
Abstract
Introduction
Musculoskeletal disorders are a leading cause of disability and mortality. 1 The term refers to a large constellation of conditions; musculoskeletal disorders can affect the bones (e.g. fractures), the joints (e.g. arthritis), the muscles or extra-articular soft tissues (e.g. fibromyalgia), or the periarticular tissue (e.g. bursitis). 2 The prevalence of musculoskeletal disorders increases dramatically with age and an ageing population can be expected to result in an increasing demand for treatment and rehabilitation. 3
Rehabilitation has the potential to improve both physical functioning and overall mortality in older patients.4,5 Though they tend to be more disabled on admission then their younger counterparts, older adults have been shown to benefit asmuch as young adults from rehabilitation services. 6 A recent meta-analysis of randomized controlled trials found that there are statistically significant short- and long-term improvements associated with geriatric rehabilitation related to functional status, admission to nursing homes and mortality. 5 Rehabilitation can be offered in a number of different settings, including inpatient, outpatient and home-based settings; currently there is a lack of consensus on which settings provide ideal treatment for older patients. Considering the changing demographics of our society, proper management for older patients with musculoskeletal disorders is required.
Though there are a number of benefits associated with inpatient rehabilitation, hospitals may not be an ideal care setting for older patients. Because of comorbid conditions, medical complexity and frailty, older adults are at higher risk of having negative complications while in hospital. 7 Hospitalization in this patient group is associated with increased risk of infections, accelerated bone loss and sensory deprivation, any of which could lead to irreversible functional decline.7–9 In addition, the passive hospital routine can act as an initial step towards longer term institutionalization. Creditor 7 found that as many as three-quarters of older adults aged 75 or older who were functionally independent on admission to the hospital for acute illnesses, were no longer independent on discharge. These concerns regarding the hazards of hospitalization for older adults, accompanied by the high cost of inpatient treatment, suggest that alternative settings may be appropriate for rehabilitation.
As recovery for musculoskeletal patients tends to focus more on functional than medical issues, home-based rehabilitation may be more appropriate than inpatient services. Some argue that for many musculoskeletal patients, home-based rehabilitation can help to reduce overall costs to the health system by decreasing the patient’s length of stay in hospital and replacing treatment with less expensive home visits without impeding the patient’s recovery.10–13 In this setting, patients live and are treated at home by physiotherapists, occupational therapists and other allied health professionals which frees hospital bed space and decreases the strain on costly specialists such as physiatrists. There is also the potential for numerous non-financial benefits associated with providing rehabilitation at home, including increased patient choice, increased patient and caregiver satisfaction and improved health outcomes.12,14 In 2008, seniors over the age of 65 represented 14% of the population, and accounted for 44% of total health expenditures – this is expected to increase to 20% and 60% in 2030 respectively. In home care, seniors represent the majority of clients receiving services. 15 In 2003, 15% of non-institutionalized adults aged 65+ received home care and the average age for all home care clients was 62 years. 16 As older adults make up a substantial proportion of the population receiving home care, it is reasonable to conclude that even small changes targeted at this group will have a correspondingly large impact on the system as a whole.
While there have been recent reviews of the literature comparing the benefits of rehabilitation settings for older respiratory, 17 stroke, 18 cardiac 19 and mentally ill 20 patients, we are unaware of an existing review focusing on older musculoskeletal patients. The objective of this review was to evaluate the effectiveness of inpatient rehabilitation compared to rehabilitation at home on patient outcomes for older adults with musculoskeletal disorders.
Methods
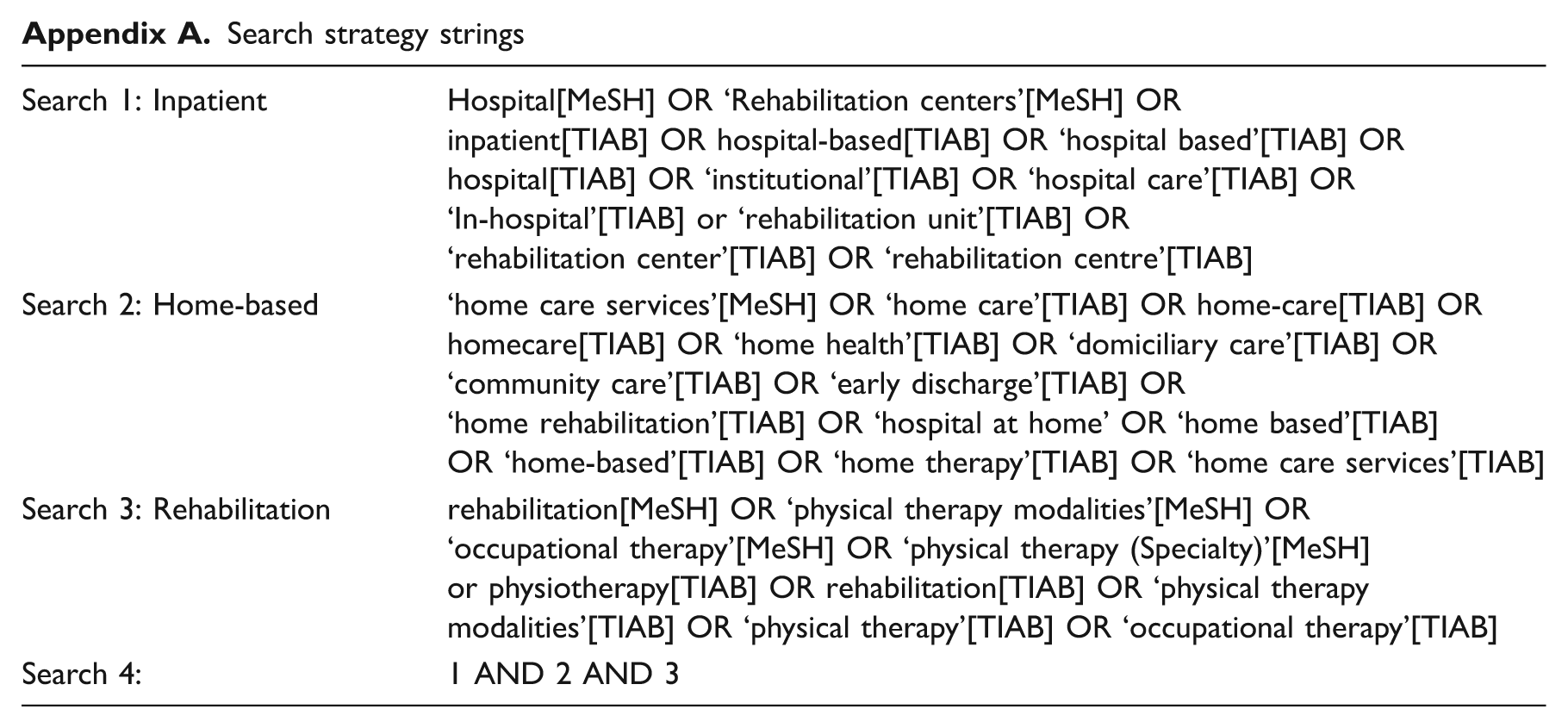
Relevant articles published prior to August 2011 were identified using MEDLINE, CINAHL and the Cochrane Central Register of Controlled Trials databases. A combination of free-text terms and the appropriate controlled vocabulary were used to systematically search each database. The search strategy was a combination of three search strings;inpatient, home-based and rehabilitation (Appendix A).
Articles that compared patient outcomes of home-based and inpatient rehabilitation for older adults were included. A senior population was defined as having a mean age of over 55 years. 21 Rehabilitation was classified as inpatient when patients received occupational therapy or physiotherapy while residing in an acute care hospital or other rehabilitation facility. Rehabilitation was classified as home-based when care was given by an occupational therapist or physiotherapist in the patient’s residence while the patient was living at home. Outpatient care was not included as home-based or inpatient rehabilitation. Only articles in English were considered for inclusion. Studies that focused on samples with musculoskeletal disorders (as defined in the introduction) were considered for inclusion, while studies on populations of respiratory, 17 stroke 18 cardiovascular diagnoses 19 or intermittent claudication 22 were excluded because previous reviews have recently been completed with these populations. As we feel that patient outcomes, including functional ability and mortality, should be considered prior to the assessment of cost savings, this review focused only on patient outcomes. Articles that focused exclusively on cost effectiveness of home and inpatient rehabilitation programmes were excluded. For articles that investigated patient outcomes as well as economic impact, only the patient outcome data will be reported in this review.
One author eliminated irrelevant articles by inspection of title and abstract using the inclusion and exclusion criteria described above. When there was uncertainty about its relevance, the full article was retrieved for review. Two second authors inspected and discussed the article when relevance was ambiguous. The references of the selected articles were then hand-searched for additional relevant studies. Each of the selected articles were summarized using a PICO chart, 23 which is a method used to identify the components of a research question: population, intervention/exposure, comparison, and outcome. All selected studies were evaluated using the PEDro scale, 24 a checklist for internal validity of randomized control trials. The articles that were not randomized controlled trials were still evaluated using the PEDro with the rationale that if they were valid studies, they would excel in all other areas not related to randomization. Moseley and colleagues 25 defined studies with PEDro scores above 5 as moderate to high quality. Each article was first assessed for validity independently by two reviews (LW and CG), followed by a consensus meeting with a third reviewer (PS).
Results
The initial search yielded 3871 articles, of which 634 were removed as duplicates. Of the remaining 3237 articles, 3199 articles were excluded based on their abstracts and titles, as per the inclusion and exclusion criteria. One additional article was obtained through hand-searching the reference lists of relevant articles. Figure 1 illustrates this process. Two of the articles by Crotty and colleagues were found to be of the same study, with one reporting long-term follow-up data. The articles were treated as one study with both the short- and long-term results examined in this review.12,26 Of the 12 studies included in the final sample, eight were randomized controlled trials and four were cohort studies.
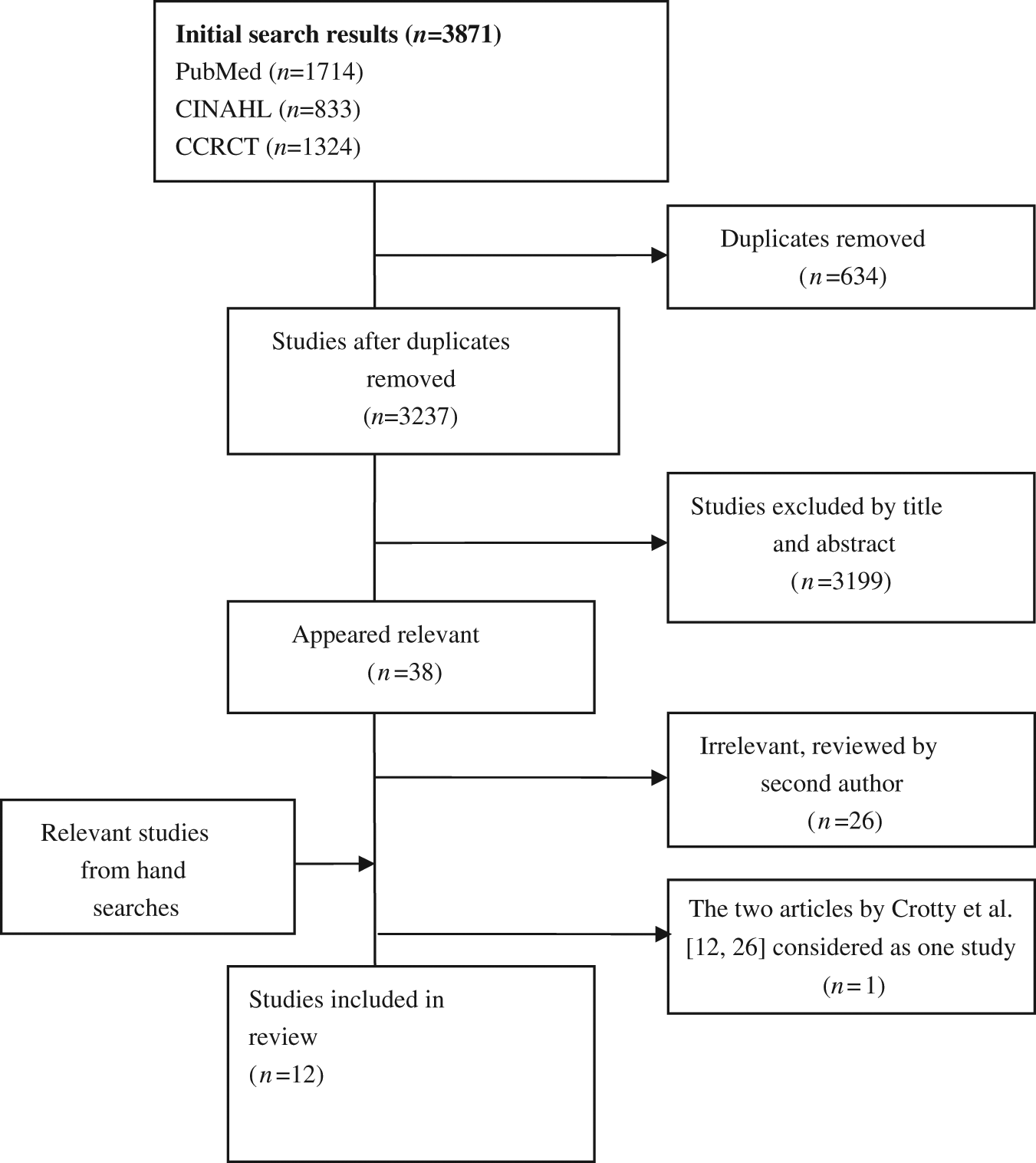
Results of search strategy.
Table 1 lists the PEDro scores for each of the studies. All 12 articles were in the moderate to high category with scores ranging from 5 to 9 points. The mean score was 6.7 (SD 1.4).
PEDro scale results
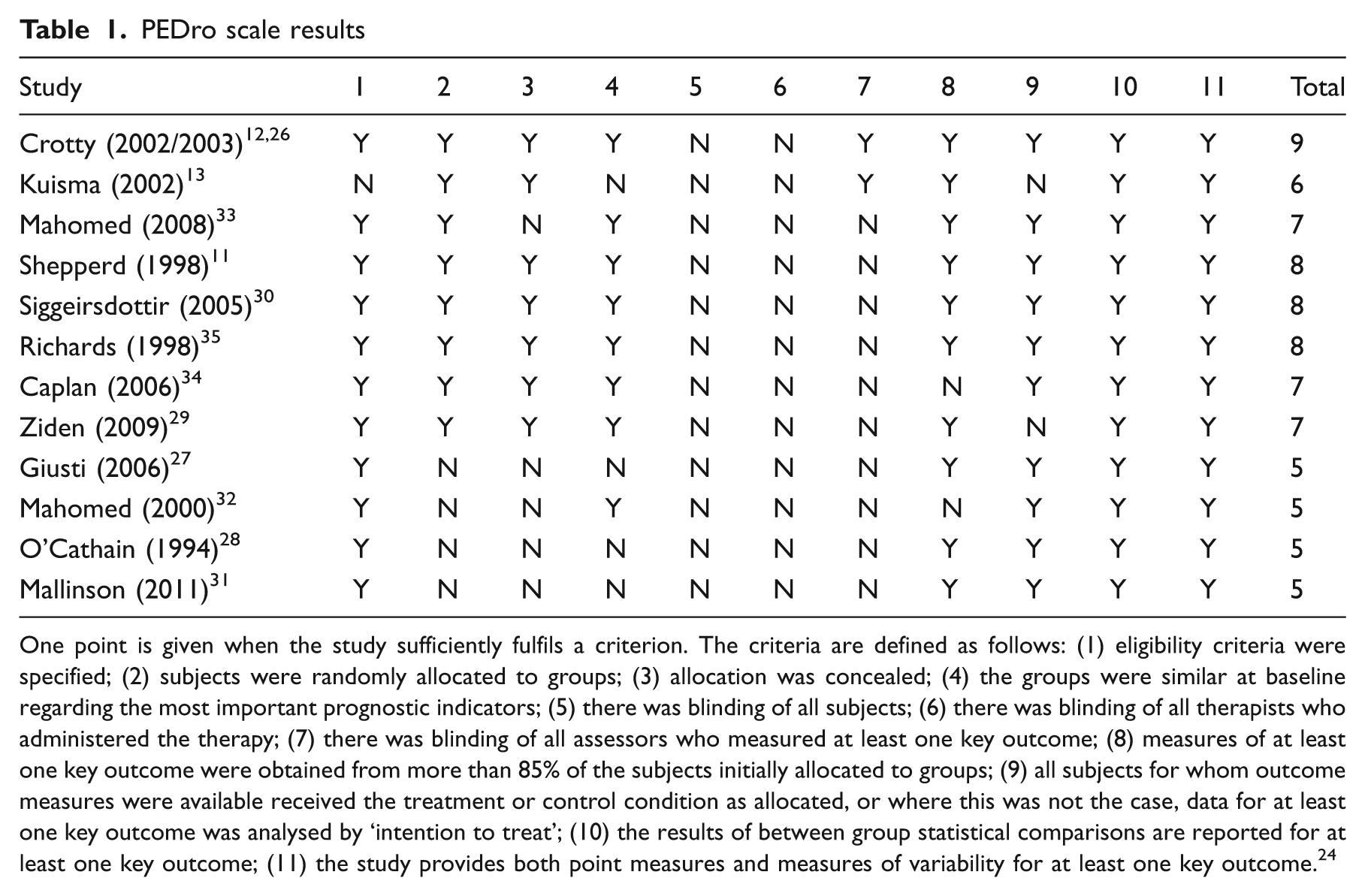
One point is given when the study sufficiently fulfils a criterion. The criteria are defined as follows: (1) eligibility criteria were specified; (2) subjects were randomly allocated to groups; (3) allocation was concealed; (4) the groups were similar at baseline regarding the most important prognostic indicators; (5) there was blinding of all subjects; (6) there was blinding of all therapists who administered the therapy; (7) there was blinding of all assessors who measured at least one key outcome; (8) measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups; (9) all subjects for whom outcome measures were available received the treatment or control condition as allocated, or where this was not the case, data for at least one key outcome was analysed by ‘intention to treat’; (10) the results of between group statistical comparisons are reported for at least one key outcome; (11) the study provides both point measures and measures of variability for at least one key outcome. 24
All of the studies had an average or a median patient population age of 63 and older (The following results are also presented in table format in Appendix B available online). Five of the articles focused on hip fracture patients,12,13,26–29 two on hip replacements,11,30 one on knee replacements, 11 three on both hip and knee replacements31–33 and three on medical patients with a variety of orthopaedic conditions.11,34,35 Shepperd and colleagues 11 examined the outcomes of home-based rehabilitation in five different groups; however, each subgroup of participants were treated as being in a separate trial and results were analysed and reported separately for each group. Of these groups, only the orthopaedic and elderly medical patients were included in this review.
Several of the studies required that the subjects were community dwelling or living at home pre-injury.12,26,27,29,30,34 Physician approval was a requirement for inclusion in 4 of the 12 studies.11,28,29,35 Some of the studies excluded individuals without an adequate home environment for home-based rehabilitation.11,12,26,28,34 This adequacy was defined inconsistently across articles but tended to focus on sufficient social support and safe and available facilities at home. The inpatient rehabilitation setting was an acute care hospital for seven studies11,12,26–30,34 and a rehabilitation facility for five studies.13,31–34 The outcomes of 1596 subjects involved in the 12 studies were considered in this review.11–13,26–35
The home treatment varied between groups with respect to the frequency and/or type(s) of care. Three of the studies incorporated early discharge as part of their home rehabilitation option.12,26,30,34 Early discharge was based on the length of stay in the acute hospital and not patient status, whereas the patients in the other three-quarters of the studies were discharged from the acute hospital only once a certain level of independence was achieved.
The studies varied in the content and frequency of rehabilitation services provided. For the six studies that reported mean number of home visits, the mean was 9.7 ± 6.0, ranging from 4.1 28 to 20. 34 Siggeirsdottir and colleagues 30 and Ziden et al. 29 reported median number of home visits of 4 and 4.5, respectively. Four of the articles did not report the number of visits made.11,27,32,34 All home-based rehabilitation consisted of visits from a physiotherapist and/or occupational therapist; other members of the home-based rehabilitation teams included speech pathologists,13,14,26 nurses/nurses’ aides,11–13,28–30,32,34,35 social workers and podiatrists,12,28 physicians 34 and support workers.12,26,28,35 With the exception of the studies by Caplan et al., 34 Giusti et al. 27 and Mallinson et al., 31 the treatments given as home rehabilitation were specifically designed for the study and differed from usual home care given in the community. Often they included services above the usual home care given and had multiple components such as pre-operative education30,32 or goal-setting.12,26,29
Table 2 summarizes the functional, mental and quality of life outcomes measured in the articles reviewed. With the exception of one, 28 all articles measured functional outcomes. The most common assessment tools used were the Functional Independence Measure (FIM 36 ),29,34 Barthel Index (BI 37 ),11,27,35 Timed Up and Go (TUG 38 ),12,28,29, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC 39 )32,33 and Oxford Hip Scores (OHS 40 ).11,30 The two studies31,34 to measure cognitive outcomes used the Mini-Mental State Examination, 41 the Confusion Assessment Method 42 and the Minimum Data Set 2.0. 31 The only quality of life assessment tool that was used consistently was the Short Form-36 (SF-36 43 ).12,26,29,32,33
Summary of functional, cognitive and quality of life results at baseline and follow-up

Values presented in mean ± SD unless otherwise indicated.
ABC, Activities-Specific Balance Confidence Scale; 44 BBS, Berg Balance Scale; 45 BKS, Bristol Knee Score; 46 BI, Barthel Index; 37 CAM, Confusion Assessment Method; 42 CESD, Centre of Epidemiological Studies Depression Scale; 47 D-COOP, Dartmouth COOP charts; 48 EM, Elderly Medical patients; EQ-5D, EuroQol; 49 FAI, Frenchay's Activity Index; 50 FES, Falls Efficacy Scale; 51 FIM, Functional Independence Measure; 36 GDS, Geriatric Depression Score; 52 HHS, Harris Hip scale; 53 HR, hip replacement patients; IAM, Instrumental Activity Measure; 54 IRF-PAI, Inpatient Rehabilitation Facility Patient Assessment Instrument; 31 KR, knee replacement patients; LHS, London Handicap Scale; 55 MBI, Modified Barthel’s Index; 56 MCS, Mental Component Summary; MDP, Merule D’Abuigne and Postel; 57 MMSE, Mini-Mental State Examination; 41 MDS 2.0, Minimun Data Set 2.0; 31 NHP, Nottingham Health Profile; 58 OHS, Oxford Hip Scores; 40 PAAF, Patients Admission and Assessment Form; 12 PCS, Physical Component Summary; SF-36, Short Form-36; 43 STS, Sit-to-Stand; 59 TUG, Timed Up and Go; 38 WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; 39 IQR, interquartile range.
A higher score indicates a positive outcome; ◊ a lower score indicates a positive outcome.
Significant difference at α = 0.05 between home and hospital groups.
N/A, data not available or explicitly presented.
For all studies that measured functional improvement and quality of life, the home group had scores equal to or better than the hospital group. Of significance, four studies found that the functional status of the home group was significantly better than the inpatient group after the rehabilitation period.13,27,29,30 Also, four of the 12 studies found quality of life was significantly better for the home-based rehabilitation group11,26,29,30 and one found that the rate of delirium was significantly lower for clients receiving rehabilitation at home. 34
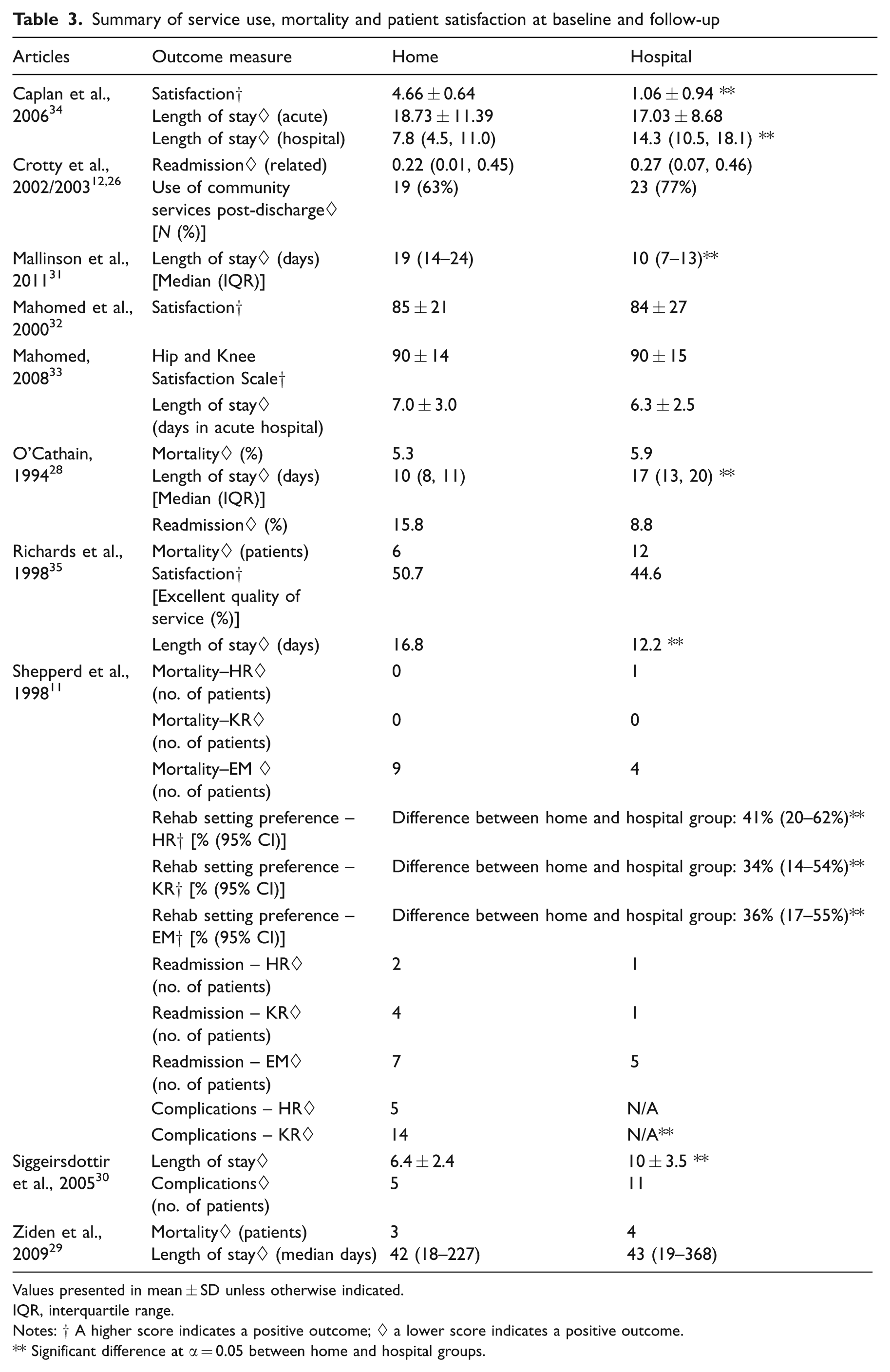
Nine of the 12 articles tracked service use, mortality rates and/or satisfaction scores (Table 3). Of significance, the home group had better scores in level of satisfaction 34 and preference of rehabilitation setting. 11 In four studies, length of stay was defined as the number of days in hospital, and each found the home group to have a shorter length of stay than the inpatient group.26,28,30,34 Richards and colleagues 35 defined length of stay as time from admission to acute hospital until the end of rehabilitation (including home-based rehabilitation) whereas Mallinson and colleagues 31 defined length of stay as the length of the rehabilitation treatment. Both studies concluded that the home group had a significantly longer length of stay than the inpatient group. Four of the 12 articles tracked mortality rates and found no difference between the home and inpatient groups.11,28,29,35 Shepperd and colleagues 11 measured the number of complications in knee replacement patients and found that 30% in the home group were unable to be discharged due to complications, however, other researchers did not replicate these findings.32,33
Summary of service use, mortality and patient satisfaction at baseline and follow-up
Values presented in mean ± SD unless otherwise indicated.
IQR, interquartile range.
Notes: † A higher score indicates a positive outcome; ◊ a lower score indicates a positive outcome.
Significant difference at α = 0.05 between home and hospital groups.
Because of the variation in study designs, study populations, interventions, and outcome measures, statistical pooling of study results was not performed.
Discussion
Overall, the studies consistently found that home rehabilitation was equal or superior to hospital-based rehabilitation in nearly all patient outcomes assessed.
A range of study designs, samples, interventions and assessment tools have been used to compare these rehabilitation settings. Between studies there was variation in the composition of the treatment programme, staffing and level of care provided in the community as well as a wide range of outcome measures used to assess patient characteristics. For example, functional ability was assessed in all 12 articles; however, 21 different assessment tools were applied with the most frequent tools only appearing in three studies. The heterogeneity of these articles created a challenge for accumulating the findings and establishing conclusive recommendations. Interestingly, despite this variation, the studies had relatively uniform conclusions and there were no discernible relationships between outcomes and study design. Therefore, this consistency of findings across multiple designs likely strengthens the evidence that home-based rehabilitation is an effective option for this population. However, future research should aim to standardize home interventions and assessment methods and replicate previous study designs so that the findings can be more easily validated, accumulated, compared and implemented.
The findings from this study are reflective of previous literature reviews comparing home-based to inpatient rehabilitation in other patients groups. For example, a review on neurological patients showed that rehabilitation at home is at least equally as effective as in a hospital setting and found a preference for rehabilitation at home by patients and caregivers. 60 Similar findings were reported for cardiac patients where rehabilitation based in either the home or centre improved clinical and health-related quality of life equally. 19 For stroke patients, it was found that early supported discharge increased their level of independence in the long term. 18 Further, a review by Shepperd and colleagues looked at the acute medical population over 18 years of age and found that there was insufficient evidence to conclude effectiveness of either home or inpatient rehabilitation settings with regards to most outcome measures but did find that there was a reduced risk of institutionalization at follow-up and increased patient satisfaction in the early supported discharge group. 61 Home-based rehabilitation for mental health patients has also been shown to reduce the number of days spent in hospital, and benefits in regular patient visits and special considerations to social care were evident. 20
Together these reviews support the view that home care is equally effective in improving clinical and health quality outcomes of a number of chronic health conditions that are prevalent in older patients. As population ageing in Canada has challenged the healthcare system to meet the needs of the growing number of seniors, one potential strategy is to increase the emphasis on policies surrounding ageing in place initiatives. 62 Some view home-based programmes as a comprehensive approach to community care that could lead to a more sustainable healthcare system, and drive benefits in other key priority areas including a reduction in hospital wait times. 63 Home care has been described as the ‘next essential service’ and is currently the fastest growing section of the healthcare system in Canada. 64 With systems pressures leading to more complex conditions being managed in the community, continued research is necessary to ensure that both clients and the system are benefitting from home-based services such as rehabilitation. 65
When considering the findings from this review, it is important to acknowledge that many of the studies recruited a selective group of patients for their intervention which may impact the generalizability of their findings within the heterogeneous population of older orthopaedic patients. For instance, many of the papers had rigorous inclusion criteria such as only including older adults who lived in the community prior to their admission to hospital, requiring patients to receive permission from their physician for home-based rehabilitation or early discharge, and appraisals for adequate home environments prior to discharge. These criteria likely result in the selection of patients for which home rehabilitation is most likely to be feasible and beneficial. This was recognized by Giusti and colleagues 27 who thus attempted to examine the effects of home rehabilitation on an unselected elderly population. They found that home rehabilitation was slightly more effective than inpatient rehabilitation even in older adults with pre-fracture cognitive impairments or functional impairments and was feasible in half of this population. 27 Further research is required that compares the effectiveness of rehabilitation settings for older adults with more complex characteristics, such as those who lack informal caregivers or those who have pre-existing comorbid medical conditions. Some of the studies had home-based interventions that went above and beyond the usual care offered by home care services. This may impact the external validity of the findings as it is often difficult to determine which aspects of the intervention impact the patients.
Also, several limitations of this review are recognized. Although a detailed search strategy was developed to locate articles that fit the criteria for this study, it is possible that studies that did not label the programme as rehabilitation but provided occupational or physical therapy, especially in community, may have been unintentionally excluded. Second, by focusing our search on older patients we may have decreased the generalizability of the findings. It is possible that we would have different results if we focused on a different age group; however, as older adults are the primary users of health services in most countries this is a particularly relevant population to spotlight.
For some outcomes measured, no significant results were found between the home-based and inpatient groups. Future research is needed with larger sample sizes to investigate these relationships, especially for outcomes such as morbidity and hospital readmissions. Further reviews are needed that focus on the system level impacts, including resource utilization and cost-effectiveness of home-based versus inpatient rehabilitation in this population. These issues should continue to be explored while keeping in mind the level of home and hospital treatment provided compared to that of usual care. Caregiver outcomes and impacts should also be examined further as their health and quality of life should also be considered when choosing a rehabilitation setting.
Clinical messages
Home-based rehabilitation was shown to be no less effective than inpatient rehabilitation.
Significant differences in favour of home rehabilitation were found in a number of studies.
Health professionals should consider rehabilitation at home as an alternative to hospital rehabilitation.
Further research is required to compare the cost of home-based and inpatient rehabilitation.
Footnotes
Appendix
Search strategy strings
| Search 1: Inpatient | Hospital[MeSH] OR ‘Rehabilitation centers’[MeSH] OR |
| inpatient[TIAB] OR hospital-based[TIAB] OR ‘hospital based’[TIAB] OR | |
| hospital[TIAB] OR ‘institutional’[TIAB] OR ‘hospital care’[TIAB] OR | |
| ‘In-hospital’[TIAB] or ‘rehabilitation unit’[TIAB] OR | |
| ‘rehabilitation center’[TIAB] OR ‘rehabilitation centre’[TIAB] | |
| Search 2: Home-based | ‘home care services’[MeSH] OR ‘home care’[TIAB] OR home-care[TIAB] OR |
| homecare[TIAB] OR ‘home health’[TIAB] OR ‘domiciliary care’[TIAB] OR | |
| ‘community care’[TIAB] OR ‘early discharge’[TIAB] OR | |
| ‘home rehabilitation’[TIAB] OR ‘hospital at home’ OR ‘home based’[TIAB] | |
| OR ‘home-based’[TIAB] OR ‘home therapy’[TIAB] OR ‘home care services’[TIAB] | |
| Search 3: Rehabilitation | rehabilitation[MeSH] OR ‘physical therapy modalities’[MeSH] OR |
| ‘occupational therapy’[MeSH] OR ‘physical therapy (Specialty)’[MeSH] | |
| or physiotherapy[TIAB] OR rehabilitation[TIAB] OR ‘physical therapy | |
| modalities’[TIAB] OR ‘physical therapy’[TIAB] OR ‘occupational therapy’[TIAB] | |
| Search 4: | 1 AND 2 AND 3 |
Conflict of interest
None declared.
Funding
This work was supported in part by operating grants from the Canadian Institutes of Health Research (MOP 87377 and MOP 89828).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.