
Abstract
Objective:
To identify and critically appraise clinical measurement tools used to assess sitting posture, seated postural control or functional abilities for children with motor impairment who are candidates for seating interventions.
Data sources:
Searches were run in 15 electronic databases along with hand searching. The search included articles published in English to December 2011.
Review methods:
Key terms included: posture, sitting, sitting posture, seated posture, seated postural control, sitting position, seating, wheelchair(s), outcome and assess(ment). The PRISMA statement was followed with inclusion criteria set a priori. Two reviewers independently screened titles, reviewed abstracts and identified full-text articles that met criteria. Data extraction included tool description and clinical utility. Two quality-rating scales were used to evaluate conduct of the studies and psychometric properties of the tools.
Results:
Of the 497 titles found in the search, 29 full-text articles met the inclusion criteria and 19 tools were identified. Tools represented all components of the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY), with emphasis on body structure and function and activity components. Evidence supporting reliability and validity varied, with small sample sizes influencing quality ratings. Evidence of the tools’ reliability was more prevalent than evidence of the tools’ validity. Only four tools reported on responsiveness, an important consideration for evaluating change. Little information on clinical utility was provided.
Conclusion:
Although a number of tools are available, evidence supporting their use for seating interventions is limited, as is the evidence supporting the strength of their measurement properties. Few tools address participation, environmental factors or the child’s and family’s perspective.
Introduction
Children with motor impairments such as cerebral palsy, muscular dystrophy and spina bifida commonly have limited postural control abilities. Specialized seating is a therapeutic intervention used to address the needs of individuals with limited postural control.1,2 Seating interventions, ranging from simple to complex, may facilitate optimal health and maximize participation despite limited postural control.
The International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) 3 should be adopted when evaluating seating interventions in order that ‘clinicians, researchers, families, and policy makers may share a common understanding of the functional role of seating devices in children’ (ref. 4, p.108). Costigan and Light 5 suggest that seating can be used to enhance body structure and functioning as well as activity and participation. Seating interventions directed at the level of body structure and functioning impairments may, for example, enhance respiratory function, influence muscle tone or reflexes, reduce risk of, or accommodate for, anatomical deformity or address skin interface pressure management.5–7 Seating directed at the level of activity limitations may be aimed at improving stability in sitting, safety and comfort, or enhancing fine motor activity performance.4,8,9 Seating designed to foster engagement in life roles may reduce participation restrictions. 5
Although measurement tools assist in evaluating the effects of therapists’ interventions, 10 a lack of appropriate clinical tools exists to address the needs of individuals who have postural compensations affecting the entire body. 7 A limited number of tools capture information related to seated postural control specific to seating interventions, 11 with most such measures developed for adults.12–14 Well-developed tools assure confidence that the tools measure what they are supposed to measure consistently, are responsive to change, and have clinical meaning interpretable by the user.12,15 Reviews on the effectiveness of seating interventions have been published for children with different diagnoses,1,4,8,16–18 with few touching on the measurement tools used in the studies.9,19,20 A systematic review summarizing the range of tools available would be useful for clinicians with limited time and resources. 10
We conducted a systematic review of the literature to identify and critically appraise the evidence underlying measurement tools for assessing sitting posture, seated postural control or functional abilities for children with motor impairments who are candidates for seating intervention. Our clinical question was: ‘For children under 19 years of age with motor impairments (who are candidates for seating intervention), what clinical measurement tools are used to assess sitting posture, seated postural control or functional abilities?’ Related questions were ‘What are the psychometric properties of these measurement tools?’ and ‘What components of the ICF-CY 3 do these tools address?’
Methods
Two reviewers with graduate-level research training in the field of rehabilitation conducted the search. Health librarians experienced in systematic review development assisted in planning and recording the search, which was restricted to studies published in English to December 2011 and included peer-reviewed articles from 15 electronic databases: OT Seeker; Physiotherapy Evidence Database (PEDro); Cochrane Central Register of Controlled Trials; Cochrane Database of Systematic Reviews; Database of Abstracts of Reviews of Effects; ACP Journal Club; CINAHL; Medline OVID SP; EMBASE; PsychInfo; ERIC; Google Scholar; National Quality Measures Clearinghouse; Health and Psychosocial Instruments; and Health Technology Assessment.
A core set of key terms was identified based on several eligible articles: posture, sitting, sitting posture, seated posture, seated postural control, sitting position, seating, wheelchair(s), outcome and assess(ment). Two types of searches were performed; the first used the terms as subject headings or medical subject heading (MeSH) descriptors, and the second used the terms as keywords.
Two reviewers independently screened titles, and abstracts were retrieved for those appearing to meet criteria. Both reviewers independently reviewed all abstracts to decide if the full text should be obtained. The terms ‘screen’, ‘tool’, ‘instrument’, ‘measure’, ‘scale’ and ‘outcome’ were used to identify studies where data had been captured in a standardized manner. A manual search of electronically retrieved bibliographies was completed to identify other relevant peer-reviewed articles. Targeted searching of authors and other known titles that did not appear in the electronic search was also completed. The two reviewers independently reviewed full-text articles to determine if they met inclusion criteria. Consensus was achieved through discussion at all stages without need to involve a third reviewer.
Inclusion criteria were identified prior to the search to determine all relevant literature: (1) participant(s) had a motor impairment or movement disorder related to a neurological or neuromuscular condition; (2) a seating system, seating components, or wheelchair, and/or physical characteristics of the participants were described in enough detail to determine that they would typically use a seating and mobility system (e.g. Gross Motor Function Classification System 21 levels III–V for children with cerebral palsy); (3) a detailed description of the assessments used as outcomes in the evaluation of sitting posture or seated postural control, including psychometric properties (reliability, validity, responsiveness) and/or clinical utility; and (4) inclusion of at least one child or adolescent (0–19 years of age). To capture a broad spectrum of literature, a variety of research designs were included with no restrictions on measurement methods.
Exclusion criteria were: (1) non-English language publications; (2) studies related specifically to adults; (3) studies related only to children who were typically developing; (4) measurement method not feasible for use in a typical rehabilitation clinical setting (e.g. X-ray, EMG, force-platform); and (5) non-peer-reviewed articles, including dissertations or conference proceedings.
To assess study quality, we used both the COnsensus-based Standards for the selection of health status Measurement INstruments (COSMIN) checklist22,23 and the McMaster Outcome Measures Rating Form, 24 referred to hereafter simply as the McMaster Rating. The COSMIN checklist22,23 was chosen to rate the overall methodological quality and conduct of individual studies, whereas the McMaster Rating 24 provided ratings of reliability and validity results while emphasizing clinical utility of the measurement tools. The PRISMA statement 25 was used to structure this systematic review.
The reviewers extracted data including evidence source, psychometric properties, conduct and rigour of tool development. Evidence source information included author, outcome measures, study design and population characteristics. Psychometric details of the measurement tools, the focus of this review, included evidence for reliability and validity, with a particular emphasis on responsiveness. Clinical utility and response format of each tool were also extracted. Because the reviewers conducting this review have been involved in the research development and clinical use of two of the measures being evaluated, the Seated Postural Control Measure 26 and the Level of Sitting Scale, 26 an external reviewer independently completed ratings on these two measures to reduce potential for bias.
Tools were divided into three groups: those developed specifically to assess posture within a seating system in order to assess the outcome of seating interventions (seating tools); tools of sitting posture or balance that have wider therapeutic application (sitting balance and posture tools); and those designed to evaluate functional ability that may be impacted by seated postural control (functional ability tools). Whenever only a portion of a tool was relevant for our review, only that information is reported. For example, the Chailey Levels of Ability 27 has several scales addressing lying, standing and sitting. Only the Box Sitting Ability Scale is relevant to this review and we refer to it as the Chailey scale. 27 The Seated Postural Control Measure 26 has two different sections – Alignment and Function 28 ; reliability information is reported separately. Similarly, the Sitting Assessment for Children with Neurological Dysfunction 29 has a subsection called Abnormal Postural Responses, and the Sitting Assessment Scale30,31 has a subsection called Counting Pathological Movements; for these reliability information is reported separately. For the Spinal Alignment and Range of Motion Measure, 32 only the alignment items are relevant for this review.
Results
Figure 1 illustrates the PRISMA flowchart, 25 outlining each step. Six hundred articles were identified through electronic database searches, with another 121 identified through manual searching. After de-duplication, there were 497 titles, with 48 articles (10%) meeting inclusion criteria based on title and abstract. Agreement between reviewers on abstractsthat should be reviewed as full text was 98% (n = 47). From full-text review, 29 articles (60%) met the inclusion criteria, with 95% agreement between reviewers; 21 of these articles (72%) were identified through manual searching.
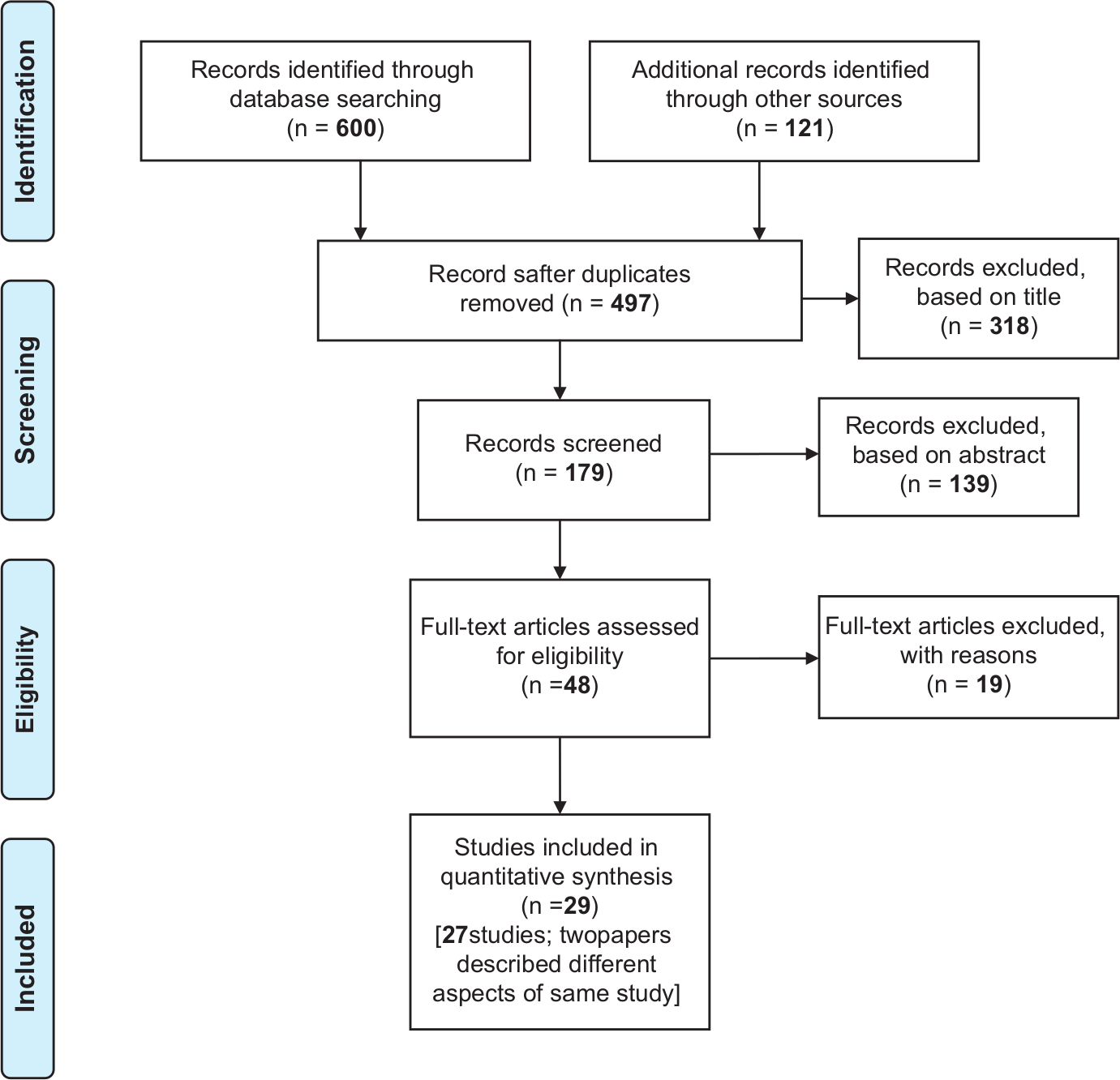
PRISMA 2009 flow diagram. Reproduced with kind permission from PLOS Medicine. 25
Of the 19 articles that did not fully meet criteria, three (16%) did not address the desired population,33–35 three (16%) were descriptive or theoretical in focus,5,36,37 one (5%) was not feasible for use in clinical practice, 38 one’s (5%) purpose related to ADL performance, 39 and finally 11 (58%) failed to include details of the psychometric properties of their outcome measures.40–50
Table 1 (online) summarizes the evidence source characteristics of each study, presented alphabetically, in which 29 articles representing 27 studies were included. Several studies reported on more than one tool,26,28,54,56,57 while several articles reported on different aspects of the same study.56,57,63,64 Of the 27 studies, 11 (41%) were methodological with a focus on tool development and evaluation of measurement properties.26–29,32,51,54,55,70,76,79 The remaining 16 studies (59%) were primarily intervention studies that used a measurement tool for evaluation and provided some information on psychometric properties.30,31,51,53,56,57,58,59,61,63–66,69,71,73,74,78 Because our review focused on evaluating the tools used and not the specific intervention outcomes of the study, readers are referred to other reviews of paediatric seating interventions for an evaluation of the quality of evidence provided in these intervention studies.1,7–9,16–20 Three reviews9,19,20 highlighted psychometric properties of tools used to evaluate seating interventions: the Sitting Ability Scale, 30 the Modified Schober Measurement of Spinal Extension (referred to simply as Schober for the remainder of this article),61,62 and Hulme’s assessment instrument.56,57
Table 2 (online) summarizes the psychometric details of the 19 measurement tools identified. Evidence for reliability and validity are presented.
Measurement tool ratings are summarized in Table 3 (online) for reliability evidence and Table 4 (online) for validity evidence. After independently appraising the evidence, the initial agreement between reviewers was 87%. Consensus for all ratings (the COSMIN checklist22,23 for overall rating of the conduct of each study and the two McMaster Ratings 24 ) was achieved through discussion. The two sections of the McMaster Rating 24 included both an individual study rating and an overall rating based on the number of studies completed. For example, one or two studies with adequate or excellent evidence ratings would merit an overall rating of adequate. For studies in which the statistical results were not low enough to merit a poor rating on the McMaster Rating, 24 we created a combined rating of ‘P/A’ to highlight our concerns about the conduct of the study or the statistical methodology used. There were several tools with evidence from numerous sources; while evaluation of all these sources was beyond the scope of this review, their psychometric properties were reported.
Reliability using the COSMIN checklist22,23
Most seating tools and six of the sitting balance and posture tools received poor ratings, due mainly to small sample size. The Level of Sitting Scale26,28,54 and Seated Postural Control Measure26,28,54 achieved excellent, 28 good 54 and fair 26 inter-rater reliability ratings, and good 54 and fair 26 test-retest reliability ratings. The Trunk Control Measurement Scale 55 and Segmental Assessment of Trunk Control51,52 achieved good and fair ratings respectively for inter-rater reliability. For the functional ability tools, most ratings were reported as they included numerous sources.72,75 However, those functional ability tools evaluated by the reviewers rated poor.53,59,60,66–68
Reliability using the McMaster Rating 24
The Seated Postural Control Measure-Function26,28,54 achieved an excellent overall inter-rater reliability rating. Overall inter-rater reliability was adequate for the Level of Sitting Scale,26,28,54 Sitting Assessment of Children with Neurological Dysfunction,29,58,69,70 Spinal Alignment and Range of Motion Measure,32,79 Sitting Assessment Scale,30,31,65 Segmental Assessment of Trunk Control,51,52 Seated Postural Control Measure-Alignment,26,28,54 Trunk Control Measurement Scale 55 and Trunk Impairment Scale.76,77 Overall intra-rater reliability (where original video-recordings are re-scored by the same rater) was adequate for the Sitting Assessment Scale,30,31,65 Segmental Assessment of Trunk Control51,52 and Trunk Impairment Scale.76,77 Test–retest reliability was more commonly reported for tools that require hands-on assessment and is more relevant for clinical use. Overall test–retest reliability ratings were adequate for the Level of Sitting Scale,26,28,54 Sitting Assessment for Children with Neurological Dysfunction,29,58,69,70 Spinal Alignment and Range of Motion Measure,32,79 Seated Postural Control Measure-Function26,54 and Trunk Control Measurement Scale, 55 while the Schober,61,62 and Head Position Trainer59,60 were reported to have adequate test–retest reliability. Evidence for reliability was reported in numerous studies88,89 for the Canadian Occupational Performance Measure 72 and the Pediatric Evaluation of Disability Inventory Caregiver Assistance Scale. 75 The remaining tools either did not present evidence for reliability, or were rated poor to adequate, or poor.
Validity using the COSMIN checklist22,23
The Level of Sitting Scale,26,28,54 Sitting Assessment of Children with Neurological Dysfunction,29,58,69,70 Spinal Alignment and Range of Motion Measure,32,79 Segmental Assessment of Trunk Control,51,52 Seated Postural Control Measure26,28,54 and Trunk Control Measurement Scale 55 achieved excellent ratings for content validity, while the Chailey scale 27 achieved a good rating. The Chailey scale, 27 Spinal Alignment and Range of Motion Measure,32,79 and Segmental Assessment of Trunk Control51,52 achieved fair ratings for hypothesis testing; the remaining tools rated poor, again mostly due to sample size. Evidence for responsiveness was provided only for the Level of Sitting Scale26,28,54 and Seated Postural Control Measure,26,28,54 with both achieving a fair rating. Evidence for responsiveness was reported in numerous studies for the Canadian Occupational Performance Measure 72 and the Pediatric Evaluation of Disability Inventory Caregiver Assistance Scale. 75
Validity using the McMaster Rating 24
Adequate overall content and construct validity ratings were achieved by the Chailey scale, 27 Sitting Assessment for Children with Neurological Dysfunction,29,58,69,70 Spinal Alignment and Range of Motion Measure,32,79 Segmental Assessment of Trunk Control,51,52 and Trunk Control Measurement Scale. 55 The Jebsen–Taylor Hand Function Test66–68 achieved adequate overall construct validity 66 and reported adequate overall content validity,67,68 while the Schober61,62 reported adequate overall ratings for both. Evidence for responsiveness was provided for the Level of Sitting Scale26,28,54 and Seated Postural Control Measure,26,28,54 with both achieving adequate overall responsiveness ratings in addition to having adequate overall content validity. The Canadian Occupational Performance Measure 72 and the Pediatric Evaluation of Disability Inventory 75 overall ratings for responsiveness, content and construct validity were reported to be adequate to excellent from numerous sources. The remaining tools either did not present evidence for validity, or were rated poor to adequate.
Table 5 (online) provides information related to test description and clinical utility in addition to the associated ICF-CY 3 component(s). Three tools were developed specifically for seating intervention studies: Hulme’s assessment,56,57 videography 78 and direct selection of targets on a speech-generating device (referred to as Targeting on a speech-generating device). 53 Although little was done to evaluate psychometric properties, enough information was provided in the articles to meet our inclusion criteria. Seven tools can be used within the seating system to measure outcome of seating interventions: force transducer and interface pressure measurement, 63 Hulme’s assessment,56,57 Sitting Assessment for Children with Neurological Dysfunction,29,58,69,70 Sitting Assessment Scale,30,31,65 Seated Postural Control Measure26,28,54 and videography. 78 Seven additional tools quantify or classify sitting ability and generally involve sitting on a bench or box: the Chailey scale, 27 Level of Sitting Scale,26,28,54 Schober,61,62 Spinal Alignment and Range of Motion Measure,32,79 Segmental Assessment of Trunk Control,51,52 Trunk Control Measurement Scale 55 and Trunk Impairment Scale.76,77 Five tools evaluate functional abilities that may be impacted by seated postural control: Canadian Occupational Performance Measure, 72 Head Position Trainer,59,60 Jebsen–Taylor Hand Function Test,66–68 Pediatric Evaluation of Disability Inventory Caregiver Assistance Scale 75 and Targeting on a speech-generating device. 53
Discussion
In this systematic review, 19 measurement tools were identified for evaluating sitting posture, seated postural control or functional abilities for children with motor impairments who are candidates for seating intervention. There were no measures that met all criteria for instrument development,12,15 suggesting room for improvement in establishing robust and appropriate measurement tools that reflect all components of health as determined by the ICF-CY. 3
Although some authors commented on clinical usefulness26,61,64–66,78 there was little objective evidence. Most tools use items commonly found in clinical practice (e.g. tape measures, goniometers and toys). However, four tools (Segmental Assessment of Trunk Control,51,52 Spinal Alignment and Range of Motion Measure,32,79 Trunk Control Measurement Scale 55 and Trunk Impairment Scale76,77) have requirements that may limit their clinical utility. The Trunk Impairment Scale76,77 and Trunk Control Measurement Scale 55 are appropriate only for children in Gross Motor Function Classification System 21 levels I–III, limiting use for children who require external support to maintain a sitting position (typically Gross Motor Function Classification System levels IV and V). This review highlights the need for research on clinical utility of the tools, as this is essential for the adoption of outcome measurement tools in clinical practice. 2
It is important that measurement tools represent the range of ICF-CY 3 health components.4,12 This review confirmed that there are tools available to evaluate the different components. All the seating tools address the ICF-CY components of body structure and function and activity. 3 Two of the sitting balance and posture tools address body structure and function: Schober,61,62 and Spinal Alignment Range of Motion Measure32,79; whereas five tools address activity: the Chailey scale, 27 Level of Sitting Scale,26,28,54 Segmental Assessment of Trunk Control,51,52 Trunk Control Measurement Scale 55 and Trunk Impairment Scale.76,77 Within the functional ability tools group, there was more variation in ICF-CY 3 components. The modified Pediatric Evaluation of Disability Inventory 75 addresses environmental factors whereas the Jebsen–Taylor Hand Function Test66–68 and Targeting a speech-generating device 53 address activity. The Head Position Trainer59,60 addresses body structure and function and activity while the Canadian Occupational Performance Measure 72 addresses user-defined goals related to participation and activity. Tools that evaluate participation or environmental factors, or tools that capture the child’s and/or parent’s perspective are limited. Most tools were fairly evenly distributed between body structure and function and activity, in keeping with the evolution of theoretical frameworks used to support clinical practice over the years. Participation and environmental factors have more recently been acknowledged as important components to measure when evaluating health status. 12 The results of this review may assist in identifying tools aimed at specific ICF-CY 3 components to evaluate seating intervention outcomes.
Ryan 4 discussed the need for tools with adequate reliability and validity that are responsive to meaningful change specific to seating interventions. Although there are a number of tools available to measure sitting posture, seated postural control and functional abilities, most do not fully meet the standards for a well-developed tool.12,15 The two rating scales used in this review22–24 focused on different perspectives of quality assessment, and together they provided a comprehensive overview of the strengths and limitations of each tool. There is far more evidence supporting reliability for the identified tools than for validity or responsiveness; this is in keeping with standard test development procedures 15 and the growth of critical evaluation for this clinical specialty.12,86
Evidence of inter-rater reliability was more prevalent in this review than test–retest reliability, with even less evidence for intra-rater reliability. This is understandable given that establishing test–retest reliability is challenging in this population due to variability in posture and functional abilities.
Evidence regarding face and content validity was provided for most tools while evidence for discriminative validity and responsiveness was limited. Given that validity standards encompass a broad range of evidence for construct validity, 87 further research is warranted.
The Canadian Occupational Performance Measure, 72 and Pediatric Evaluation of Disability Inventory 75 are reported to have adequate to excellent reliability, validity and responsiveness but it was beyond the scope of this review to analyse all the studies published on these tools.88,89 The Pediatric Evaluation of Disability Inventory 75 was modified for use in the study included in this review 74 ; psychometric properties of the original tool may not apply. Although work has been done establishing the validity of the Canadian Occupational Performance Measure 72 by parent/caregiver proxy90–92 and by children with disabilities,93,94 use of this tool for seating intervention outcomes is limited.71,74,95 Psychometric properties related to its use for this specific purpose have not been explored fully.
Some tools, such as force transducers and interface pressure measurement devices, 63 are commonly used in other therapeutic applications or other technical fields. However, confirmation of the reliability, validity and responsiveness of these tools for the specific purposes of seated postural control evaluation would be helpful. More importantly, the psychometric properties for the particular device models should have been included.
Several limitations to this review could affect the applicability of the results. First, there may be useful tools published in non-English language journals that contribute to this topic but were not included. Second, selective reporting within studies may have limited exposure to meaningful information about tool development. Third, two tools were reviewed by another reviewer to help minimize bias. Finally, the long time span over which the studies occurred was a challenge, as reporting standards have changed over the years. While some earlier studies were considered high quality for their time, study description and statistical methods used no longer meet contemporary expectations, influencing rating of individual studies and comparisons across tools.
Conclusion
In this systematic review, a critical appraisal of 19 measurement tools determined that no single tool met all criteria for instrument development.12,15 Establishing credible measurement tools will ultimately strengthen the evidence for seating interventions, increase confidence in the results of future studies and make findings more meaningful to clients, their families, clinicians and equipment funders 4 ; priorities recognized by others in the field.2,7,11 Chung et al. stated ‘there is limited high quality research available to determine the effectiveness of adaptive seating … studies with higher levels of evidence need to be conducted’ (ref. 1, p.14). This must begin by using measurement tools that are of higher quality – a theme echoed by several authors over the years.4,9,19
Clinical messages
There are 19 tools available to measure sitting posture, seated postural control and functional abilities for children with motor impairments who may use seating interventions, but none meet all criteria for a well-developed measure.
Few tools address participation, environmental factors, or the child’s and family’s perspective.
Footnotes
Acknowledgements
Special thanks to Jackie Casey MSc, BSc (Hons) OT, PgCHEP, Lecturer in Occupational Therapy, School of Health Sciences, University of Ulster, for agreeing to be an independent reviewer for the Seated Postural Control Measure and Level of Sitting Scale quality assessments. Acknowledgements to UBC and Sunny Hill Health Centre for Children health science librarians for their assistance in planning and carrying out the literature search; Susan R. Harris, PhD, PT, Professor Emerita, UBC, for her editorial expertise and Lori Roxborough MSc OT/PT, Associate Director, Therapy Department, Sunny Hill Health Centre for Children, for her guidance, support and encouragement. Recognition goes to our colleagues on the Positioning and Mobility team at Sunny Hill Health Centre for Children who provided inspiration for this manuscript from their discussions regarding evidence-based practice.
Contributors
DF initiated the idea, but both authors (DF and RL) designed the study, undertook the search, evaluated the evidence and wrote the manuscript. DF is the guarantor.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
Debra Field would like to acknowledge the Canadian Institutes of Health Research Fellowship Award, and the Canadian Occupational Therapy Foundation Blake Medical Distribution Scholarship Award for funding her time to write this manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.