
Abstract
Objective:
To investigate the acute effect of knee joint icing on knee extension strength and knee pain in patients shortly after total knee arthroplasty.
Design:
A prospective, single-blinded, randomized, cross-over study.
Setting:
A fast-track orthopaedic arthroplasty unit at a university hospital.
Participants:
Twenty patients (mean age 66 years; 10 women) scheduled for primary unilateral total knee arthroplasty.
Interventions:
The patients were treated on two days (day 7 and day 10) postoperatively. On one day they received 30 minutes of knee icing (active treatment) and on the other day they received 30 minutes of elbow icing (control treatment). The order of treatments was randomized.
Main outcome measures:
Maximal knee extension strength (primary outcome), knee pain at rest and knee pain during the maximal knee extensions were measured 2–5 minutes before and 2–5 minutes after both treatments by an assessor blinded for active or control treatment.
Results:
The change in knee extension strength associated with knee icing was not significantly different from that of elbow icing (knee icing change (mean (1 SD)) –0.01 (0.07) Nm/kg, elbow icing change –0.02 (0.07) Nm/kg, P = 0.493). Likewise, the changes in knee pain at rest (P = 0.475), or knee pain during the knee extension strength measurements (P = 0.422) were not different between treatments.
Conclusions:
In contrast to observations in experimental knee effusion models and inflamed knee joints, knee joint icing for 30 minutes shortly after total knee arthroplasty had no acute effect on knee extension strength or knee pain.
Introduction
Patients who have undergone total knee arthroplasty are characterized by reduced functional performance,1,2 which is pronounced early after surgery. 3 The reduction in functional performance after total knee arthroplasty relates to a corresponding reduction in knee extension strength, suggesting a causal relationship.1,2,4 We recently reported average knee extension strength to be reduced by as much as 83% at hospital discharge 2.4 days 3 after fast-track total knee arthroplasty, 5 and others report residual knee extension strength deficits from three months 1 up to 2.8 years after total knee atrhroplasty.1,6,7 As walking ability is known to correlate with knee extension strength, 2 it seems particularly important to improve knee extension strength early after surgery, to reduce further atrophy and improve functional performance to a higher level more quickly.
The initial reduction in knee extension strength after total knee arthroplasty seems to be caused primarily by quadriceps muscle inhibition due to postoperative knee swelling, pain and inflammation – also known as arthrogenic quadriceps muscle inhibition.8–12 Some support for this notion exists in the clinically swollen knee, since the initial knee extension strength reduction is negatively related to the degree of postoperative knee swelling early after total knee arthroplasty, 3 and aspiration from chronically swollen knees acutely increases knee extension strength. 13 Similar findings are observed in experimental knee effusion human models.14,15 Applying ice locally to the experimentally effused human knee reduces arthrogenic quadriceps muscle inhibition,8,11,16 and a similar effect is seen after ice treatment of the inflamed knee joint in individuals with tibiofemoral osteoarthritis. 17
Therefore, the objective of this study was to investigate the acute effect of knee joint icing on, first, knee extension strength, and, second, knee pain in patients shortly after total knee arthroplasty. Elbow icing was used as control treatment. We hypothesized that knee extension strength would increase more, and knee pain decrease more after knee icing compared to the control treatment.
Methods
The study used a prospective, single-blinded, randomized, cross-over design, in which patients undergoing primary unilateral total knee arthroplasty from a specialized fast-track orthopaedic unit 5 were investigated on two days: day 7 and day 10 in the second postoperative week, after the prescribed multimodal pain treatment had ended (see below). During one day, they received 30 minutes of knee icing (active treatment) and on the other day, 30 minutes of elbow icing (control treatment), administered by a treatment assessor blinded to the measurements described below. The order of treatments was randomized, using 24 pre-filled envelopes specifying the treatment order (12 of each treatment order). The allocation was determined on the first treatment day after the treatment assessor had drawn an envelope. All measurements were performed on both days before and after treatments (Figure 1) by the outcome assessor. The outcome assessor was blinded for active or control treatment, as the plastic bags with ice were removed by the treatment assessor before the second measurements. The outcome assessor used sunglasses to avoid seeing possible colour changes after icing and thermal gloves to avoid recognizing whether the measured knee joint was cooled or not. Finally, the patients were instructed not to divulge or to ask any questions about the treatments to the outcome assessor.
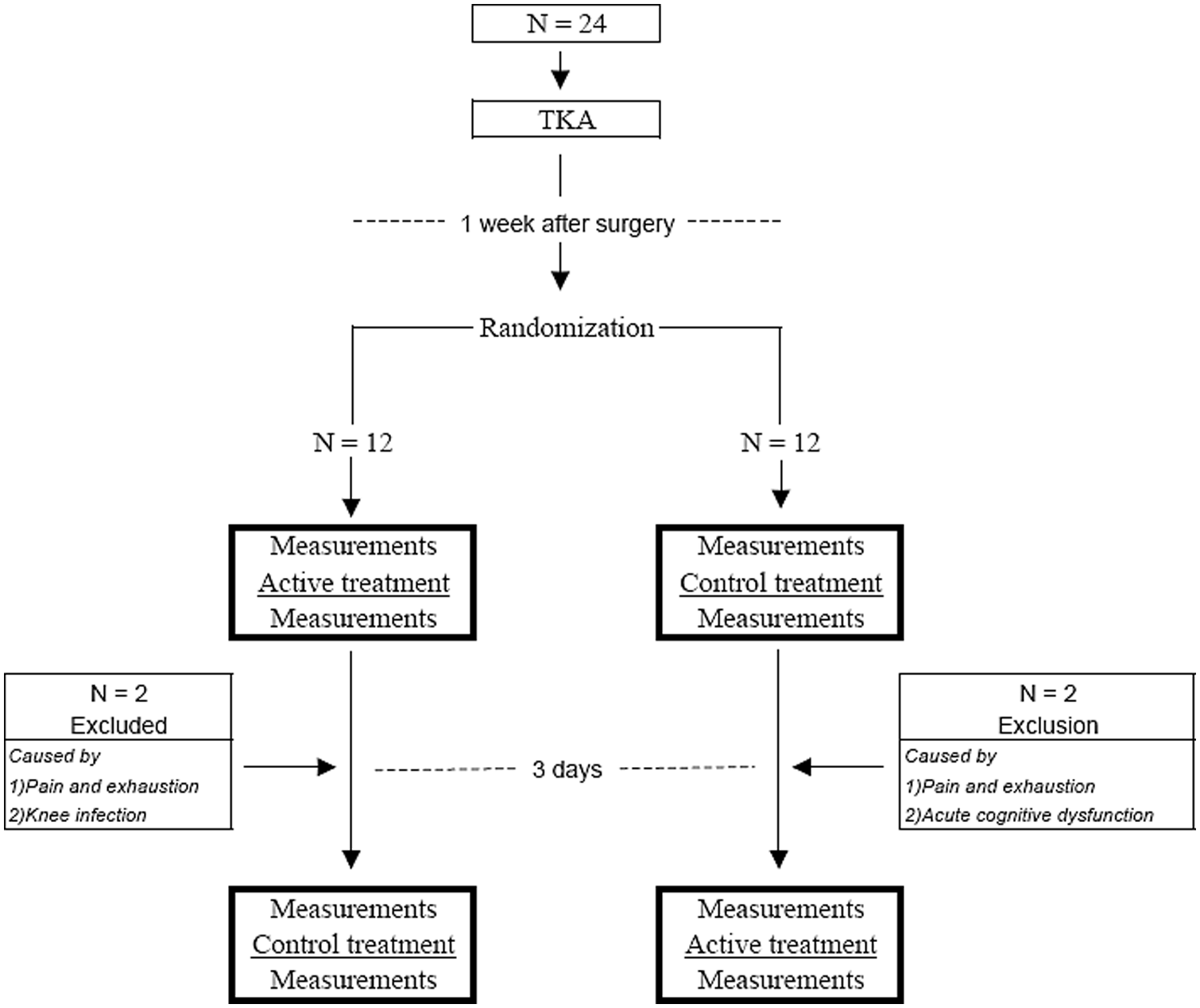
Design and flow of participants.
Twenty-four patients who underwent primary unilateral total knee arthroplasty at a single institution between April 2010 and August 2010 were included. The inclusion criteria were planned primary unilateral total knee arthroplasty; the exclusion criteria were inability to speak and understand Danish, and inability to perform the tests due to other diseases, such as rheumatoid arthritis, polyneuropathy or lower extremity peripheral paresis. Four patients dropped out of the study after the first treatment session (two because of knee pain and exhaustion, one because of suspicion of knee infection, and one because of acute postoperative cognitive dysfunction). Baseline characteristics for the remaining 20 participants are shown in Table 1.
Participant characteristics
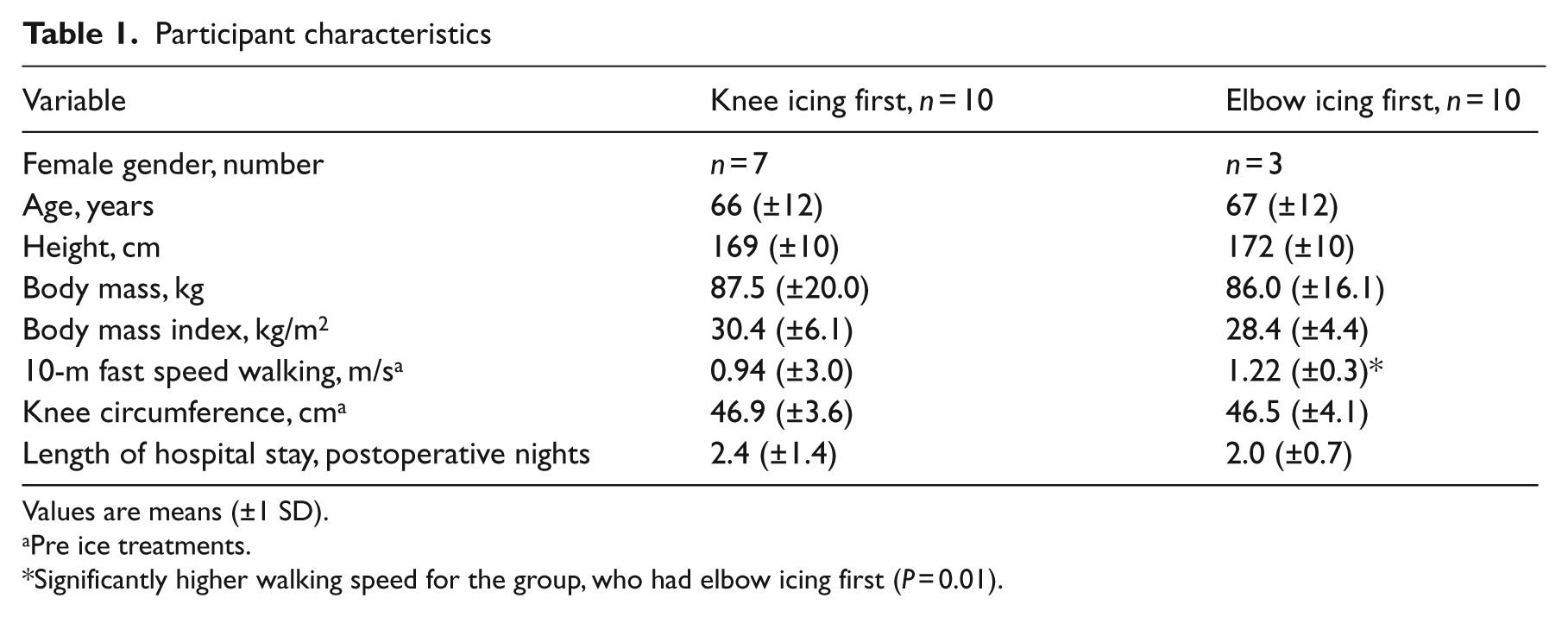
Values are means (±1 SD).
Pre ice treatments.
Significantly higher walking speed for the group, who had elbow icing first (P = 0.01).
The four patients who dropped out appeared to be comparable to the 20 patients who completed the study with regard to their mean (1 SD) age of 65 (8) years, height of 174 (8) cm, body mass of 102 (11.6) kg, body mass index of 33.8 (3.2) kg/m2, length of hospital stay of 2.0 (0) days, pretreatment knee extension strength of 0.12 (0.05) Nm/kg, pain at rest of 28.5 (36.1) mm and pain during the knee extension strength measurement of 58 (24.5) mm (no statistics were performed for these four patients as n = 4).
We gave all patients written information about the procedures of the study, and obtained informed consent in accordance with the declaration of Helsinki. The ethical committee in Copenhagen approved the study (H-A-2008–063, no. 24100). ClinicalTrials.gov Identifier: NCT01249612.
Based on a pilot study in seven patients after total knee arthroplasty receiving active treatment and following the exact same experimental protocol as described in the present study, a power analysis determined that 20 patients needed to be included, using 15% as a clinically meaningful effect (15% or larger knee extension strength increase due to the active treatment), a type I error rate of 5% (P < 0.05), and a type II error rate of 20% (80% power). To account for a potential drop-out, 24 patients were included.
All patients followed a fast-track programme for total knee arthroplasty. 5 We admitted patients to a specialized ward for patients receiving arthroplasties only, where they received preoperative multidisciplinary education, standardized multimodal pain treatment, postoperative rehabilitation including early ambulation. Preoperatively, we initiated a daily dose of gabapentin (900 mg/day), paracetamol (4 g/day) and celecoxib (400 mg/day) on the morning of surgery, and continued for six days. Two experienced surgeons performed all operations. Patients underwent the operation with spinal anaesthesia supplemented with ‘local infiltration analgesia’ infiltrated at the end of surgery.18,19 All patients had a medial parapatellar approach (midline skin incision), with a cemented tricompartmental prosthesis with fixed bearing (including resurfacing of the patella). No patients had drains.
Postoperatively, we used oxycodone (5 mg) as a rescue analgesic for moderate or severe pain (multimodal pain treatment). All patients were advised to elevate the operated leg when resting. The postoperative rehabilitation included mobilization with a high walker on wheels on the day of surgery (within a few hours), with further daily standardized physiotherapy according to an established clinical pathway. 20 All patients were discharged to their homes according to well-defined discharge criteria, 5 and were informed to continue with further daily analgesics following the six-day prescribed pain treatment, ordered by their general practitioner.
During both treatments the patients laid supine with pillows under the head and elbow. A thin cotton cloth was placed around the treated joint, and two plastic bags (1.5 L each) with crushed ice were placed on the anterior and posterior surfaces of the treated joint, respectively.8,11 We wrapped another cotton cloth tight around both ice bags to keep the ice in close contact with the joint. 21 The treatment assessor observed the patient for any complaints every 5 minutes during the 30 minutes of treatment. 8 We told all patients to use the same pain treatment at both treatment sessions. To ensure a cooling effect, we measured skin temperature (Celsius) (Technoterm Typ 3000. Buhl & Boensoee LDT Firm, Copenhagen, Denmark) at the medial joint line before and after icing, and found that joint skin temperature decreased after both treatments, knee icing by 9.0°C, and elbow icing by 12.3°C.
Maximal knee extension force was measured using a fixed hand-held dynamometer (JTECHmedical PowerTrack, II Commmander. Viborg, Denmark). 3 After warm-up and familiarization with the procedure, the patients sat at the end of the examination couch with a hip angle of 90°, knee angle of 60° (0° = full extension), and the feet supported by a small bench to ensure the correct knee angle (60°). We attached a large Velcro strap to the examination couch and the patients’ ankle (perpendicular to the lower leg), 5 cm proximal to the lateral malleolus. Then we placed the transducer at the front of the ankle under the Velcro strap in order to measure the knee extension force. We instructed patients to contract ‘as forcefully as possible with a gradual increase in force’, and provided strong and standardized verbal encouragement during the contractions. They performed five contractions, separated by 60-second pauses, and the highest value was used as the result. Knee extension strength was subsequently expressed at the maximal voluntary torque per kilo body mass (Nm/kg), using the external lever arm length and body mass of each patient. We performed the test according to the procedure used by Gagnon et al., 22 as this procedure has documented substantial reliability in patients with total knee arthroplasty, with an intraclass correlation coefficient (ICC) of 0.99 and an SEM% of 8–10%.
Knee pain was quantified using a visual analogue scale. 23 Patients rated the pain at rest in and around the operated knee when lying supine, and immediately after the active measurements (knee extension strength test) using a ruler with a scale from 0 to 100 mm, where 0 represented no pain and 100 represented the worst pain imaginable (VAS-ruler. Norpharma A/S. Hoersholm, Denmark).
Variability around mean values is expressed as ± 1 SD, as data were normally distributed (Kolmogorov–Smirnov). Between-group differences (knee icing first or last) for descriptive variables at day 7 after total knee arthroplasty were investigated, using independent-samples t-tests. To investigate between-treatment differences in knee extension strength and knee pain, univariate general linear model analyses were performed, using the changes in knee extension strength and knee pain as dependent variables. Treatment (knee or elbow icing), treatment order (knee ice first or last) and time period (day 7 or day 10) were used as fixed factors, and subject (ID) as random factor. P < 0.05 was considered statistically significant. For data analyses, SPSS 19.0 (SPSS Inc., Chicago, IL, USA) was used.
Results
First, we found no effect of knee icing on knee extension strength, as no main effect of treatment was found (change associated with knee icing –0.01 (0.07) Nm/kg, change associated with elbow icing –0.02 (0.07) Nm/kg, P = 0.493 (Table 2). No effects of treatment order (P = 0.363) or time period (P = 0.201) were observed for knee extension strength.
Changes in knee extension strength and knee pain associated with knee and elbow icing
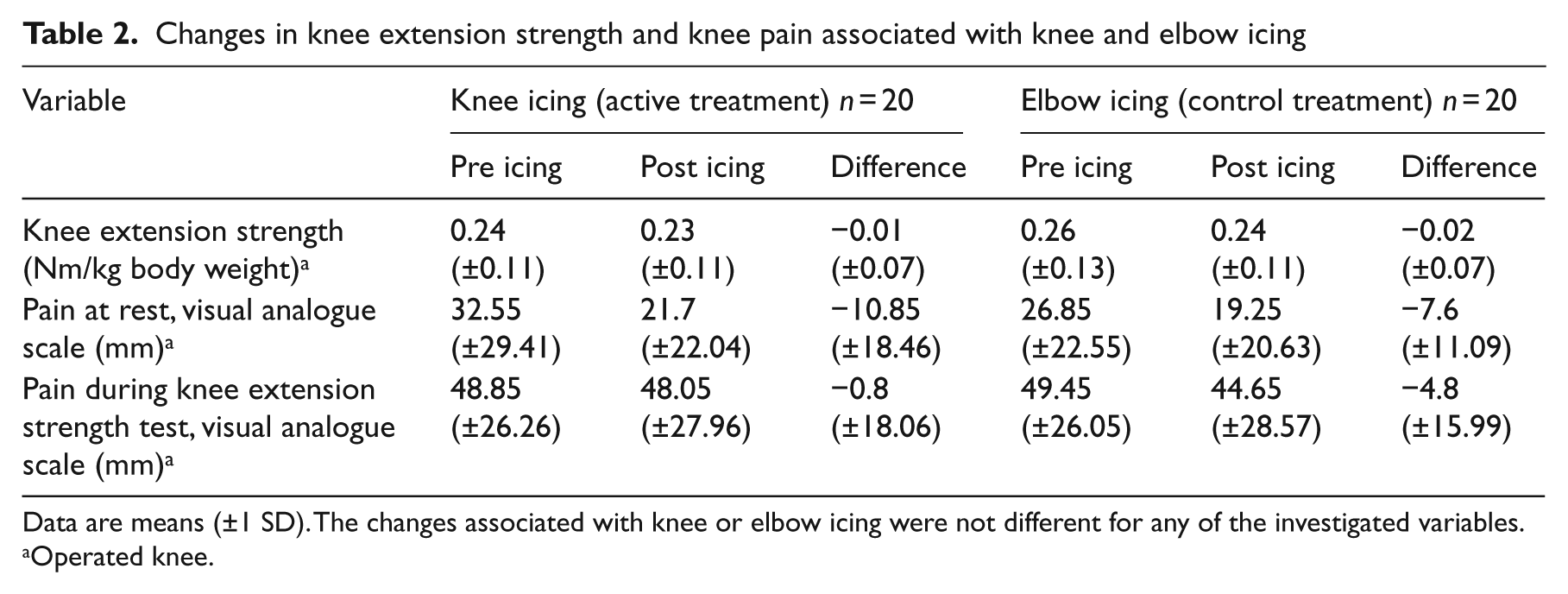
Data are means (±1 SD). The changes associated with knee or elbow icing were not different for any of the investigated variables.
Operated knee.
Second, we found no effect of knee icing on pain at rest (P = 0.475) or pain during the knee extension strength test (P = 0.422) (Table 2). No effects of treatment order (P = 0.934) or time period (P = 0.886) were observed for knee pain at rest. For knee pain during the knee extension strength measurements, however, an effect of time period (P = 0.024) was observed, indicating that knee pain during the knee extension measurements increased more – but was clinically irrelevant – during the experimental protocol at day 7 (VAS pain increase 1.2 (1.6) mm) compared to day 10 (VAS pain increase 0.4 (1.5) mm).
Discussion
The main findings of the present study were that knee joint icing for 30 minutes shortly after total knee arthroplasty had no acute effect on knee extension strength or knee pain, which is in contrast to observations in experimental knee effusion models and inflamed knee joints.
By using a cross-over, within-subject design, we were able to address a simple clinical question, by reducing some of the between-subject variation in knee extension strength early after a total knee arthroplasty. We decided that knee extension strength had to increase by at least 15% to be considered clinically relevant, given the considerable strength reduction early after total knee arthroplasty. 3 To this end, the defined minimum clinically relevant strength increase needed to be greater than the average test–retest variation reported for the knee extension strength measurement in patients with total knee arthroplasty. 22 Hence, the present study had the statistical power to detect strength increases of 15% or more, but not smaller changes.
It has been shown that cryotherapy using ice bags has reversed the decline in quadriceps H-reflex amplitude after experimental knee effusion of the healthy human knee joint, 8 and has increased knee extension strength and muscle fibre conduction velocity in healthy subjects and volunteers with mild arthritis.11,17,21 We found no evidence for a similar positive effect of cryotherapy on knee extension strength after total knee arthroplasty, even though we used two plastic bags, each containing 1.5 L of crushed ice for 30 minutes, similar to the cryotherapy modality used in one previous study, 8 and for a longer time than used in three other studies that reported a strength-preserving effect of cryotherapy applied to the human knee joint.11,17,21 We measured skin temperature at the medial joint line after knee icing, which showed a decrease after icing to 23.8°C, but not as low as reported elsewhere (14–25.4°C),8,11,16,24 probably due to different pretreatment temperatures and different points of measurement. Our pretreatment temperature of 32.8°C was higher than in the above-mentioned studies (26–30°C). We did, however, find a decrease of 9°C after knee joint icing, suggesting that an intra-articular cooling took place, as plastic bags with crushed ice have been shown to reduce both skin and intra-articular knee temperature after 30 minutes of knee icing in healthy subjects. 25 Also, the skin temperature may have been lower had we measured on the anterior part of the knee joint, where most of the ice was placed, as reported by others.8,16,24 However, for hygiene reasons we chose to measure away from the sutures. Nevertheless, our results may call for additional investigations to evaluate the effect of ice treatment on knee extension strength shortly after total knee arthroplasty.
In contrast to our hypothesis, we found no acute effect of knee icing on knee extension strength. This is in contrast to that reported in other studies investigating the effect of cryotherapy on knee extension strength in experimental human knee effusion models,8,11 or human knees with mild inflammation caused by osteoarthritis, 17 probably because patients after total knee arthroplasty experience more massive arthrogenic quadriceps muscle inhibition. It is possible that operated knees with major joint damage after surgery and, hence, knee swelling, behave differently from non-operated but swollen knees, as seen in experimental knee effusion models and knee joints with mild inflammation. That is, even though the decrease in intra-articular temperature may be the same, the temperature decrease may need to be larger in the clinically swollen knee shortly after total knee arthroplasty for any cryotherapy to have a substantial disinhibitory effect on the quadriceps muscle. Especially as the experimental knee effusion model may not mimic the changes in articular afferent discharge that occur with total knee arthroplasty – due to structural damage, inflammation and pain. 12 Along the same lines, insufficient cooling may also help explain why knee icing had no effect on knee pain. It suggests that the discharge of the large majority of afferent fibres innervating the knee, 26 responding to strong mechanical, thermal and chemical stimuli, was not reduced enough to modulate knee pain at rest, nor during the maximal knee extensions.
Hypothetically, some cases of arthrogenic quadriceps muscle inhibition may arise due to a loss of sensory output from knee receptors. 27 This could be the case in total knee arthroplasty, where joint receptors are often damaged preoperatively due to end-stage arthritis or during the operative procedure itself. In this case, cooling the knee to reduce the afferent discharge of joint receptors will do nothing to increase knee extension strength. Therefore, differences between the present study and others that examine experimental knee effusion models and knee osteoarthritis populations might be the extent of tissue damage and subsequent sensory nerve loss, which deserves more attention in future studies.
Knee icing appears to have no acute effect on knee extension strength or knee pain shortly after total knee arthroplasty, as seen in experimental human knee effusion models. Interventions that temporarily reduce arthrogenic quadriceps muscle inhibition early after total knee arthroplasty are important for any early postoperative rehabilitation, as they will enable rehabilitation to be conducted with greater voluntary contribution. Future interventions to serve this purpose include submaximal voluntary contractions, as they have shown to decrease arthrogenic quadriceps muscle inhibition in experimental human knee effusion models, 28 and electrical stimulation, as this has shown to increase the quadriceps muscle activation ratio in patients with tibiofemoral osteoarthritis. 8
Clinical messages
Knee icing for 30 minutes shortly after total knee arthroplasty has no acute effect on knee extension strength.
Knee icing for 30 minutes shortly after total knee arthroplasty has no acute effect on knee pain.
Footnotes
Acknowledgements
The authors wish to thank PhD student Thomas Linding Jakobsen and BSc student Mathilde Kofoed-Hansen for assisting in parts of the experimental work, and the nurses from the Department of Orthopaedic Surgery at Copenhagen University Hospital, Hvidovre for their assistance related to performing this investigation.
Conflict of interest
Each author certifies that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the study.
Funding
This study was supported by a grant from the Lundbeck Foundation for Fast-Track Hip and Knee Arthroplasty and the Danish Association for Physiotherapists (grant number 10-12-2010/13.44).