
Abstract
Objective:
To determine the probability of spontaneous disc regression among each type of lumbar herniated disc, using a systematic review.
Data sources:
Medline, Cochrane Library, CINAHL, and Web of Science were searched using key words for relevant original articles published before March 2014. Articles were limited to those published in English and human studies.
Review methods:
Articles had to: (1) include patients with lumbar disc herniation treated conservatively; (2) have at least two imaging evaluations of the lumbar spine; and (3) exclude patients with prior lumbar surgery, spinal infections, tumors, spondylolisthesis, or spinal stenosis. Two reviewers independently extracted study details and findings. Thirty-one studies met the inclusion criteria. Furthermore, if the classification of herniation matched the recommended classification of the combined Task Forces, the data were used for combined analysis of the probability of disc regression of each type. Nine studies were applicable for probability calculation.
Results:
The rate of spontaneous regression was found to be 96% for disc sequestration, 70% for disc extrusion, 41% for disc protrusion, and 13% for disc bulging. The rate of complete resolution of disc herniation was 43% for sequestrated discs and 15% for extruded discs.
Conclusions:
Spontaneous regression of herniated disc tissue can occur, and can completely resolve after conservative treatment. Patients with disc extrusion and sequestration had a significantly higher possibility of having spontaneous regression than did those with bulging or protruding discs. Disc sequestration had a significantly higher rate of complete regression than did disc extrusion.
Introduction
Low back pain and radicular leg pain are common problems in physical medicine and rehabilitation. Lumbar intervertebral disc herniation is one of the most frequent causes of such pain. Around 60% to 90% of lumbar disc herniations can be successfully treated with a conservative approach alone.1,2 Active conservative treatment produces a satisfactory outcome, even for patients with obviously extruded discs or marked neurological deficits.3,4 Many studies have evaluated the natural history of lumbar disc lesions, and have documented the fact that disc lesions can become smaller and can even completely resolve, as shown on computed tomographic (CT) and magnetic resonance imaging (MRI) scans.3–5
In 1984, Guinto et al. first reported a case of lumbar disc regression after conservative treatment. 6 In the next year, Teplick and Haskin reported 11 cases of spontaneous disc regression. 7 Thereafter, many other researchers reported similar findings but described varying rates of spontaneous disc regression. This can be explained by the different methods used in individual studies, such as: dissimilar imaging modalities, inclusion criteria, follow-up periods, classification of disc herniation, and regression criteria.
Results of previous studies have revealed that disc herniations are reduced in 35% to 100% of patients over a period of from 3 to 40 months.3,4,8–16 The reported rates vary because different classifications of disc herniation were used by different researchers. Thus, the aim of this study was to investigate the probabilities of disc regression and complete resolution among different types of lumbar intervertebral herniation, by using a systematic review and combined analysis.
Methods
We performed electronic searches, without restriction of publication date, of the following databases: Medline, Cochrane library, CINAHL and Web of Science. The date that the search was undertaken on March 3rd, 2014.The exact search syntaxes used are listed in Appendix 1 (supplementary material). We included only articles published in English and that included human subjects, and excluded review articles and case reports. The references of all relevant studies were cross-checked to augment the electronic search. The titles and abstracts of retrieved articles were then independently reviewed by two authors (Chun-Chieh Chiu and Wen-Yen Hsu), to identify the studies of interest.
Selection criteria
The studies selected investigated reported cases of regression of lumbar herniated discs not treated with surgical intervention. Our basic selection criteria required that the individual study include at least two images, taken at baseline and follow-up, as their method of investigating disc regression. This criterion applied whether the images were made with myelography, CTs, or MRIs. We accepted all different follow-up protocols, herniation disc classifications, and regression grading. Patient treatments could include bed rest, analgesics, nonsteroidal anti-inflammatory drugs, exercise, physical therapy, or epidural steroid injection. However, uncontrolled studies of patients who received chymopapain injections were excluded due to possible enzymatic nucleolysis. Subjects with spinal infections, tumors, spondylolisthesis, spinal stenosis or previous lumbar surgery were also excluded because of different pathophysiology.
Data extraction for probability calculation of disc regression
To calculate the probability of disc herniation, we adopted the classification system of disc herniation provided by the combined task forces of the North American Spine Society, the American Society of Spine Radiology, and the American Society of Neuroradiology. 17 This classification system (known as the combined Task Forces) composed of “bulge, focal protrusion, broad-based protrusion, extrusion, and sequestration.”
We reviewed all the selected studies and selected data when it clearly matched the herniation type definition of disc classification proposed by the combined Task Forces. 17 The data extraction and categorization had to be approved by two authors, Chun-Chieh Chiu and Wen-Yen Hsu. If disagreements exist after discussion, a third author (Kwang-Hwa Chang) will make the final decision. We grouped all the data for each type of disc herniation, and then calculated the probability of disc regression among all the different disc morphology classifications. We also calculated the probability of complete resolution and the odds ratio. For the probability calculation, we needed at least two effective studies. If the effective data could only be obtained from one study, we excluded that data in the probability calculation and analysis.
Methodological quality assessment
The issues involved in investigating disc regression were more likely centered on the nature of the history of the herniated disc, rather than details about the intervention. There was no consensus on which criteria list should be used for assessing the methodological quality of natural history studies, thus we developed six criteria. These criteria were: prospective study design, eligibility, blind assessment of image outcome, clear disc regression criteria, an acceptable drop-out rate, and a clearly defined image follow-up protocol. Studies were determined to be eligible when there was an adequate description of patients’ clinical signs and symptoms, and inclusion and exclusion criteria. Disc regression criteria had to be quantitative, or described in detail. An acceptable drop-rate was defined as having at least 85% of subjects in the study receive a second imaging evaluation. Image follow-up protocol was considered clear when follow-up images were taken at fixed intervals in all patients or when they conformed to specific criteria when taken. Each study’s quality assessment was scored using a 6-point scale. Based on the scoring, each study was defined as low quality (score 0-2), moderate quality (score 3-4), or high quality (score 5-6), respectively.
Statistics
Pearson’s chi-square test was used to analyze differences between groups. P-values below 0.05 were considered significant. Odds ratio and 95% confidence interval were also used to judge the influence of different disc morphology.
Results
We identified 31 articles that conformed to the selection criteria, and these were included in the systematic review. (Figure 1) Among the 31 studies, we found that various methods were used in the morphologic classification of disc herniations, regression grading of herniations, and different imaging modalities and imaging interval protocols. Some articles3,4,20,21 investigated different issues but used the same subjects. In such cases, when we calculated the disc regression probability, we omitted those subjects’ data from either study, to avoid duplicate calculation. After sorting out the subject who clearly fit the herniation type definition of disc classification system proposed by combined Task Forces, 17 we obtained and extracted data from nine articles, which we then analyzed for the probability of disc regression (Table 1).
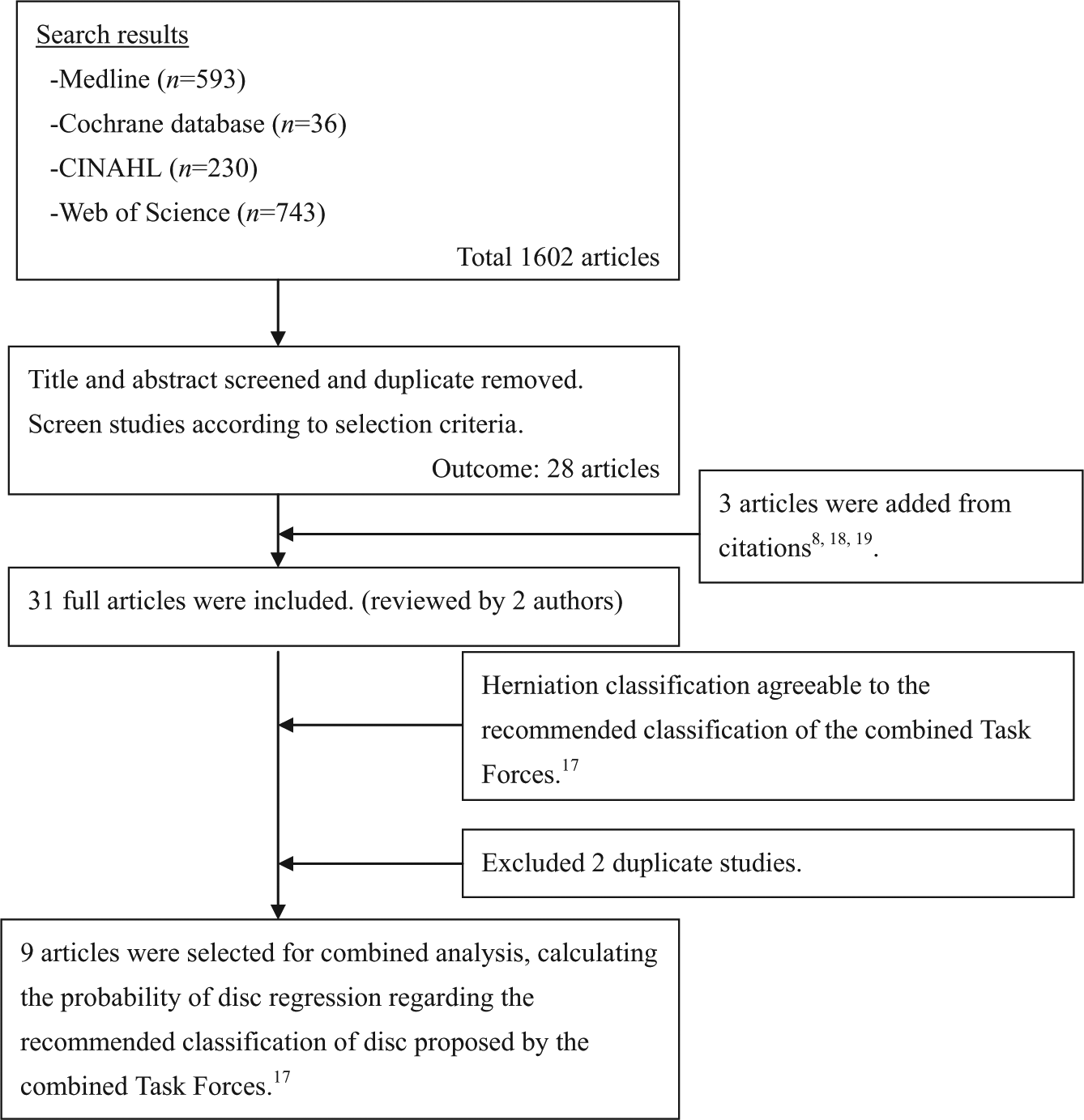
Flowchart of literature selection.
Characteristics of the nine studies included for combined analysis.
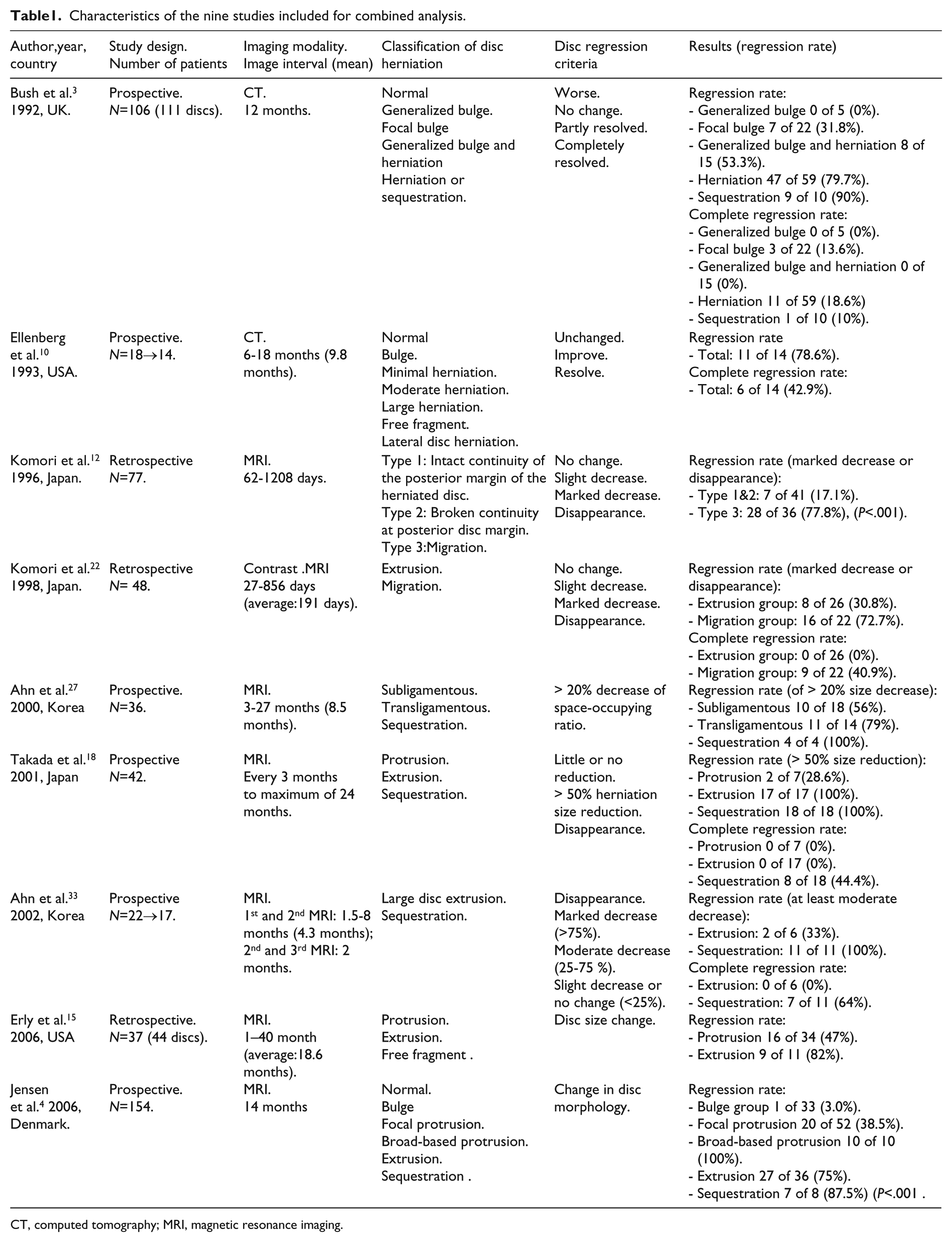
CT, computed tomography; MRI, magnetic resonance imaging.
The methodological quality assessment of these nine studies is shown in Supplementary Table 1. Six studies had a prospective design. Among the nine studies, five were considered to be of high quality, three were of moderate quality, and one was of low quality.
We sorted out the data that best matched the classification proposed by the combined Task Force. 17 Using the case number of disc regression research, the data were collected to calculate the probability of disc regression by each classification. The data from the retrieved articles are listed in the reference columns of Tables 2–4.We identified 361 cases of lumbar herniated discs, which were retrieved for further analysis of regression probability. The cases included 60 bulging discs, 93 protruded discs, 154 extruded discs and 54 sequestrated discs. The results revealed that the rate of a herniated disc becoming smaller over time was 96% (52/54) for sequestrated discs, 70% (108/154) for extruded discs, 41% (38/93) for protruded discs, and 13% (8/60) for bulging discs (P<0.001). This suggested there is strong evidence of a significant correlation between herniation morphology classification and rate of regression (Table 2).
Percentage of disc regression of lumbar disc herniation.
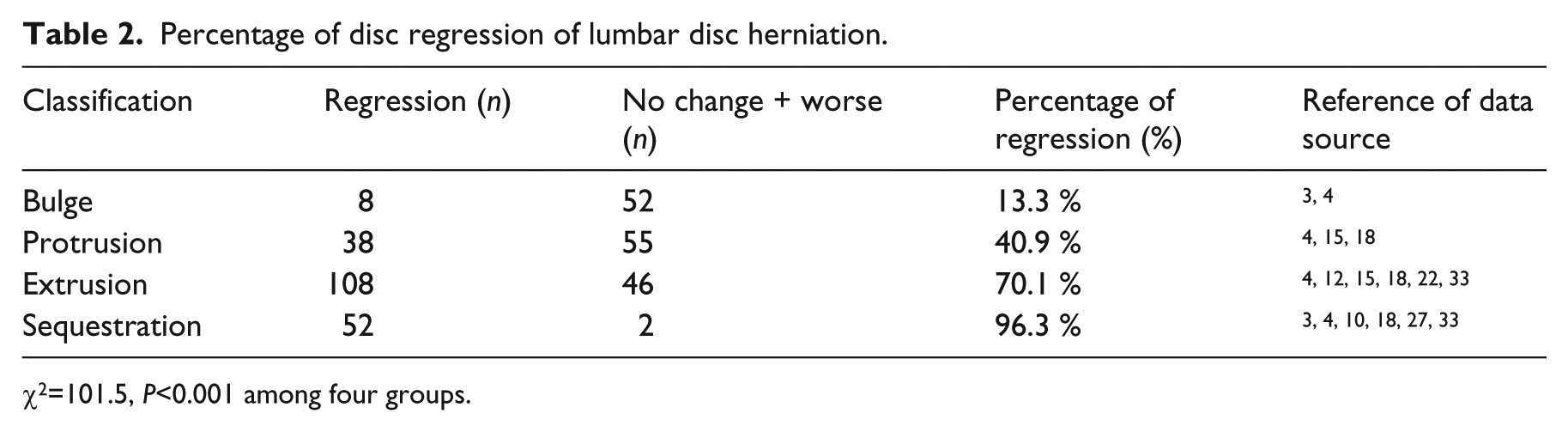
χ2=101.5, P<0.001 among four groups.
Percentage of disc regression between ‘bulging and protruded disc’ and ‘extruded and sequestrated disc’.
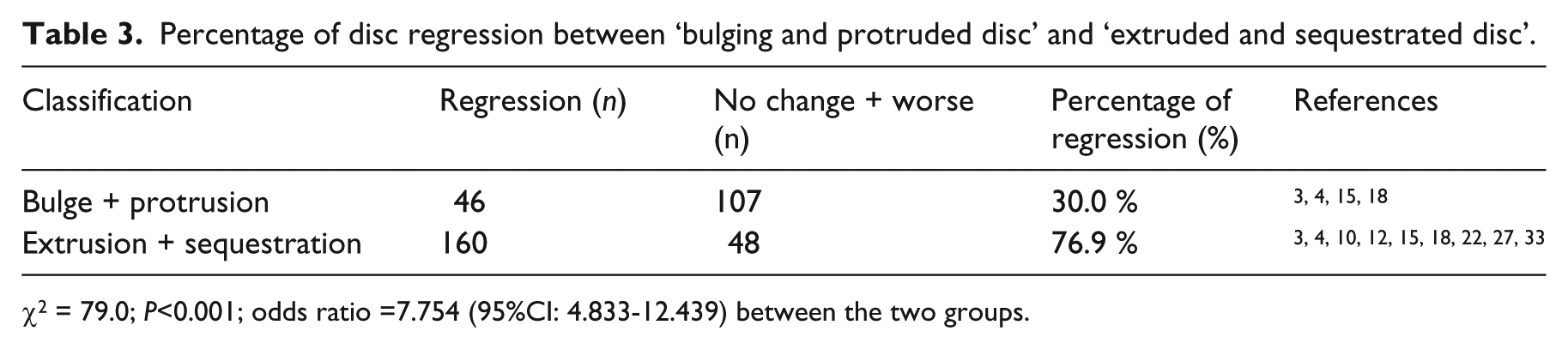
χ2 = 79.0; P<0.001; odds ratio =7.754 (95%CI: 4.833-12.439) between the two groups.
Percentage of complete resolution of lumbar disc herniation.
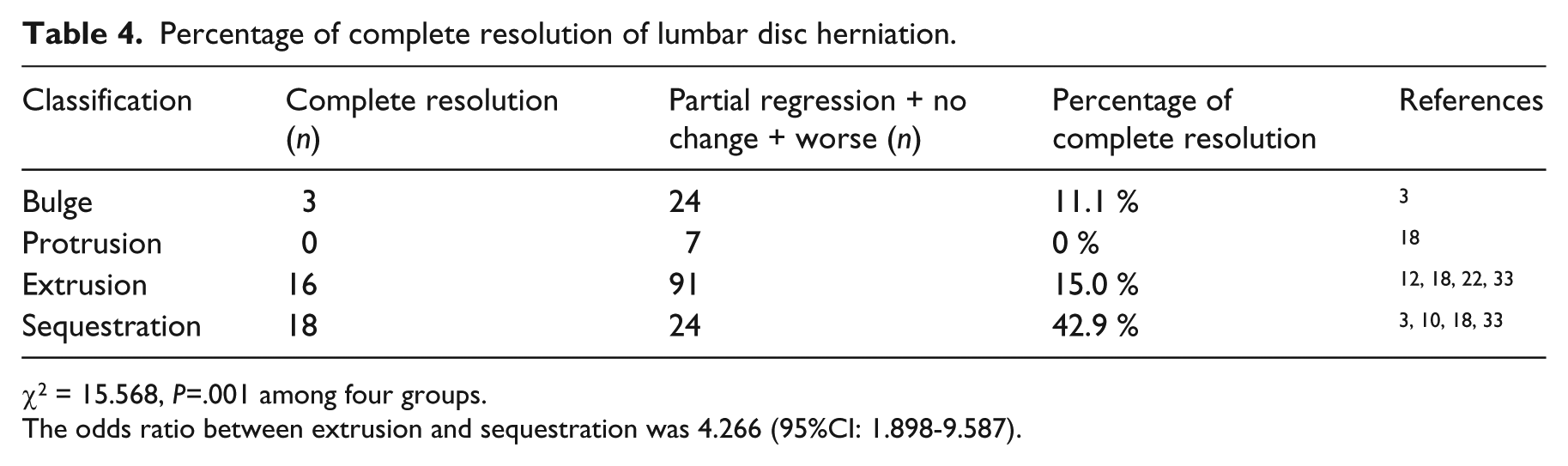
χ2 = 15.568, P=.001 among four groups.
The odds ratio between extrusion and sequestration was 4.266 (95%CI: 1.898-9.587).
We further analyzed which groups of disc herniation were: (A) disc extrusion and sequestration, and (B) disc bulge and protrusion. The former group had a 77% (160/208) regression rate, significantly higher than the 30% (46/153) regression rate in the latter group. (P<0.001, Table 3) The odds of regression to extrusion and sequestrated discs were 7.8 times higher than of regression to bulging or protruded discs.
Table 4 lists the rate of “complete disc resolution” among the different types of herniated discs. The probability was that about 43% (18/42) of sequestrated discs would completely resolve at follow-up over time, compared to only 15% (16/107) of extruded discs (0% of protruded discs and 11% of bulging discs were found). There was a significantly higher chance that sequestrated discs would completely resolve; in fact, the odds were 4.3 times greater that sequestrated discs would resolve than extruded discs would resolve (P<0.001).
We listed the conclusions and important information of the other twenty-two studies those were not included into probability calculation in Supplementary Table 2. Many studies have investigated the relationship between disc herniation regression and other factors, such as migration of herniated discs, subligamentous or transligamentous herniation (broken posterior longitudinal ligament, PLL), with or without contrast enhancement, and high or low MRI T2 signal intensity of the herniated disc, size of the herniated disc, age, duration of symptoms and so on. Among our 31 retrieved studies, three investigated the correlation between herniated disc migration and disc regression,12,16,22 and all supported the fact that disc migration leads to a higher regression rate than does disc extrusion without migration. We identified five studies that investigated whether disc herniation with positive contrast enhancement is related to disc regression. All five affirmed that disc herniation with positive enhancement contributes to regression of disc herniation.13,16,19,22,23 Two studies11,16 investigated if subligamentous or transligamentous herniation related to disc regression, both studies favored transligamentous herniation had a positive predictive effect on disc regression compared to herniations with intact PLL. There were four studies14,15,23,24 supporting that higher MRI T2 signal intensity of disc herniation can be predictive of a higher rate of disc regression or higher reduction of disc size. Ten studies investigated the relationship between the size of herniated disc and disc regression, however the results were not conclusive. Seven studies8,9,11,15,24–26 supported larger disc herniation tended to have higher possibility of disc regression but three studies did not supported this.10,27,28
Among the 31 retrieved studies, we identified 14 studies that had investigated if the disc regression correlated to the clinical outcome. Eight9, 12,13,16,18,25,27,29 of the fifteen studies supported cases where disc regression correlated with better clinical outcome, however, the other six3,11,21,30–32 studies revealed non-correlation. Some studies found complete resolution or significant disc size regression favored better clinical outcomes9,18 and also fast disc regression group had better symptoms and disabilities improvement than slow regression group. 16
Discussion
We performed a systematic review of natural history of lumbar disc herniation. To our knowledge, this is the first systematic review about this topic. Thirty-one studies were identified and nine studies were extracted for calculation of spontaneous regression probability of disc herniation based on the classification system provided by the combined Task Forces. 17 The probability of spontaneous regression was 96% for disc sequestrations, 70% for extrusions, 41% for focal protrusions, and 13% for disc bulges. (P <0.001, Table 2) The results gave the fact that the higher grade of disc herniation type, the higher rate of spontaneous regression. The probability was that about 43% of sequestrated discs would completely resolve at follow-up over time, compared to only 15% of extruded discs (Table 4). After combined analysis, the probability of herniation regression did not differ from previous studies. In Jensen et al.’s study, only 3 % of bulges and 38% of focal protrusions regressed, whereas 75% to 100% of the other more substantial herniations (broad-based protrusion, extrusions, and sequestrations) showed disc regression (P <0.0001). 4 Erly et al. observed that 82% (9/11) disc extrusions regressed, while 47% (16/34) disc protrusions regressed during an average follow-up of 18.6 months (1 to 40 months). 15
It is also well to mention that we could not determine the size of regression due to differing definitions of “regression” used among the retrieved studies. For example, some studies measured percentage of change of the antero-posterior diameter8,11,18,25,31 or area of herniation.13,14,27,28,33 Some studies used qualitative grading, such as disappearance, marked decrease, slight decrease, and no change.3,9,10,12,20,22–24 In addition, the intervals for imaging follow-up often varied. Therefore, we could show the probabilities of disc regression, meaning the disc did become smaller, but it was not easy to predict disc size change in our study.
We conclude that predictive factors for spontaneous regression of lumbar herniated disc were extruded and sequestrated type herniation, migrated disc, transligamentous herniation, herniation with contrast enhancement, and high MRI T2 signal intensity of the herniated disc. Disc migration is a subtype of disc extrusion and the herniation is exposed into epidural space as well as transligamentous herniation. In 1996, Komori et al. reported that 78% (28/36) migrated discs regressed, whereas only 17% (7/41) non-migrating discs regressed (P <0.001). 12 Complete resolution rate was also higher in the migration group than in the non-migration group in Komori’s study (41% versus 0%). 22 Matsubara et al. reported that herniations with broken PLL showed a greater degree of reduction than did herniations with intact PLL (26% versus 9%; P <0.02). 11
Contrast enhancement of herniated disc imply that the periphery of herniated tissues is vascularized and an inflammatory stage signaling for macrophage phagocytosis. Splendiani et al. reported that 83% (25/30) of cases with contrast enhancement showed disc resolution, which was significantly different from cases without contrast enhancement (P < 0.05). 23 Autio et al. further pointed that higher thickness of enhancement rim was also a significant determinant of disc regression. 16 High T2 signal intensity implies that herniated tissue may shrink because of dehydration. Henmi et al. found that the T2 signal intensity is higher in a herniated disc than the original disc in patients with shorter duration of illness, and the T2 signal decreased over time. 14 Besides, those herniated discs with high T2 signal intensity showed higher reduction ratio than those with low T2 signal intensity. These predictive factors lead the focus to the mechanism of how herniated disc regressed and even completely disappeared.
The correlation between disc regression and improvement of clinical outcome is controversial. Several reasons may relate to the discrepancy. There are many factors that can influence clinical outcomes besides the size of disc herniation, such as poor lumbosacral stability causing mechanical low back pain, chemical radiculitis, 34 nerve root adhesion, and psychological factors as examples. Therefore the sole factor of “disc regression” cannot predict or be well correlated to better clinical outcome. Conversely it was observed that the clinical outcome can improve even without disc size regression. 3 A second observation is that the definition of disc regression varied among these retrieved studies, which also influenced the study conclusions. Some studies defined regression as disc size reducing more than 70%, 9 whereas some studies used 50% 18 or 20%; 27 disc regression measurement also varied among the studies: volume change, cross section area change, or diameter change, are all found among different studies.
Although disc regression is not well correlated to clinical outcome, some studies did find complete resolution or significant high regression rate, for example a disc size reducing more than 70% had better correlation between disc regression and clinical outcome. There were eight cases of complete disc resolution in Takada et al.’s study, 18 all of the eight cases had excellent or good clinical outcome; while only 20% patients with herniation reduction less than 50% had good clinical outcome. Bozzao et al. 9 followed up 46 patients and observed 61% (19/31) patients whose disc size reduction more than 70% had complete resolution of clinical outcome, while none of the other patients whose disc size reduction less than 70% had.
Most spontaneous disc regression happened within the first year,16,18 however disc regression could be observed within first two 16 or three 18 months. In Takada et al.’s study, 18 there were 27% (10/37) spontaneous disc regression found at three months from the onset and disc sequestrations were more prone to regress earlier than disc extrusions or protrusions. The other interesting observation is the fast disc regression group had better clinical improvement than slow regression group. 16 Autio et al. 16 did follow-up MRI scans at 2 months and 12 months after baseline scan. This study found leg pain intensity and Oswestry disability decreased significantly more in the fast resorption group (more than 40% decrease in herniation volume at 2 months) compared to the slow resorption group. This study also found that herniations with higher rim enhancement thickness or with higher Komori classification 12 had a more rapid resorption rate. Although the correlation between disc regression and improvement of clinical outcome is still not conclusive, complete resolution or significant disc size regression and fast disc regression groups tend to favor better symptoms and disabilities improvement. The current authors suggest the need for more researches to investigate the relationship between disc regression and clinical outcomes with standardized study design, also investigating if different timing of disc resolution would influence the symptoms and disability improvement and what factors could be used early to determine patients will have good clinical improvements and good possibility of significant disc regression.
Three hypotheses have been proposed to explain how a herniated disc becomes smaller or disappears. Various types of herniation and bulges seem to have different pathways to regression: (1) the herniation could retract back into its parent disc,7,35,36 which possibly happens with disc bulges and disc protrusions. This hypothesis was supported by an in vitro study by Scannell and McGill 37 and was consistent with McKenzie’s theory. 38 (2) Disc regression is related to the dehydration process, which correlates to the reports of higher MRI T2 signal intensity with higher regression rates.14,15,23,24 (3) Disc herniation into the epidural space causes an inflammatory reaction and neovascularization, resulting in absorption of herniated disc by phagocytosis and enzymatic degradation.
This third mechanism has been supported by many in vitro and in vivo animal studies.39–45 In the case of spontaneous regression of herniated discs, the hypothesis of disc absorption by macrophage phagocytosis and MMP enzymatic degradation is more convincing than the other two hypotheses. The absorption process can reasonably explain the complete disappearance of herniated disc while the dehydration hypothesis cannot. It is also reasonable to explain those MRI studies regarding disc regression. For example, transligamentous herniation, or penetration of a herniated disc through PLL, as shown on MRIs, leads to contact of the disc tissue with the epidural space. This will cause further inflammation, a neovascularization reaction, subsequent macrophage phagocytosis, and enzymatic degradation. Disc herniation with positive contrast enhancement indicated the existence of neovascularization and an inflammatory reaction. Extrusion, sequestration type of herniation, or herniation with migration has greater exposure into the epidural space than does protrusion, bulge-type herniation, or herniation without migration. As sequestrated herniation is totally isolated into the epidural space, inducing surrounding inflammation, it is not surprising that it has the highest rate of complete resolution. Readers may refer to a review article by Benoist, who reviewed the mechanism in the pathomorphological change of disc herniation. 46
Limiting studies to those published in English is a selection bias in our study. Only a few studies could be included in the combined analysis, in which data need to match the definitions of the combined Task Forces classification. Therefore the number of studies included was relatively small. Furthermore, there were differences among studies in research methods and imaging follow-up time points. There also was heterogeneity among studies regarding the definition of disc regression, different studies has different size definition as “disc regression”. Different types of image modalities and different types of MR scanners which had different field strengths and protocols among studies would affect the interpretation of the scan. These differences would cause heterogeneity of the data and also made them difficult to give some further conclusive clinical information. The current authors suggest the need for further studies to investigate this issue especially focusing on the relationship between disk pathology, symptoms, and disability; with study design base on combined Task Forces classification, standardized MRI scanner and scan protocol, standardized herniated disc measurement, standardized disc regression definition, standardized MRI scan follow-up protocol, and standardized clinical outcome measurements.
Clinical messages
Lumbar disc herniation can regress or disappear spontaneously without surgical intervention.
Disc extrusion and sequestration are more prone to regress than disc bulge and protrusion. (77% versus 30%).
Disc sequestration had a significantly higher rate of complete regression than did disc extrusion. (43% versus 15.0%).
Footnotes
Acknowledgements
We wish to thank the Center of Excellence for Clinical Trial and Research in Neuroscience for assistance with statistical analyses in this study. (DOH100-TD-B-111-003) Professor Winston W. Shen provided editorial comments on a previous version of this manuscript.
Presented at the Annual Conference of Taiwan Academy of Physical Medicine and Rehabilitation, April 9, 2011, Taipei, Taiwan
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.