
Abstract
Objective:
To assess the additional benefits of individualized nutritional counselling by a registered dietitian in geriatric patients’ home after discharge from hospital, in relation to risk of re-admissions, functional status, nutritional status, use of social services and mortality.
Design:
Twelve-week single-blind randomized controlled study.
Setting and subjects:
Geriatric medical patients (65+ years) at nutritional risk.
Interventions:
Participants were randomly allocated to receive a visit in their homes, either three individualized nutritional counselling by a registered dietitian complemented with three follow-up visits by general practitioners or three follow-up visits by general practitioners alone.
Main measures:
Primary outcome was risk of re-admissions. Secondary outcomes were functional status (hand grip strength, chair stand, mobility, disability and tiredness in daily activities, rehabilitation capacity), nutritional status (weight, BMI, energy and protein intake), need of social services (home care, home nursing, meals-on-wheels) and mortality.
Results:
One hundred and fifty-two patients were included; 132 (87%) completed the first and 124 (82%) the second data collection after 12 weeks. Ten per cent of the participants had three contacts with their general practitioner, while compliance with the dietetic intervention was almost 100%. Odds ratio for re-admission and mortality after 26 weeks was 1.62 (95% confidence interval (CI) 0.85 to 3.10) and 0.60 (95% CI 0.17 to 2.13). The intervention had a positive effect on functional status (i.e. mobility, P = 0.029), and nutritional status (i.e. weight, P = 0.035; energy intake, P < 0.001; protein intake, P = 0.001) and the use of meals-on wheels was reduced (P = 0.084).
Conclusion:
Follow-up home visits with registered dietitians have a positive effect on the functional and nutritional status of geriatric medical patients after discharge.
Introduction
Undernutrition is common in old people admitted to the hospital, and nutritional state often deteriorates further during hospital stay. 1 This means that at discharge a large number of older patients will still be undernourished or at nutritional risk, with an increased risk of re-admission.2,3
The period after discharge is an important time for intervention. Hospital stays are generally getting shorter, which leaves less time to improve poor nutritional status. Furthermore, geriatric patients very often lose muscle mass during hospital stay, which requires a focused effort after discharge.
In spite of this, there is a dearth of published evidence of benefit or harm. To our knowledge, only six studies have assessed the benefits of oral nutritional support to geriatric patients at risk of or already undernourished, initiated in relation to discharge. 4 Most studies showed a positive effect on energy and nutrient intake, nutritional status and, in some, also functional status. In contrast, the effect on rehabilitation capacity and survival was very limited. 4 One explanation for the limited effect could be the relatively low level of compliance with oral nutritional supplements reported in some of the earlier studies. 4 None of these studies have included individual goal setting, energy-dense menus, and counselling focusing on nutritional risk factors (i.e. expert advice from a registered dietitian).
Inappropriate medical treatment often has inadvertent effects, and a number of admissions are attributable to inappropriate medical treatment that could be avoided. In a former randomized Danish study it was shown that comprehensive discharge follow-up in geriatric patients’ homes by general practitioners and district nurses reduced re-admission risk in the intervention group. 5 The main focus in that study was general practitioner follow-up on hospital treatment and medications with no special emphasis on nutrition.
The aim of this study was to assess the additional benefits of individualized nutritional counselling by a registered dietitian in geriatric patients’ homes after discharge from hospital, in relation to risk of re-admissions, functional status, nutritional status and use of social services.
Methods
This study was designed as a randomized controlled trial comparing discharge follow-up in patients’ home by general practitioners (GP or family doctors) vs. discharge follow-up in patients’ home by GP and registered dietitians. Patients were eligible for this study if aged 65+ years and at nutritional risk according to the level 1 screen in Nutritional Risk Screening 2002 (NRS2002). 6 Participants were randomized at discharge. Each allocation using generated random numbers was written on paper and concealed in a serially numbered, opaque envelope. The scientific research assistants opened the next envelope after recruiting each participant and then contacted the GP and, if relevant, the registered dietitians. Hence the scientific research assistants, who collected the outcome data, knew which group a participant was in. The principal investigator was the only one blinded for the intervention.
All elderly patients (65+ years of age, living in three municipalities – Herlev, Roedovre or Gladsaxe), hospitalized for a minimum of two days in the geriatric medicine wards of the University Hospital of Herlev, were screened by the nursing staff or a scientific research assistant for nutritional risk. Patients were excluded from the study when they; suffered from senile dementia or terminal disease; could not understand the Danish language; were residing in nursing homes; or were unable to or willing to give informed consent.
Patients were eligible for this study if they were identified as at nutritional risk according to the level 1 screen NRS2002 6 : body mass index (BMI in kg/m2) <20.5; and/or weight loss within the last three months; and/or a reduced dietary intake in the last week; and/or serious ill (e.g. in intensive therapy).
For all patients the discharge follow-up by GPs was planned to consist of three contacts, conducted approximately one, three and eight weeks after discharge in both control and intervention participants. The contacts were guided by an agenda (based on Rytter et al. 5 ):
Check the discharge letter for specific recommended paraclinical or clinical follow-up.
Check need for adjustment of medication.
Check the family’s medical cabinet.
Check the general health status (nutrition (vitamin D), physical activity, alcohol, continence, depression, dementia).
The contacts were either in the GP’s clinic or as a home visit depending on the participant’s overall condition.
For patients randomized to nutritional intervention the registered dietitians performed a comprehensive nutritional assessment at the first home visit as a basis for developing a nutrition care plan consistent with estimated nutritional requirements and nutritional rehabilitation goals. Basal metabolic rate was assessed by means of Schoefield equations and a factorial method, eventual accounting for weight gain factors, and was used to estimate the total energy and protein requirement for each participant (based on Pedersen and Ovesen 7 ).
To assess dietary intake, the registered dietitians performed a standardized dietary interview with each participant to determine total energy and protein intake at each visit. Strategies for achieving energy and protein requirements included dietary counselling with attention to nutritional risk factors, timing, size and frequency of meals, recommendations for nutrient-dense foods and drinks, and provision of leaflets with information. Supplementation with energy- and protein-dense meals-on-wheels, subscription of commercial oral nutritional supplements (ONS) as well as recommendations for vitamin D, calcium and other vitamin minerals was also considered to achieve optimal nutritional status.
All in all, it was planned that the registered dietitians should perform three home visits approximately one, three and eight weeks after discharge, to perform dietetic care and maximize participants’ nutritional status by way of reviewing the nutrition care plan, dietary counselling, motivation and education, monitoring participant weight, and ensuring energy and protein requirements were achieved. If it was considered relevant, the participants received short follow-up consultations by telephone by the registered dietitians in order to give advice and to stimulate compliance to the proposed nutritional intake (between the home visits).
It was planned that at least one counselling session should be together with the participant’s GP, in order to discuss the treatment, either at home or at the GP’s clinic.
After obtaining the participant’s informed consent (at the hospital) an inventory was made of possible confounders. This included the following characteristics:
socio-demographic data (age, gender);
medical diagnosis;
new mobility score (assessment of mobility before admission (total score 0–9, where 9 is best) 8 ;
additional discharge interventions (e.g. outgoing hospital teams, discharge follow-up phone calls).
At the first visit in the participant’s home, the scientific research assistant confirmed the participant’s acceptance of the involvement of his or her GP. The GP then received a letter the inclusion of the participant and the plan for discharge follow-up contacts, including a journal for documentation and a request to return the journal after the last contact/visit. Before the start of the project all GPs in the three municipalities had received information about the project from the Regional Practice Committee, including a statement of the Committee’s support to the project. The registered dietitians were also contacted and asked to contact the participants in the intervention group for the first home visit and make an appointment with the GP for one counselling together. After 12 weeks the participants were contacted by the scientific research assistants via telephone to organize the visit for the follow-up assessments.
If there was no response, the scientific research assistants contacted the hospital to check for an eventual re-admission.
The outcome parameter prevalence of re-admissions (the primary outcome parameter) and mortality was collected from the hospital database. Secondary outcome parameters were measured in the participants’ homes as soon as possible after discharge (first visit) and at +12 weeks (second visit).
All outcome parameters measured are listed below. Unless otherwise stated, the data was gathered by scientific research assistants in the participant’s home at the first and second visit.
Re-admissions between first and second visit and 26 weeks after discharge were evaluated by means of the hospital patient register. Information about the number of days to first re-admission and the number of days spent in hospital was also collected from the register by the principal investigator.
Hand grip strength (in kg) was measured with a Jamar 5030J1 Hydraulic Hand Dynanometer. Participants were seated with forearms rested on the arms of the chair. They were asked to perform three maximum force trials with their dominant hand and using the second handle position. The maximal grip score from the three values was used in the analysis of data.
Chair stand was used to test the physical performance. The participants were asked to fold their arms across their chest and to stand up and sit down on a chair without pushing off with arms, as many times as possible during 30 seconds. They were allowed to use the arms for assistance or for safety if needed. 9 The mode of chair stand was registered.
Mobility was assessed using the validated de Morton Mobility Index (DEMMI). 10 The DEMMI is a 15-item one-dimensional instrument that measures mobility across the spectrum from bed bound to independent mobility by observation of physical performance. The raw score total (0–19) must be converted to a DEMMI SCORE (0–100, where 100 is independent mobility).
Disability was measured by asking questions about need of help in the following six activities: (1) transfer, (2) walk indoors, (3) get outdoors, (4) walk out of doors in nice weather, (5) walk out of doors in poor weather, and (6) manage stairs. Tiredness in daily activities was measured by asking the participants if they feel tired after performing the same six activities and the answers combined into the validated Mob-T scale (0–6 where 6 is best). 11
Restoration of function after discharge was assessed by means of the Functional Recovery Score (FRS). The 11-item questionnaire comprises three main components: basic activities of daily living (BADL) assessed by four items, instrumental activities of daily living (IADL) assessed by six items, and mobility assessed by one item. Basic activities of daily living comprise 44% of the score; instrumental activities of daily living comprise 23% and mobility comprises 33%. Complete independence in basic and instrumental activities of daily living and mobility results in a score of 100%. 12 Participants received instructions from the scientific research assistants on how to fill in the questionnaire. They received the questionnaire in advance of the visits. At the visits the finalized questionnaire was inspected and ambiguous entries clarified.
Weight was measured (with participants wearing light indoor clothes and no shoes). Information about weight was also obtained by the registered dietitians during the visits to the intervention group. BMI was calculated as actual weight in kilograms divided by the square of height in metres. As measurement of height is often not feasible in this chronic diseased, old and frail population, data on height was retrieved from self-reported height.
Energy and protein intake was assessed by means of a four-day dietary record. Participants received instructions from the scientific research assistants on how to fill in the dietary record. They received the dietary records in advance of the visits. At the visits the finalized records were inspected and ambiguous entries clarified. If the participants had not been able to perform the dietary registration a 24-hour recall was performed. The intake of energy and protein was calculated by means of a computer program based on the Danish food composition table (available at www.foodcomp.dk). Schoefield equations were used to calculate the basal metabolic rate (BMR) by means of information about age and body weight. 13 Underreporting of dietary intake was considered when calculated energy intake/BMR was below 1.1.
Information about social services (i.e. the use of home care, home nursing, meals-on-wheels and day care with exercise) was obtained from the participants or their relatives. It was also recorded whether the participant resided in their own home, a rehabilitation unit or a nursing home.
Mortality 26 weeks after discharge was evaluated by means of the hospital’s patient register.
Ethics
The protocol was sent to the Danish Ethical Board which concluded that approval was not needed and that the project could be carried on as described. Nevertheless, informed consent was obtained from all participants. They were also informed about their right to withdraw their consent at any time.
Statistical analysis
For a clinically relevant difference of 10% in re-admissions and an expected drop-out rate of 12% (based on Rytter et al. 5 ), a statistical significant level of 0.05 and a power of 80%, two groups of 80 participants each was calculated to be necessary.
Data entry and control was conducted by the scientific research assistants under supervision of the principal investigator. The primary investigator was responsible for the data cleaning and analysis.
All statistical analysis was performed using IBM SPSS Statistics 19. Data were entered in EXCEL and were subsequently exported into SPSS software for analysis. Primary analysis was undertaken using intention-to-treat principles. Wilcoxon signed rank sum test, Mann–Whitney U-test, and odds ratio or chi-square test of associations was used as appropriate. Data are presented as mean (±SD), number (%) or odds ratio (95% confidence interval (CI)). A P-value <0.05 was considered significant.
The analysis was undertaken by the principal investigator blinded to the randomization.
Results
A total of 277 patients were invited to participate in the period January to August 2011 and 152 (55%) accepted. There was no difference between the participants and non-participants in relation to age, sex and admission diagnosis (data not shown). The participants were randomized into two groups after inclusion. Their characteristics are presented in Table 1.
Characteristics of participants
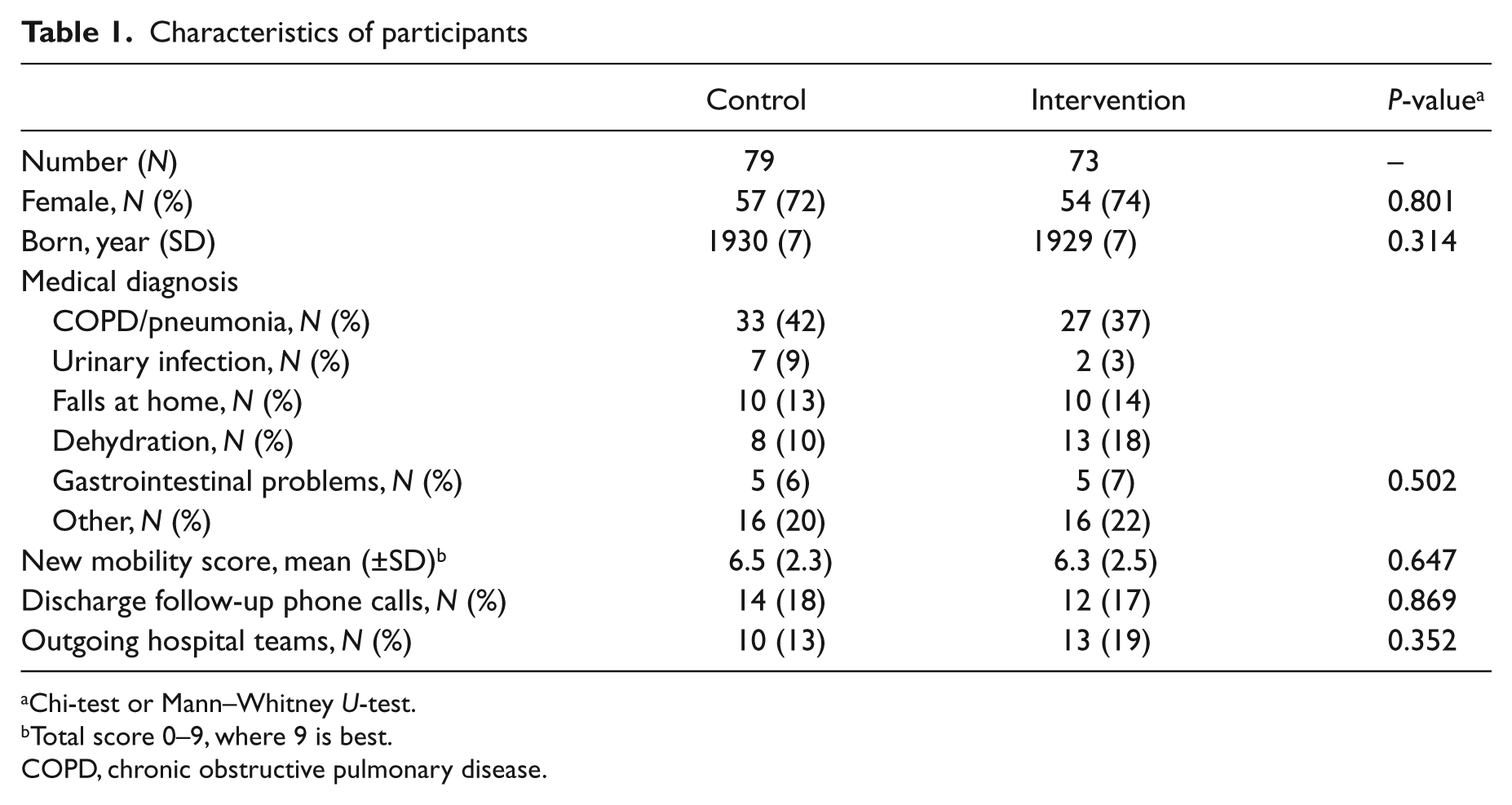
Chi-test or Mann–Whitney U-test.
Total score 0–9, where 9 is best.
COPD, chronic obstructive pulmonary disease.
A total of 132 (87%) participants completed the first data collection and 124 (82%) the second, see flowchart (Figure 1).
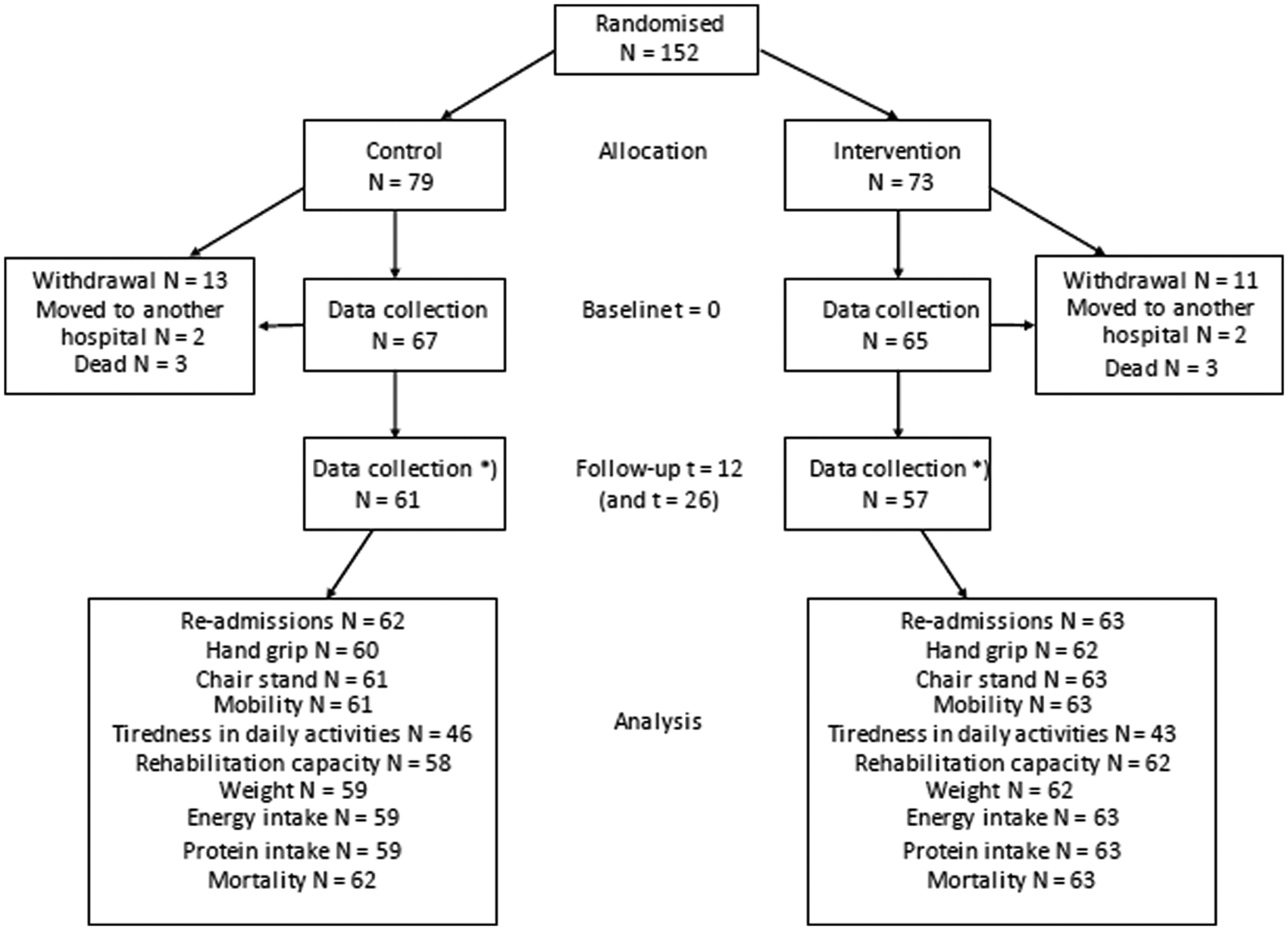
Flowchart for the study. *It was possible to obtain follow-up data from some of those who withdrew.
Data about functional and nutritional status, the use of supplements and social services collected at the first visit are presented in Table 2. There were no differences between the two groups.
Functional status, nutritional status, use of supplements, and need of social services at first visit
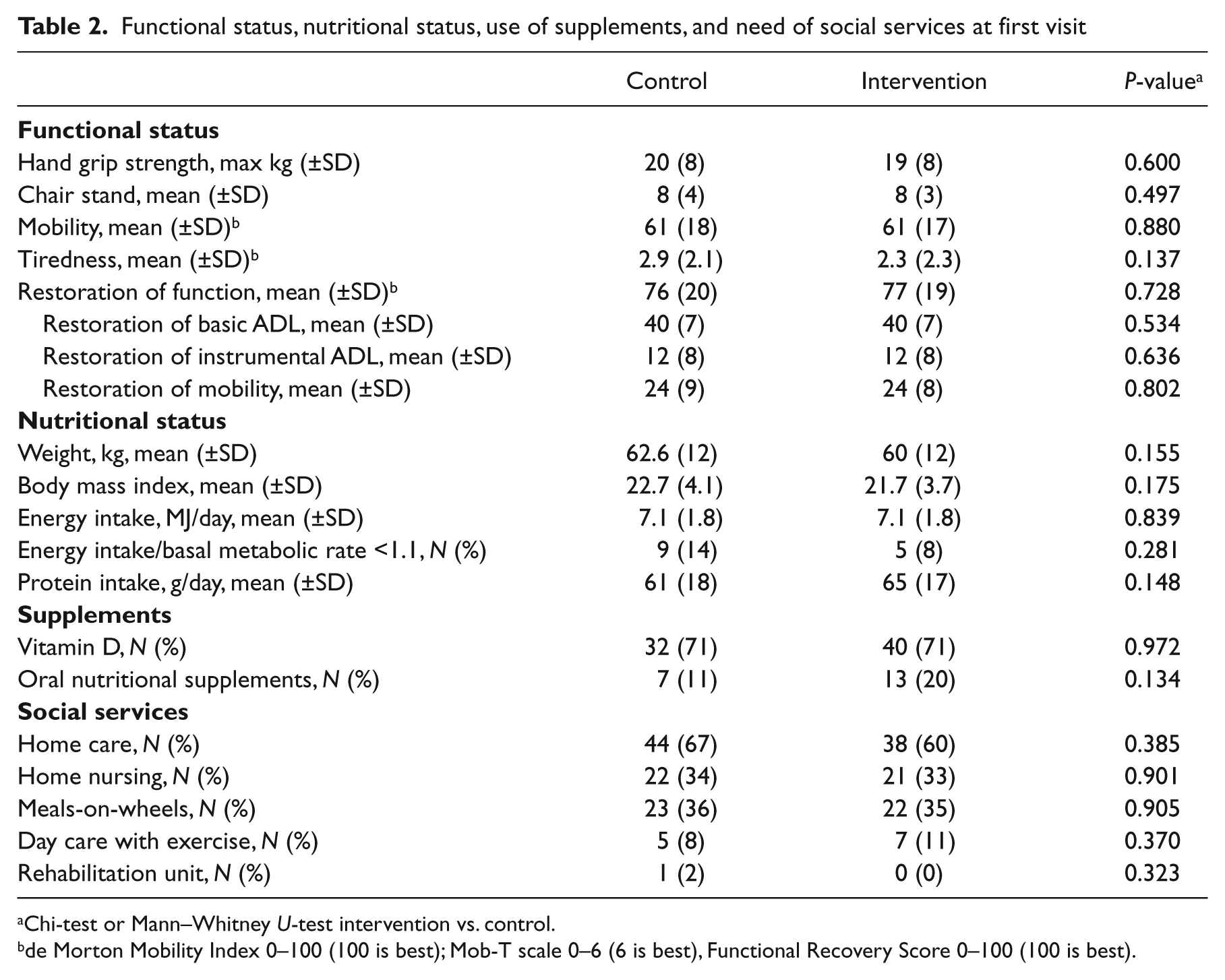
Chi-test or Mann–Whitney U-test intervention vs. control.
de Morton Mobility Index 0–100 (100 is best); Mob-T scale 0–6 (6 is best), Functional Recovery Score 0–100 (100 is best).
The discharge follow-up was planned to consist of three contacts and so was the nutritional intervention. However, around 20% of the participants did not want a visit from their GP, not all GP wanted to participate, and only half of those who did had three contacts. All in all, 15 (10%) of the participants had three contacts with their GP. In contrast the compliance with the dietetic intervention was almost 100% (Table 3). On average, the registered dietitians spent 2 hours per visit, including preparation and documentation of data afterwards. No adverse events were reported.
General practitioner (GP) follow-up and registered dietitian intervention
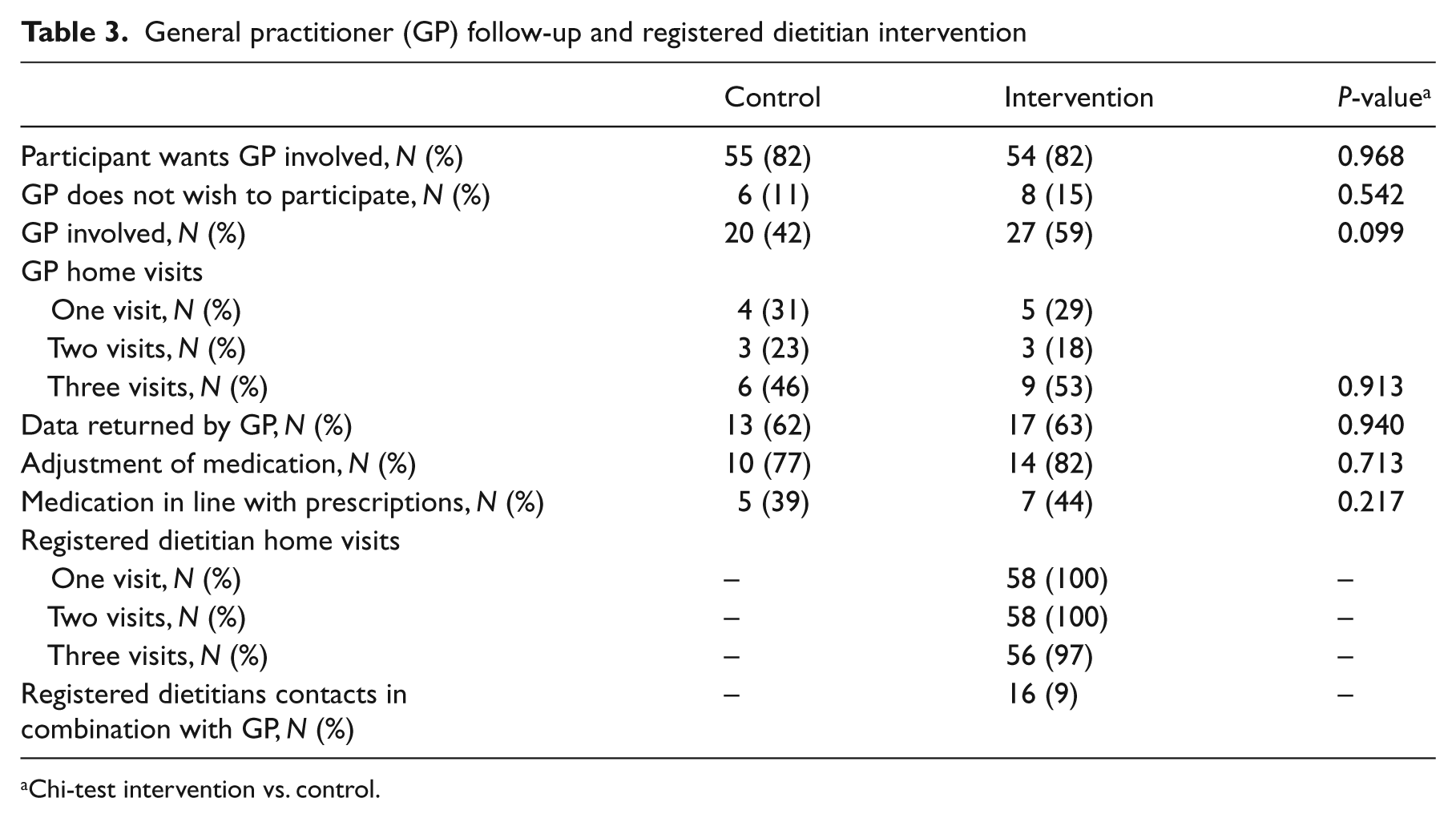
Chi-test intervention vs. control.
Re-admissions between visits 1 and 2 in the participant’s home, and 26 weeks after discharge, the number of days to first re-admission and the number of days spent in hospital are presented in Table 4. All results tended to be in favour of the control group. The odds ratio for re-admission after 26 weeks was 1.62 (95% CI 0.85 to 3.10).
Re-admissions between visit 1 and visit 2 and 26 weeks after discharge, the number of days to first re-admission and the number of days spent in hospital
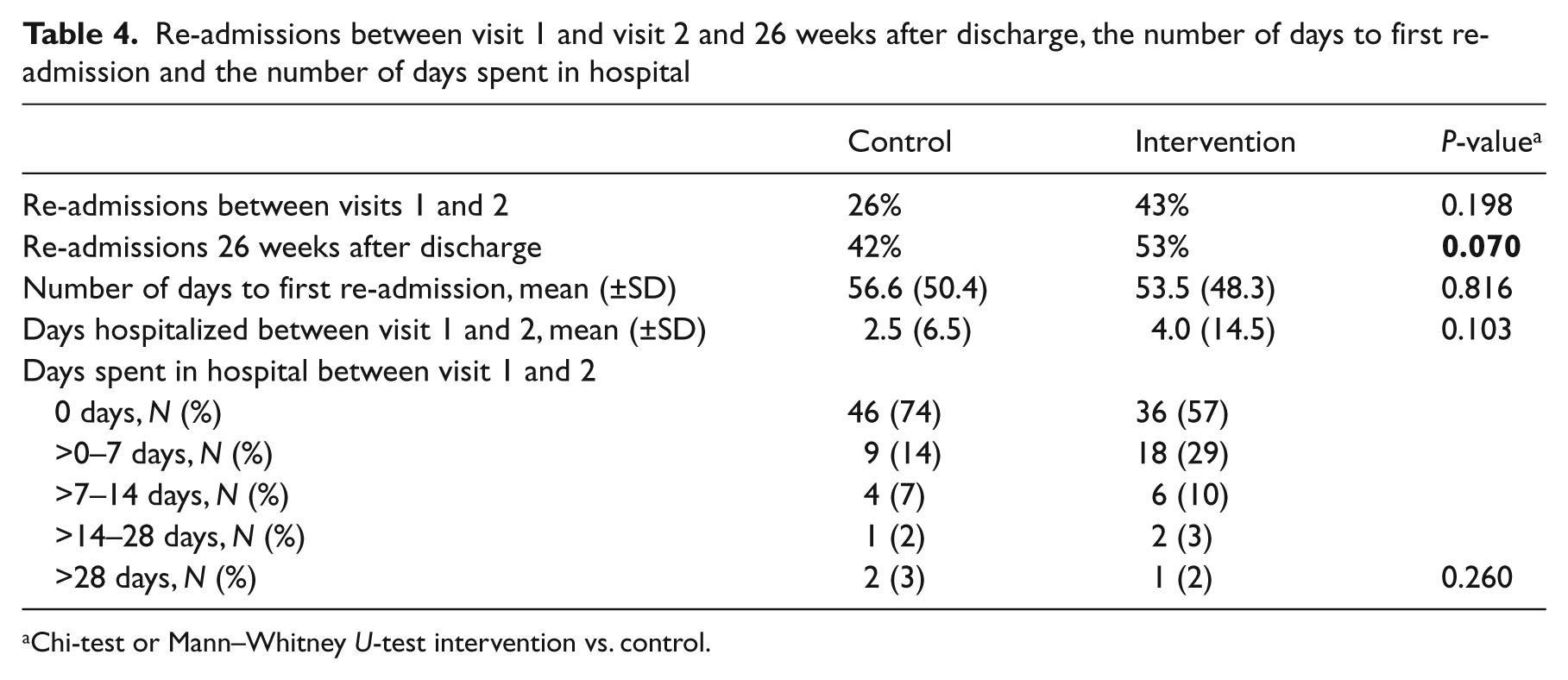
Chi-test or Mann–Whitney U-test intervention vs. control.
Data about the changes in functional and nutritional status, the use of supplements and social services at follow-up visit are presented in Table 5.
Effect on functional status, nutritional status, use of supplements and need of social services
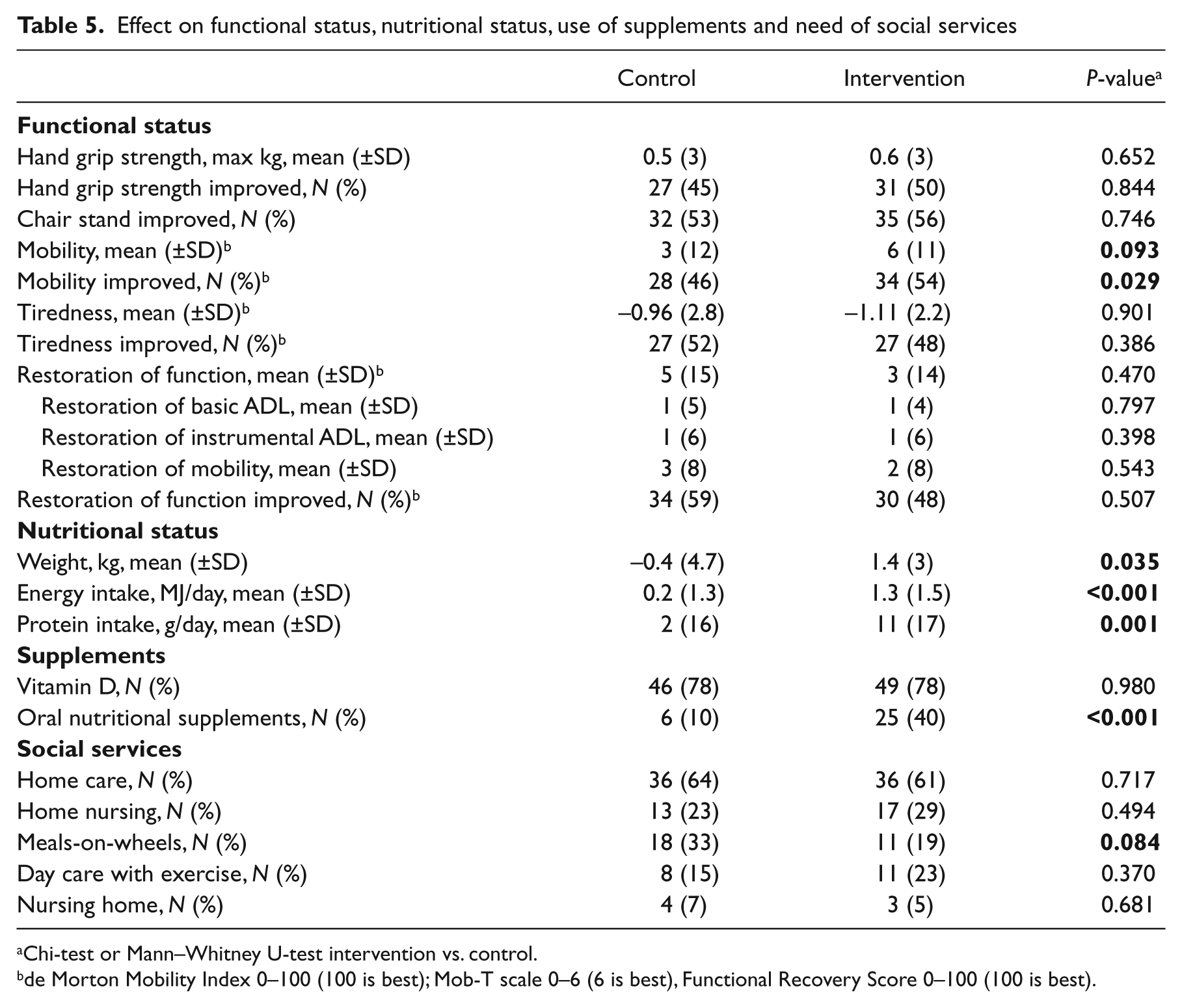
Chi-test or Mann–Whitney U-test intervention vs. control.
de Morton Mobility Index 0–100 (100 is best); Mob-T scale 0–6 (6 is best), Functional Recovery Score 0–100 (100 is best).
There was a general improvement in functional status in both the control and intervention group. There was a significant difference between the two groups in relation to the percentage who improved their mobility (54 vs. 46%, P = 0.029).
Nutritional status was unchanged in the control group but improved in the intervention group. There was a significant difference between the two groups in favour of the intervention, in relation to change in weight (P = 0.035), energy intake (P < 0.001) and protein intake (P = 0.001). Further, the intervention group had a significant higher intake of ONS (40 vs. 10%, P < 0.001).
With regard to social services, the intervention group had a reduced use of meals-on-wheels at the follow-up compared with the control group (P = 0.084).
Twenty-six weeks after discharge seven of the participants in the control group and four in the intervention group had died (9 vs. 6%, P = 0.314), odds ratio 0.60 (95% CI 0.17 to 2.13).
Discussion
In this study we found that individualized nutritional counselling by a registered dietitian in the geriatric patient’s home after discharge from hospital had a positive effect on functional status (i.e. mobility) and nutritional status (i.e. weight, energy and protein intake) but no effect on risk of re-admissions or mortality. The major strength of the study is the high compliance to the nutritional intervention. The major weakness is the low rate of visiting by the GPs, contrary to the protocol which required a higher rate of visiting. Our intervention was not able to reduce the risk of re-admission or mortality rates. The most likely reason is that this study lacked power in terms of participant numbers and had a follow-up time that was too short.
This was also the conclusion in a systematic review of the benefits of oral nutritional support of older patients after discharge from hospital, 4 where the odds ratio for re-admissions and death were, respectively, 0.80 (95% CI 0.46 to 1.39) and 1.07 (95% CI 0.71 to 1.61).
Compared with the previous study using discharge follow-up in the patient’s home by GPs, 5 the compliance of the GPs in the present study was very low. The reason for this difference is unknown since the GPs were paid for the follow-up visits/contacts in both studies.
More GPs were involved in the participants in the intervention group (42 vs. 59%, P = 0.099). Also, 16 of the registered dietitian contacts were together with the participant’s GP (see Table 3). Hence, the increased risk of re-admissions (1.62 (95% CI 0.85 to 3.10) might actually have been due to a closer follow-up of the patients.
In light of the increased risk of re-admission in the intervention group, we were still able to achieve a positive effect on functional status and nutritional status. One explanation might be the very high compliance with the nutritional intervention (see Table 3).
Previous nutritional intervention studies among geriatric patients after discharge have all used commercial oral nutritional supplements and the drop-out rate has been up to 44%, especially among medical patients. 4 Therefore we decided to use a more comprehensive approach to nutritional therapy, combining individual education, motivation and counselling, dietary modification and supplementation offered by a registered dietitian. In spite of the comprehensive approach the intervention was not very time consuming, averaging 2 hours per visit. That dietary counselling given with or without ONS is effective in increasing nutritional intake and weight is supported by a recent meta-analysis by Baldwin and Weekes. 14 Unfortunately, these authors found that there were insufficient data on functional outcomes to make any consistent conclusions. 14
Strength training is an effective intervention for improving physical functioning in older people. 15 In Denmark it is part of the legislation to offer eligible patients rehabilitation in the form of physiotherapy. Therefore it was decided not to include training as a specific part of the comprehensive intervention, but instead register any difference between the two groups in the prevalence of participants discharged to day care with exercise. As shown in Table 2, there were no differences between the groups.
Our study suffers from some weaknesses. For example, it was not possible to blind the scientific research assistants who gathered the data in the participants’ home at the first and second visit. Also, the dietary record method used has not been validated in this population. However, as can be seen from Table 5 the control group did not increase their nutritional intake and kept a stable weight while the intervention group increased both. Furthermore, only in around 10% of the dietary records the calculated ratio between energy intake and basal metabolic rate was below 1.1 (see Table 2). Both findings support the validity of the dietary recordings.
A total of 277 patients were found to be eligible for the study and invited to participate over an eight-month period. A large number (55%) accepted the invitation and of the 152 enrolled participants, only 24 (16%) withdraw their consent to participate. The majority of these withdrew before the first visit. The reason may be the timing of the inclusion, at the hospital, where potential participants were understandably preoccupied and anxious about their impending return to the community and therefore, when returning home, regretted their consent.
The high compliance in relation to the nutritional intervention and the positive findings compared to former studies, 4 is the major strength of our study, and supports the relevance of such an offer to geriatric patients at discharge. Future trials may benefit from a longer intervention period and more participants.
Clinical messages
Twelve weeks of follow-up home visits by registered dietitians have a positive effect on the functional and nutritional status of geriatric medical patients after discharge.
A larger study with a longer intervention period is needed to see if there is a positive effect on risk of re-admission and mortality.
Footnotes
Authors’ contributions
AMB initiated the study, designed it, monitored progress and decided on analytic strategy. BSH, SK, RLS, KT-J, were responsible for carrying out the study and collecting the data. AMB drafted the manuscript and BSH, SK, RLS, KT-J and CB critically reviewed and contributed to drafts. All authors read and approved the final manuscript.
Trial registration
ClinicalTrials.gov 2010 NCT01249716.
Conflict of interest
The authors declare that they have no competing interests.
Funding
The project was funded by grants from the Health Insurance Foundation, the Tryg Foundation and the General Practitioners’ Foundation for Development of General Practice. These are all non-commercial founds and had no role in study design, or in the collection, analysis, interpretation and publication of the data. TDC provided cell phones for scientific research assistants and registered dietitians and, as the others, had no role in study design, or in the collection, analysis, interpretation and publication of data.