
Abstract
Objective:
To develop a practical taxonomy of falls and to determine whether these different fall groups have different outcomes.
Design:
Descriptive study examining patient characteristics at the time of each fall and iterative development of falls taxonomy.
Setting:
An inpatient stroke rehabilitation ward.
Methods:
All falls over 21 months were reviewed retrospectively. Case notes were reviewed and each patient’s level of functioning at the time of fall, together with admission profile and discharge outcomes, were collected. Outcomes for fallers (as opposed to falls) were compared using the predominant fall type.
Results:
There were 241 falls in 122 patients and most falls occurred around the bed (196 (81%) falls). Toileting-related falls occurred in 54 patients (22.4%). The taxonomy proposes seven main fall types. One fall type (‘I’m giving it a go’) appeared quite different and was associated with better functioning at time of fall and better outcomes. Other fall types were related to high dependency needs, visuospatial difficulties or delirium. Medication-related falls were uncommon in this cohort.
Conclusions:
The falls taxonomy developed showed four main types of falls with different, but overlapping, patient characteristics at time of fall with different outcomes. Different fall-prevention strategies may be required for each group.
Introduction
Unfortunately, falls are common for older patients while in hospital. The risk of falling varies according to the type of ward1,2 with lower prevalence in acute wards (4–11% or 2.2–11.7 falls/1000 bed days), higher risk in general rehabilitation units (7–47% or 1.7–19.9 falls/1000 bed days) and possibly even higher during stroke rehabilitation (14–54%, or 2.2–22.8 falls/1000 bed days ).3–5 Stroke patients have multiple ‘intrinsic’ risk factors 6 for falling including slow and abnormal gait, poor balance, visuospatial deficits, cognitive impairment and impulsivity. All of these make them inherently vulnerable to fall, over and above other risks associated with older people in hospital. 3 Furthermore, medications, such as sedatives and antidepressants, are commonly used following stroke, and may increase the risk of falling. 7
The evidence for successful fall prevention programmes in falls in hospital is limited, with modest results from a small number of randomized controlled trials.8–12 A multifactorial and interdisciplinary approach, based on existing risk factors, appears the best way to preventing falls.11,13 Similar to community studies, 14 balance and exercise programmes may be of benefit in those with longer hospital stays 8 but evidence is limited, particularly for stroke patients.4,15
Our hypothesis was that not all falls and fallers are the same. Different falls may have different causes and potentially different outcomes. Our clinical experience suggests some falls occur early during a very dependent phase, others later as the person regains their independence. Some patients appear to make poor risk assessments whereas others strive to regain independence. If there are different types of falls, it should be possible to develop a taxonomy of falls. A number of studies have looked at predicting falls based on patient characteristics on admission.7,16–18 However, patients’ health and function changes over time and so these admission characteristics may not be reflective of their function at the time of fall. In order to develop this taxonomy of falls, as opposed to predict falls, it is more appropriate to gather information about the patients’ status as close as possible to the time of fall.
The aims of this study were to (a) examine the types of falls on an inpatient stroke rehabilitation unit, including the functional characteristics of the faller at the time of fall (as opposed to admission profile), (b) develop a broad classification or taxonomy of falls and (c) determine whether any of these fall groups have different outcomes.
Methods
The stroke rehabilitation unit is a 23-bed inpatient unit for older patients (65 years and older) and was established in 2001. 19 The admission policy is to take all patients who require inpatient rehabilitation after an acute stroke, including the very severe strokes, for a trial of rehabilitation. 20
A fall was defined as ‘a sudden, unintentional change in position causing the individual to land at a lower level, on an object, the floor or other surface’. 21 Blackouts, arrhythmias or seizures were excluded from this definition.
The department has had an active falls prevention programme for many years 22 and falls risk assessments are done routinely on admission and after any fall or major change in clinical status. This falls-assessment tool links risk factors to specific fall prevention strategies, which is an approach that has been used successful elsewhere. 9
After every inpatient fall there is a Quality Incident Event Report (QIER) completed. These forms are collated centrally and the incident reporting system has been used for several years, with no changes made to this reporting during the study. Each QIER for each fall in the stoke unit during the study period (1 January 2008–30 September 2009) was reviewed. The clinical notes (and electronic results where applicable) of all these stroke patients who fell were then reviewed retrospectively by one author (KLW). Each fall was assessed separately, although one patient may have had more than one fall. Basic demographic data on those who did not fall during their inpatient stay were also collected to allow comparisons with fallers, but case notes of non-fallers were not reviewed.
For each fall, we extracted information on characteristics of both the fall and the faller. The elements included an in-depth evaluation of the characteristics of the faller at time of admission, at the time of the fall and on discharge, as well as the stroke type (Oxfordshire Community Stroke Project Classification) 23 and severity. Each patient’s ability in activities of daily living (ADL) at the time of the fall was assessed using the Functional Independence Measure (FIM), 24 which was collected on admission, discharge and weekly during the inpatient stay. For each fall, the most recent FIM was used as the time of fall FIM. Nursing notes were reviewed to ascertain the reported functional status at time of fall for continence, toileting status and mobility status. A ‘traffic light system’ is used to indicate current levels of allowed independence in the following activities: bed mobility, sitting, transfers, standing and walking. 22 Mobility status at time of fall was assessed from these traffic light notations. Formal assessments of balance, such as Berg Balance Score, 25 are used on the unit, and were recorded if performed within one week before each fall. The presence or absence of hemianopia, inattention or neglect, other or visuospatial deficits, cognitive impairment, and impulsivity as documented in the notes were used. Medications at the time of the fall were also recorded.
Details of each fall were also collected, which included details of where, when, what happened, whether witnessed or not, as well as the activity being undertaken at the time of fall. This activity being attempted (and the assumed intent of the faller) was compared with their ‘allowed’ levels of mobility and independence at the time of each fall. This ‘allowed’ activity level was assessed from the traffic light system above for mobility, the nursing notes and from the weekly goal sheets.
The information was then used to create a classification system of falls based on the fall and faller characteristics, and activity being attempted at the time of fall. The development of the fall taxonomy was an iterative process among all three researchers. An initial ‘a priori’ taxonomy was evaluated on the first 20–25 falls, with types of falls and definitions refined and then extended. Further re-evaluation occurred after another 20–25 falls and then again when 100 falls had been reviewed. At each of these iterations, all three authors met to discuss complicated cases and to improve the face validity, appropriateness and the definitions within the taxonomy. Each time the definitions were tightened or rejected. As a result, the groupings and definitions were reworked several times as the project developed. Falls were then assigned by the developed definitions and any given fall could fit into more than one category. A small number did not fit into any category, despite different iterations of the taxonomy.
Discharge outcomes for each faller included mobility and continence status, FIM, domicile. Injuries sustained during the fall were also noted.
The study was approved by our local ethics committee (URB/09/08/EXP).
Statistical analysis
Comparisons were made at the level of both falls and fallers. For falls, each group within the taxonomy was compared with data from all the other groups combined (e.g. A vs. non-A, B vs. non-B, etc.).
Outcomes belong to either the fall (e.g. injury from one fall), or more usually the faller (e.g. discharge outcomes). Fallers may have several falls and some of these falls may have been of different types. Therefore, to avoid double counting when assessing faller discharge outcomes, the main type of fall for that individual was used. The main type of fall was defined as either the most frequent type (for multiple falls) or the category that best fitted the fall description (for a fall that met several different categories). Continuous variables were compared using Student’s t-tests or Mann-Whitney U-tests, whereas discrete variables were compared by Chi-square analysis. Owing to multiple comparisons between groups, we used Bonferroni correction for α=0.05 level.
Results
In the study period, there were 250 falls for the 401 patients admitted (18.2 per 1000 bed days or 58.8 per 100 admissions). Nine falls were not analysed as the admission notes were unavailable. Therefore, a total of 241 falls were analysed for this study. These falls occurred in 122 patients. A total of 29% of the total falls were from single fallers and 71% of the total falls occurred in multiple fallers.
The study group demographics are outlined in Table 1. Nearly one-third of all patients (122/401 or 30.4%) fell during the study period. As a group, fallers were significantly more functionally impaired both on admission and on discharge, and had poorer outcomes on discharge than non-fallers.
Demographics (and outcomes) of study population (fallers) and comparison with stroke patients who did not fall during study period.
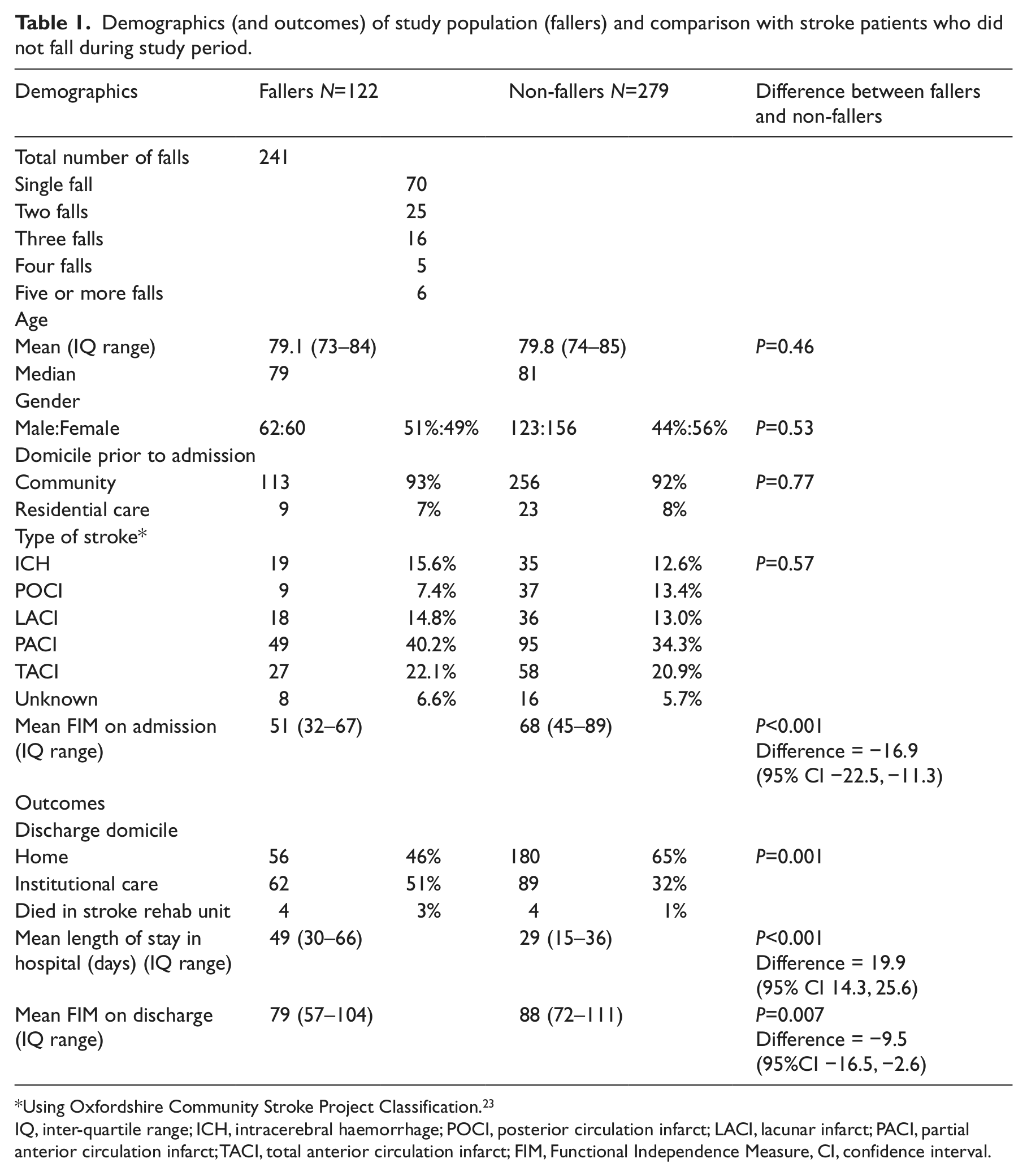
Using Oxfordshire Community Stroke Project Classification. 23
IQ, inter-quartile range; ICH, intracerebral haemorrhage; POCI, posterior circulation infarct; LACI, lacunar infarct; PACI, partial anterior circulation infarct; TACI, total anterior circulation infarct; FIM, Functional Independence Measure, CI, confidence interval.
Almost all of the fallers (116 or 95%) were assessed as at high risk of falls and had fall prevention strategies in place prior to the fall.
The time from the stroke to fall ranged from 4 to 134 days (mean and median of 42 and 38 days, respectively) and time between admission to rehabilitation and fall varied from 0 to 122 days (mean (median) = 31 (25)). As lengths of stay (LOS) are variable, timing of fall was also recalculated as a percentage of the whole admission. Falls occurred on average at 49% way through the admission (range 0–100%, interquartile range (IQR) 21–75%) suggesting falls occurred throughout the admission, right up until day of discharge. Falls occured throughout the 24-hour period.
The vast majority of falls occurred around the bed (196 (81%) falls). This included falls from a bed or that occurred around the bedside. All other locations were much less common, with falls occurring in the bathroom (21.9%), in the dining room (11.5%), in the corridor (5.2%) and in therapy area (5.2%). Three falls occurred off the ward. A total of 84% of falls were not witnessed by a staff member.
At the time of the fall, most patients were dependent on staff for basic cares and mobility (see Table 2). Despite this dependence, 50% were attempting to transfer or walk without assistance at the time of fall. Falls occurred during attempts to go to the toilet or during the process of toileting in 54 patients (22.4%).
Functional status at the time of fall.
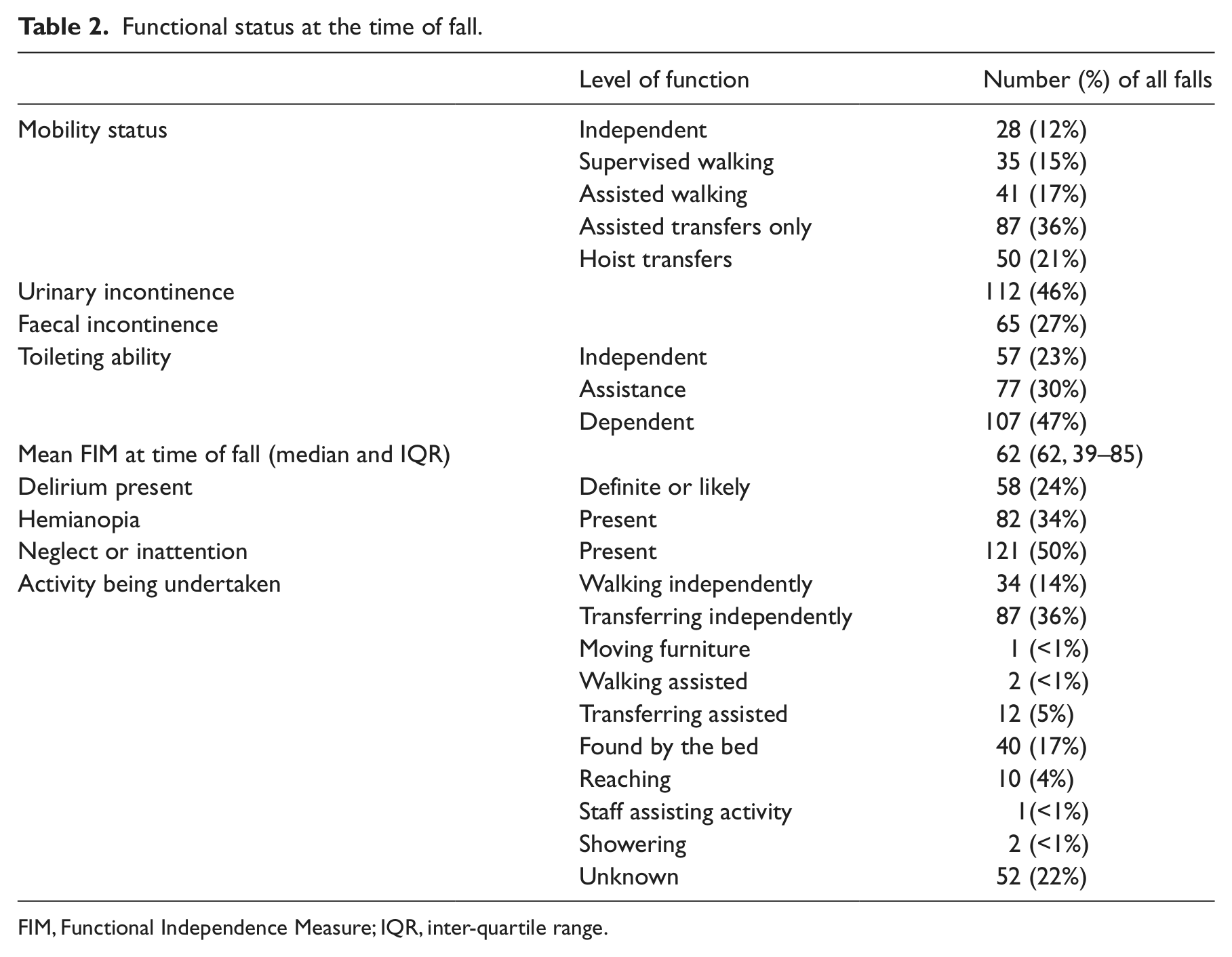
FIM, Functional Independence Measure; IQR, inter-quartile range.
Three (1.2%) falls resulted in major injury (fracture, dislocation, head injury or skin laceration requiring grafts or suturing) and there was no injury sustained in 176 (73%) of falls.
Taxonomy
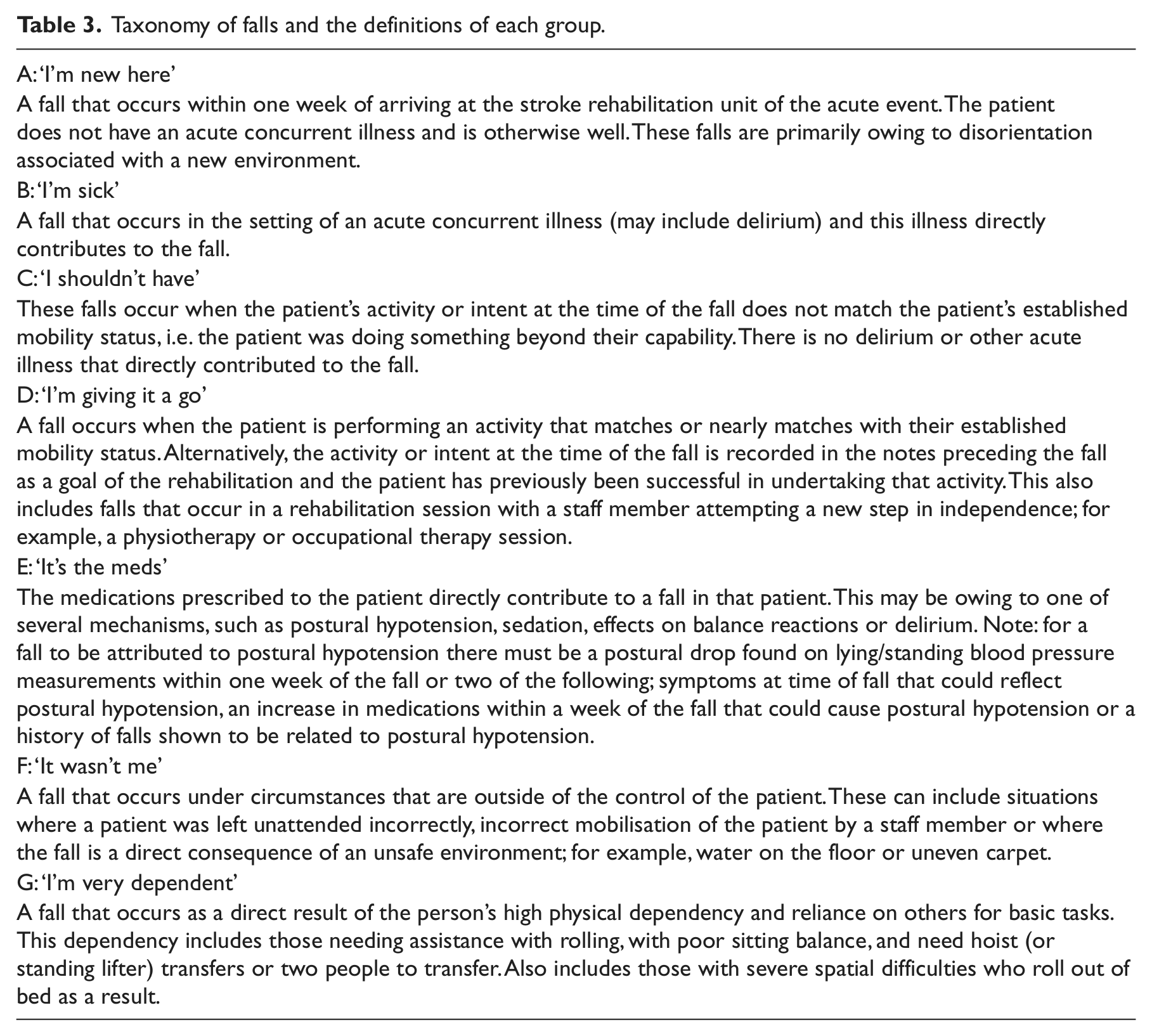
The categories and definitions for the taxonomy are shown in Table 3. The proportions of falls in each category are shown in Figure 1 with the degree of overlaps.
Taxonomy of falls and the definitions of each group.
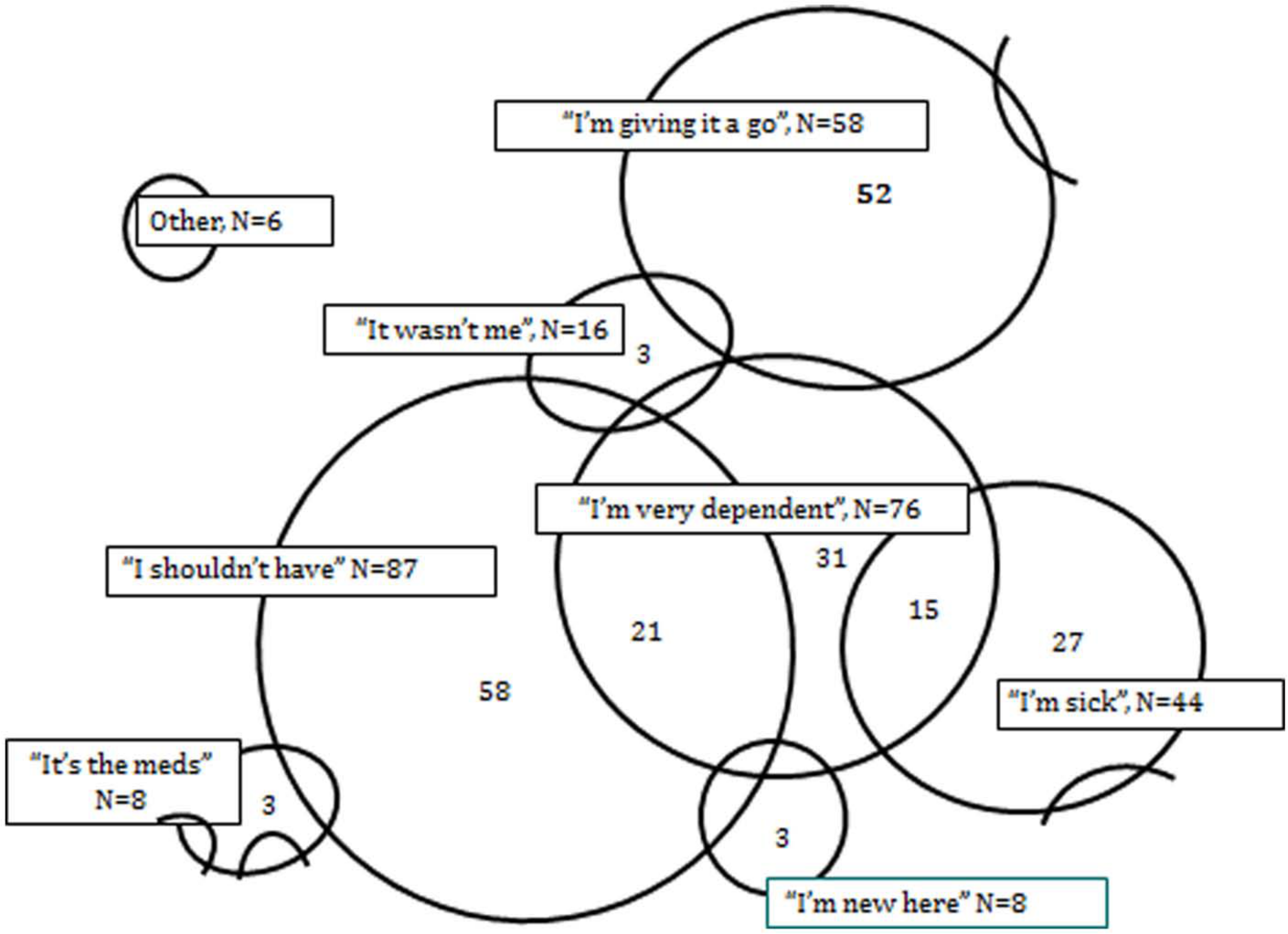
Taxonomy of falls, together with a schematic representation of the overlap between categories. Each fall may be in more than one category so total is greater than the 241 falls.
Time of fall characteristics for each fall category are shown in Table 4. While one patient may have several different types of falls during their admission, one type usually dominated. For the example given in Figure 2, C-type falls (‘I shouldn’t have’) dominated early in the stay, while D-type (‘I’m giving it a go’) and E type (‘It’s the meds’) falls dominated later.
Time of fall characteristics of falls in each fall category.
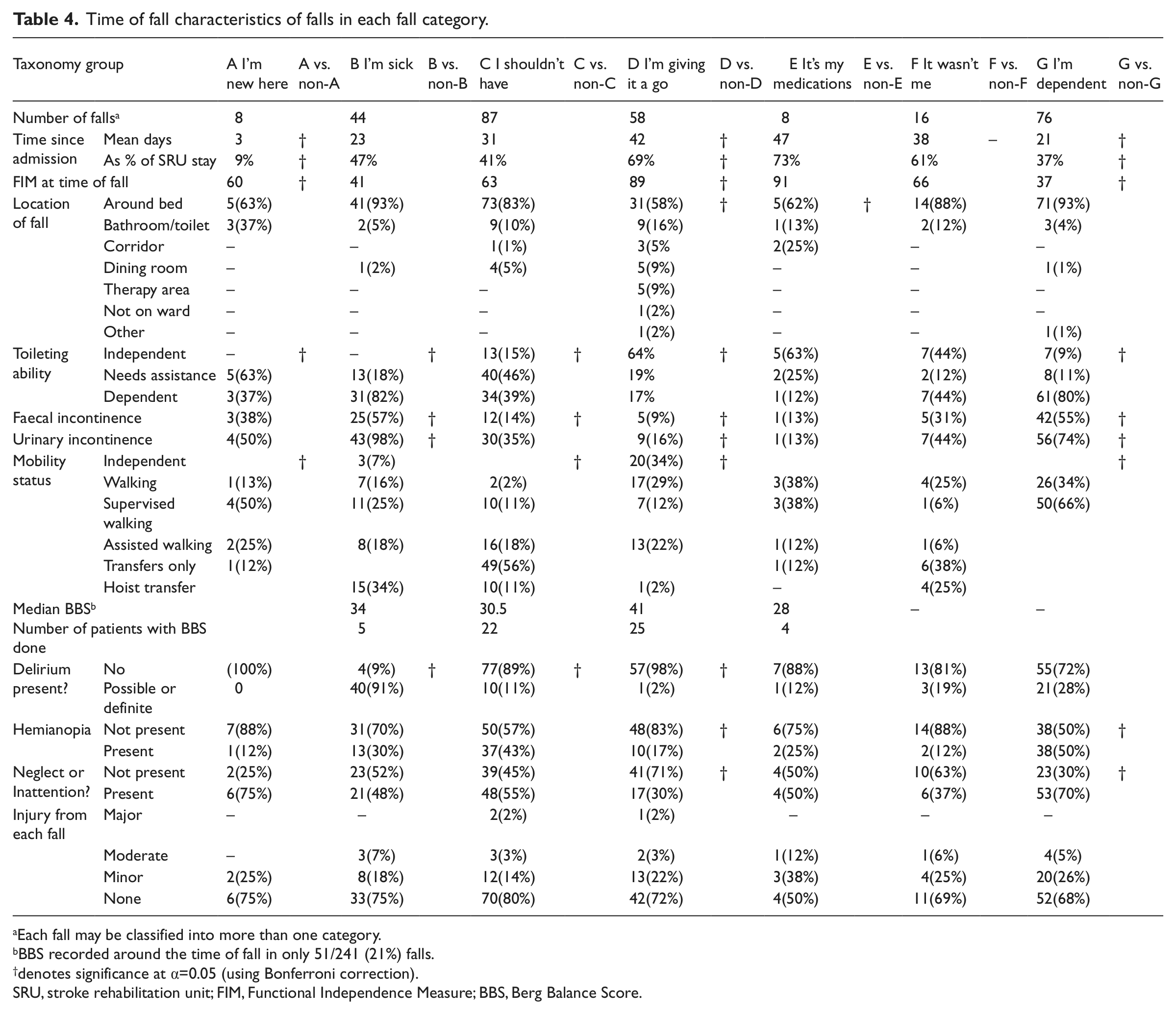
Each fall may be classified into more than one category.
BBS recorded around the time of fall in only 51/241 (21%) falls.
denotes significance at α=0.05 (using Bonferroni correction).
SRU, stroke rehabilitation unit; FIM, Functional Independence Measure; BBS, Berg Balance Score.
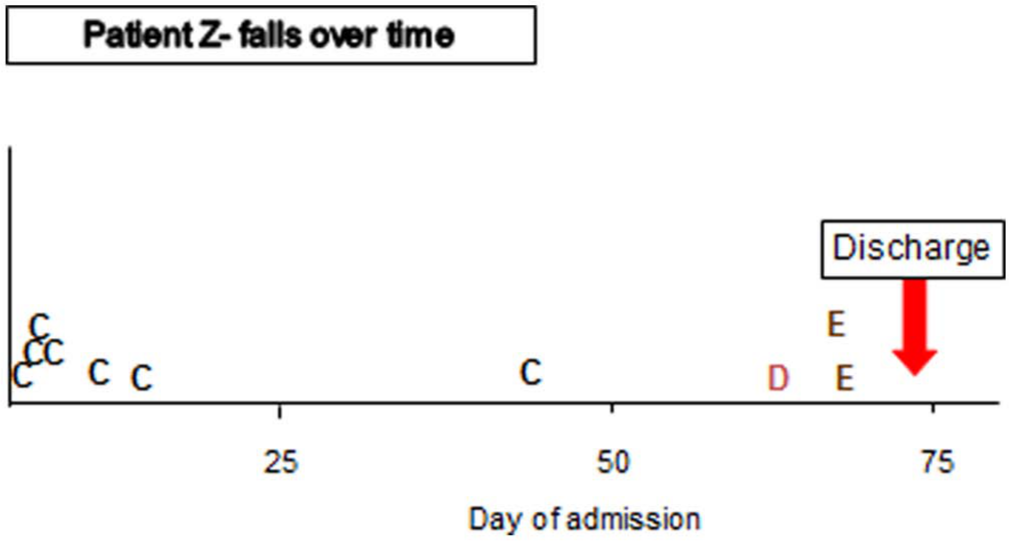
One patient’s falls over their inpatient stay. Each fall represented by a letter indicating type of fall (see taxonomy in Table 3 for definitions).
Outcomes for fallers (as opposed to falls) are shown in Table 5, where the taxonomy group shown is the main type of fall for any given patient.
Discharge outcomes for each taxonomy group (using predominant fall type for each faller, as opposed to falls).
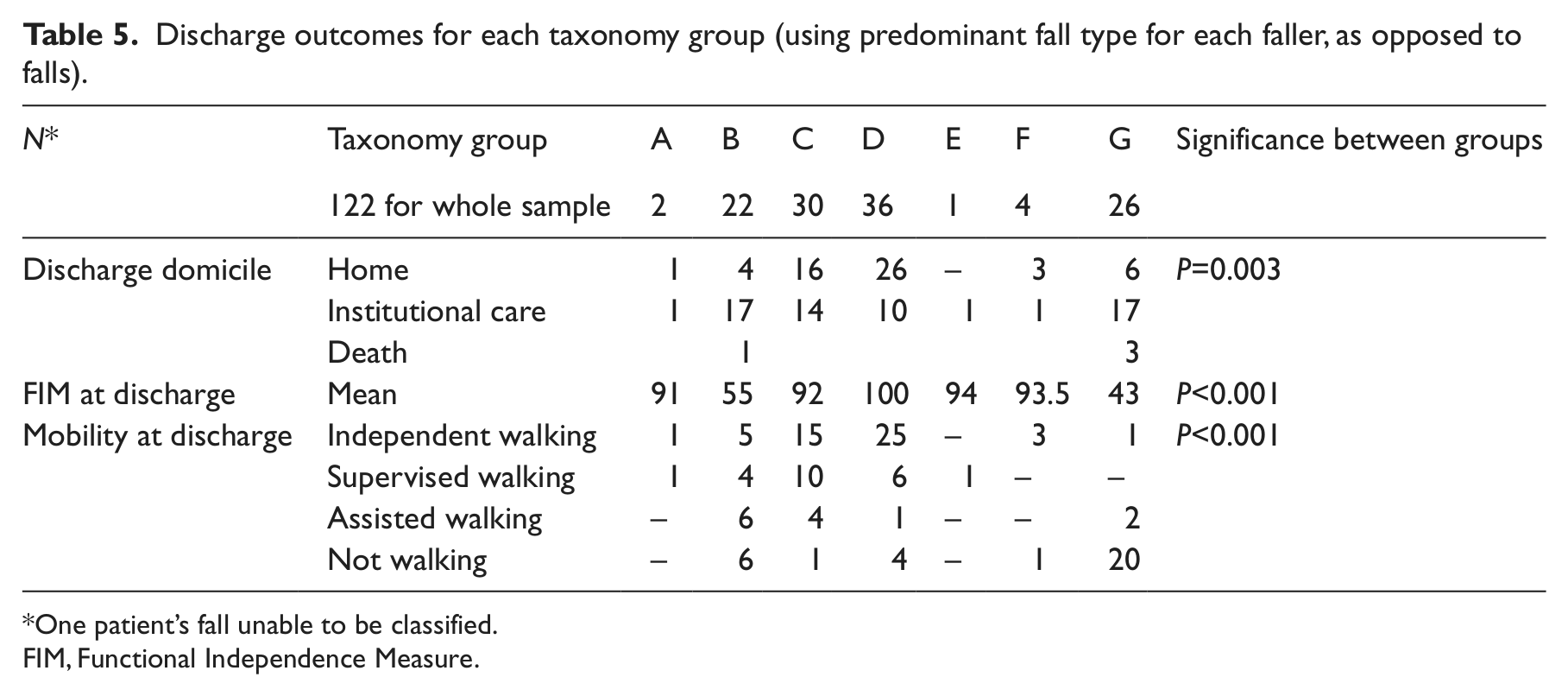
One patient’s fall unable to be classified.
FIM, Functional Independence Measure.
Discussion
In this study, falls could be divided into different fall subtypes, albeit with some overlap between groups. This taxonomy is based on the functional abilities and behaviours of the faller as well as the activity being undertaken at the time of each fall. It is apparent that some fall types are more prominent at the beginning of rehabilitation, when the patient is more dependent or sick, whereas falls later in admission may be owing to staff giving them greater independence.
This study confirms that not all falls are the same. Falls differ not only in apparent causation, but also in the functional abilities and behaviours of the patient at the time of falling, and the timing relative to admission. A clinical implication of these differences is that falls-prevention strategies need to be individualised to the patients’ needs and behaviours. To illustrate, a fall in an independently mobilising man who is almost ready for discharge has different needs to a dependent person who rolled out of bed owing to inability to appreciate where the edge of the bed is. Furthermore the outcomes of patients in each of the fall categories appear to differ as well.
Risk factors for falls in hospital can be broadly grouped into five key areas of mobility and balance problems, confusion and/or agitation, incontinence or toileting issues, previous falls and use of sedatives. 2 Our taxonomy is based not on risk factors prior to their fall, but the person’s functioning (including behaviour) at the time of fall. Despite this, there are some similarities with these risk factors, including poor judgement, toileting issues and impaired mobility. However there are also marked differences in this stroke rehabilitation cohort with very few medication-related falls whereas high physical dependency and visuospatial difficulties appear to have a greater influence.26,27 The minor role of medications was unexpected as the medications commonly prescribed in this group (antihypertensive and antidepressants) are also implicated in falls. 28
Furthermore our taxonomy highlights an additional group of falls where patients are taking what appear to be calculated risks as they attempt to regain independence. ‘I am giving it a go’ type falls (Group D) appear to be quite different to the other groups (Group E ‘it’s the medications’ also similar but very small numbers). These falls occurred later in the admission, at a time when the patients were more independent for mobility and toileting, and had less visuospatial difficulties and delirium. These patients fell during an activity that staff had deemed appropriate for them to do as they were regaining independence in mobility or ADL tasks. These activities are an integral part of rehabilitation and should be encouraged as they strive to regain independence. While there should be concern and investigation of the circumstances of each fall, there should not be unnecessary restrictions imposed on these patients just because they fell.
‘A unit where nobody falls is a unit where nobody moves’ 29 Bernard Isaacs 1992
The view that all falls in hospital are a negative indicator of quality of care may not apply to all groups of fallers.30,31 It is important to reduce unnecessary falls in hospital and to minimise injury as a result of falling. However, while reducing falls rate in this setting to zero might seem attractive, this may be neither realistic nor be reflective of optimal care. 32 Walking on two feet is inherently unstable and is even more so for those stroke patients as they struggle to regain these abilities. Rehabilitation is about promoting independence and autonomy for the individual and the rehabilitation process is associated with calculated risk taking. This risk taking needs to be adjusted according to the individuals’ abilities at the time and in line with their values. 33 We contend that some falls, such as these ‘I am giving it a go’ falls, may be a necessary part of calculated risk taking inherent in rehabilitation.2,34 Unnecessarily restricting their attempts at independence may compromise their longer-term goals of independence. In support of this, these ‘I am giving it a go’ patients had more favourable discharge outcomes of returning home, walking independently and higher functional abilities.
‘I’m dependent’ type falls (Group G) are at the opposite end of the fall spectrum from the ‘I’m giving it a go’ falls. These patients were highly dependent on staff for mobility and had a high prevalence of urinary and faecal incontinence as well as visuospatial problems. The majority of these falls occurred around the bedside. Rolling out of bed (as opposed to attempting to get out of bed) appears uncommon in general hospital population, 35 but in this group some rolled out of the bed. This may be owing to their visuospatial deficits. In contrast to Group D falls, these falls are potentially preventable as these patients are reliant on staff for all their mobility needs. Unfortunately, patients who had mainly ‘I’m dependent’ falls did not have favourable discharge outcomes with low FIM scores, and a high probability of being discharged to institutional care. It is unclear whether these poorer outcomes are related to the severity of their stroke or to their fall(s).
Group B (‘I’m sick’) had some characteristics similar to the dependent Group G above, but not surprisingly had a very high prevalence of delirium. Delirium in both its forms (agitated or hypoactive) impairs judgement and insight and is known as a major risk factor for falls in hospital.6,36 Like Group G, this subtype of faller had poorer outcomes. This may be mediated by the delirium itself, the underlying acute illness causing the delirium, the falls or because these were more severe strokes, which in turn are more likely to cause delirium. 37
‘I shouldn’t have’ falls are an intermediate and possibly heterogeneous group. By definition, this group were undertaking an activity that the staff did not think they were safe to do unsupervised or unassisted. They had intermediate prevalence of visual, visuospatial and mobility issues and appeared to lack insight into their deficits. In the notes, they were frequently described as ‘impulsive’. There was a high proportion of recurrent falls (65%) in this group, which may reflect this poor judgement, poor self-assessment of postural stability or limits, 38 retention of previous instructions and not learning from ‘mistakes’. This group had a wide range of outcomes: with some positive outcomes, but also some patients did poorly. It is the authors’ anecdotal experience that some patients go through this risky phase as they progress through their stroke rehabilitation. This is perhaps analogous to toddlers learning to walk, but falling often as they attempt to acquire new skills. This ‘risky phase’ contention is supported by some patients having several different types of falls during their admission (Figure 2).
Strengths and weaknesses
The records for all fallers over the study period were reviewed, with first and recurrent falls included, thus providing a representative snapshot of all falls on a stroke rehabilitation unit. An important difference in this study was the assessment of function at time of fall, rather than admission characteristics. The collection of this data was limited to what was written in the notes. This is both a strength and weakness – strength in that it reflects contemporaneous function, but limiting as the absence of documentation may not always mean absence of that characteristic. This was mitigated by undertaking a full case note review to ascertain functional abilities, rather than sole reliance on QIER data, which has been shown to be very sparse on detail. 39 Formal tests were not required to make a judgement of neglect or delirium, but instead the written judgements of experienced stroke unit staff were used, supplemented by any formal tests already undertaken. This approach is less standardised, but allows for detection of fluctuating conditions, such as delirium. Similar to other studies, the majority of falls are unwitnessed2,3 so potential causes of fall needed extrapolation. This adds a subjective element to the classification of each fall. However, we tried to mitigate this by maximising the amount of information about the fall prior to determining a fall category. An ideal method is direct observation, such as video cameras, but even this method is limited as it could not capture falls in bedrooms and bathrooms where the majority of our falls occurred. 40 In addition, this study has the weaknesses of any single centre, retrospective review. All the above limit generalisability to other cohorts. Despite these shortcomings, the study was able to define different types of falls with different outcomes.
The different fall types found suggests that fall prevention strategies need to be individualised and what works for one person, or group of people, may not work for another. It is unclear what should be done for the ‘I’m giving it a go’ fallers – restricting their activities seems less appropriate as this will also deprive them of opportunities to practise and regain independence. In this group, injury prevention, such as hip protector use may be more appropriate. In contrast, highly dependent patients and sick patients are particularly vulnerable and need vigilance from staff to prevent falls. Bedrails for some of these dependent immobile patients with visuospatial difficulties who are likely to roll out of bed may be one strategy. 41 Perhaps the most challenging group are the intermediate ‘impulsive’ patients (‘I shouldn’t have’) – their lack of insight, poor planning or visuospatial skills make them particularly at risk as they attempt to mobilise. Extra vigilance from staff, regular walking or toileting, delirium strategies and sensor alarms may be some appropriate fall prevention options.
Clinical messages
Retrospective classification of falls is possible, has face validity and the groups have different outcomes.
The differences in fall types and outcomes may have implications for fall prevention strategies.
Footnotes
Acknowledgements
The authors are grateful to the Editor and the two anonymous reviewers for their helpful comments.
Contributors
All authors contributed to the design of the study and the development of the taxonomy. KLW collected the raw data. HCH wrote the first draft of the article and all authors contributed to subsequent drafts.
Conflict of interest
The author declares that there is no conflict of interest.
Funding
KLW received a summer student grant from Older Persons Health Specialist Services that enabled her to undertake the study. No other funding was received.