
Abstract
Objective:
To determine whether EMG-triggered electrical stimulation applied to multiple muscles daily is a feasible intervention and to determine its effect on strength and activity in very weak stroke patients.
Design:
A prospective, randomized trial with blinded assessment.
Setting:
Metropolitan mixed acute and rehabilitation units.
Participants:
Thirty-three people within four weeks of a stroke with less than Grade 3 strength in three out of four muscle groups (shoulder flexors, elbow extensors, wrist and finger extensors and thumb abductors) of the affected arm.
Interventions:
Participants were randomly allocated to receive EMG-triggered electrical stimulation to the four muscle groups of the affected arm plus usual therapy five times a week for four weeks, or usual therapy only.
Main measures:
Feasibility of the intervention was measured by examining compliance with the trial protocol. Strength was measured using manual muscle testing summed across muscle groups (0–20). Activity was measured using the Motor Assessment Scale, summed upper limb items (0–18).
Results:
The experimental group received 87% of the intervention. Following the intervention period, there was no difference between the groups for strength (mean between-group difference, 0 out of 20, 95% confidence interval (CI) −3 to 3, p = 0.91) or activity (mean between-group difference 1 out of 18, 95% CI −2 to 4, p = 0.44).
Conclusions:
It is feasible to apply EMG-triggered electrical stimulation to multiple muscles of the upper limb in very weak people early after stroke. However, it does not appear to improve strength or activity beyond usual arm therapy that contains strengthening.
Introduction
Following stroke, the primary impairment contributing to activity limitations is loss of strength.1–3 Numerous descriptive studies have reported significant correlations between muscle strength and activity after stroke. 4 Longitudinal studies measuring muscle strength and other impairments including dexterity, sensation, contracture and spasticity, identify strength as the impairment with the largest impact on activity.5–7 Hence the importance of increasing strength after stroke is now widely acknowledged.
Reviews of the effect of progressive resistance exercise (PRE) on strength after stroke support the use of PRE to increase strength8,9 and guidelines also recommend the use of PRE after stroke. 10 Hence there is information to guide practice for muscles that are strong enough to move against resistance and can use PRE for further strengthening. However, there is very little information to guide practice in strengthening very weak muscles, i.e. those that have too little strength to move against resistance and therefore cannot use PRE. In a systematic review of all interventions with the potential to increase strength after stroke, in which there were 14 trials in the pooled analysis of strength outcomes, only five of these trials were in people with very weak muscles. 11 The interventions used in very weak muscles included electrical stimulation, which was shown to have a moderate effect on strength in people that are very weak early after stroke, and EMG biofeedback, which was shown to have a large effect on strength in people that are very weak late after stroke. 11 EMG-triggered electrical stimulation combines EMG biofeedback and electrical stimulation, and has been shown to be more effective than cyclical electrical stimulation. 12
In very weak muscles, increases in strength may well carryover to the activity level, since at low levels of strength, even small increases in strength result in large increases in activity.4,13 However, to make a difference at the level of activity, it is likely that strength needs to be increased in multiple muscles. Therefore, in the current trial, four muscle groups of the affected arm were targeted in order to enhance carryover to activity. The four muscle groups chosen were the shoulder forward flexors, elbow extensors, wrist extensors and thumb abductors, as these muscles are all involved in reach and grasp activities of the arm.
Considering that most recovery is made in the acute and subacute phases after stroke, 14 attempting to maximise strength gains early in order to allow people to do more task-specific training is vital. Therefore, this pilot trial targeted individuals with very weak arm muscles early after stroke. The rationale for the trial was that the application of EMG-triggered electrical stimulation to four major muscles of the arm, in addition to usual arm therapy, was likely to be a feasible intervention and have a significant effect, not only on strength but also on activity. If this could be shown to be a feasible and effective intervention in this patient population, it has the potential to significantly improve outcomes. Therefore, the research questions were as follows.
Is it feasible to apply daily EMG-triggered electrical stimulation to four muscle groups (shoulder flexors, elbow extensors, wrist and finger extensors and thumb abductors) of the affected arm in addition to usual arm therapy in acute stroke patients?
Does EMG-triggered electrical stimulation to four muscle groups of the affected arm after stroke result in increased strength and arm activity compared with control participants?
Methods
An assessor-blinded, prospective randomized controlled pilot trial was undertaken (Figure 1). Very weak, acute stroke patients admitted to the stroke units of two metropolitan hospitals were screened and randomly allocated to the experimental or the control group. The allocation sequence used random permuted blocks of two and four. These were computer generated before commencement of the study and centrally located, thereby concealing randomization from the recruiter. After recruiting a participant, the recruiter telephoned the central location to find out the participant’s group allocation. Both groups received four weeks of usual arm therapy and the experimental group also received EMG-triggered electrical stimulation to four muscle groups of the affected arm. Measures were taken at baseline, at Week 4 (the day following the last intervention) and at Week 12, by a blinded measurer. The trial was approved by the relevant Human Research Ethics Committees and all participants gave written informed consent.
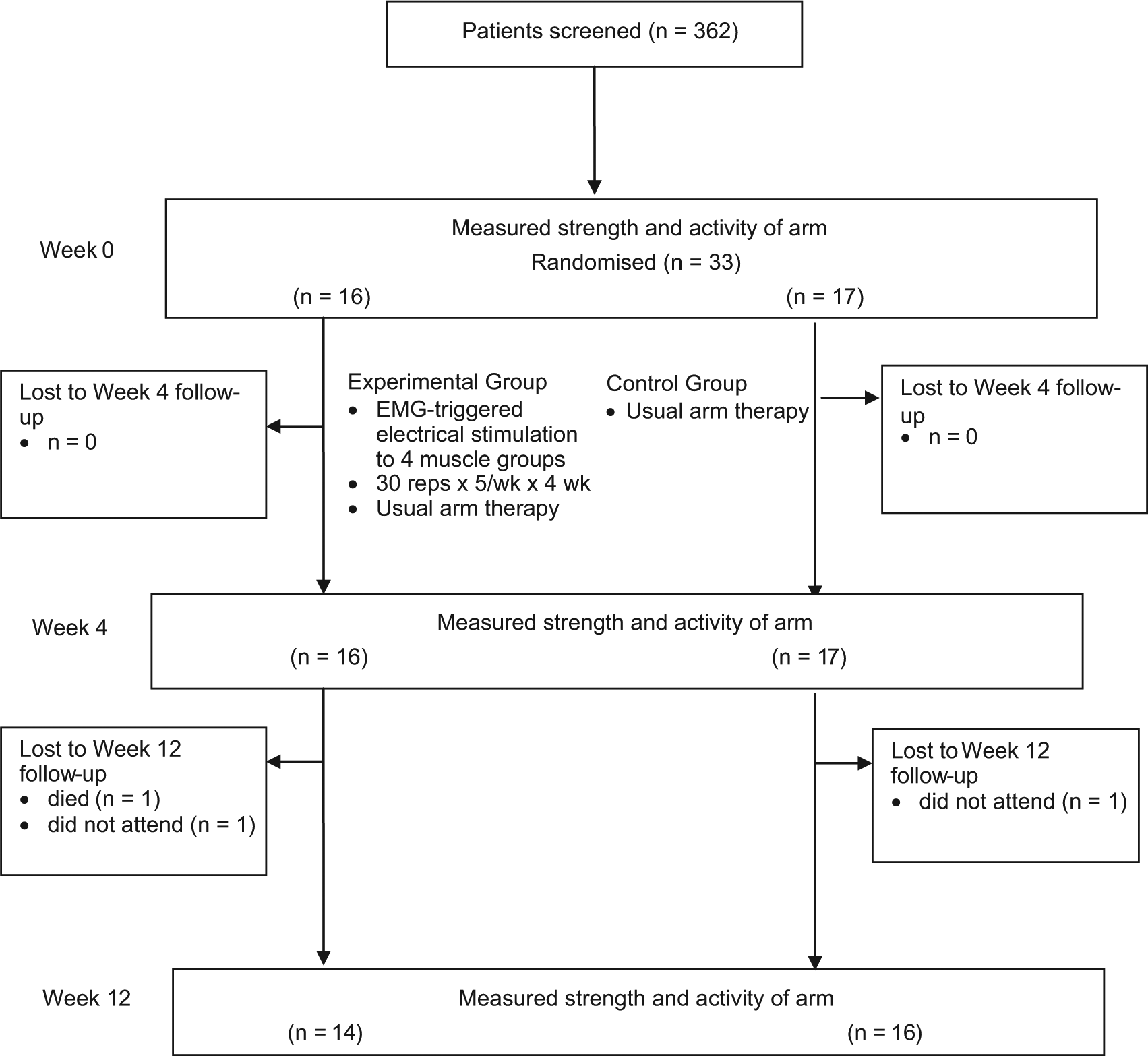
Design and flow of participants through the study.
Patients were eligible for inclusion in the trial if they had a diagnosis of stroke less than four weeks before, were between 50 and 85 years old, had not had a previous stroke that resulted in motor deficits, had been able to reach and manipulate objects independently prior to their stroke and had less than Grade 3 muscle strength on the Oxford grading system in at least three of the following four muscle groups of the affected arm: shoulder flexors, elbow extensors, wrist extensors and thumb abductors. Patients were excluded if they: had a demand-style cardiac pacemaker, had any barriers to taking part in a physical rehabilitation programme or were lacking sufficient cognition and communication to understand the purpose of the study and give informed consent. The presence of spasticity, sensory loss and neglect were recorded in order to describe the sample. Spasticity was measured using the Tardieu Scale, where zero is normal and four is severe spasticity. 15 Tactile sensation and proprioception was measured using the Nottingham Assessment, where zero is normal and two is severe impairment. 16 Neglect was measured using the Line Bisection Test, where zero is normal and two is severe impairment. 17
Therapists providing the intervention were included if they were registered physiotherapists or occupational therapists and prepared to undergo specific training to follow the trial protocol. Students were only involved under the supervision of a trained therapist.
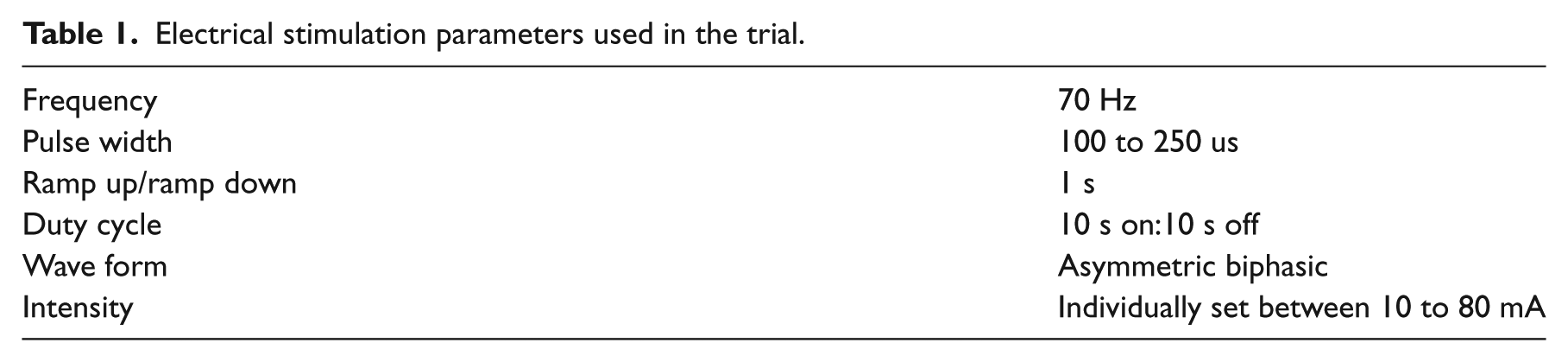
The experimental group received usual therapy plus EMG-triggered electrical stimulation five days a week for four weeks. The EMG-triggered electrical stimulation was applied to the shoulder flexors, elbow extensors, wrist extensors and thumb abductors. The EMG threshold was set at the maximum amount of electrical activity the participant was able to produce in the muscle and the machine was set on automatic mode, which adjusted the threshold up after a successful trial or down after an unsuccessful trial. The electrical stimulation parameters produced near maximum muscle contractions (Table 1). The electrodes used were of various sizes to suit the size of the muscle group being stimulated, one electrode was placed over the motor point of the muscle and one electrode was placed over the muscle belly. The EMG-triggered electrical stimulation was applied to each muscle group for 30 trials per day, this number of trials allowed for all four muscle groups to be targeted within one session and was considered to be a sufficient number of trials to increase strength in the muscle. If a participant was unable to produce five millivolts of EMG activity in a muscle, the machine was set on EMG feedback mode for 15 trials to provide feedback while the participant attempted to produce more EMG activity in the muscle. The machine was then set to cyclical electrical stimulation mode to give the muscle 15 stimulated muscle contractions. Both groups were undergoing inpatient rehabilitation, which continued as usual, including usual arm therapy. Usual arm therapy was delivered as three hours per week of group therapy and one to two hours per week of individual therapy, plus some independent practice. For very weak muscles, i.e. Grade 0, 1 and 2, usual arm therapy involved providing an environment where repetitive active movements could be attempted using gravity-eliminated positions, decreasing friction and shortening the lever arm of the limb. 18 For stronger muscles, i.e. Grade 3 or 4, usual arm therapy included PRE and task-specific training.
Electrical stimulation parameters used in the trial.
The control group received usual arm therapy only.
The feasibility of delivering EMG-triggered electrical stimulation to four muscle groups of the arm was determined by examining compliance with the intervention, retention of participants and monitoring adverse events. Information describing the number of muscles treated each session and any reasons for not delivering the intervention were recorded.
Strength was measured by manual muscle testing using the Oxford grading system, where zero is no strength and five is normal strength. 19 Strength was measured in the four muscles of the arm and the scores were summed to produce a single score for strength (resulting in a score from 0 to 20). If a participant scored Grade 3 or more on a manual muscle test, the strength of that muscle group was also measured with hand-held dynamometry.
Activity was measured using the arm items of the Motor Assessment Scale. The scores for the arm items of the Motor Assessment Scale (items 6, 7 and 8, upper arm function, hand movements and advanced hand activities) were summed as described by Lannin 20 to produce a single score for activity (resulting in a score from 0 to 18). When a participant was able to do so, activity was also measured with the Nine-hole Peg Test.
Intervention recording sheets were used to calculate descriptive statistics on the delivery of the intervention. Repeated measures analyses of variance were used to compare the changes in outcome measures variables between groups at Week 4 and at the follow-up at Week 12. Mean between-group differences (MD) (95% CI) were calculated. Probabilities of less than 0.05 were considered significant. All data were analysed on an intention-to-treat basis. It was planned to recruit at least 30 participants to this trial in order to establish a power analysis for a larger trial, based on a minimum clinically worthwhile difference for strength of four out of 20 for the summed manual muscle tests. This minimum clinically worthwhile difference was chosen as it represents an increase of one grade per muscle on the manual muscle test and any increase of strength of this magnitude represents a functionally significant change. For example, to improve from Grade 0 to Grade 1 means that a muscle that had no activation now has some palpable activation; to improve from Grade 2 to Grade 3 means that a muscle that was unable to move a limb against gravity can now do so.
Results
A total of 362 stroke patients were screened for eligibility for the trial. Thirty-six patients were eligible, but three declined to participate. These participants were randomized to groups, 16 to the experimental group and 17 to the control group. The mean age of the participants was 68 years (SD 12) and the mean time since stroke was 16 days (SD 7). The characteristics of the participants are summarised in Table 2. The groups were well-matched at baseline for age, side of hemiplegia, gender, time since stroke, arm strength, arm activity, spasticity, sensory loss and neglect.
Baseline characteristics of participants.
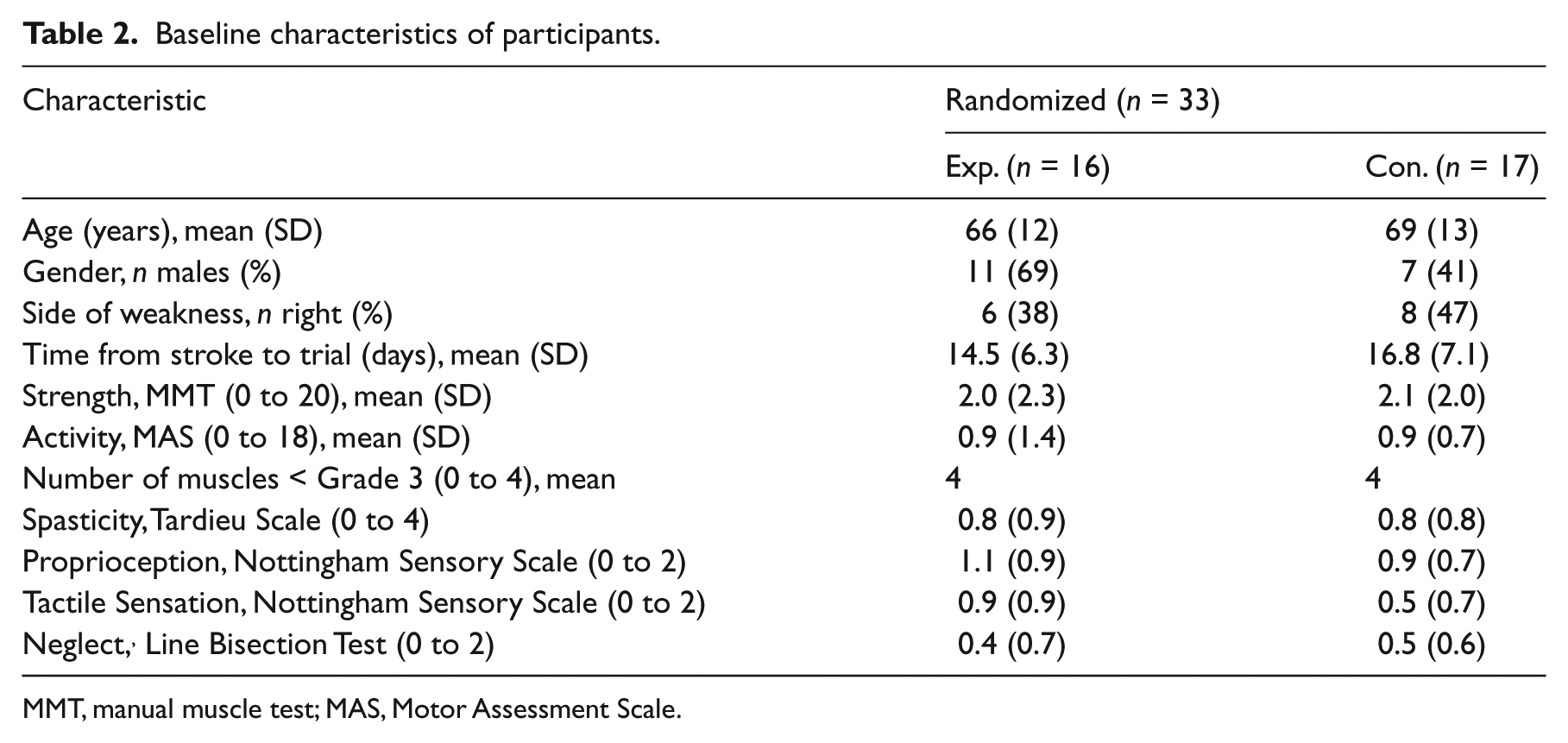
MMT, manual muscle test; MAS, Motor Assessment Scale.
The flow of participants through the trial is shown in Figure 1. All measures were obtained from all participants at Week 0 and Week 4. However, three participants were not able to be measured at Week 12. One experimental group participant died and one experimental group participant and one control group participant did not attend the final measurement session.
EMG-triggered electrical stimulation to four muscle groups took slightly more than an hour to deliver, with each muscle group taking around 15 minutes. Examination of the records of intervention revealed that 1101 out of a potential 1260 (87%) of the prescribed experimental intervention sessions were completed. The main reasons for missed sessions were; patient unavailable (69 sessions, 5%), patient unwell (48 sessions, 4%) and patient refused (18 sessions, 1%). The EMG-triggered electrical stimulation was well tolerated, with no participants withdrawing from the study and no adverse events during the intervention phase.
There was no significant effect of four weeks of EMG-triggered electrical stimulation in addition to usual arm therapy (Table 3). There was no difference in strength measured using manual muscle testing for the experimental compared with the control group at Week 4 (MD 0 out of 20, 95% CI −3 to 3, p = 0.91) or at Week 12 (MD = −1 out of 20, 95% CI −6 to 4, p = 0.92). At baseline, given that one of the inclusion criteria was that the arm muscles were very weak, hand-held dynamometry could not be obtained. By Week 4, 37 of the 132 muscles (28%: experimental group 27% and control group 29%) could be measured with hand-held dynamometry. By Week 12, 50 of the 120 muscles (42%: experimental group 46% and control group 38%) could be measured with hand-held dynamometry.
Mean (SD) outcome for each group, mean (SD) within-group difference and mean (95% CI) between-group difference.
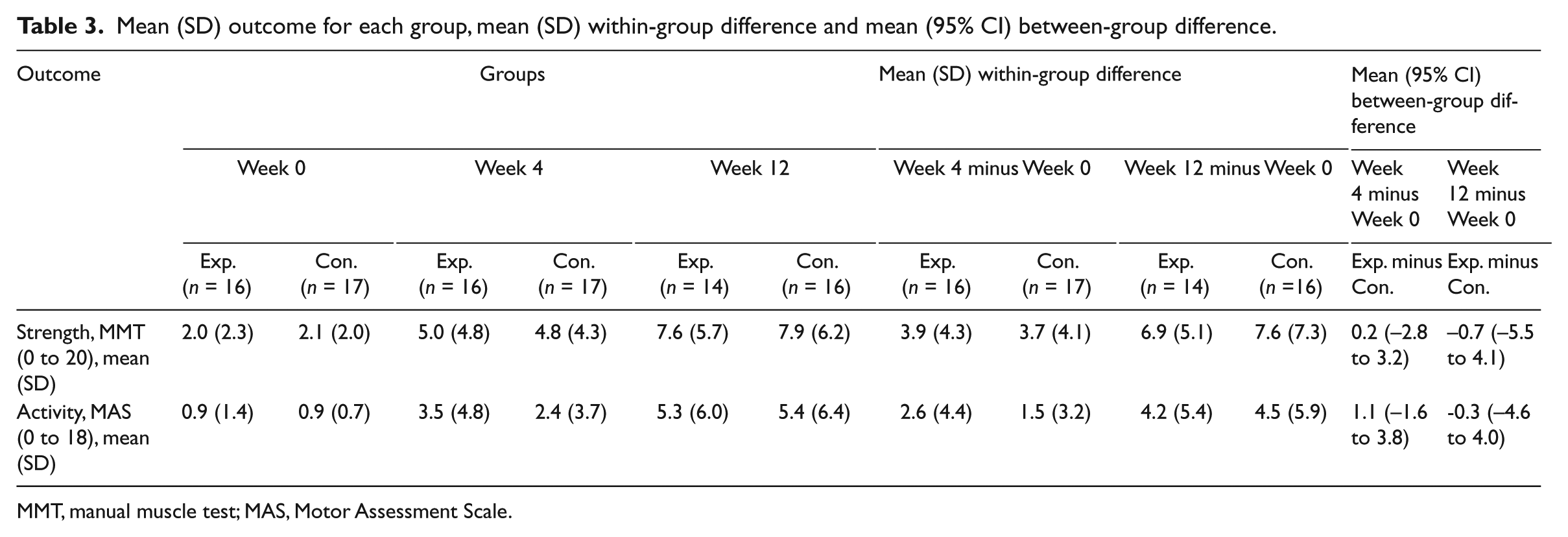
MMT, manual muscle test; MAS, Motor Assessment Scale.
There was no difference in activity measured by the Motor Assessment Scale for the experimental compared with the control group at Week 4 (MD = 1 out of 18, 95% CI −2 to 4, p = 0.44) or at Week 12 (MD = 0 out of 18, 95% CI −5 to 4, p = 0.97). At baseline, no participants could be measured on the Nine-hole Peg Test. By Week 4, two participants (6%) and by Week 12, seven (4%) participants could be measured on the Nine-hole Peg Test.
Discussion
The delivery of four weeks of EMG-triggered electrical stimulation to multiple arm muscles appears to be a feasible intervention in very weak people early after stroke, with a high proportion of sessions being completed. However, this intervention, in addition to usual arm therapy, did not result in greater strength or activity compared with usual arm therapy alone. Since the 95% CIs exclude the a priori between-group difference of 4 out of 20 in terms of strength, it appears that our finding is the result of lack of effect of the EMG-triggered electrical stimulation rather than a Type II error. Hence a larger trial of the same design and intervention is not warranted since it would be expected to decrease variability in the data and therefore the width of the 95% CI, rather than result in a larger between-group difference.
The addition of EMG-triggered electrical stimulation to usual arm therapy was well tolerated in the experimental group. No participants withdrew from the study and there were very few instances of participants refusing the intervention. When participants did refuse the intervention, on the whole, they were refusing therapy owing to fatigue, rather than a problem with the experimental intervention. The dose of intervention, 30 repetitions per muscle five days a week for four weeks, was chosen in order to be able to apply the intervention to four muscle groups within a realistic time frame of one hour while the participants were undergoing inpatient rehabilitation. Choosing a larger dose would probably have affected the feasibility of the intervention and it is unclear whether a larger dose would have had an effect over and above that of usual arm therapy. This highlights the lack of guidelines in choosing an effective dose of strengthening interventions that can be used for very weak muscles, unlike PRE, which has well-established guidelines for what constitutes an effective dose. 21
There are three trials of triggered-electrical stimulation in early very weak stroke patients that are similar in design to our trial, in that both groups received usual arm therapy and the experimental group received triggered electrical stimulation in addition.22 –24 However, in these trials, there were significantly better strength outcomes for the experimental groups than the control groups. There are a number of possible explanations for this discrepancy. First, in these trials, usual arm therapy was based on the Bobath approach. At the time of these studies – from 16 to 34 years ago – this approach discouraged interventions that strengthened muscles, in the belief that this would increase spasticity. 25 Given that only the experimental group was receiving a strengthening intervention, perhaps it is not surprising that they had greater improvements in strength. In contrast, the ‘usual arm therapy’ in our trial included strengthening very weak muscles. What we have shown is that the addition of EMG-triggered electrical stimulation does not result in more strength increases than usual arm therapy when usual arm therapy incorporates strengthening.
Second, in the previous trials,22 –24 although the participants could be described as very weak, they were not as weak as the participants in our trial. In our trial, the average manual muscle test score across all participants was 2 out of 20 for the four muscle groups at baseline and 5 out of 20 after four weeks of intervention. While this represents some improvement, an average score of one for each muscle means that there is still less than anti-gravity strength in most muscles, i.e. less strength than that required to lift the arm or extend the wrist and elbow to perform an arm activity. The amount of improvement in activity mirrored this small improvement in strength. The average Motor Assessment Scale score across all participants was 1 out of 18 at baseline and 3 out of 18 after four weeks of intervention. While this also represents some improvement, it does not represent a score that equates to being able to use the arm to reach and manipulate objects. At four weeks, only two participants were able to do the Nine-hole Peg Test and at 12 weeks, only seven participants could do it. Even with comprehensive and intensive rehabilitation, these very weak arm muscles did not recover strength, and therefore the ability to carry out activities. This raises the question of whether intensive therapy over longer periods of time would make a difference in these people who are very weak following stroke.
The strengths of the current study are, first, that it examines the feasibility of adding additional therapy to usual arm therapy, providing us with information about whether at a pragmatic level this could be achieved in a rehabilitation environment. Second, it examines the effect of EMG-triggered electrical stimulation when it is given in addition to usual arm therapy that focuses on strengthening very weak muscles, hence informing us about whether this intervention provides additional benefit if strengthening is already a focus of usual arm therapy. A limitation is that this does not inform us about the effectiveness of EMG-triggered electrical stimulation compared with usual strengthening exercises. A trial that matched the dosages of EMG-triggered electrical stimulation and other strengthening exercises would provide this information.
It is possible that the inability to blind the participants and therapists in a trial of complex interventions, such as this one, can affect the results. However, given that there were no between-group differences in this trial, this does not appear to be the case. Finally, the only measure of strength that could be used for between-group analysis was manual muscle testing, which is the only recognised way to measure strength in very weak muscles. Manual muscle testing has been shown to have very good inter-rater and intra-rater reliability in testing with stroke patients. 26 Furthermore, using manual muscle testing to measure very weak muscles is considered more objective than measuring stronger muscles, since the examiner is assessing how well the muscle can move the limb in relation to gravity, a standardised force, rather than assessing movements against examiner-applied force, which is not standardised. 27
Clinical messages
It is feasible to apply EMG-triggered electrical stimulation to multiple muscles of the affected arm in acute, very weak stroke patients.
EMG-triggered electrical stimulation in addition to usual arm therapy, where usual arm therapy contains strengthening exercises, does not appear to offer additional benefit.
Footnotes
Conflict of interest
The author declares that there is no conflict of interest.
Funding
This research received funding from the NSW Physiotherapists Registration Board and the Physiotherapy Research Foundation (Australia).