
Abstract
Objective:
To determine if segmental muscle vibration and botulinum toxin-A injection, either alone or in combination, reduces spasticity in a sample of patients with multiple sclerosis.
Design:
Single-blind, randomized controlled trial.
Setting:
Physical medicine and rehabilitation outpatients service.
Subjects:
Forty-two patients affected by the secondary progressive form of multiple sclerosis randomized to group A (30 minutes of 120 Hz segmental muscle vibration over the rectus femoris and gastrocnemius medial and lateral, three per week, over a period of four weeks), group B (botulinum toxin in the rectus femoris, gastrocnemius medial and lateral and soleus, and segmental muscle vibration) and group C (botulinum toxin).
Main measures:
Modified Ashworth Scale at knee and ankle, and Fatigue Severity Scale. All the measurements were performed at baseline (T0), 10 weeks (T1) and 22 weeks (T2) postallocation.
Results:
Modified Ashworth Scale at knee and ankle significantly decreased over time (p < 0.001) in all groups. Patients in group C displayed a significant increase of knee and ankle spasticity at T2 when compared with T1 (p < 0.05). Fatigue Severity Scale values in groups A and C were significantly higher at T0 [A: 53.6 (2.31); C: 48.5 (2.77)] than at either T1 [A: 48.6 (2.21); p = 0.03; C: 43.5 (3.22); p = 0.03] or T2 [A: 46.7 (2.75); p = 0.02; 42.5 (2.17); p = 0.02], while no differences were detected in group B [T0: 43.4 (3.10); T1: 37.3 (3.15); T2: 39.7 (2.97)].
Conclusion:
Segmental muscle vibration and botulinum toxin-A reduces spasticity and improves fatigue in the medium-term follow-up in patients with multiple sclerosis.
Introduction
The wide variety of symptoms in multiple sclerosis include spasticity, which may cause disability. 1 Disability resulting from spasticity is mainly the result of gait disorders, spasms, pain and fatigue, with increased levels of disability being associated with higher Ashworth Scores. 2 Spasticity in multiple sclerosis patients needs to be carefully assessed and treated as this symptom negatively affects walking performances, 3 as well as general mobility and balance. 4
Intramuscular injections of botulinum toxin A have been shown to effectively treat spasticity in multiple sclerosis patients, 5 especially when associated with early mobilization and physical therapies. 6 Botulinum toxin represents an effective treatment option for focal spasticity in multiple sclerosis, particularly for treating adductor spasticity, pes equinus, striatal toe and adductor spasticity of the shoulder joint. 7 However, it has been suggested that botulinum toxin may increase fatigue in multiple sclerosis patients. 8 Moreover, it has yet to be fully clarified whether it represents a cost-effective treatment. 7
Recently, segmental muscle vibration was proposed as a new therapeutic modality for the treatment of focal spasticity in post-stroke patients. 9 Briefly, it’s a technique that applies a low-amplitude/high-frequency vibratory stimulus to a specific muscle using a mechanical device. It induces the generation of Ia inputs by activating muscle spindle primary endings. 10 The Ia inputs activated by segmental muscle vibration can alter the excitability of the cortico-spinal pathway 11 by modulating intra-cortical inhibitory and facilitatory inputs to the primary motor cortex. 12 No data are yet available on the effectiveness of segmental muscle vibration on spasticity in multiple sclerosis patients. Owing to its modulating effects on cortico-spinal plasticity, we hypothesize that segmental muscle vibration may reduce spasticity in multiple sclerosis patients.
We therefore designed a single-blinded randomized controlled trial in order to verify the ability of segmental muscle vibration, either alone or combined with botulinum toxin A, to reduce spasticity in a sample of multiple sclerosis patients.
Materials and methods
Men and women affected by multiple sclerosis, according to the McDonald criteria, 13 were included in the study. The inclusion criteria were as follows: age 18–65 years, secondary progressive disease course, functional level ≥2 and ≤6 as assessed by the Kurtzke Expanded Disability Status Scale, 14 spasticity scores in the lower limbs ≥2 points as measured by the Modified Ashworth Scale, 15 anti-spastic/anti-epileptic treatment stable for at least three months prior to study entry and, lastly, written informed consent.
Patients were excluded if they presented one of the following: history of previous orthopaedic surgery to lower limbs; history of neurological disorders other than multiple sclerosis; any psychiatric disorders or severe cognitive impairment that could preclude safe participation in the study; pregnancy or breastfeeding; known history of alcohol or substance abuse; previous botulinum toxin type A injections or treatment with segmental muscle vibration.
The study protocol was approved by the local ethics committee. The experimental protocol was explained to the participants and their informed consent was obtained. Participants who satisfied the eligibility criteria were enrolled and then randomly assigned in a 1:1:1 ratio, using simple block randomization in groups of four, to group A (segmental muscle vibration group), group B (botulinum toxin A + segmental muscle vibration group) or group C (botulinum toxin A group) by an independent person who selected a sealed envelope 30 minutes before the intervention was due to start. All the participants underwent a clinical evaluation before the training started (T0), four weeks after the end of the training period (T1: 10 weeks postallocation) and three months after the end of the training period (T2: 22 weeks postallocation) (Figure 1). All the data were analysed by an independent assessor who was blinded to the randomization.
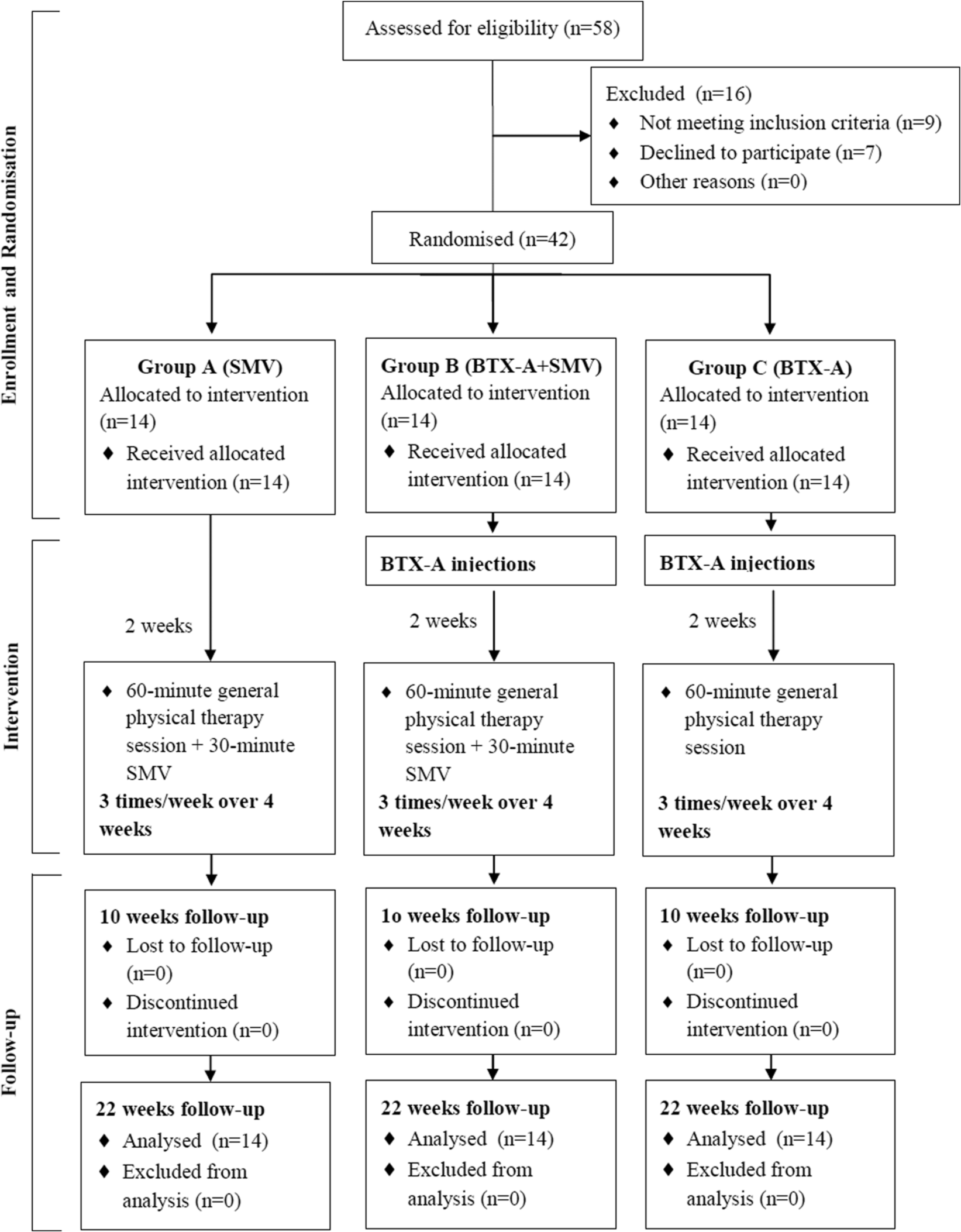
Flow-chart diagram of the study.
All the participants underwent a 60-minute general physical therapy session, three times per week, over a period of four weeks. These sessions involved regular activity designed to maintain muscle length through passive or active exercise, as well as a stretching regimen on the injected/vibrated area (40 minutes for each session), consisting of soft movements of joints with short pauses in the final position and reciprocal movements to prevent contractures and permanent shortening of muscles. Participants in Group C received an injection of botulinum toxin at least 15 days before the general physical therapy program started. Participants in groups A and B received a further 30 minutes of segmental muscle vibration therapy, which was delivered at the end of each general physical therapy session, with the patients lying supine. The botulinum toxin injection in group B patients preceded the general physical therapy and segmental muscle vibration program by at least 15 days. In order to allow homogeneity of timing of follow-up, in group A the treatment started 15 days after allocation (Figure 1). At the end of each therapy session, patients in groups A and B were orally interviewed and clinically evaluated in order to detect whether muscle pain or skin lesions (i.e. irritation, reddening, abrasions) had occurred.
All the patients agreed to receive the full course of treatment, which was performed in an outpatient facility, and to perform all the assessments as specified in the protocol. Caregivers also agreed to help the patient to comply with the study requirements if necessary.
Every patient in each of the three groups received a complete clinical evaluation that included evaluation of lower limb spasticity by means of the Modified Ashworth Scale, evaluation of fatigue by means of the Fatigue Severity Scale and independence in activities of daily living, as assessed using the Barthel Index.
The Modified Ashworth Scale grades the level of resistance encountered during manual passive stretching (score from 0 to 5, with 0 indicating no increase in muscle tone and 5 corresponding to joint fixed rigid in a position). In all patients, it was calculated for knee extensor and for ankle plantarflexor muscles on the more severely affected side. The Fatigue Severity Scale is a brief self-report measure of fatigue severity containing nine items. The score for each item ranges from 0 to 7, with higher scores indicating a more severe fatigue problem. 16 The Barthel Index is a self-scoring scale consisting of 10 items concerning fecal and urinary incontinence, and the need for help with grooming, toilet use, feeding, transfers, walking, dressing, climbing stairs and bathing. 17
Low-amplitude segmental muscle vibration at a fixed frequency of 120 Hz was delivered over the muscles belly of the target muscles, i.e. the rectus femoris and gastrocnemius medial and lateral, by means of a commercial device (Horus, Akropolis, Rome, Italy). The Horus is an acoustic-wave vibratory device composed of a control unit and three multiple probe transducers with four head transducers, each for the transmission of the vibratory stimulus. The acoustic production device, located in the control unit, generates an acoustic wave that is induced within the probe cavities and then translated into a vibratory stimulus within the transducer heads that are fixed to the body surface with elastic bands. The vibration amplitude was set at 10 μm, which is sufficient to drive Ia spindle afferents, 18 but avoids muscle fibre injury, 19 and is subthreshold for the tonic vibration reflex. 20 The 30-minute stimulation session was delivered in trains of six seconds divided by one-second pauses.
Botulinum toxin injections were administered to all the patients by the same well-trained neurologist who was unaware of group allocation. Botulinum toxin A (Botox; Allergan, Irvine, CA, USA) 100–300 U diluted (50 U/mL) was injected in the rectus femoris (three sites), gastrocnemius medial and lateral (three sites) and soleus (two sites). The dose was modified for less spastic muscles, though the total amount and the site of the botulinum toxin injections were similar in both groups. Injections were given under electromyographic guidance.
Statistical analysis
The statistical analysis was performed using the SSP 2.5 statistical package (Smith’s Statistical Package, version 2.75, 2004, Gary Smith, Pomona College, Claremont, California). Data normality was verified by means of the D’Agostino-Pearson test, and parametric or non-parametric analyses were performed, as appropriate. Repeated-measures analysis of variance (ANOVA) of Friedman ANOVA were used to determine changes over time of the outcome variables in the three groups. One-way ANOVA or Kruskal-Wallis (KW) test were used to determine differences at each follow-up between groups. The level of significance was set at p < 0.05 for all the analyses. A Bonferroni correction was used to correct tests for multiple analyses.
Results
A total of 42 patients were randomized (Figure 1) to group A (n = 14), group B (n = 14) or group C (n = 14). The demographic and clinical baseline characteristics of the three groups are shown in Table 1. No adverse effects were observed in any of the groups, and all the patients completed the treatment and performed the posttreatment assessments (Figure 1). Table 2 shows the clinical values in the three groups at T0, T1 and T2. The knee Modified Ashworth Scale scores (Table 3) significantly changed over time in group A (χ2r = 17.17; degrees of freedom (DF) = 2; p < 0.001), in group B (χ2r= 63.27; DF = 2; p< 0.001) and in group C (χ2r = 15.43; DF = 2; p< 0.001). Post-hoc analyses revealed significant differences (p < 0.05) in all three groups between T0 and T1 and between T0 and T2. Moreover, the knee Modified Ashworth Scale scores were significantly higher (p < 0.05) at T2 than at T1 in group C alone, though no differences were detected between groups at either T1 (KW = 2.41; DF = 2; p = 0.26) or T2 (KW = 2.3; DF = 2; p = 0.29).
Demographic characteristics of the three groups at baseline. Side indicates the most affected side.
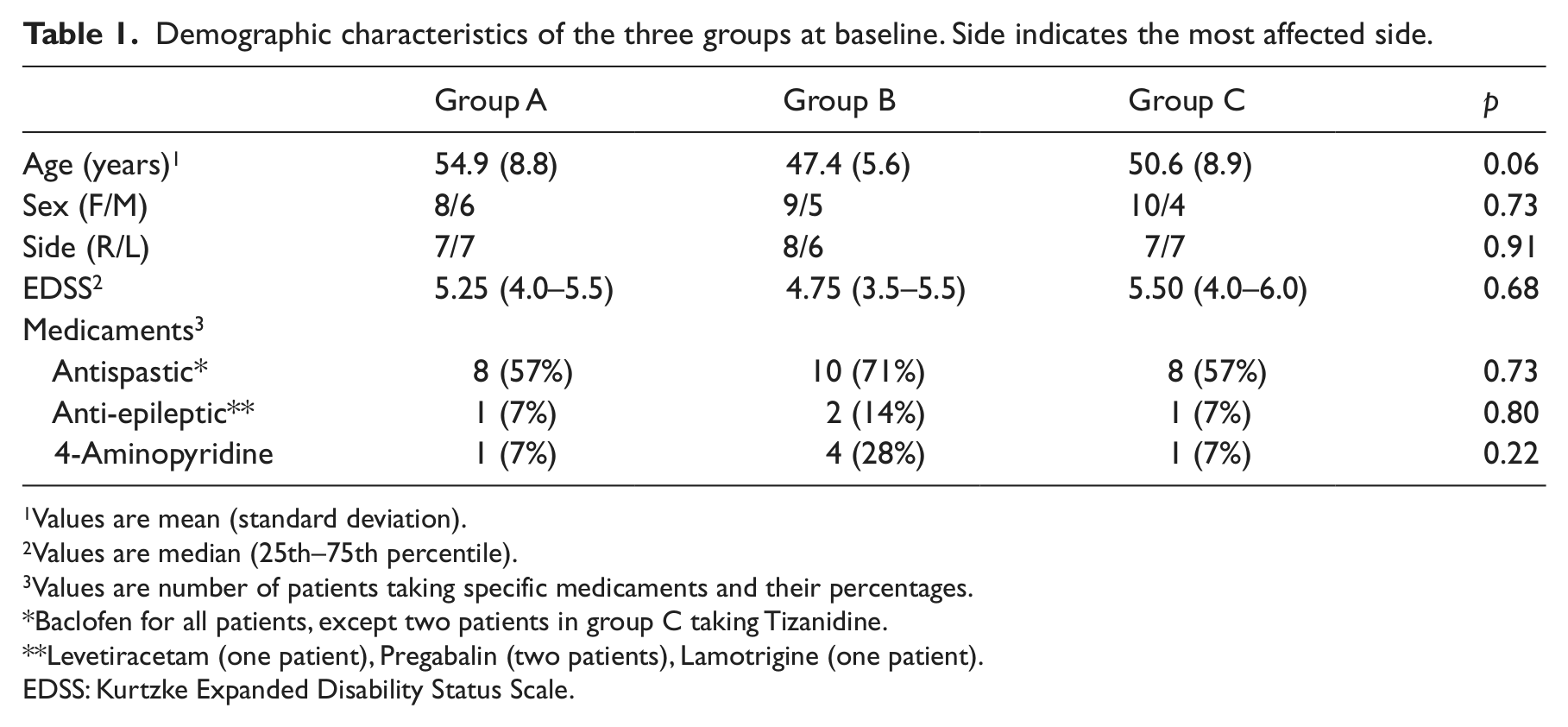
Values are mean (standard deviation).
Values are median (25th–75th percentile).
Values are number of patients taking specific medicaments and their percentages.
Baclofen for all patients, except two patients in group C taking Tizanidine.
Levetiracetam (one patient), Pregabalin (two patients), Lamotrigine (one patient).
EDSS: Kurtzke Expanded Disability Status Scale.
Values of the Modified Ashworth Scale at the knee (K-MAS) and ankle (A-MAS), of the Fatigue Severity Scale (FSS) and of the Barthel Index in all three groups at T0 (baseline), T1 (10 weeks postallocation) and T2 (22 weeks postallocation).
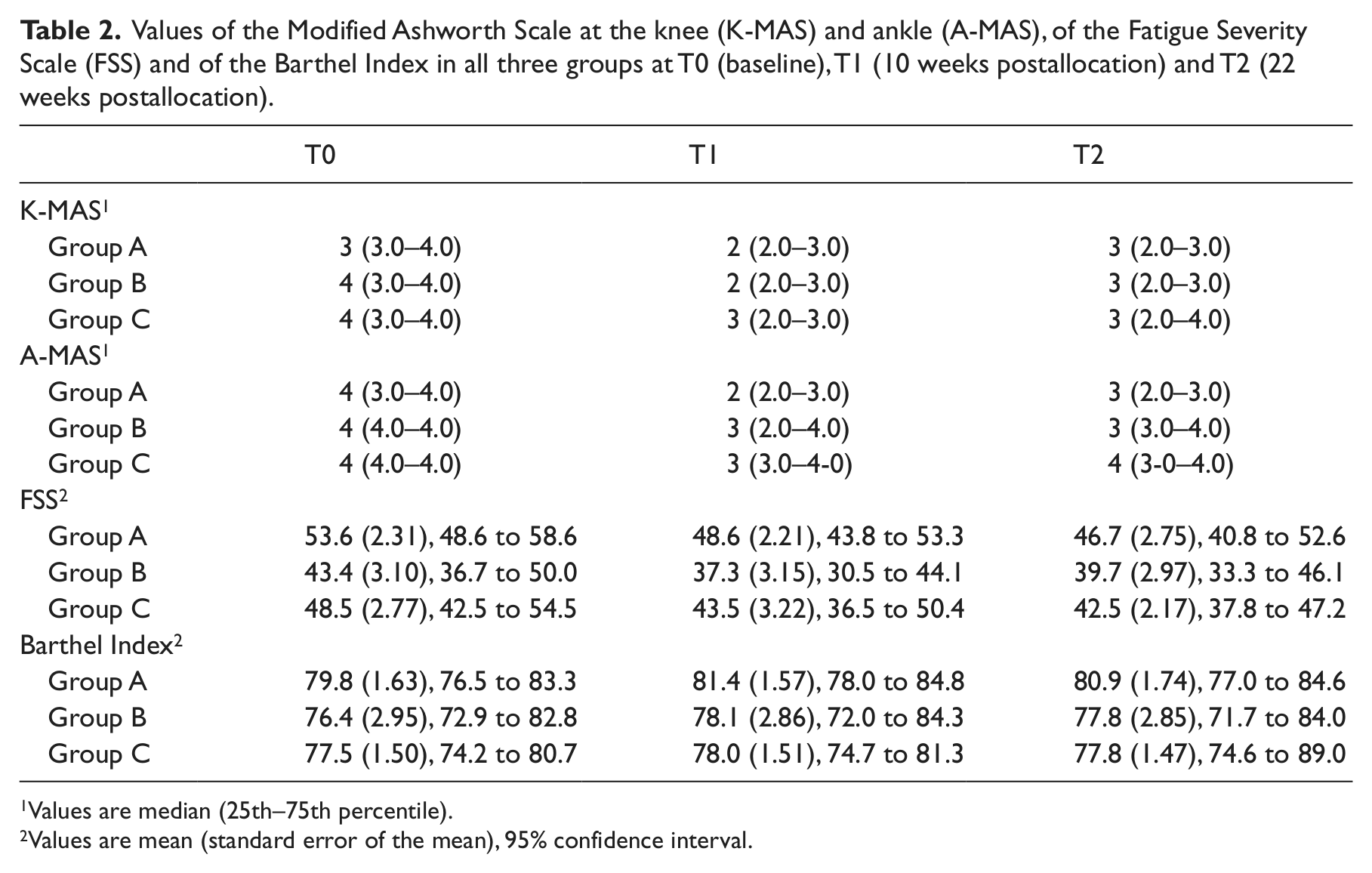
Values are median (25th–75th percentile).
Values are mean (standard error of the mean), 95% confidence interval.
Number (and percentage) of patients presenting with different values of the Modified Asworth Scale (MAS) for knee extensor and ankle plantarflexor muscles in all three groups at T0 (baseline), T1 (10 weeks postallocation) and T2 (22 weeks postallocation).
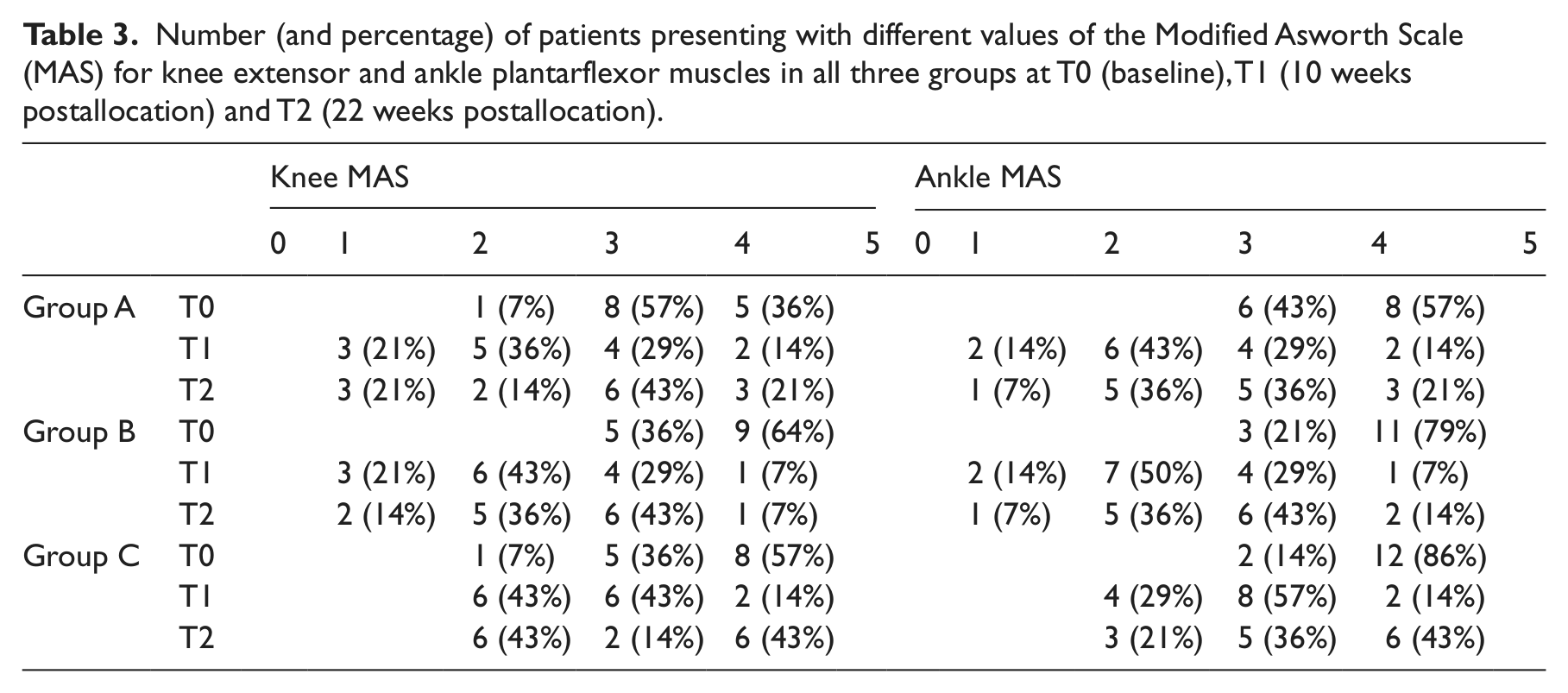
The ankle Modified Ashworth Scale scores (Table 3) significantly changed over time in group A (χ2r = 25.61; DF = 2; p < 0.001), in group B (χ2r = 50.78; DF = 2; p < 0.001) and in group C (χ2r = 20.63; DF = 2; p < 0.001). Post-hoc analyses revealed significant differences (p < 0.05) in the scores between T0 and T1 and between T0 and T2 in all three groups. Moreover, in group C the ankle Modified Ashworth Scale scores were significantly higher (p < 0.05) at T2 than at T1, though no differences were detected between groups at either T1 (KW = 2.41; DF = 2; p = 0.26) or T2 (KW = 2.3; DF = 2; p = 0.29).
The Fatigue Severity Scale scores significantly changed over time in group A (F = 8.68; DF = 1.492; p = 0.004), in group B (F = 4.25; DF = 1.18; p = 0.05) and in group C (F = 5.06; DF = 1.738; p = 0.02). At the post-hoc analysis, values in group A were significantly higher at T0 than at either T1 (p = 0.03) or T2 (p = 0.02). Fatigue Severity Scale values were significantly higher in group C at T0 than at either T1 (p = 0.03) or T2 (p = 0.02), while no differences were detected in group B. It is noteworthy, however, that the Fatigue Severity Scale values in group B were slightly, though significantly, lower than in the other groups at T0 (F = 3.507; DF = 2; p = 0.04) and at T1 (F = 3.87; DF = 2; p = 0.03), whereas no such difference was detected between groups by the one-way ANOVA at T2 (F = 1.764; DF = 2; p = 0.185).
No differences emerged from the Barthel Index scores over time in either group A (F = 3.28; DF = 1.569; p = 0.07) or group C (F = 1.54; DF = 1.773; p = 0.236), whereas a significant change was detected in group B (χ2r = 6.945; DF = 2; p = 0.004). Post-hoc analysis in group B revealed lower values at T0 than at T1 (p < 0.05) and T2 (p < 0.05). There were no significant differences in the Barthel Index scores between groups at either T1 (KW = 1.799; DF = 2; p = 0.40) or T2 (KW = 2.173; DF = 2; p = 0.33).
Discussion
Our results demonstrate that segmental muscle vibration and botulinum toxin, either alone or in combination, decreased muscle tone and reduced fatigue symptoms at both the one-month and three-month follow-up in a population of multiple sclerosis patients.
In our study, however, the addiction of segmental muscle vibration to botulinum toxin caused further advantages, mostly in terms of prolongation of the effect on muscle tone over time. We did not observe any difference between groups in both knee and ankle Modified Ashworth Scale values at either clinical follow-up. However, the within-group analyses showed that in group C both values were higher at T2 than at T1, thereby indicating a re-increasing of muscle tone in patients who were treated with botulinum toxin alone. Table 3 shows that the number of patients with increased Ashworth values at T2 was generally higher in group C than in either groups A or B. This suggests that the effects yielded by botulinum toxin injections alone persist less than those obtained with segmental muscle vibration alone or with the two therapies combined.
To our knowledge, this is the first time that the ability of segmental muscle vibration to reduce muscle tone has been reported in a population of multiple sclerosis patients. Indeed, in previous studies designed to investigate the effects of vibrations on multiple sclerosis symptoms, the vibratory stimulus was applied as whole body vibration by means of vibrating platforms,21,22 which ultimately leads to an aspecific delivery of mechanical stimulus to the whole body. Segmental muscle vibration is instead muscle-specific and has characteristic properties that lend themselves to the treatment of focal spasticity.
It is widely known that a vibratory stimulus applied directly to a muscle induces presynaptic inhibition of Ia afferents 23 and is likely to reduce transmitter release from the Ia afferents, 24 thereby decreasing the monosynaptic reflex excitability. Vibration also reduces the stretch-related afferent input through a ‘busy-line’ phenomenon, whereby the Ia discharge is locked to vibration and is consequently unable to faithfully transmit the stretch-induced volley owing to the high vibration frequency (>90 Hz) and the entrained action potentials in the Ia fibres. 25 Indeed, the application of a 91-Hz vibratory stimulus to the spastic upper limb muscles of post-stroke patients results in a significant and persistent (up to 30 minutes) reduction in muscle tone, accompanied by a reduction in F-wave amplitude and F/M ratio, both of which point to a reduction in motor-neuronal excitability.9,26 Moreover, vibration also reduces the H reflex, probably through mechanisms of postactivation depression and dendritic depolarization. 27 Indeed, a reduction in muscle tone and in the H/M ratio has been demonstrated in patients with complete or incomplete spinal cord injury after a 50-Hz vibratory stimulus over the quadriceps belly. 28
Nevertheless, the peripheral actions of segmental muscle vibration cannot, we believe, fully explain all the clinical effects observed in our patients. The persisting reduced muscle tone, in particular, may be ascribable to functional central nervous system plasticity. Segmental muscle vibration also exerts its effects at the central nervous system level, as demonstrated by numerous transcranial magnetic stimulation studies.12,29–31 A repeated muscle vibration intervention, applied during a voluntary contraction of the target muscle (i.e. flexor carpi radialis), induces a long-lasting increase in intra-cortical inhibition of the flexor carpi radialis and an inverse pattern in its functional antagonist. 32 These findings raise the hypothesis that muscle vibration might, by eliciting motor cortical reorganization, influence functional recovery during neurological disorders. In keeping with this hypothesis, segmental muscle vibration applied over the affected lower limb leads to an improvement in the gait parameters in chronic stroke patients, which was detectable not only on the paretic side, but also on the contralateral, unaffected side. 33
The ability of botulinum toxin to reduce spasticity is supported primarily by its peripheral action. Botulinum toxin inhibits acetylcholine release from the presynaptic neuromuscular terminals, thus weakening the agonistic muscle. 34 A decrease in the H/M ratio has recently been described in a population of cerebral palsy children one-month after botulinum toxin injections, 35 which led to altered excitability in spinal cord circuitry modulated by a decreased spindle afferent input to the spinal cord. 34 It should be borne in mind that an increasing body of experimental data also support the role of central nervous system structures in the efficacy displayed by botulinum toxin.36,37
In our study, neither segmental muscle vibration nor botulinum toxin had negative effects on fatigue. The patients in our groups may have been fatigued at baseline, 38 even though patients in group B presented slightly lower Fatigue Severity Scale values than those in groups A and C. Interestingly, at the three-month follow-up, the fatigue values were significantly lower than at baseline in all groups. One of the causative mechanisms believed to play an important role in the genesis of multiple sclerosis-related fatigue is the distortion of functional connections within the brain-muscle circuit. 39 One intriguing hypothesis is that the improvement observed in fatigue symptoms might be ascribable to functional changes that are induced by the segmental muscle vibration or botulinum toxin injections and express the modulation of Ia afferent fibres that are ‘more open and sensitive’ to therapeutic training. 35
No adverse events were recorded in our patients, as the fact that every patient in all three groups completed the treatments and attended the follow-up examinations.
One limitation of the present study is that we did not measure functional ability and were thus unable to understand whether the improvement in spasticity was accompanied by a gain in functionality. We only assessed changes in disability by means of the Barthel Index, which is one of the most widely used indicators of disability status and of its changes, despite being recommended in a community setting alone. 40
Moreover, as we limited our follow-up to three months after the end of therapy, no conclusions can be drawn regarding the long-term effects of segmental muscle vibration or botulinum toxin on multiple sclerosis-related spasticity.
Concerns may exist about the use of the Modified Ashworth Scale as an outcome measure. Fleuren et al., 41 recently conducted a cross-sectional study on 30 patients with upper motor neuron syndrome and spasticity in the elbow flexors and/or knee extensors, and found the validity and reliability of the Modified Ashworth Scale insufficient to be used as a measure of spasticity. Recently, however, the same scale was tested for psychometric properties in a population of patients with multiple sclerosis, demonstrating a good internal consistency as well as good test–retest reliability, thereby being considered applicable in both clinical practice and research. 42
Finally, the sample size of our study was obviously limited. Based on the present results, we calculated that 62 patients per group should be included in to a clinical study in order to estimate if segmental muscle vibration is more effective than botulinum toxin on spasticity with type I and a type II error of 0.05 and 0.20, respectively.
Clinical messages
Segmental muscle vibration and botulinum toxin injections either alone or in combination, reduce spasticity and improve fatigue symptoms in a population of patients with multiple sclerosis.
Positive effects of both treatments can be observed three months after therapy ended.
Footnotes
Contributors
MP (Physiatrist) designed the study, contributed to following the study procedures and in writing the manuscript. MG (neurologist) performed botulinum toxin type A treatment in patients of groups B and C. MM (engineer, PhD in Physical Medicine and Rehabilitation) performed the study randomization and carried out the statistical analysis. EDP (physiatrist) performed SMV treatment, contributed to following the study procedures. ET (physiatrist) performed the clinical evaluations in all patients and contributed in writing the manuscript. LL (resident in neurology) helped in the planning and organization of the study and helped to revise the manuscript. AB (physiatrist) supervised the rehabilitative treatment in all groups. VS (Director of the Physical Medicine and Rehabilitation unit) designed and supervised the study, discussed the results and helped in preparing and revising the manuscript. CP (Director of the Multiple Sclerosis Centre) designed and supervised the study, discussed the results and helped in preparing and revising the manuscript, he is guarantor for the accuracy and honesty of the report and the morality of the study.
Conflict of interest
None declared.
Funding
This work was supported by FISM (Fondazione Italiana Sclerosi Multipla) Cod. 2008/R/23.