
Abstract
Objective:
To evaluate the effect of progressive resistance strength training as additional training measured on functional outcomes in older hospitalized patients.
Design:
A single-blinded randomized controlled trial.
Setting:
Department of Geriatric Rehabilitation in university hospital.
Participants:
A sample of 71 patients were successively included and randomized either to the treatment group (TG) (n = 36) or the control group (CG) (n = 35). Fifteen participants dropped out (TG n = 7; CG n = 8), leaving 56 participants with a mean age of 79 (SD 7).
Intervention:
Participants in the treatment group were treated in groups with progressive resistance strength training in addition to standard care. Progressive resistance strength training of the lower extremities was performed in three sets of 12–15 repetitions, intensity 60–70% of one repetition maximum, in four 50-minute sessions per week.
Main measures:
The effect was evaluated by timed up & go test, 30-second chair-stand test, 10-m walk test, three tasks (transfer, walking, stairs) of the Barthel Index, and use of walking aids.
Results:
Significant improvements in the 10-m walk test (P < 0.01) and Barthel Index (walking) (P = 0.01) were demonstrated within the treatment group but not in the control group. Both groups had significant improvements in timed up & go, 30-second chair-stand (modified) and Barthel Index (transfer and walking). No significant difference was found between groups except for the Barthel Index (stairs) (P = 0.05). Analysis by the mixed-effects model showed that the treatment group improved more than the control group in all outcome variables.
Conclusion:
The results indicate that for older hospitalized patients progressive resistance strength training as additional training may have an effect compared to standard care, but no statistically significant effects were demonstrated when measured by functional outcomes.
Introduction
Strength training is a key component in the rehabilitation of older hospitalized patients. Reduced muscle strength in the lower extremities affects not only functions like walking, stair climbing and standing from a sitting position but also activities of daily living, occurrence of falls 1 and discharge destination. 2
A large number of diseases require hospitalization with prolonged bed rest and physical inactivity. Bed rest decreases muscle strength by 1.0–1.5% per day, 3 and inactivity-induced loss of muscle mass, which predominantly affects the lower body musculature, is especially rapid during the initial days/weeks of inactivity.4–6
In addition to disease and inactivity, muscle strength is affected by the ageing process in muscle mass and capacity as a result of neuromuscular changes.7–11 Muscle strength shows a slow decrease until about 50 years of age; thereafter it declines at 12–15% per decade, with yet more rapid loss above the age of 65. 12
Progressive resistance strength training belongs to ‘the dynamic external resistance’ model 13 and is defined as a training method in which the load is gradually increased to facilitate adaptation. Progressive resistance strength training is an effective method for improving muscle strength because it induces higher levels of neuromuscular activation than functional exercises. 14 This type of strength training is recommended for older people because of its significant effects on neuromuscular function.11,15,16
Several studies on progressive resistance strength training in older people have reported increased muscle strength and amelioration of some functional limitations.15–17 However, few studies have included older hospitalized patients and those that did showed non-significant or small effects.18,19
The objective of this study was to evaluate the effect on functional outcomes of progressive resistance strength training as additional training for older hospitalized patients.
Methods
Between 1 September 2006 and 1 January 2008, older patients from the Department of Geriatric Rehabilitation at Copenhagen University Hospital, Glostrup, Denmark were successively referred by medical doctors for regular physiotherapy and were screened by medical records for participation.
The inclusion criterion was ability to stand independently with or without walking aids (rollator, crutch) or bed/bench support. Exclusion criteria were: expected length of stay < 7 days; dementia, according to medical record; inability to communicate, as evaluated by medical staff at the department; inability to be active, as evaluated by medical staff at the department. The participants received verbal and written information and signed an informed consent before study entry.
The study was approved by the Ethical Committee of Copenhagen County (H-KA-2006-0144) and registered in the Danish Register for Data protection and in Clinical Trials.gov Protocol Registration System (Clinical Trials ID: NCT01371097).
Design
The design was a prospective single-blinded randomized controlled clinical trial. All participants had a three-day run-in period with baseline registration and pre-test. After the run-in period they were randomized to either treatment group or control group by a randomized procedure using sealed, numbered envelopes.
The randomization was performed by a physiotherapist with no other links to the study.
The post-test took place directly after the intervention and before discharge.
The randomization code remained blinded for the two assessors (who were physiotherapists) until the last participant had been tested.
Intervention
Participants randomized to the treatment group were treated at the Department of Geriatric Rehabilitation, in groups of between one and six with a frequency of four sessions per week. 20 Each session lasted 50 minutes and was supervised by two of the same four trained, experienced rehabilitation physiotherapists.
The treatment was carried out in three sets of 12–15 repetitions, 20 with an intensity of 60–70% of one repetition maximum (1RM). 1RM was defined as the heaviest load the participant could lift once throughout the completed range of motion. The intensity and progression of load was assessed from the participant’s perception of difficulty using a modified Borg Scale. 21
Intensity was increased by 0.5 kg (sand bag) in the backpack and by an elastic band with different resistance when the participant reported that the load was: easy or moderate on the modified Borg Scale and could do more than 15 repetitions.
The ordinal scale was graded into easy, moderate and hard.
Each set consisted of the following:
Exercises for the hip adductor muscles, knee flexor and extensor muscles performed in sitting position.
Stand up from sitting to standing position with a backpack loaded with weights.
Walking sideways with an elastic band fixed round the ankles as resistance.
Elevation up and down on the toes with a backpack loaded with weights. The participants performed in standing position, starting from a position with slight dorsal flexion in the ankle joints. The participants stood on a step bench without heel contact on the ground.
Training in a weight-adjustable, stair-stepping machine (Power-step). 22
All participants in both groups received regular physiotherapy (standard care) while in the Department of Geriatric Rehabilitation.
Measurements
The outcome was measured by five functional parameters: timed up & go test, 30-second chair-stand test, 10-m walk test, three tasks of the Barthel Index, and use of walking aids.
Timed up & go test (primary outcome)
The timed up & go test assesses basic functional mobility. 23 The participants had three attempts with the best time being recorded. Likewise, walking aids used at pre- and post-test were recorded. The timed up & go test has been tested for intra-rater, inter-rater and test–retest reliability and validity in older people.24–26 The test–retest reliability of the timed up & go test in older people showed that the slower the participants performed the test, the more the variance increased. 27
The 30-second chair-stand test (primary outcome)
The 30-second chair-stand test is part of the Senior Fitness Test, 28 which reflects lower body muscle strength and functional capacity in older adults. It has a moderately high correlation between chair-stand performance and maximum weight-adjusted leg-press performance for both men and women, which supports the criterion validity of the chair stand as a measure of lower body muscle strength. 28 Construct validity was demonstrated by the test’s ability to detect differences between community-dwelling older adults of various ages and levels of physical activity. 28 The 30-second chair-stand test is a reasonably valid and reliable indicator of lower body strength in generally active community-dwelling older adults. 28 The original version in English has been translated and culturally validated into Danish 29 using accepted translation methodology. The participants were also measured by a modified 30-second chair-stand test in which they used upper extremities and the arm rests.
The 10-m walk test (primary outcome)
The 10-m walk test 30 assesses the maximum walking speed over a short distance. The participants started from a standing position and continued walking for 10 m. The fastest of three attempts was recorded. The test–retest reliability of the 10-m walk test in older people showed high reliability. 31
Three tasks of the Barthel Index (secondary outcome)
The Barthel Index 32 consists of ten functional items, three of which focus on moving and walking. Item 8 ‘transfer’ assesses the ability to move and is rated on a 0-, 5- and 10-point ordinal scale. Item 9 ‘walking’ assesses the ability to walk rated on a 0-, 5- or 10-point scale. Item 10 ‘stairs’ assesses the ability to walk on stairs and is rated with 0, 5, 10 or 15 points. A score of 0 indicates complete dependency and 15 indicates independence. The Barthel Index has been recommended by the Royal College of Physicians 33 for routine use in the assessment of older people, 34 although de Morton found it to have limited validity for measuring and monitoring the health of older medical patients. 35 The test–retest reliability of individual items of the Barthel Index in older people showed low reliability. 34
Walking aids (secondary outcome)
Use of appropriate walking aids was assessed by a modified version of the Functional Ambulatory Categories Classification, consisting of six items (walk independently without any walking aids, walk with one crutch, walk with two crutches, walk with rollator, walk with a high frame on wheels, no ability to walk).36,37 Rating was done on an ordinal scale from 0 (no ability to walk) to 25 points (walk independently without any walking aids). Validity and reliability of scores in the Danish version in older patients has not been published to the author’s knowledge.
Statistical analysis
Statistical analysis was carried out using IBM SPSS (Statistical Package of Social Science) version 18 (SPSS Inc, Chicago, IL, USA). The results are presented as mean ± standard deviation for data measured by continuous scales and as number and percent for data measured on ordinal scales. Null-hypotheses between groups were tested by the Mann–Whitney U-test and the Wilcoxon test within groups. In addition, the effect of the treatment was tested by including the interaction between treatment and period in the mixed effects model.
Sample size was estimated by a power calculation in which an assumption of an improvement of three repetitions at 30-second chair-stand test was needed to consider the outcome to be clinically relevant. Improvement on three repetitions was based on (a) data in a Danish National Geriatric Database including baseline registration scores of the 30-second chair-stand test, which showed a baseline score of approximately 5 and (b) that a score above 8 on the 30-second chair-stand test indicates, irrespective of age, less risk of loss of functional ability according to the Senior Fitness Test Manual, Human Kinetics. 29
With 90% power (β = 0.9) and a significance level at P = 0.05, the power calculation showed that a total of 56 participants were needed for the study.
For all tests, the level of significance was set to P < 0.05.
Results
Participants
Medical records of 225 older patients were screened for inclusion; 131 found to be eligible were invited to participate. Seventy-one participants accepted the invitation and were randomized: 36 in the treatment group and 35 in the control group.
Fifteen (21%) participants dropped out: 7 from the treatment group and 8 from the control group. Thus, 56 participants with mean age 79 (SD 7) years completed the study: 29 in the treatment group and 27 in the control group (Figure 1).
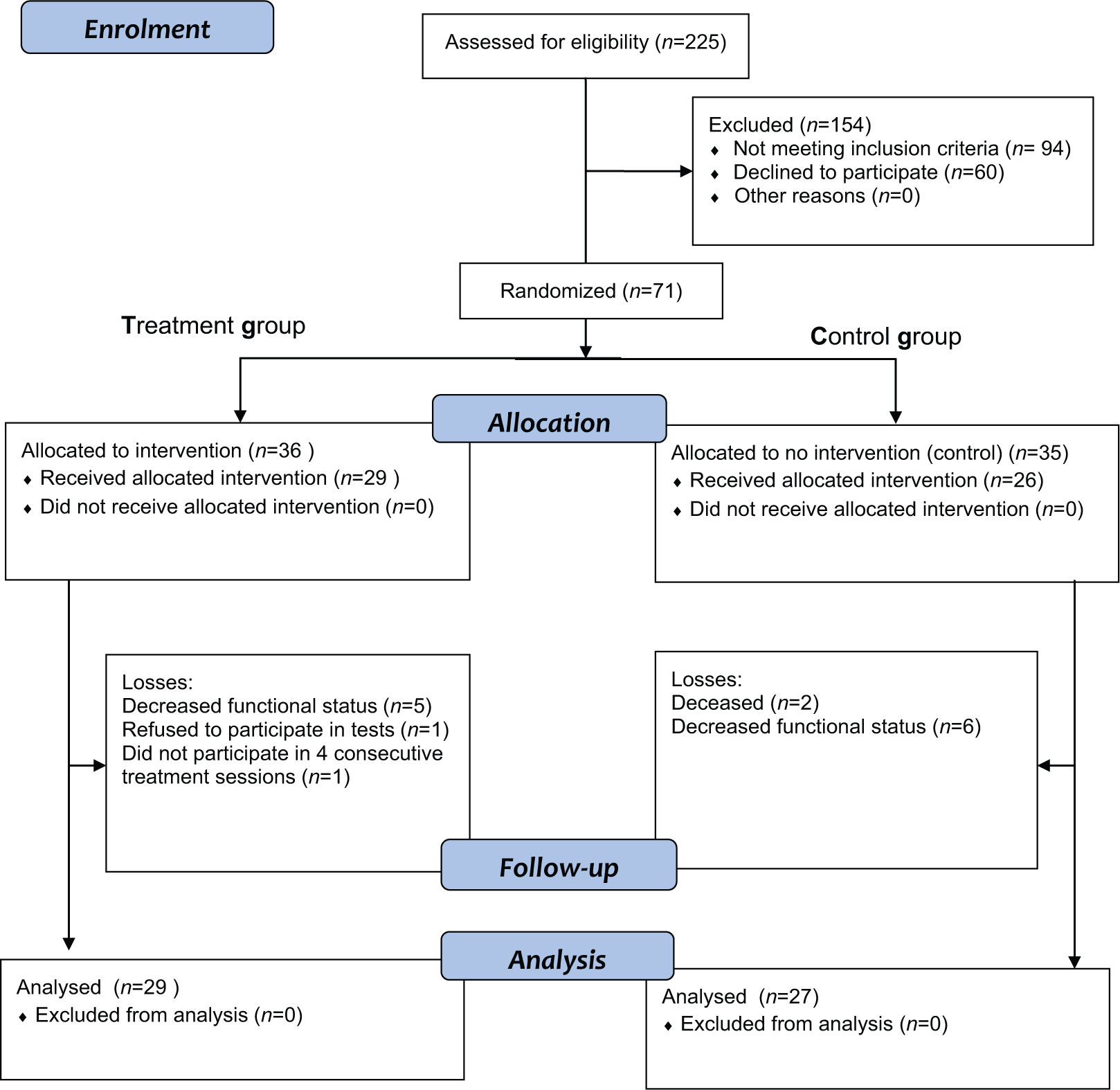
Flow diagram of the study.
Mean treatment session attendance rate in the treatment group was 10 (SD 7) and mean total intervention time was 8 hours 20 minutes (SD 6 hours).
Characteristics
Baseline demographic characteristics of the participants who completed the study are presented in Table 1. There were no significant differences between the two groups.
Demographic baseline characteristics of 56 randomized hospitalized older patients, excluding drop-outs.
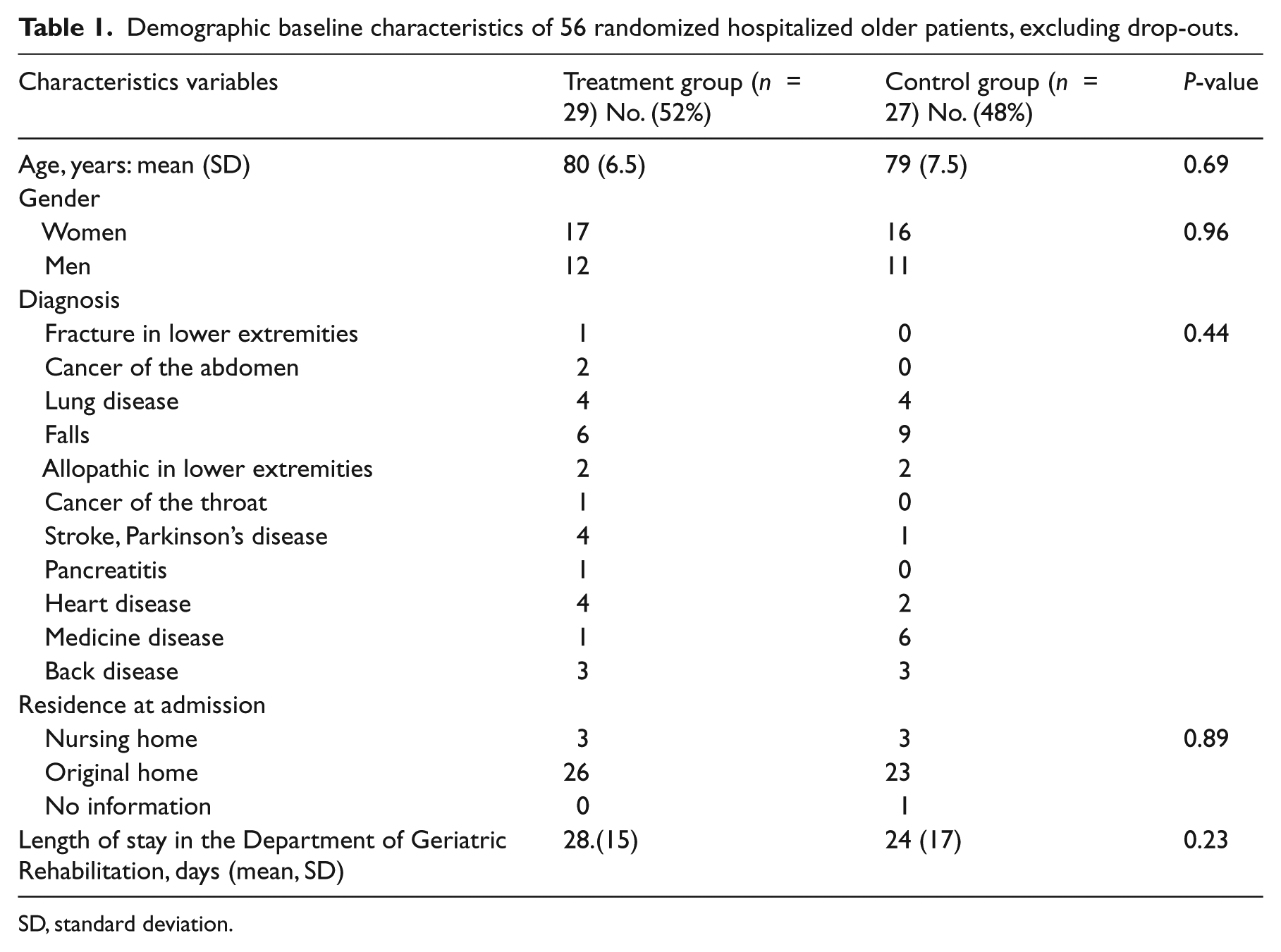
SD, standard deviation.
There was no significant difference in baseline demographic characteristics between participants who completed the study and those who dropped out, except for length of stay at the Department of Geriatric Rehabilitation (P = 0.02).
Outcome data were missing from 4 (7%) participants in the Barthel Index and 34 (39%) participants in the 30-second chair-stand (modified) (Table 2).
Results within and between treatment group and control group of progressive resistance strength training as additional training in older patients in hospital.
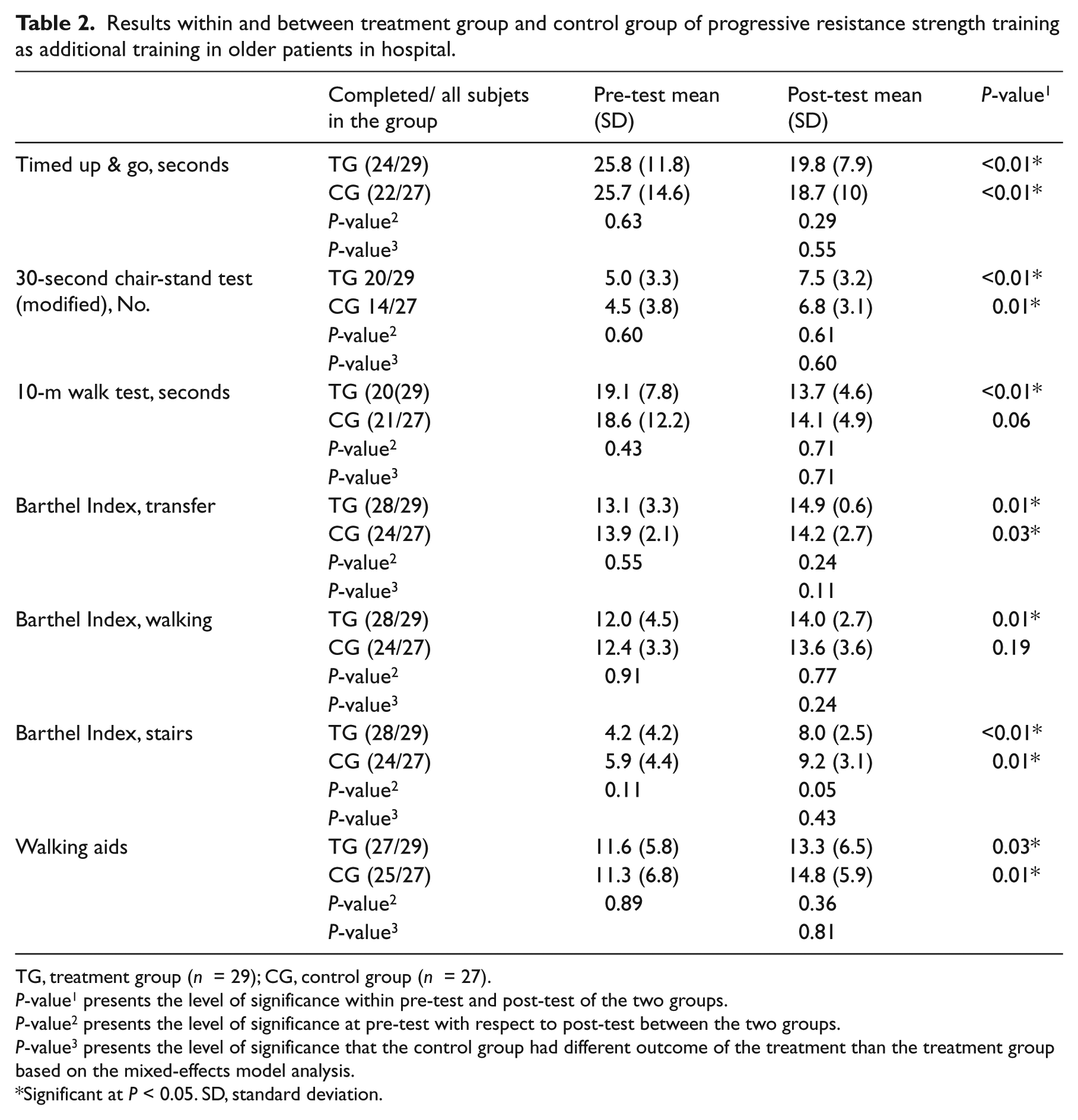
TG, treatment group (n = 29); CG, control group (n = 27).
P-value1 presents the level of significance within pre-test and post-test of the two groups.
P-value2 presents the level of significance at pre-test with respect to post-test between the two groups.
P-value3 presents the level of significance that the control group had different outcome of the treatment than the treatment group based on the mixed-effects model analysis.
Significant at P < 0.05. SD, standard deviation.
Measured effects
The results (Table 2) showed no significant difference between the treatment and control groups, either at pre-test or at post-test measured by any parameters. The only trend toward significant effect was in the treatment group (P = 0.05) measured by the Barthel Index (stairs) as compared to the control group.
Analysis by the mixed-effects model showed that the treatment group improved more than the control group in all outcome variables, but in no case was there any statistically significant effect (P-value3 in Table 2).
A significant change in the treatment group, not shown in the control group, was measured by the 10-m walk test (P < 0.01) and the Barthel Index (walking) (P = 0.01) (Table 2).
Only four participants completed the 30-second chair-stand test (standard); this number was too small for statistical analysis and the results from this test are not presented here.
Discussion
The present randomized controlled trial evaluating the effect of progressive resistance strength training as additional training showed no significant improvement measured on functional outcomes for older hospitalized patients. However a trend was shown in one out of five outcome variables, and analysis by the mixed-effects model showed that the treatment group improved more than the control group in all outcome variables.
A previous study by Latham et al. reported a positive effect of progressive resistance strength training compared to regular physiotherapy in older hospitalized patients measured by timed up & go test. 19 This is in contrast to our findings. However, their study was inadequate in power (n = 20) and they did not used unblinded assessors. 19 Recently, Liu et al. published a meta-regression analysis of randomized controlled trial outcome assessors in 73 trials in older adults. The results showed that the use of blinded assessors (n = 18) tend to report smaller effect size than those who did not (n = 55) with a difference of −0.80 (95% confidence interval, −1.35 to −0.25). 38 In our study we used blinded outcome assessors to increase the internal validity of the study.
Donald et al. reported positive effects within groups of progressive resistance strength training comparing two modes of physiotherapy: (a) progressive resistance strength training in addition to regular physiotherapy versus (b) conventional physiotherapy, both measured by 10-m walk test in older hospitalized patients. The results did not show significant improvement between groups, which is in agreement with our results. 18 Latham et al. also showed a positive effect within groups of progressive resistance strength training measured by 10-m walk test, but again with non-significant effect between groups. 19
With regard to our results measured by the 30-second chair-stand test, we did not find any published studies to compare with; this was also the case with the results measured by the three tasks of Barthel Index. Our results measured by the item ‘stairs’ approached a significant effect (P = 0.05) between the two groups in favour of the treatment group. This finding could be a major clinical information for a future study regarding discharge destination for older hospitalized patients. 39
There are several methodological issues in this study that need to be addressed. The first is the large number of drop-out events caused by the low level of physical functioning in the participants. Higher levels of physical functioning in the inclusion criteria might have reduced the number of drop-outs. Hence the participants might not be representative of the patients at the Department of Geriatric Rehabilitation and thus there is a risk of selection bias. The fact that the number of drop-outs was smaller in the treatment group than in the control group indicated that progressive resistance strength training was not the cause for dropping out.
Based on this large number of drop-outs, some authors recommend an intention-to-treat analysis,16,40 which may lead to small changes in the results.
Second, the large amount of missing outcome data lessens the internal validity of the study. However, the numbers were almost identical for the two groups. The amount of missing data increased markedly from 7% in the Barthel Index to 39% in the 30-second chair-stand modified test. One explanation may be the low level of physical functioning in the participants, which gave a ‘floor effect’, with only four participants completing the 30-second chair-stand (standard) test. This was similar to the study by Donald et al., in which only 59% of older inpatients tested completed strength measurements at admission and discharge. 18
Recently, de Morton et al. argued for more clinically relevant and valid instruments to measure changes in functional mobility across the spectrum from bed-bound patients to those with functional independent mobility.35,41 Since, then de Morton et al. have developed a new instrument, the De Morton Mobility Index (DEMMI), 42 which provides clinicians with an accurate and valid method of measuring the mobility of geriatric patients in the subacute hospital setting. 43
The third issue is the low intensity of progressive resistance strength training in the training. The minimum intensity that has been shown to increase strength in young healthy Individuals is 60–65% of 1RM. However, 50–60% of 1RM has been shown to increase strength in special populations. 44 In the present study we have chosen a low intensity of progressive resistance strength training performed by backpack with load, step machine and elastic band, as it might be problematic to maintain adherence to training at a higher intensity of progressive resistance strength training such as more exhausting training or complex and non-functional equipment. Furthermore, a backpack and elastic band system was relevant, inexpensive and easy to handle. Likewise, a low intensity of progressive resistance strength training in the training was chosen to reduce the risk of loss of motivation. Stand up from a chair and stair climbing, however, demand close to 100% of maximum strength for older inpatients.
Training in a group has a beneficial social effect due to the motivation, but requires close supervision by the physiotherapist to ensure safety, such as prevention of illness and falls. In the first phase of the study by Latham et al. 19 safety was investigated before progressive resistance strength training intervention was used for older hospitalized patients. In our study no adverse events such as injuries, falls or increased pain were reported associated with the intervention or tests.
The fourth issue is the short period of training, as at least 10 weeks are needed for the benefits to be clear. 45 However, 10- to 12-week stays for strength training are not realistic for acute university hospitals.
Further research is suggested to investigate the possible effects of progressive resistance strength training as additional training providing extra physical therapy in older hospitalized patients 46 and using the new DEMMI instrument. 42 Recently, a systematic review by Peiris et al. showed that extra physical therapy, defined as longer or more frequent sessions, decreases the length of stay in hospital and significantly improves mobility, activity and quality of life. 46
In conclusion, this randomized controlled trial showed that progressive resistance strength training as additional training in older hospitalized patients did not demonstrate any significant effect measured by timed up & go, 30-second chair-stand test, 10-m walk test, Barthel Index (transfer, walking) and use of walking aids, except for the Barthel Index (stairs). However, the analysis by the mixed-effects model showed that the treatment group improved more than the control group in all outcome variables, but with no measure statistically significant effect.
Clinical messages
It is possible to treat older inpatients with progressive resistance strength training as additional training. However, even with selection it is suitable for only around 50% of all patients.
Progressive resistance strength training as additional training in older inpatients has at best small effects on functional outcomes.
Footnotes
Acknowledgements
The authors thank the staff at the Department of Geriatric Rehabilitation and the Department of Physiotherapy and Occupational Therapy, Copenhagen University Hospital, Glostrup for their assistance. They also thank all the patients for participating the study.
Conflict of interest
No commercial party has provided financial support for this study or has any financial interest in the results of this study. The authors declare that there are no conflicts of interest.
Funding
This study was supported by the Department of Physiotherapy and Occupational Therapy, Copenhagen University Hospital, Glostrup, Denmark and a grant for the staff with Medium Term Education, Copenhagen University Hospital, Glostrup, Denmark.