
Abstract
Objective:
To explore individuals’ experiences of receiving either standard care or comprehensive cardiac rehabilitation post minor stroke or transient ischaemic attack.
Design:
A qualitative study using semi-structured interviews, alongside a randomized controlled trial, exploring the effectiveness of comprehensive cardiac rehabilitation compared with standard care. Interviews were transcribed verbatim and subjected to thematic analysis.
Setting:
Individuals’ homes.
Subjects:
People who have experienced a minor stroke or transient ischaemic attack and who were partaking in a secondary prevention randomized controlled trial (6–7 months post the event, 17 males, five females; mean age 67 years).
Interventions:
Not relevant.
Main measures:
Not relevant.
Results:
Four themes were identified: information delivery, comparing oneself with others, psychological impact, attitudes and actions regarding risk factor reduction. Participants indicated a need for improved information delivery, specific to their own risk factors and lifestyle changes. Many experienced psychological impact as a result of their minor stroke. Participants were found to make two types of social comparison; the comparison of self to another affected by stroke, and the comparison of self to cardiac patients.
Conclusion:
Comprehensive cardiac rehabilitation was reported to have positive effects on people’s motivation to exercise. Following a minor stroke, many individuals do not recall information given or risk factors specific to them. Downward comparison with individuals who have had a cardiovascular event led to some underplaying the significance of their minor stroke.
Introduction
Twenty thousand people experience a minor stroke or transient ischaemic attack (TIA) in England every year. 1 Although all symptoms are fully resolved within 24 hours post TIA, patients with a minor stroke will be often be left with residual physical, cognitive or visual deficits. 2 However, despite a good physical recovery, the risk of future vascular events remains high after a minor stroke 3 with coronary heart disease (57%) and cerebrovascular disease (36%) being the most common cause of death for this patient group. 4 Thus, rehabilitation may be of benefit to effect lifestyle changes and reduce risks of further cardiac and cerebrovascular events.5–7 However, there are no programmes specifically designed for people who have suffered a minor stroke.
Risk factors for cerebrovascular disease are broadly similar to those identified for cardiovascular disease 8 with similar age profiles and incidence levels for both cardiac and cerebrovascular events. 9 However, there are considerable differences in the secondary preventative programmes offered to those with cardiac disease or a minor stroke. 10 Cardiac patients are commonly offered a comprehensive cardiac rehabilitation programme, which has been proven to improve risk-factor profiles, slow disease progression 11 and reduce cardiac mortality and all-cause mortality. 12 Further, lifestyle changes have been reported to influence modifiable risk factors for cerebrovascular disease.13–20 Nevertheless, uptake of rehabilitation among cardiac patients is suboptimal. 21 To date, the impact of comprehensive cardiac rehabilitation on secondary prevention has been evaluated in more severe stroke, but not in minor stroke.10,22 A recently completed trial in Southern England investigated whether comprehensive cardiac rehabilitation is more effective than standard care in improving secondary disease prevention for patients post minor stroke (UKCRN ID 7348). It is essential to explore how such programmes are perceived by people with minor stroke. This study was therefore conducted alongside the aforementioned trial, to explore patients’ experiences of receiving standard care or taking part in comprehensive cardiac rehabilitation.
Methods
This study employed a qualitative methodology comprising semi-structured interviews, conducted by two of the researchers (KH and HK). As little is known about patients’ experiences of rehabilitation programmes after a minor stroke or TIA it was considered more appropriate to use a qualitative study than a questionnaire-based design. In addition, qualitative approaches allow a more in-depth exploration than quantitative designs. 23 The interview guide (Table 1) was used flexibly, enabling participants the freedom to express themselves. Interviews were audio-taped and transcribed verbatim.
Interview guide.
TIA, transient ischaemic attack.
Access
All participants in the trial were invited to take part in the qualitative study by the independent assessors of the trial research team, one month after conclusion of the randomized controlled trial (RCT) itself (after the last assessment 6–7 months post minor stroke). The initial RCT information sheet also contained information about the qualitative study and trial participants had another opportunity to ask any questions about the interviews when invited at the end of the trial. Trial participants had been recruited via TIA outpatient clinics and stroke services in Hampshire (Southern England). People with minor stroke were included in the RCT if they had a diagnosis of TIA (resolution of symptoms <24 hours of onset), or minor stroke (a National Institute of Health Stroke Survey score of <3), 24 no previous experience of cardiac rehabilitation, lived within the geographic locality covered by the local Cardiac Rehabilitation Team, and were aged 18 years or older. An additional inclusion criterion for the qualitative study was the ability to participate in semi-structured interviews without the need for an interpreter. Those with significant speech impairment or significant cognitive impairment (Mini Mental Test score <7 25 ) affecting their ability to give consent were excluded. The trial interventions (control group: standard care – experimental group: comprehensive cardiac rehabilitation) are depicted in Appendix 1 (available online).
Procedure
Interviews took place predominantly in participants’ homes and a small number chose to be interviewed in the research offices at the hospital. Interviews lasted on average 45 minutes. Families and carers were included in the interviews at the participants’ discretion, though all questions were directed at the participant.
Data analysis
Thematic analysis was conducted using the procedural steps described by Braun and Clarke. 26 Initially, each data set was analysed separately by the lead author (KH). This involved close reading of each transcript line by line, identifying and coding interesting features. Six coded transcripts were independently reviewed by members of the team and alternative interpretations were documented and discussed. A second round of peer review was used in which colleagues reviewed the collated codes. Any discrepancies regarding these codes were discussed in subsequent meetings and any necessary refinements were made. This process of multicoding encourages thoroughness and helps to enhance rigour in qualitative research. 27 The interpretation of the analysis was not checked with study participants as this may have led to additional burden over and above what was already required from participants both for the trial and the qualitative component. In addition, member checking is challenging, for example when participants change their views over time or feel exposed by the analysis. 28 Data analysis continued until data saturation was evident.29,30 For this purpose we aimed to recruit between 15 and 30 people into the qualitative study. Illustrative quotes are provided with a participant number followed by a letter identifying group allocation (C = control group, E = experimental group). For ease of reading we will use the terms minor stroke hereafter to encompass both TIA and minor stroke.
Ethics approval was provided by Southampton and South West Hampshire Research Ethics Committee (REC number: 09/H0504/46) and participants gave informed consent.
Results
Twenty two people from the complete trial (out of a total of 24) agreed to be interviewed (response rate 92%; 17 men, five women; mean age 67 years, range 47–84; 12 randomized to standard care and 10 to comprehensive cardiac rehabilitation). Participants’ cerebrovascular events (nine minor stroke and 13 TIA) had occurred between July 2009 and April 2010 (Table 2).
Participant demographics.
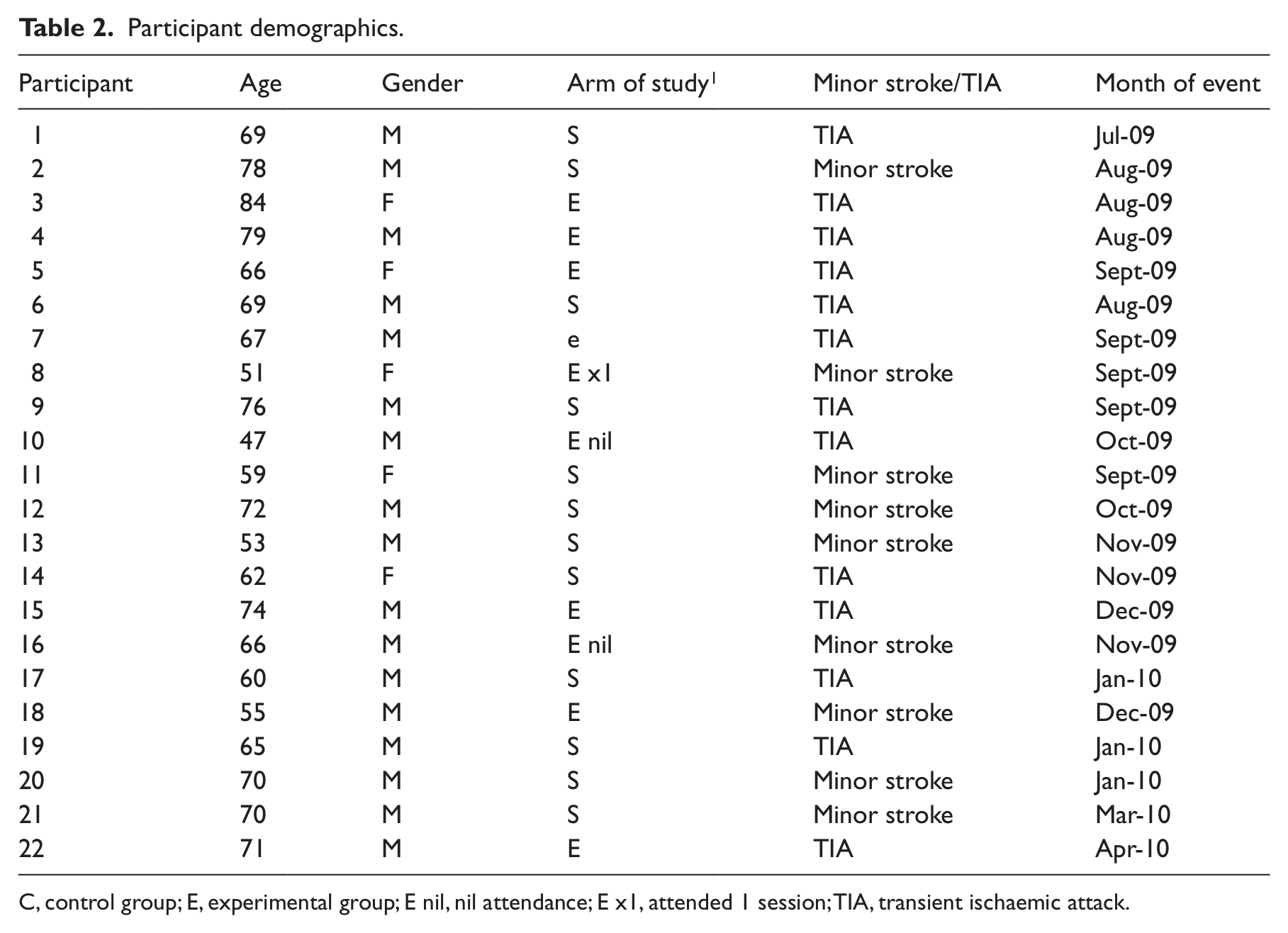
C, control group; E, experimental group; E nil, nil attendance; E x1, attended 1 session; TIA, transient ischaemic attack.
Seven patients in the experimental group attended all sessions, one person attended one session, and two people did not attend any sessions. Reasons for non-attendance included work commitments, dislike of the location of cardiac rehabilitation programme, and perceived self as too well. The majority of those who attended reported feeling satisfied with the service that they had received, that the sessions provided opportunity for socialisation, gave them a sense of comradeship, increased their confidence to exercise post minor stroke and enabled them to seek answers to questions that were either not asked or were insufficiently answered while receiving standard care. However, some also identified that committing to weekly rehabilitation classes was quite a burden and that the educational sessions were only partially relevant to their own circumstance or just vaguely informative. Notwithstanding, participants in the experimental group generally reported that their engagement in the programme improved their healthcare experience post minor stroke. Those that received standard care also generally reported feeling happy with the care that they received; some regarding their care as being first class and efficient, while others simply regarding it as being quite nice or difficult to fault. However, time pressures and lack of communication was a common criticism of standard care.
Data saturation was achieved in the analysis. Four themes were identified: information delivery, comparing oneself with others, psychological impact, attitudes and actions regarding risk factor reduction. These themes were at play in both the standard care and the experimental group and the results have therefore been combined in the following section.
Information delivery
The diagnostic period was identified to be a particularly stressful time by many respondents, impacting on their ability to recollect details of events and information they had received, and linking this with their own cerebrovascular event.
When you are diagnosed what it is, and you are told what it is and you think blimey … so to try and remember what happened at that TIA Clinic on Monday was, I can’t really (10E). I think we probably discussed the fact that it was a blood clot but never discussed what a TIA was, or what might have caused it, or anything like that, no (06S). You know, it’s all right, very well having the test and someone say ‘that’s fine and then this is fine’, but they should be able to say how that affects you and this actual problem, you know (17S).
Several participants reported talking to their general practitioner, chatting to friends affected by stroke, sourcing literature and surfing the internet in an attempt to improve their knowledge of minor stroke. Those in the experimental group had further opportunity to develop their knowledge through the programme. Of these, four reported that the sessions improved their understanding of cardiovascular disease, possible causes and lifestyle modification. Others felt the sessions merely reinforced what was already known (e.g. regarding the dangers of smoking). One participant also noted difficulty recalling the information that was pertinent to cerebrovascular disease so felt his understanding of minor stroke had not improved. Hence, it was suggested more information on ‘the brain side’ (15E) should be included in the future.
Social comparison
Some compared themselves with others affected by stroke and considered themselves to be lucky compared with people with more severe stroke. This affected their views on preventative strategies: No, no, I’m certainly not worried by it. Uuum, only in so much that if I did have one, and it was far worse, and seeing some of the people that was in the Stroke Clinic, I mean, you know, that’s enough to make you try to, try to avoid having a, another one (13S).
However, two participants in the control group reported that the speed of their recovery made them feel like a fraud for accessing healthcare, hence they were concerned about utilising a bed unnecessarily and wasting health professionals’ time. Similarly, a speedy recovery made three participants in the experimental group feel that others (family and medical staff) were making a fuss unnecessarily.
I didn’t think there was much, much wrong with me, and they [TIA clinic] seem to be making a big fuss about it (07E).
Some participants in the experimental group compared themselves with cardiac patients. This contributed to one participant leaving the programme after attending only one session: I didn’t really want to keep going all the time because I felt as though I was more active than some of the people there … I also thought to myself that my slot could do for somebody with greater needs than me (08E).
Similarly, one person in the experimental group perceived minor stroke to be less significant and less harrowing than a cardiac event, affecting how he perceived the possibility of experiencing future cerebrovascular events: So I have never really been worried. I’ve had two attacks and a third one, um, unidentified. Ok, I may get another one, but if it’s like the others, then it’s all over (laughing) in a very short time, and so my attitude towards life in general is, now well, may happen, may not. It’s not as if I’m going to keel over and die (chuckles) because it’s not the heart (15E).
Psychological impact
Participants from both groups expressed a range of reactions to their experience of minor stroke. The majority expressed feelings of shock and disbelief. Some referred to a greater awareness of their own mortality and were frightened by this: I think I was more frightened of the fact that, I started to think of brain bleeds, and am I just going to die here without saying goodbye to my family, you know (08E). Probably two years down the line or something, it probably won’t be the same, but at the moment, any little problem I get, I think ‘Ooooh!’ you know! (18E).
A few reported experiencing minimal psychological impact owing to their symptoms resolving quickly, and two reported that, upon reflection, the minor stroke had a positive effect on their life because it made them prioritise their health: So I am glad it happened, cos it just, er, it, er, it woke me up and gave me a kick to sort myself out (10E).
Some reported feeling frustrated by their family and friends being over-protective and inhibiting their participation in daily activities: She even carries the shopping ‘Don’t you carry it, I want to carry it’. She makes me feel like an invalid (07E).
Consequently, support and education for the immediate family was identified as an unmet need. It was felt this would improve people’s knowledge of minor stroke and recovery, and would help families deal with the psychological impact of a family member having had a minor stroke.
Participants also spoke of their own need for psychological support and some were grateful to be given the opportunity to talk about their experience of minor stroke as part of the research, with someone other than family and friends.
It’s still good to come back to the time and just talk about how it happened and what it meant … especially when family, friends don’t understand exactly what a – never heard of a TIA (10E).
Participants felt a follow-up appointment with the TIA clinic should be offered as part of standard care as a forum for reviewing health and discussing queries: I think if you had a follow up, it would give the patient, an inkling yourself; a bit more confidence that everything was going OK (09S).
Attitudes and actions regarding risk factor reduction
Some reported disbelief that there are known risk factors or that changes in lifestyle can reduce such factors. Others said that ill-health was non-preventable and that minor strokes just happen. For example, one participant whose risk factors included hypertension, hyperlipidaemia, excessive alcohol consumption and a significant family history of cardiovascular and cerebrovascular disease said: I don’t think it necessarily follows that, if you stay in trim and do a lot of exercise, it’s still going to make any difference you know, if it’s in the genes as such (13S).
Another participant, who was a smoker, reported that healthcare professionals blame minor stroke on people’s vices: You know, if you’re a smoker, it’s smoking, if you’re a non-smoker and you’re fat, they’ll put it down to obesity! … If you’re thin and don’t smoke, right! They put it down to something else (17S).
Consequently, some continued undesirable health behaviours: I walk into town sometimes, but very rare. I shouldn’t see why I should walk when I got a car! Which I know is stupid! But I’m like that (16E).
By contrast, some were aware that minor stroke is a risk factor for future stroke and so perceived it as a warning to change their lifestyle: It’s amazing in hindsight you think, ‘well yeah’, I knew I wasn’t, eer, exercising enough, I knew I wasn’t eating properly at times, so. So, yeah, it was, it was worthwhile, shall we say, yeah, in terms of the warning that it gave me yeah (10E). I try and go to work with a lunch box which I’ve never done before. You know, full of fruit and er, proper sandwiches and that sort of things, yeah (10E).
Some suggested that the lifestyle advice should be more specific and directive: Yeah, I mean, if they turned round and said ‘You really, really ought to lose – er, to lose a little bit more weight’ then, then I’d obviously do something about that. But, unless somebody specifically says it, well you feel, well, you know, I don’t think I’m doing badly (13S).
Discussion
This study provides unique insights into participants’ experiences of standard care and comprehensive cardiac rehabilitation following minor stroke. One limitation of this study was that it recruited people who were partaking in a randomized controlled trial. The nature of such studies excludes many people since they may not meet strict inclusion criteria or choose not to take part in a study in which they have 50% chance of not receiving a new intervention. 31 Future research should explore views of people not included in a trial, including those with poor English, with significant speech impairment, or with significant cognitive impairment (with support from translators, family or close others, and speech and language therapists).
The results suggested poor recall of information received and that information was often not specific enough to individuals’ own situation. In addition, some disregarded information about known risk factors for minor stroke or that lifestyle changes can reduce such factors. This finding concurs with the conclusion from a recent systematic review of information provision strategies aimed at improving outcomes for stroke or TIA patients, which showed that information provision in itself results in only small benefits in relation to patient/carer knowledge. 32 This review also found that programmes that used an active approach (e.g. classes, personalised records, workbooks) were more effective than passive programmes (e.g. copy of notes, information packs) in improving patients’ depression and anxiety. In our study, those in the control group received information using a passive approach, while those in the experimental group received information using an active approach, though this was not stroke specific. Consequently, more information on the cause of the minor stroke and what actions to take in order to reduce cardiovascular risks were raised as important issues by participants in the experimental group. More patient-centred approaches in rehabilitation may be better suited to this population and result in better psychological outcomes. 33 It is possible that information, provided in a way that people can really understand and act upon the knowledge gained 34 and within a model that helps people address and deal with barriers and facilitators to changing health behaviours,35–37 would prove a more effective means of changing behaviours. This warrants further exploration in programmes for the secondary prevention of stroke.
This study also highlighted that some participants compared themselves with others with stroke or cardiovascular disease, in both groups. Downward comparison occurs when individuals compare themselves to others who are deemed as socially or personally worse off, while upward acts in the opposite direction. Both comparison types can lead to people viewing their situations in a more positive way. 38 In our study, the tendency was for participants to downwardly compare, resulting in feelings of relative well-being. Arguably, for one individual, this act of downward comparison contributed to her decision to leave the experimental programme. For another, it seemingly led to the perception that minor stroke is less traumatic than a cardiac event. It is possible that the psychological impact of the minor stroke played a part in this downward comparison as it has been suggested that negative emotional states need to be addressed before active problem-directed strategies, such as information-seeking about how others cope with their disease, can take place.39,40 Studies have shown that peer support can help individuals to make sense of their condition, increase their confidence post event, and develop an awareness of self-management skills.41–44 However, participants in our experimental group were often the only minor stroke patient within a class and so had limited opportunity to share their experiences with fellow minor stroke sufferers. This may have hindered their ability to develop their knowledge of minor stroke. Notwithstanding, comprehensive cardiac rehabilitation was found to have positive effects on people’s motivation to exercise: camaraderie of the group, approachability of staff and supervision during exercise were found to be influencing factors. This is similar to findings from studies exploring cardiac patients’ experiences of cardiac rehabilitation.45–47 Thus, there is a need to further evaluate the benefits of secondary prevention rehabilitation programmes specific for minor stroke.
Clinical messages
Patients want a greater understanding of their minor stroke and the risk factor specific to them than is currently provided.
Comprehensive cardiac rehabilitation was reported to have positive effects on people’s motivation to exercise.
Comparison with individuals who have had a cardiovascular event can lead to some people underplaying the significance of their minor stroke.
Footnotes
Acknowledgements
We are grateful to the participants for giving their time to this study, the research nurse at the Wellcome Trust Clinical Research Facility, the stroke team at Southampton General Hospital, the cardiac rehabilitation nurses at Solent Healthcare and Grace Aubrey for providing feedback on the data analysis.
Contributors
HK and PK conceived the qualitative study, PK provided supervision to KH, data analysis was led by KH and HK, the manuscript was drafted by KH and PK and approved by all authors.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This qualitative study was funded by the Private Physiotherapy Education Foundation. The funders played no role in the design or implementation of the study. Similarly the funders were not involved in the production of this article. The trial was funded by the Physiotherapy Research Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.