
Abstract
Objective:
To compare the effects of contralesional sensory cueing and limb activation with that of sham control in the treatment of unilateral neglect after stroke.
Design:
A randomized, single-blinded, sham-controlled pilot study.
Setting:
Two rehabilitation hospitals.
Subjects:
Forty subacute left hemiplegic stroke inpatients with unilateral neglect.
Interventions:
Participants were assigned randomly to 1 of 2 groups. The experimental group wore a wristwatch cueing device over the hemiplegic arm for three hours a day, five days per week, for three weeks, and also underwent conventional rehabilitation. Patients were encouraged to move their hemiplegic arm five consecutive times after each prompt. The sham group underwent the same rehabilitation process, except they wore a sham device.
Main measures:
Neglect, arm motor performance, and overall functioning were assessed pre- and posttraining, and at follow-up.
Results:
There were no significant differences between groups in outcome measures except the neglect drawing tasks (p = 0.034) (the mean gain score from baseline to follow-up assessment was 5.2 (3.7) in the experimental group and 1.9 (3.5) in the sham group), across three time intervals. The experimental group showed greater improvement in arm motor performance than did the sham group.
Conclusion:
The results did not confirm that sensory cueing and limb activation treatment is effective when compared with those receiving placebo to reduce unilateral neglect, but it might be useful for promoting hemiplegic arm performance in stroke patients.
Introduction
One common perceptual impairment caused by strokes is unilateral neglect, which varies in incidence from 13% to 81% in right hemisphere stroke patients. 1 Severe contralesional neglect occurs more often after right hemisphere lesion and is found to have serious effects on rehabilitation and functional recovery.2,3 One of the reasons of neglect was explained by the interhemispheric rivalry model of spatial attention, which says that the cueing of the hemispatial system over the ipsilesional side is inadequate on its own, even though spatial sectors in both hemispheres activate motion, and would result in a strong rightward spatial bias in right hemisphere stroke patients. 4
Recent literature shows that treatments for unilateral neglect fall under two types of behavioural approaches. They are either recruiting the hemiplegic side or limbs to reduce a spatial preference over the ipsilesional space, or improving awareness of the contralesional space to promote patients’ attention,5,6 Studies based on these two approaches have reported varying results, but some approaches appear to be more promising, which include ipsilateral eye patching,7–9 prism adaptation,10,11 voluntary trunk rotation,12,13 functional electric stimulation, 14 spatial cueing combined with hemiplegic limb activation, 15 and constraint-induced therapy. 16 Although these methods are effective, their effects are often task specific or transient and often cannot be generalized to daily functioning.4,17,18
One technique recently reported is sensory cueing therapy. One experiment used a neglect-alert device that had an automatic alert. 19 This device emitted a ‘loud voice’ to alert patients to their limb, and it was shown to help patients activate their affected limb when patients responded to the tone by making small movements with their left fingers or left foot to make the alarm stop buzzing. Two case studies showed that the device produced a temporary reduction in left-side neglect, however, the question of whether limb activation can effectively reduce neglect remains to be seen.20,21. One randomized controlled trial indicated that it improved hemiplegic motor function, but did not improve unilateral neglect. 22 Recently, a pilot study conducted by our team applying sensory cueing from an ambulatory wristwatch device on the voluntary use of hemiplegic hands revealed that a combination of sensory cueing and movement-based strategies was a useful and feasible treatment improving hemiplegic arm functions among participants with chronic stroke 23 or unilateral cerebral palsy. 24
The purpose of this study was to test the effects of a novel training – the combined contralesional sensory cueing and limb activation vs. a sham control in left hemiplegic patients with subacute stroke and unilateral neglect over a three-week period of daily training. We hypothesized that sensory cueing (vibration and auditory signals emitted from a new ambulatory wristwatch device tied to the wrist of the hemiplegic arm), followed by consecutive arm movements subsequent to the cues, when compared with those receiving sham treatments, was feasible and would promote patients’ awareness over their contralesional field, reduce unilateral neglect, and improve hemiplegic arm functions. Because sensory inputs are received from both sides of the body simultaneously, the interhemispheric rivalry between sensations resulting from unilateral neglect means the body only recognizes stimuli on the contralesional side; the proposed sensory cues emitted from the experimental device would thus promote the sensory afferent inputs from the contralesional side.
Methods
This is a multicentre, randomized, sham-controlled pilot investigation with blinded outcome assessment. Subacute inpatients with stroke were recruited by convenience sampling from two rehabilitation hospitals (Centres A and B) in Hong Kong. Principal inclusion criteria were: (i) cerebral vascular disease diagnosed by computed tomography scan or magnetic resonance imaging in a medical report and compatible with unilateral hemispherical involvement; (ii) evidence of unilateral neglect from neurological testing or Behavioural Inattention Test (BIT) conventional subtest score < 129; 25 (iii) right handed; (iv) within eight weeks after stroke; (v) able to understand verbal instructions and follow one-step commands; (vi) severe to moderate unilateral upper limb paresis, defined as levels 1–5 in the Functional Test for the Hemiplegic Upper Extremity (FTHUE) 26 with the range of some beginning voluntary motion of the hemiplegic shoulder and elbow to beginning ability of the hand to combine components of strong mass flexion and strong mass extension patterns. Eligible participants were excluded if they had: (i) significant impairment in visual acuity caused by cataracts, diabetic retinopathy, glaucoma, hemianopia, and so on, or (ii) a history of other neurological diseases, psychotic disorders, or alcoholism.
The sample size of this study was estimated with reference to a pooled analysis of four studies8,12,27,28 using line bisection in a recent Cochrane’s review of spatial neglect following stroke. 18 By assuming 80% power at 5% Type I error for one-tailed test, 19 subjects were needed per group to detect significant between group differences with a large effect size of 0.84 after immediate treatment (G*power, Version 3.1.3, University of Kiel, Germany, 2010).
Patients were randomly assigned to either the experimental group or the sham control in the two occupational therapy departments using computerized random number generators according to random permuted blocks of four. Allocation-to-treatment sequences were concealed from all investigators responsible for carrying out the training or patients involved. The experimental group underwent conventional rehabilitation and wore the cueing wristwatch, which they were told should cue five consecutive movements. The devices included a built-in actometer that was designed to record the amount of arm movement in both horizontal and vertical directions.
The sham control group wore a sham device and was told to move as much as possible. Patients in this group underwent the same conventional rehabilitation process, except that their device had no cueing function. The sham device did still record the amount of arm movement. Both groups wore the device for the same period of time. They were told to move their arms as much as possible during the wearing period. In this study, sham devices were used rather than no treatment because even a non-active unit worn on the hemiplegic side might act as a cue to use that extremity and thereby confound any effects of sensory cueing. 29 In addition to the cueing device, patients participated in the conventional rehabilitation programmes, including occupational therapy, physiotherapy, speech therapy, and patient and family discussions with healthcare workers at the rehabilitation hospitals. These treatments did not specifically target unilateral neglect explicitly.
All tests were administered by a research assistant who was blinded to the group assignment. Assessments were carried out without any device present. All patients were tested one day before the treatment started and one day after the treatment ended. Each centre had its own independently trained occupational therapists to carry out the treatments according to the study protocol, but they were not blinded to the treatment conditions. Therapists were told to have their patients continue wearing the wristwatch devices during the treatment period. Participants gave informed written consent prior to data collection. The study was approved by the Human Ethics Committee of The Hong Kong Polytechnic University and two affiliated ethics committees of the Hong Kong Hospital Authority.
The only piece of equipment used in this study was a small ambulatory wristwatch device that was 30 mm(h) × 75 mm(l) × 50 mm(w) and weighed 91 g (as shown in the figure available online as supplementary material). The sensory cueing device was designed with neoprene straps to be worn on the left hemiplegic arm of stroke patients. It could be set to emit a vibration cue (196 Hz, similar to the vibration of a cell phone) supplemented by a simultaneous auditory signal (a buzzing noise at 67 dBA) at a predetermined time interval. The signal would go off for three minutes straight as long as its red de-activation button was not pressed. The wristwatch is charged by rechargeable batteries that give it a battery life of 30 hours if it is used every five minutes for three hours a day, five times per week. It also had a built-in actometer that recorded the amount of arm movement in both horizontal and vertical directions, with numbers appearing in the digital counter on the cover of the device. The participants in both groups were instructed to wear the device on the hemiplegic wrist daily for three consecutive waking hours (except bathing) during the daytime (e.g. 9 am to noon) over a three-week period, excluding Saturday and Sunday at hospital wards or therapy departments.
In the experimental group, patients had to press the acknowledgement button on the device with their right hand as soon as possible after each cue. Patients were told to follow every sensory cue with customary consecutive movements of their hemiplegic arm. They were instructed to perform the movement consecutively five times after each sensory cue. The cues came in intervals of five minutes for three hours. There were two kinds of customary movements tailored for participants according to the severity of their arm impairments: Patients in levels 3–5 of the FTHUE who had partial use of their shoulders or arms were instructed to flex or extend their elbows, while those in levels 2–3 of the FTHUE who had some voluntary motion of the shoulder were told to flex or abduct their shoulders. If they forgot to perform the tasks after cueing while a therapist was present, they were reminded by the therapists to continue.
First, information was collected on the participants’ demographic characteristics and medical history. The Mini-Mental State Examination was administered to all participants at baseline. 30 A blind assessor made the assessments at Week 0 (pretrainng), after Week 3 (posttraining), and Week 6 (follow-up). Primary outcome measures were selected that would provide results at four levels: unilateral neglect, arm impairments, arm functions, and basic functional performance. All of these scales have demonstrated good reliability and validity in Hong Kong samples. Unilateral neglect was assessed with the BIT. 25 The test is divided into two categories: the conventional and the behavioural subtests. This study used the conventional subtest, which is made up of six items: line crossing, letter cancellation, star cancellation, figure and shape copying, line bisection, and representational drawing. A cancellation subscore was calculated by adding the first three cancellation tasks together and a drawing subscore by adding the remaining three tasks. To measure arm impairments, this study used the upper extremity motor subscore of the Fugl-Meyer Assessment (FMA). 31 It has 22 items measured on a three-point scale with a maximum total score of 66. The total score can be further divided into upper extremity (shoulder and elbow) and hand subscores (wrist, grips, and coordination). Participants also took the FTHUE. The test was developed according to Brunnstrom’s developmental stages of stoke recovery according to a hierarchy of seven functional difficulty levels and it has been validated in Hong Kong by adding some culture-related items, like using chopsticks. 32 The Functional Independence Measure was used to measure basic functional performance. 33 In this study, only the motor subscale was used.
The secondary outcome measure in this study was the total counts of arm movement over the intervention period, which was calculated as the sum of the arm movements recorded daily as captured by the actometer for three weeks over the intervention period. Each therapist had a daily log to record the number of movements after the patient took off the device every day.
Data analysis
After removing dropout cases, all available data were analysed in an intention-to-treat analysis. The ‘last observation carried forward’ method was used; that is, if a subject dropped out, missing values were replaced by the last assessment score of that variable. Chi-square tests were used to test for demographic differences between Groups 1 and 2, and t-tests were used to analyse the differences in baseline functionality measures between the two groups. Between- (experimental vs. sham) and within-group differences over time in three repeated-measurement intervals (Week 0, 3, and 6) were evaluated using analysis of variance (ANOVA) for repeated measurements, with the baseline of each outcome measure entered as a covariate. Significance was set to 0.05 (two tailed).
Results
Figure 1 is a trial profile that indicates the number of participants recruited at different stages. From an eligible pool of 294 subacute inpatients (Centre A: n = 248; Centre B: n = 46), 40 inpatients (Centre A: n = 36; Centre B: n = 4) were selected by convenience sampling from two rehabilitation hospitals in Hong Kong. There were five dropouts in total, for a 12.5% dropout rate. The baseline characteristics were similar in the two groups, with no significant differences, except that there were more females in Group 2 and that the neglect cancellation tasks were in favour of Group 2 at study onset. Table 1 shows the demographic characteristics of the participants.
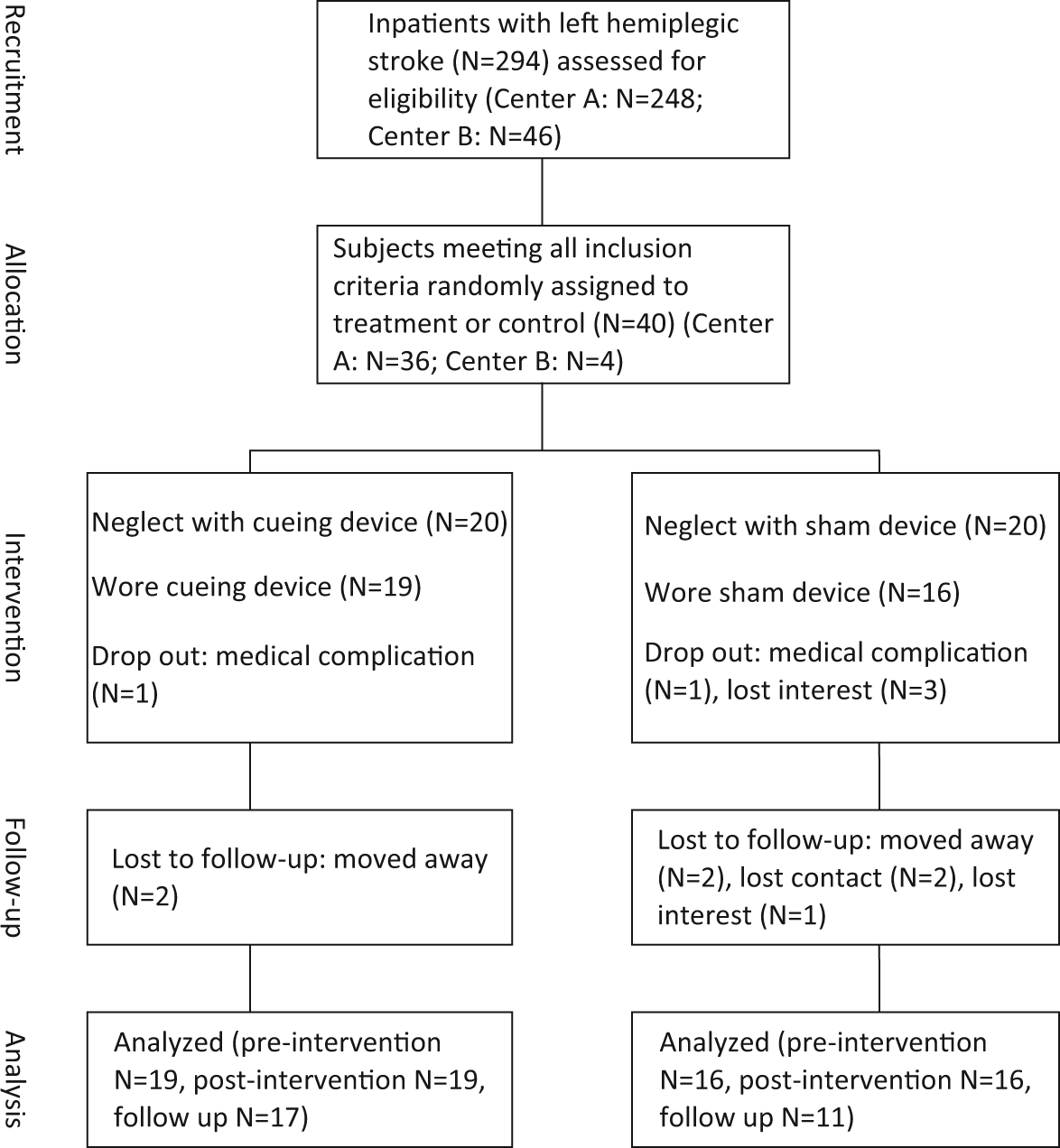
Trial profile showing the flow of participants.
Demographic baseline of participants.
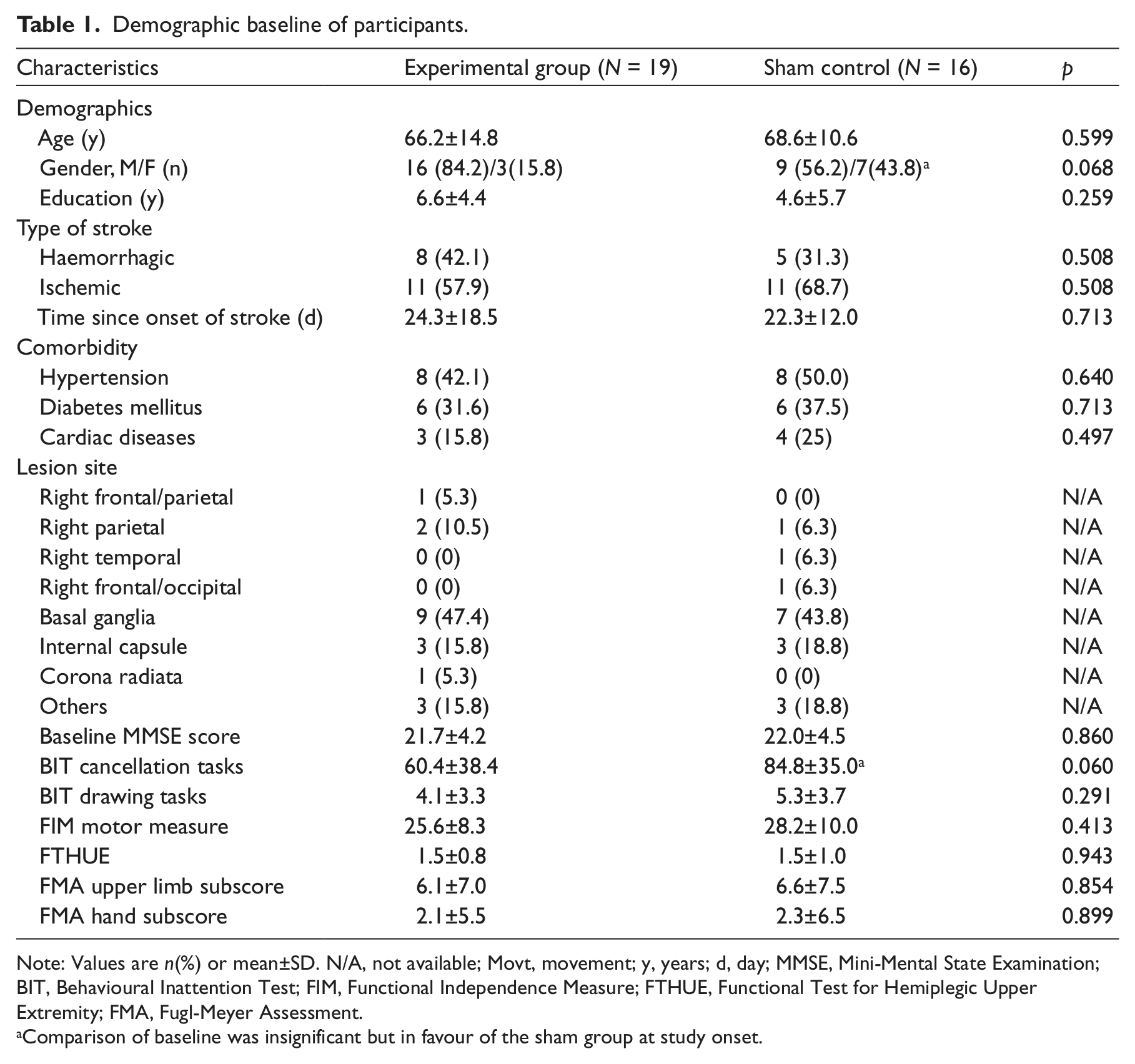
Note: Values are n(%) or mean±SD. N/A, not available; Movt, movement; y, years; d, day; MMSE, Mini-Mental State Examination; BIT, Behavioural Inattention Test; FIM, Functional Independence Measure; FTHUE, Functional Test for Hemiplegic Upper Extremity; FMA, Fugl-Meyer Assessment.
Comparison of baseline was insignificant but in favour of the sham group at study onset.
Table 2 reports the results of the differences in outcome measures at Week 0, 3, and 6. For between-group effects, there were no significant differences between the two groups across three time intervals except that the experimental group had overall significant higher scores on the BIT drawing tasks than Group 2 (F[1,32] = 4.91, p = 0.034). Posthoc analysis revealed significant within-group differences (when compared with baseline) in the Week 3 and Week 6 assessments for both groups. The percentage gains in the experimental group were 109.8% and 126.8% (compared with baseline) when compared with 49.1% and 35.8% for the sham group. Neither the group nor the group-by-occasion interaction effect was statistically significant in the neglect cancellation tasks, the Functional Independence Measure, the FTHUE, and the total score of Fugl-Meyer Assessment. Nevertheless, it should be noted that there were significant within-group differences in the FMA hand subscore in the experimental group, but not in the sham group, while the between-group differences were not statistically significant.
Differences in outcome measurements between groups at Week 0, 3, and 6.
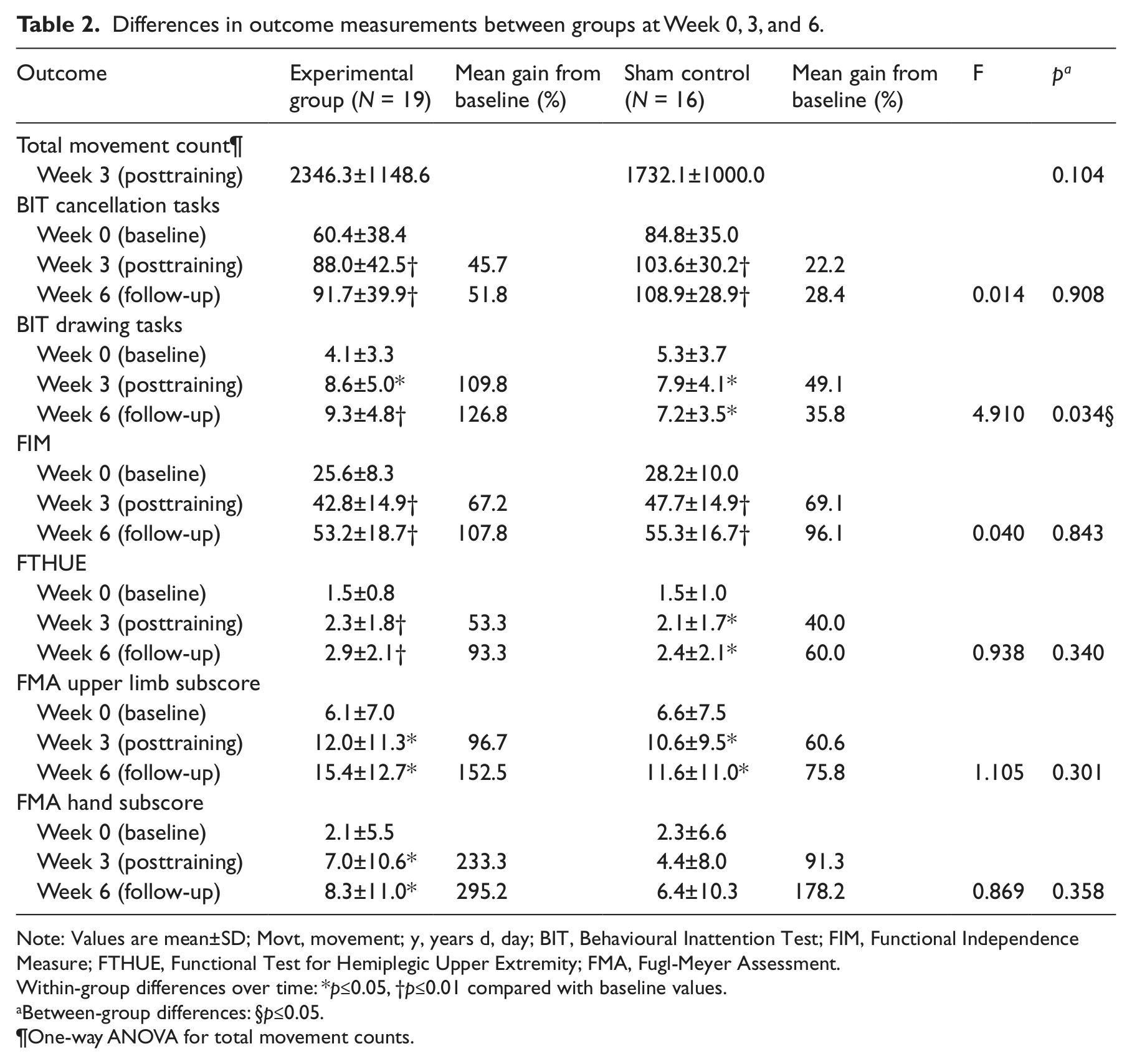
Note: Values are mean±SD; Movt, movement; y, years d, day; BIT, Behavioural Inattention Test; FIM, Functional Independence Measure; FTHUE, Functional Test for Hemiplegic Upper Extremity; FMA, Fugl-Meyer Assessment.
Within-group differences over time: *p≤0.05, †p≤0.01 compared with baseline values.
Between-group differences: §p≤0.05.
One-way ANOVA for total movement counts.
Regarding the mean total movements recorded by the wristband, the upper extremity movements in the experimental group were greater than that of the sham group after wearing the cueing device, but the difference did not reach statistical significance (p = 0.104). The mean gains from baseline in the BIT, the Functional Independence Measure, the FTHUE, and the FMA after intervention (Week 3) and at the Week 6 follow up were greater for the experimental group than the sham control, except for the Functional Independence Measure, which was similar between the two groups. The experimental group improved almost two times more than the sham group in the BIT and the FMA hand score. This difference persisted at Week 6 follow-up. In the FTHUE, for example, the experimental group improved 53%–93%, while the sham group gained 40%–60% (Table 2).
Discussion
Contrary to our expectations, the experimental group did not show significant improvements in all impairment and functional measures after training or at follow up, except that the experimental group showed significantly higher scores on the drawing tasks than the sham group. It is likely that spontaneous recovery occurs after a subacute stroke. Patients in both groups were encouraged to move their hemiplegic arm, but patients in the experimental group were primed by sensory cueing to move five consecutive times after each prompt. Although the total movement count was greater in the experimental group than that of the sham control, the difference did not reach statistical significance. It is unclear whether the positive effect on unilateral neglect in both groups was to be attributed to an increase in active motor output, proprioceptive input, or both, as limb movement itself can act as a cue to activate multiple spatial representations of the contralesional side. 14
The higher centres in the brain let emotional, attentional, and cognitive elements influence sensory inputs. Although individuals are continuously bombarded by incoming sensory stimuli from the environment, one only attends to the sensory cues when one chooses to do so, such as responding to one’s own cell phone. 34 In this experiment, a small device attached to the wrist was used that could cue patients with intensive sensory stimuli during their everyday activities. Sensory cueing would increase the patients’ awareness of their hemiplegic field, and promote patients to respond with repetitive movements when primed, leading to a better interhemispheric symmetry that would reduce unilateral neglect over their contralesional field, and improve hemiplegic arm motor performance. This novel approach is relatively safe and simple, which can be easily applied in a clinical situation, and requiring no extra time or costs to existing supervised therapy.
Unilateral neglect is a multifactorial, multifaceted syndrome that has two common manifestations. The first is spatial representation, which is the ability to form a whole representation of space, and usually extinction is said to co-exist when patients respond accurately to unilateral stimulation of the contralesional side, but consistently ignore bilateral simultaneous stimulation. 35 The second aspect of neglect is motor exploration, whereby patients conduct visual searches or oculomotor scanning with a covert bias to the ipsilesional side. 35 The results indicate that the treatment used in the experimental group brought about significant improvements in the neglect drawing tasks. When compared with the sham group, the treatment gains in the drawing tasks were more than double throughout the Week 3 and Week 6 assessments. Although the results were comparable with a previous limb activation study that found its neglect treatment was not as positive as predicted, 15 it is difficult to draw conclusions at this stage that sensory cueing and limb activation strategy used in this study may be more useful for reducing rightward spatial preference (the drawing tasks) than visual target detection (the cancellation tasks) as more control conditions and test variables would be necessary to discriminate specific attention and motor effects of the treatment.
Even though it was unclear whether sensory cueing and limb activation could help patients with neglect improve their hemiplegic arm function, it is interesting to note that patients with and without neglect increased their arm movements, especially in the wrist and hand as measured in the FMA hand subscore. This improvement was significant in the experimental, but not the sham group. Extinction caused by neglect of the left side of the body results in under or nonuse of the hemiplegic upper extremity, which decreases the general activation of the perceptual motor attentional circuits in the damaged hemisphere. As shown by the mean movement counts in the digital counter of both the experimental and sham devices, sensory cueing promoted more arm movements. We speculate that the increase in amount of arm movement practice was associated with improvement in their hemiplegic extremity. This observation further supports the findings reported in a previous study on chronic post-stroke patients. 23 Further study is warranted to find out whether this reinforcement in intensive practice from sensory cueing can overcome nonuse of hemiplegic upper extremity for patients in their daily life.
However, this study did not support the use of sensory cueing and limb activation to improve overall functional performance as measured by the Functional Independence Measure in subacute patients with unilateral neglect. The effect was comparable in both groups of patients; patients with neglect only made functional gains after conventional rehabilitation services. This result is similar to those of Cochrane findings that found that neglect interventions improve performance on some impairment level tests, but their effect on disability is unclear. 18 Patients with neglect have lower Functional Independence Measure scores than patients without neglect, and neglect is a major predictor of functional outcome from admission to follow up in inpatients with left hemiplegic stroke. 36 Although different behavioural approaches or theory-driven methods to treat neglect have been developed in the last decade, recent reviews were unable to find which approaches were most useful.5,6,18,22 Future research efforts should be taken to develop behavioural interventions that have generalized effects into activities of daily living and that endure over much longer periods of time.
This study was quite rigorous in that it was a single-blinded randomized trial at two trial sites with a sham control of a sensory cueing device and not usual care, but it is still subject to a few limitations. For one, the small sample size and dropouts meant that the study did not reach its estimated power. It would be helpful to replicate this study with a larger sample size and incorporate patients with left hemisphere lesions. Also, the uneven group sizes could have limited the capacity to detect differences between groups. Although we believed that the gender differences did not bias the results, the better score of the sham group in the neglect cancellation tasks might have made it more difficult for the experimental group to reach a statistically significant result on that score. The study cannot be excluded that a sham device itself is a cue to promote patients’ awareness over their contralesional field. Therefore, it would have been interesting to include a third group that undergoes conventional rehabilitation only, as pure controls. Furthermore, this study only examined treatment effectiveness up to three weeks after treatment ended because this is the average length of stay of inpatients in rehabilitation hospitals. That means we still do not know whether longer treatment can achieve bigger reductions of neglect and enduring arm motor performance. Future studies should consider different protocols, including alternative wearing regimens, in order to maximize the treatment effects.
In conclusion, this randomized, sham-controlled pilot study failed to confirm that the sensory cueing treatment, in combination with limb activation, was effective when compared with those receiving sham control to reduce unilateral neglect, and it was noteworthy that sensory cueing might be able to promote hemiplegic arm motor performance in stroke patients with neglect. This study serve will help influence future studies of attention-driven training for hemiplegic arm recovery.23,24 A prospective randomized controlled study is required to determine the beneficial role of sensory cueing treatment in combination with limb activation for hemiplegic arm in non-neglect stroke patients.
Clinical messages
The use of sensory cueing and limb activation—relative to the sham treatment—was not effective in reducing unilateral neglect in subacute left hemiplegic stroke patients.
The usefulness of sensory cueing treatment in combination with limb activation strategy for promoting hemiplegic arm functions needs further exploration.
Footnotes
Acknowledgements
Part of the material in the manuscript was presented at the 4th World Congress of the International Society of Physical and Rehabilitation Medicine on 10–14 June 2007 in Seoul, Korea.
Conflict of interest
The authors declare no conflicts of interest with respect to the authorship or publication of this article.
Funding
This work was wholly supported by research grant A-PA4Q and A-PJ36 from The Hong Kong Polytechnic University, Hong Kong.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.