answer in and I just don’t bother then.’ F: Moderate – 10 mths
Listener awareness
There was an interesting dichotomy between participants’ perception of the impact unfamiliar listeners’ awareness of their dysarthria had on their communication. Some described the benefits of taking time to explain to the listener their circumstances and the nature of their dysarthria. In contrast, others clearly expressed a preference for interactions where their dysarthria was not acknowledged.
‘As soon as I explain my situation I felt better inside and my speech got better.’ F: Mild – 23 mths
‘I was in Boots and this lady came over and said “I’m looking at your scooter”…. I explained all about the scooter and there was no slurred speech. I don’t know why. I think if people don’t know, as I said, I’m fine.’ F: Moderate – 7 mths
In many cases, the impact listener awareness had on the individual’s speech appeared to be linked to participants’ self-confidence. For some, their self-confidence increased if the listener was fully aware while for others the opposite was true.
Context
Participants reported considering the context of a potential or planned communicative interaction and how it might impact on their ability to communicate. Factors considered included whether they were undertaking simultaneous physical activity (e.g. walking), ambient temperature, fatigue, the number of speakers, stress and anxiety. One participant in particular described reviewing the context of potential communicative interactions in detail and the likely impact each context might have on her ability to communicate. In order to maximize her ability to communicate successfully she chose to limit her engagement within conversations in certain situations (for example, on a cold morning when she felt her speech muscles would stiffen up), while in other situations she demanded an improved interaction context (by asking her husband to move into the same room when speaking to her).
‘I’m aware how my speech is affected in different situations now and that helps me. Like going up to school in the morning, if it is nippy outside I know my face will seize up and I know “Don’t get into a big conversation”. If I’m tired, “Don’t speak to me, I am going to my bed”.’
‘I was standing ironing last night and I was in the living room and Andy [husband] was in the kitchen and he was shouting through to me something … I was trying to shout back through to him. I thought, “Why am I doing this?”… I said “I am not speaking to you unless you come through”.’ F: Mild – 23 mths
Ongoing monitoring
Most individuals within a communicative interaction monitor their contribution and the degree to which they are successful in delivering the information in their conversation to the listener. Such ongoing monitoring typically occurs at a subconscious level for most participants within an interaction, only becoming apparent to observers when a breakdown in communication occurs. For people with dysarthria the ability to monitor their own speech is vital, not just to become a successful communicator but it is an essential prerequisite for the effective management and rehabilitation. Many of the participants reported problems with their monitoring abilities, especially in the early stages following their stroke. For some, it seemed to continue to be a challenge while for others their ongoing monitoring became highly acute and identified flaws that most listeners would not.
‘I mean, I thought I was doing alright, but people kept saying, “(Pardon?) What did you say?” It was all quite mixed up.’ M: Moderate – 5 mths
‘They [friends] say “What did you say?” and I get angry. I say “Could you not have listened to me the first time and I wouldn’t need to say it again?”.’ F: Moderate – 10 mths
‘I hear my flaws. People don’t but I do.’ F: Mild – 23 mths
Many participants in this study described a constant state of heightened communication monitoring when speaking with others, continually scrutinizing the quality of their own speech and requesting confirmation of listeners’ understanding. Many spoke of immediate self-initiated adjustments (or repairs) to their conversational contribution when they identified (which, by description, appeared to be mildly) problematic speech.
‘If I think that that word or sentence is not understandable then I’ll repeat myself without being asked. Because if I feel it was wrong or if I feel it was slurred or slower, I would repeat myself.’ F: Mild – 23 mths
‘Usually that would be the first thing I would ask them, “Can you?”, “Aye, I can make you out. Carry on”.’ M: Moderate – 6 mths
Repairing a breakdown in conversation
Where conversational interactions did breakdown, participants spoke about the need for determined persistence to repair the interaction. They described a range of strategies for stalling while they put repair strategies in place including – perseverance, trying your best, staying calm and relaxed. One participant employed a novel visual distraction technique while he went about repairing the communication breakdown.
‘[I] wave my arms about. Distract them while I’m thinking.’ M: Mild – 9 mths
Conversational repair techniques varied from repetition, alteration, substitution, writing it down, using alphabet charts to cue the listener into the word, using ‘sounds like’ activities and pointing.
‘I just say it again. Then change it round afterwards.’ M: Moderate – 34 mths
Some participants described a staged approach to their communication. First attempts at communication were based on speech alone. If that failed, then supportive techniques were employed such as writing it down or using an alphabet board (homemade or as provide by the therapist) to give the listener the first letter.
‘I speak and if they don’t understand I use this [augmentative communication device – an alphabet board].’ F: Severe – 8 mths
Others described pausing before responding to queries, thus letting other family members respond first, which gave the individual with dysarthria more time to prepare for and formulate a response if required.
‘I would have waited until he [husband] said and he’s not backwards at coming forwards.’ F: Mild – 8 mths
Speech rehabilitation
Most participants were clear that their recovery from dysarthria was an ongoing process, and described a surprising number and range of rehabilitation strategies employed by themselves, their carers, their therapists and others to this end. We present these below as self-directed, carer-directed, other-directed and therapist-directed rehabilitation activities.
Self-directed rehabilitation
Participants described a clear sense of responsibility for their own rehabilitation. In some cases this appeared to be because of necessity. In others, it appeared to have resulted from transference of this responsibility from the clinician. The participants that placed themselves upon a path of continuing recovery perceived motivation as highly important and they described a range of self-directed speech rehabilitation activities – rehabilitation activities designed to improve speech production and (a lesser number of) activities designed to encourage participation within a communicative interaction.
Responsibility
Many of the participants expressed a clear sense of responsibility for their own rehabilitation. Even when the formal rehabilitation was led by others, participants still expressed the importance of investing in that process.
‘… I am very happy with the treatment I got for my speech, very happy with it …. but I think an awful lot has to come from yourself. …. I don’t know how you begin to educate the general public that they need to put something in.’ F: Mild – 8 mths
‘… they [other patients] don’t want help. I mean I was shocked with people not taking things away. “Is that you with your homework?” – they were kidding me on. If they wouldn’t do it for themselves who was going to do it? In one conversation I said, “It’s no good going there one or maybe even twice a week and doing nothing at home. Not trying yourself”.’ F: Mild – 8 mths
In one case, a participant was wholly reliant on their own initiative to secure access to rehabilitation services.
‘… in all took about six months before I got organized. And it’s been a case of me going down to the doctors and saying “I want a stroke physio”. It was into June before I got it, because Hazel [SLT] kept saying “Why have you not been here before?”.’ F: Moderate – 7mths
For other participants responsibility for the rehabilitation process had been placed in their domain from the start, was transferred to them during rehabilitation or they assumed responsibility as their rehabilitation progressed.
‘I went to the therapist and they said they could only do so much, the rest was up to me.’ M: Mild – 5 mths
‘I think again praise for the speech therapist ‘cause she made me realise why it had happened, how it had happened and there was so much I could do to make it better.’ F: Mild – 4 mths
‘Well, at first she gave me words, but now I’ve got my own wee words and we have a chat. I think she [speech and language therapist] can see how I’m getting on.’ F: Moderate – 7 mths
For others, self-directed rehabilitation was seen as the only remaining option to achieve their rehabilitation goals following the cessation of professional rehabilitation input.
‘She [speech and language therapist] said “You’re talking fine”, so I’ve just to get on with it.’ F: Moderate – 10 mths
‘She [speech and language therapist] says that I’ve just to keep practising my vowels and look after myself.’ M: Mild – 9 mths
Motivation
The participants’ strong sense of responsibility for their own rehabilitation occurred in conjunction with descriptions of high motivation, an aspect known to impact upon outcomes and professionals’ interaction with patients.
‘Because I’m working for myself I was pushing myself more. When working for an employer most people would take the attitude that well, my wages are getting paid. There’s no reason to rush back, you know. Whereas I’ve got to earn money and I’ve got to learn to speak.’ M: Mild – 9 mths
‘… you are the main person to try and force yourself to talk and laugh and cry and manoeuvre your mouth and it’s amazing what you can do.’ M: Mild – 5 mths
Speech rehabilitation activities
The range of speech production rehabilitation activities participants actively engaged in was wide and varied. Many described reading-aloud activities (paper, books, TV listings, road signs and questions in board games e.g. Trivial Pursuit) or speaking-aloud activities (word games). These were seen as purposeful and functional activities. In addition, some described using this activity to support additional rehabilitation activities such as using the task to generate a list of problematic words for further repetitive practice throughout the day. Several reported how helpful it had been to record their speech, listening back to it for additional feedback or for comparison over the post-stroke period.
‘Oh, I have my little routine in the morning, reading out the paper and I write down the words that are bad. And as the day goes on I have a wee read at my words and they improve as the day goes on. But the next day there’s another set of words ((laughs)).’ F: Moderate – 7 mths
‘I use the tape recorder (?). I’ll read a chapter of a book and listen to it.’ M: Moderate – 15 mths
‘As we go along I read the road signs.’ F: Moderate – 7 mths
Other speech production activities included conducting therapist-directed exercises, singing, relaxation, rehearsal of automatic speech (alphabet, counting) aloud and internalized speaking.
‘Singing to yourself “doe a deer, a female deer” or whatever. And go through that in your mind and try and form the words as you’re saying it and then try and say it. You know, something simple like that. Try and go through the alphabet anyway at all, try and count up to nine, ten and then repeat it backwards.’ M: Mild – 5 mths
‘I speak to myself in here. The nurses said that was a good way. Don’t just think to yourself, speak to yourself … So I do that. I speak out loud sometimes you know.’ M: Mild – 5 mths
Only one participant (with a young family) described a lack of opportunity to engage with such exercises on a regular basis. More generally, participants were able to undertake speech rehabilitation activities on a frequent basis throughout the day.
‘I’m not doing anything in any case. I could sit and do those things (speech exercises) ten times a day’ M; Mild – 4 mths
Communicative interaction activities
Some participants spoke about the importance of getting more involved in communicative interactions with the aim of building their confidence, practising and improving their speech.
‘The more I talk the more I get better.’ M: Mild – 9 mths
‘Mix with people rather than stay at the back.’ M: Moderate – 6 mths
Though some participants saw these activities as beneficial, they also described the need for courage in order to engage in communication following their stroke.
‘I try and get myself out and go out and face it, because I don’t want to be stuck in the house all the time.’ F: Mild – 3 mths
‘No, no right from the beginning I knew there were certain things that just had to be done or I had to face them, like answering the door.’ F: Mild – 4 mths
Carer-generated rehabilitation strategies
Participants recounted the strategies their carers employed to support their speech recovery and rehabilitation. As well as providing general support and encouragement, carers had a crucial role in supporting individuals’ communication success. Participants described communication with their carer as ‘easier’ as they were generally ‘quick’ to understand the meaning they were trying to communicate. For some participants, better communication with their carer was simply related to the fact they ‘just usually sat closer’ (M: Mild – 5 mths) meaning there was less need to project their voice. In many other cases, however, ease of communication related to a shared understanding of thoughts, preferences and circumstances.
‘He knew by one or two words what I wanted to say.’ F: Mild – 23 mths
As a result, particularly in the early stages following stroke, carers often became a surrogate communicator, communicating with others on behalf of the individual with dysarthria. Some participants, however, described a more prolonged reliance on surrogate communicators, particularly in situations where confidence in their speech was lacking.
‘(She) [Wife] deciphers for me.’ M: Moderate – 34 mths
‘I wouldn’t answer the phone for ages. I kept going “No. You get it. You get it”.’ F: Mild – 8 mths
Others described how reliance on a surrogate communicator was prone to change over time following their stroke. In some cases, supportive roles in place in the early stages following stroke persisted despite an individual’s improving speech and confidence. Some participants described a carer’s over-compensation for their improved speech abilities resulting in their frustration and (in one case) therapist intervention. In other cases the change in communication support was perceived by the participant to be the result of the carer’s gradual withdrawal from this role.
‘I said “But, no, I don’t, I don’t want to answer the phones. I’d rather be physically working and just keep me in the background”. I said “But you answer the phones”, you know, “You do all that stuff”. And then eventually, he kind of swung me into, “Can you get that phone Dad? I’m busy. Can you get that phone?”.’ M: Mild – 9 mths
Participants also described carers’ strategies to encourage the production of high-quality speech – encouraging reading aloud, providing immediate feedback, stepping into the therapist’s role or providing support and encouragement in social interactions, both with themselves and with others in their wider social circle.
‘He [husband] says “Slow down and tell me right”.’ F: Moderate – 10 mths
‘They [speech and language therapists] gave me some sheets with words that I had to pronounce and Ann [spouse] will hold the sheet and says the words the way the speech therapist would do it.’ M: Moderate – 5 mths
‘… between Amy [wife] taking me out as much and meeting people, you know. And having my son there as well to fall back on should I not feel comfortable.’ M: Mild – 9 mths
Many of these carer-led rehabilitation strategies were generally perceived as helpful by the individuals with dysarthria. However, for some, such strategies were at times problematic. One participant described difficulty holding prolonged conversations with his wife of 50 years while another found the manner in which her partner provided feedback on her speech actually inhibited her communication.
‘I was speaking to him [husband], I mean he was unaware he was doing it. He went, “Eh”, “What you saying?”, “Eh” …… he was finishing my sentences for me.’ F: Mild – 23 mths
Other-directed rehabilitation strategies
Participants also depicted the activities and strategies others in their communication networks (including other family members, formal caregivers, friends and other healthcare staff) used to support their rehabilitation. Other-directed rehabilitation strategies described were aimed at improving the individual’s speech production and participation in communicative interactions. Strategies to improve speech production included requests to slow down their speech or repeat what was said, as well as providing practice materials (books), encouragement, advice and feedback. One general practitioner suggested they sing to improve their speech.
‘The nurses said “Don’t think to yourself, talk as if you are talking to somebody”.’ M: Mild – 5 mths
‘As a matter of fact, my friend(s), when I do speak and they see that I’m getting, the voice is going away, they’ll say “Now, take your time Mary”.’ F: Moderate – 12 mths
‘The doctor said to me to sing it. If you sing it, it doesn’t sound very good but that seems to help a wee bit.’ F: Moderate – 7 mths
Participants described how friends encouraged their participation in conversations and facilitated their inclusion in other communicative interactions. In one case, the participant noted that her sister appeared to deliberately slow her own speech in order to assist her in slowing hers. In contrast, participants also reported exclusion from conversations with speakers addressing others present rather than them. Participants were clear that people should engage in conversation with people who have dysarthria thus stimulating their speech, but in a manner which respects their dignity and acknowledges their cognitive capacities.
‘That’s one of the things that I would train people to do. I don’t mean speech therapists and people like that, I’m talking about the ordinary staff in a hospital, you know, the nurses, cleaner, whatever, not to speak to people as if …. take it for granted that they are speaking to someone of intelligence.’ F: Mild – 4 mths
Some people described friends, family members or other healthcare staff supporting their speech rehabilitation activities by practising speech exercises or providing encouragement and motivation. Though there were also examples of a lack of understanding about dysarthria from others in their social network.
‘I started calling it [caravan] a mobile home until my great-granddaughter said I’m not talking to you again until you can say caravan. So I had to keep practicing you know.’ F: Mild – 4 mths
‘… she’s [professional carer] at the other end of the table and … I answered her. I thingymed my speech, raised my voice. She said “Why are you roaring at me?”.’ F: Moderate – 12 mths
Therapist-directed rehabilitation strategies
The speech and language therapist was clearly identified by participants as the main professional supporting their speech recovery. Participants’ perceptions of speech and language therapist-directed interventions were focused mainly around the recovery of speech (speech production strategies and exercises) and strategies to maximize the quality of communicative interactions, but which also extended to one of support and encouragement.
Speech production strategies
Participants recalled therapists’ advice on speech production strategies which could be grouped as relating to respiration, articulation, prosody and resonance as well as general advice on staying relaxed and strategies for planning ahead what they wanted to say.
‘She tells me to take plenty of breaths and keep calm and then just start saying the thing.’ F: Moderate – 10 mths
‘Jane [SLT] had said that “Background noise is something that you are going to have to learn to speak over. You’re going to have to have a loud voice. Use your projection”.’ F: Mild – 8 mths
‘I try to practise what I was taught. Keep thinking what I’m going to say before I say it. Just try and make it clear as possible.’ M: Mild – 5 mths
Participants spent a lot of time describing therapist-directed speech production activities. The use of tape recorders to provide objective feedback on the current status of the quality of their speech was welcomed by the participants. To a large extent, however, participants’ descriptions of therapist-directed rehabilitation strategies focused on exercises to improve their speech production.
The speech exercises described seemed to target articulator movement (oromotor movements, mirror-based practice), sounds, words or sentence production sheets of increasing difficulty or sequences that were challenging to produce (as one participant described ‘tongue teasers’). Participants were expected to practise these repetitively while in hospital or at home.
‘… there was facial ‘o’s and ‘a’s that I had to do. I was given big A4 sheets with small sentences initially and then they progressed onto longer sentences and longer words.’ M: Mild – 9 mths
Many participants expressed a keen interest and opportunity to undertake rehabilitation activities, however, the links between such exercises, functional relevance and speech recovery were not always clear to them.
‘Maybe if I keep on going over these words incessantly maybe it will help me. I can’t be bothered saying the words incessantly. But, maybe I should, because maybe it will help’. M: Mild – 4 mths
Some participants described the exercises as ‘ridiculous’ or ‘daft’, while others felt this way while doing these activities. Some reported adherence to these therapy tasks but quickly lost interest once they no longer challenged their speech abilities.
‘… but latterly I’ve got that I can’t be bothered going over all these words because I could go over them all without any problems.’ M: Mild – 4 mths
Adherence to the exercises was more readily described in the context of continually challenging speech production targets. Overall, there was a general lack of engagement with these rehabilitation tasks which was expressed in terms of embarrassment, boredom, indifference or humour. Some participants compared the tasks to child-like activities, perceiving them as humiliating and stigmatizing.
‘I did say them continuously. The last wee while I’ve just got browned off saying them. … Sitting on the couch saying “eeeeeee” and I think to myself I’m a bloody numpty ((laughs)).’ M: Mild – 4 mths
‘She gave me loads of words and once or twice … then I just threw it away.’ M: Moderate – 6 mths
‘I mean as tongue teasers to go through … And I was bursting out laughing because I couldn’t hold it in. And I was bringing them all home and I was saying to Margaret “Right. Listen to this”, you know, “Peter picked …”. And she was laughing and I was laughing. It was good fun. [Cough] I knew within myself that my speech was going to come back without the tongue twisters.’ M: Mild – 5 mths
‘ ‘How now brown cow’ it started with. Learning my ABCs and then going on to my vowels and learning ‘A’ ‘E’ ‘O’. Then we went on to wee fairytale stories …’ M: Mild – 9 mths
Communicative interaction strategies
Some participants recalled advice relating to communication interaction strategies including discussions about, what communication was and the roles and responsibilities of participants in a communicative interaction. Therapists were also recalled to have advocated careful preparation of predicable communicative interactions (e.g. telephone calls) and signalling when they wanted to participate within a conversation was also recommended (such as raising a hand to indicate they wanted to contribute to the conversation).
‘And we [speech and language therapist and participant] talked about communication and … if the hearer can’t understand you it’s your communication that’s at fault.’ F: Mild – 8 mths
‘If you’re in company and you want to speak put your hand up and let them know.’ M: Mild – 5 mths
Some participants felt the application of recommended strategies within a communicative situation was impractical and in such cases they were not employed.
‘See the speech therapist said “You should relax. Take your time. Breathe deeply” but when you get asked a question you’ve not got time to sit, relax and breathe deeply. You’ve got to answer the question. So that’s it.’ M: Mild – 5 mths
Therapists were also seen as having a role in encouraging the carer to adopt helpful strategies to facilitate communicative support for the individual with dysarthria, while discouraging unhelpful strategies.
‘It was along the lines of, “You can’t patronise her. Listen to what she’s saying and ask her again. No [not] “Eh?” “Eh?”, “What are you saying?” kind of attitude”.’ F: Mild – 23 mths
Discussion
Our findings provide new insights into the substantial, often internalized, inconspicuous efforts people with dysarthria go through to maximize their communicative effectiveness. While the auditory perception of speech may be considered within normal parameters, this does not necessarily reflect the effort the individual has invested in order to produce speech of that quality, any changes from their pre-stroke speech quality, nor the individuals’ perception of their own speech quality. Participants in this study also described a considerable number of strategies they employed to maximize their communicative effectiveness both before and within interactions.
We have also reported the participants’ perception of rehabilitation activities. Responsibility and motivation were important qualities shared by most participants. Self-led speech rehabilitation activities were functionally based and undertaken on a regular basis. A range of novel approaches, which they reported as beneficial, were described.
We found little indication of differences in the management and rehabilitation strategies employed by males and females with dysarthria nor between participants from different deprivation categories. Some participants described changes over time after the onset of their dysarthria, particularly in their ability to monitor the quality of their speech or the acceptance of carer support. In other cases, time since stroke seemed to bear little relationship to recovery.
Generally, participants described undertaking formal therapist-led speech exercises which were perceived by some as stigmatizing, of questionable functional relevance and which quickly became unchallenging. In contrast, advice on improving the quality of their speech (e.g. breath support, projection, intonation) and management of communication situations (e.g. internalized planning) was found to be very useful.
Few studies have explored the rehabilitation and management issues people with dysarthria experience, though many therapists will have anecdotal experience of these themes from the clinical setting. Many of the perceptions expressed by the participants could not have been anticipated prior to this study which has resulted in a remarkably rich dataset that contains much guidance for those working with people with dysarthria following a stroke. Although this was a small study of 24 participants, many of the issues raised in this study may also have relevance to other patient populations with acquired dysarthria, such as people with Parkinson’s disease or multiple sclerosis.
Disappointingly, we only had a single participant with severe dysarthria remain in the study following screening for depression, which limits the insight we have into the perceptions of this group on management and rehabilitation of severe dysarthria. It would be of interest to explore whether the issues raised in this study also reflect the perceptions and experiences of individuals with more severe dysarthria at a later point. Similarly, our ratings of dysarthria severity were specific to the point of study recruitment and so it is possible that some participants had experienced more severe forms of dysarthria immediately post-stroke. However, the ratings of severity were provided here as a clinical reference for the reader. As we have seen from this, and our previous reports,14,15 intelligibility ratings may bear little relationship to the impact of dysarthria as experienced by the individual.
Similarly, our deliberate approach of focusing upon issues specific to dysarthria meant that we excluded people with co-existing disorders, such as aphasia, apraxia, cognitive impairment and depression. Developing a greater insight into the experiences of people with these co-existing difficulties would further inform the therapeutic management of these individuals. As our efforts to recruit carers were only partially successful, 14 we were prevented from developing a better understanding of carers’ perceptions of the management and rehabilitation strategies following stroke-related dysarthria. Similarly, as the data presented relate to the descriptions of the individual with dysarthria it was not always possible to specifically identify whether strategies described originated from the insight of the individual themselves or as a result of therapeutic intervention.
Our findings in this paper resonate with those identified in a study involving people with dysarthria as a result of Parkinson’s disease. 16 Participants in that study described coping strategies that included physical, monitoring and adjustment strategies similar to those described by our participants with dysarthria as a result of stroke. Strategies described included highly effortful speech, capacity limitations (in relation to both voice and energy resources), speech production and communication facilitation strategies. 16 Interestingly, research conducted with other rehabilitation populations has also found that they develop and engage with a range of self-care activities that may not be immediately obvious to the clinician. For example, people with cardiovascular disease often engage in ongoing activities, such as monitoring and responding to symptoms. 25 The participants in that study were found to have developed sophisticated ways to address the complex logistics of daily management, 26 while their carers and families also appeared to engage in equally wide and sophisticated techniques. 27 Further research is needed to examine and clarify the inconspicuous strategies and activities used by carers of people with dysarthria.
It is vital that therapists, especially speech and language therapists, consider the patient’s perception when screening, assessing, diagnosing, treating and discharging people with dysarthria following stroke. Screening and assessment should consider the degree of effort and the nature and quantity of internalized cognitive activities required to produce speech rather than focusing upon externally observable characteristics alone. Self-monitoring skills should be explored as an essential prerequisite to improving an individual’s speech quality. Strategies to compensate for their dysarthria, maximize communicative effectiveness and encourage participation in the functional communicative activity of conversations, are hugely important.
Participant responsibility and motivation for rehabilitation were essential components to undertaking rehabilitation activities. Activities should be clearly linked to the rehabilitation goal of improving speech. Therapists should be cognisant of the stigmatizing impact of dysarthria and make every effort to avoid compounding this in their choice of rehabilitation activities, materials and targets. Challenging, functionally relevant, patient-focused activities, materials and targets are more likely to be perceived by the patient as relevant and worthwhile and are more likely to ensure adherence to recommended rehabilitation activities. These components are also known to be the characteristics of effective rehabilitation approaches for other motor recovery interventions. While there remains a paucity of evidence for effective interventions to address dysarthria following stroke, we should focus our efforts on interventions that share these characteristics and which we now know also reflect the perceptions of people with dysarthria.
Clinical messages
People with dysarthria employ numerous internal and external management and rehabilitation strategies. Patients need adequate explanation of the assessment, diagnosis and treatment approaches employed by therapists. Patients reported adherence to rehabilitation activities perceived to be challenging, functional and reflected their interests. Activities that were not were abandoned.
Footnotes
Acknowledgements
Participants, carers, recruiting therapists (Gillian Paton, Sarah de Blieck, Judith Bradley [Paisley], Alison Hamilton, Margaret Jamieson, Cath Black [Aberdeen], Sandra Walker, Catherine Dunnet, Fiona Paton, Liz Duff, Janet Moore, Audrey Williamson, Donna Swabey, Geraldine Ralph, Shatel Basi [Glasgow], Lorna McAllister, Kay Fegan, Ann-Marie Anderson, Helen Duthie, Keri Wilson, Natalie Turner, Jenny Taylor [Ayrshire], Joyce Firth, Tracy Robson [Stirling], Linda Armstrong, Jeanette Seaman, Kate MacAulay [Perth], Elaine Campbell, Emily Chestnet, Joanne Doonan, Alison MacAuley, Sarah Graham, Claire Fraser [Lanarkshire], Linda Prevett [Dumfries]). Dr L Erwin, Royal Alexandria Hospital, Paisley. Alberta Innovates: Health Solutions and the Canadian Institutes for Health Research for AMC’s career award.
Funding
Supported by funding from the Chief Scientist Office CZH/4/133. The views expressed in this article are those of the authors and not necessarily those of the Chief Scientist Office.
Key to Quotations:
All transcripts are anonymized with pseudo-names used where required
… = pause
() = single bracket indicates speech unclear but possible interpretation.
(()) = double bracket indicates an action that occurs, for example laughter/cough.
[ ] = explanation of Scottish colloquialism or a name.