
Abstract
Objective:
To determine whether symptoms of urinary incontinence is reduced by pelvic floor muscle training, to determine whether urinary incontinence can be totally eliminated by strengthening the pelvic floor muscle to grade 5 on the Oxford scale.
Design:
Prospective randomized controlled clinical trial.
Setting:
Outpatient urogynecology department.
Subjects:
One hundred thirty cases with stress and mixed urinary incontinence.
Intervention:
All participants were randomly allocated to the pelvic floor muscle training group or control group. A 12-week home based exercise program, prescribed individually, was performed by the pelvic floor muscle training group.
Main measures:
Urinary incontinence symptoms (Incontinence Impact Questionnaire-7, Urogenital Distress Inventory-6, bladder diary, stop test and pad test) were assessed, and the pelvic floor muscle strength was measured for (PERFECT testing, perineometric and ultrasound) all participants before and after 12 weeks of treatment.
Results:
The pelvic floor muscle training group had significant improvement in their symptoms of urinary incontinence (P=0.001) and an increase in pelvic floor muscle strength (P=0.001, by the dependent t test) compared with the control group. All the symptoms of urinary incontinence were significantly decreased in the patients that had reached pelvic floor muscle strength of grade 5 and continued the pelvic floor muscle training (P<0.05).
Conclusion:
The study demonstrated that pelvic floor muscle training is effective in reducing the symptoms of stress and mixed urinary incontinence and in increasing pelvic floor muscle strength.
Introduction
The pelvic floor muscles play an important role in the maintenance of continence. International Continence Society recommends pelvic floor muscle training to be the first choice of treatment for stress and mixed urinary incontinence in women. 1 There is Level A evidence that pelvic floor muscle training programs effectively treat stress and mixed urinary incontinence. 2 Success rates of 56-75% have been reported. 3
Pelvic floor muscle training involves repetitive contraction of the pelvic floor muscle, which builds strength and improves the muscle tone of the pelvic floor muscle and increases perineal support. 4 Pelvic floor muscle training leads to hypertrophy of the local skeletal muscle, enhances the cortical awareness of muscle groups, strengthens the connective tissue in the muscles, and leads to more effective recruitment of active motor neurons. 5 It has been suggested that increasing the power and tone of the pelvic floor muscle leads to a permanent elevation of the levator plate to a higher resting position inside the pelvis, thereby ‘lifting’ the pelvic viscera and restoring normal reflex activity and other protective continence mechanisms. 4 Madill et al. 6 reported that improvements in urine leakage were associated with improvements in pelvic floor muscle co-ordination, motor-control and pelvic organ support.
A previous study revealed that “the more improvement of pelvic floor muscle strength, the more decrease of urinary incontinence symptoms”. 7 Literature has been published describing investigations conducted to determine the impact of pelvic floor muscle training on pelvic floor muscle strength and the amount of urine loss. 5 Other publications dealt with differences in pelvic floor muscle strength and the effectiveness of treatment in different groups.4,8–11 Therefore, using different groups, we designed this study to show the effect of pelvic floor muscles being strengthened to grade 5 on clinical symptoms, according to the Oxford scale. Thus, examining the effect of pelvic floor muscle rehabilitation is important to better understand the role of the pelvic floor muscle in symptoms of urinary continence.
In the literature, we did not come across any training programs that were continued until a pelvic floor muscle strength of grade 5 was obtained. Therefore, we think that our study will lead to new studies by contributing to the literature. In addition, this study was undertaken to investigate its effects on all three aspects of pelvic floor muscle function in urinary incontinence, force/activation and coordination were measured with periometer, PERFECT and palpation, and pelvic floor muscle contraction were measured with ultrasonography.
Our primary purpose of this study was to determine whether symptoms of urinary incontinence is reduced by pelvic floor muscle training. Our secondary purpose was to determine whether urinary incontinence can be totally eliminated by strengthening the pelvic floor muscle to grade 5 on the Oxford scale and to determine whether symptoms of urinary incontinence are abolished by pelvic floor muscle training.
Methods
This is a prospective, randomized, single-blinded, and controlled clinical trial of the before-and-after exercises training. The study was jointly conducted by the Ege University Faculty of Medicine, Department of Obstetrics and Gynecology and the Dokuz Eylul University, School of Physical Therapy and Rehabilitation.
Ethical approval for this study was obtained from the Human Research Ethnics Committee of Ege University (Number:B.30.2.EGE.0.20.05.00-12-11.1/1). All the patients gave a written informed consent form.
Participants
The patients of this study included 176 incontinent women selected from the individuals observed at the urogynecology unit. Forty-six patients were excluded from the study because of they met one or more of the exclusion criteria. All of the patients were randomization to the pelvic floor muscle training group (n=65) or the control group (n=65) and were evaluated before and after the intervention. Randomization was carried out using a computer-generated random number table by the pre labeled sealed envelope method by the study coordinator (in which the person collecting the data knew whether the patients were in the control or experimental groups but the patients did not). Based on random number table, participants were assigned to two interventions. A total of 121 patients with stress urinary incontinence (n=56) and mixed urinary incontinence (n=65) were included in this study. The pelvic floor muscle training group had 26 (44.8 %) stress urinary incontinence and 32 (55.2 %) mixed urinary incontinence. The control group had 30 (47.6 %) stress urinary incontinence and 33 (52.4 %) mixed urinary incontinence.
The inclusion criterion was urinary incontinence diagnosed by a urogynecologist using analysis of urodynamics. The exclusion criteria included pregnancy, a history of spinal surgery, spinal or pelvic fracture, urinary tract infection, vaginal infection, known neurologic disorders, respiratory disease and menstruation at the time of assessment. To avoid any confounding effects, the patients were excluded if they had undergone pelvic floor muscle training at physiotherapy within the last two years. The patients who, upon digital palpation, had ‘zero-one’ pelvic floor muscle strength were excluded.
Procedures
Data with regards to age, body mass index, waist/hip ratio, duration of urinary incontinence, number of pregnancies, heaviest new born weight at delivery, and type of delivery were collected during the anamnesis at the initial approach. Urinary incontinence symptoms (Incontinence Impact Questionnaire-7, Urogenital Distress Inventory-6, bladder diary, pad test, stop test) and pelvic floor muscle strength measurements (PERFECT testing; perineometric measurement and transabdominal ultrasonography) were performed by a physiotherapist and gynecologist. A preliminary assessment of pelvic floor muscle function was performed by an experienced pelvic floor physiotherapist using palpation. 12 One physiotherapist performed measurements and the other performed pelvic floor muscle training. The investigators were not aware of the results of the other assessments.
Symptoms evaluation
The Incontinence Impact Questionnaire and Urogenital Distress Inventory assessed the presence of various urogenital symptoms and their effect on the patients’ quality of life. All of the patients were asked to complete the Incontinence Impact Questionnaire-7 (a 7-item measure of urogenital distress) and Urogenital Distress Inventory-6 (a 6 item measure of incontinence effect) questionnaire. 13 The Turkish translated versions of the Incontinence Impact Questionnaire-7 and Urogenital Distress Inventory-6 are reliable, consistent and valid instruments. 14
The urinary loss was measured by the simplified bladder diary, which was written down by the patient. A three-day bladder diary was allowed for pad usage. From the bladder diaries, we extracted the following information: urgent urinary voiding, day time urinary frequency, night time urinary frequency and urinary incontinence frequency.
For the stop test, after the participants had filled their bladder and initiated voiding in the bathroom in the sitting position, they were able to slow or even stop urine flow midstream. 15
The 1-hour pad test was performed based on the recommended protocol of the International Continence Society. Patients were asked to avoid emptying their bladder before the test and to wear a pad that had been weighed. The patients sat or rested until the end of the first half hour after drinking 500 mL of sodium-free liquid (e.g., distilled water) in 15 minutes. Then the patients had to complete the recommended types of exercises during the next half hour, after which the pads were reweighed to calculate urine loss. 15
Pelvic floor muscle strength evaluation
The strength of the pelvic floor muscle was measured by palpation with one-two fingers, and the pelvic floor muscle function was evaluated according to the PERFECT scheme, which includes assessments of the power (P), endurance (E), number of repetitions (R), and number of fast (1 second), contractions (F). Additionally, every (E) contraction (C) was timed (T). The power was graded from 0 to 5, according to the Oxford grading system. The PERFECT scheme of the pelvic floor muscle evaluation was recorded and was used as an exercise program for the pelvic floor muscle training group. This evaluation was adapted from the PERFECT method described by Laycock and Jerwood. 12
Perineometer measurements of pelvic floor muscle contractions showed very good interrater reliability and intrarater reliability. 16 The pelvic floor muscle contractions were measured using the Peritron 9300V perineometer (Cardio Design, Victoria, Australia), which is a conical vaginal insert 28 mm in diameter and 108 mm in length. Covered in a thin, medical-grade silicon rubber sheath, the vaginal insert was connected to a microprocessor that allowed for the transmission of pressure readings in centimeters of water (cmH2O) when the insert was compressed by external pressure. After the patients has voided, the vaginal squeeze pressure was assessed by the same examiner using perineometry. The vaginal pressure probe was placed inside the vagina at a location where 0.5 to 1 cm of the insert was visible outside the body. The perineometer was then inserted into the vagina until 1 centimeter of the sheath remained outside the body. No biofeedback was given during the measurements.
A diagnostic ultrasound imaging unit set in B mode (Ultrasonix-ES500, Canada) with a 3.5-MHz curved array transducer was used for transabdominal ultrasound measurement. For visualization of the bladder base, a standardized bladder filling protocol was used before imaging. We measured the amount of bladder base movement on ultrasound as an indicator of pelvic floor muscle contraction, based on previously established methods. The marker was first placed on the bladder base at the rest. A marker ‘X’ was placed on the image of the central portion of the bladder base at the junction of the hyperechoic and hypoechoic structures in the region of the greatest displacement visualized during a pelvic floor muscle contraction. For the displacement of the pelvic floor elevation, patients were asked to perform three pelvic floor muscle contractions. Each image was captured at the point of maximal displacement and again marked with an ‘X’. The displacement was measured as the distance between the two ‘X’ points (in millimeters). An ultrasound transducer was immediately placed in the transverse and longitudinal planes suprapubically angled in a caudal/posterior direction to obtain a clear image of the inferior–posterior aspect of the bladder. The ultrasound transducer was not displaced during the testing procedure, and the patients were not able to see the ultrasound screen to avoid a biofeedback training effect. The reliability of the transverse transabdominal ultrasound measurement for pelvic floor muscle contraction (inter-rater correlation coefficient= 0.93, standard error of measurement= 0.13) has been previously reported. 17
For the strength of pelvic floor muscle evaluation, the patients were tested in a crook-lying supine position with one pillow underneath the head. The hips and knees were flexed to 60°, and the lumbar spine was positioned in neutral. The patients were tested in the same position for the PERFECT, perineometric, and ultrasonographic measurements in lithotomy. Patients were instructed to empty the bladder for all analyses but the ultrasonographic measurements.
All of the measurements of the strength of the pelvic floor muscle were randomized to initial, second and last test to generate a table of random numbers. It was aimed preventing from bias by this way. For the alignment, the PERFECT, perineometric and ultrasonographic measurements were performed on the same day. A 30 minute resting period was given between the muscle strength tests. Each measurements technique was performed three times, and the average of these three measurements were calculated. All contractions were held for 5 seconds, with a rest of 10 seconds after each contraction.
Pelvic floor muscle training
At the first visit, the patients individually received verbal information about the pelvic floor anatomy muscle localization and function using anatomic models and illustrations. Advice on bladder hygiene was also given. We applied motor re-learning on steps to learning correct muscle contraction. 18 They then learned how to correctly contract the pelvic floor muscle without contracting the adjacent muscles (such as the abdominal, gluteal, or hip adductor muscles) with verbal instructions and palpation of the perineal body. The training focused on better pelvic floor muscle awareness and contraction and the exercises were individualized according to the degree of pelvic floor weakness, loss of proprioception, and the patient’s tolerance.
The intervention was performed by the same physiotherapist during a pelvic floor muscle training period of 12 weeks with the patients undergoing 30 min sessions three times a week for the first two weeks. These candidates, along with the patients, received posture training for the first two weeks. Damage to the pelvic floor that may develop because of bad posture was explained. They were also trained on how to fill in an exercise schedule.
After they were trained to correctly contract their pelvic floor muscles, individual exercise schedules were designed according to PERFECT scheme data. The patients were given the schedules in written form. The exercise schedules included information on the correct position to assume for each exercise, the speed of contractions (either slow or rapid), the number of repetitions, the time between contractions and the length of rest between the repetitions, the number of times to do the exercises daily and how many weekly repetitions to perform. We aimed to increase muscular strength and endurance with pelvic floor muscle training. The recommendations of The American College of Sport Medicine and the principle of progressive overload (e.g. by increasing more than normal the resistance to movement or frequency and duration of activity) in exercise prescription were applied for the general strength training for the patients. 18
When the women visited the physical therapist on the 2nd, 4th, 6th, 8th, 10th and 12th weeks, correct contraction of the pelvic floor muscles was checked by palpation of the perineal body and vaginal assessment using the PERFECT scheme. The women were asked about changes in their symptoms and adherence to pelvic floor muscle training. The exercise schedules were monitored. The patients were shown their progress from week to week, according to the PERFECT scheme. According to the progress indicated by PERFECT, exercises were added and hard copies of their new schedules were provided to the patients.
All of the women were required to keep a training diary to maintain their motivation during training. In addition, for coordination training, all women were advised to precontract and to hold a contraction before and during coughing, sneezing, and lifting in their daily lives to give added urethral support and to control leakage. Miller et al. 19 named this voluntary counterbracing-type contraction the ‘knack’. They were also advised to integrate the exercises into their activities of daily living. Volunteers in the control group were placed on a wait list for 12 weeks and then began to receive treatment. Also these volunteers had never been included in the pelvic floor muscle training group.
Additional program group
At the end of the 12-week pelvic floor muscle training, patients whose pelvic floor muscle strength did not reach a level of 5 (according to the Oxford grading system) and who agreed to do so, continued the exercise program (required pelvic floor muscle strength of grade 5, in the standing position). Of the 58 people who had completed the initial program, 34 of them continued with the additional program. The length of the program was dependent on the strength of the patients’ pelvic floor muscles. Those who had weak pelvic floor muscle strength needed to continue the exercise program for a longer time to achieve a grade of 5 compared to those patients whose pelvic floor muscle strength was higher. Twenty-four patients did not continue the program. The patients who did not continue were given a maintenance program.
Data analysis
Our sample size was analyzed using an Instat sample size calculator. A clinically relevant reduction of urine loss by a 1-hour pad test, at least 2 g, which is a medium-sized effect, was used to calculate the sample size. There was a two-sided alpha value of 0.05, a power of 0.8, and a sample size of 60 per group. To allow for dropouts, the sample size was set at 65.
All measurements were entered into a spreadsheet (Microsoft Excel v2002). The data analysis was performed using a statistical software program (SPSS Inc. v 15.0). All results were expressed as the means ± standard deviations. The size of the sample in this study adhered to the terms and conditions governing parametric tests. Values within the study groups themselves were compared utilizing a paired t-test both before and after the training. Independent t-tests were used to determine any differences in values between the pelvic floor muscle training and control group, both before and after the training. The significance level of 0.05 was chosen. Bladder diary and perineometric parameters were analyzed based on the average value of the three measurements.
The effect size was calculated for the results of the physiotherapy at before intervention and after intervention. According to Kazis et al. 20 the effect size was calculated as the mean score difference divided by the standard deviation from the initial measurement. An effect size >0.80 is considered high.
Results
A total of 130 women with stress and mixed urinary incontinence were randomized to the pelvic floor muscle training or control group, but nine women did not complete the study (drop-out rate 7%). In the pelvic floor muscle training group (drop-out rate 11%), five women dropped out because of changes in their work situation, and the other two women dropped out because of other health problems. In the control group (drop-out rate 3%), two women dropped out because they disliked the vaginal evaluation (Figure 1).
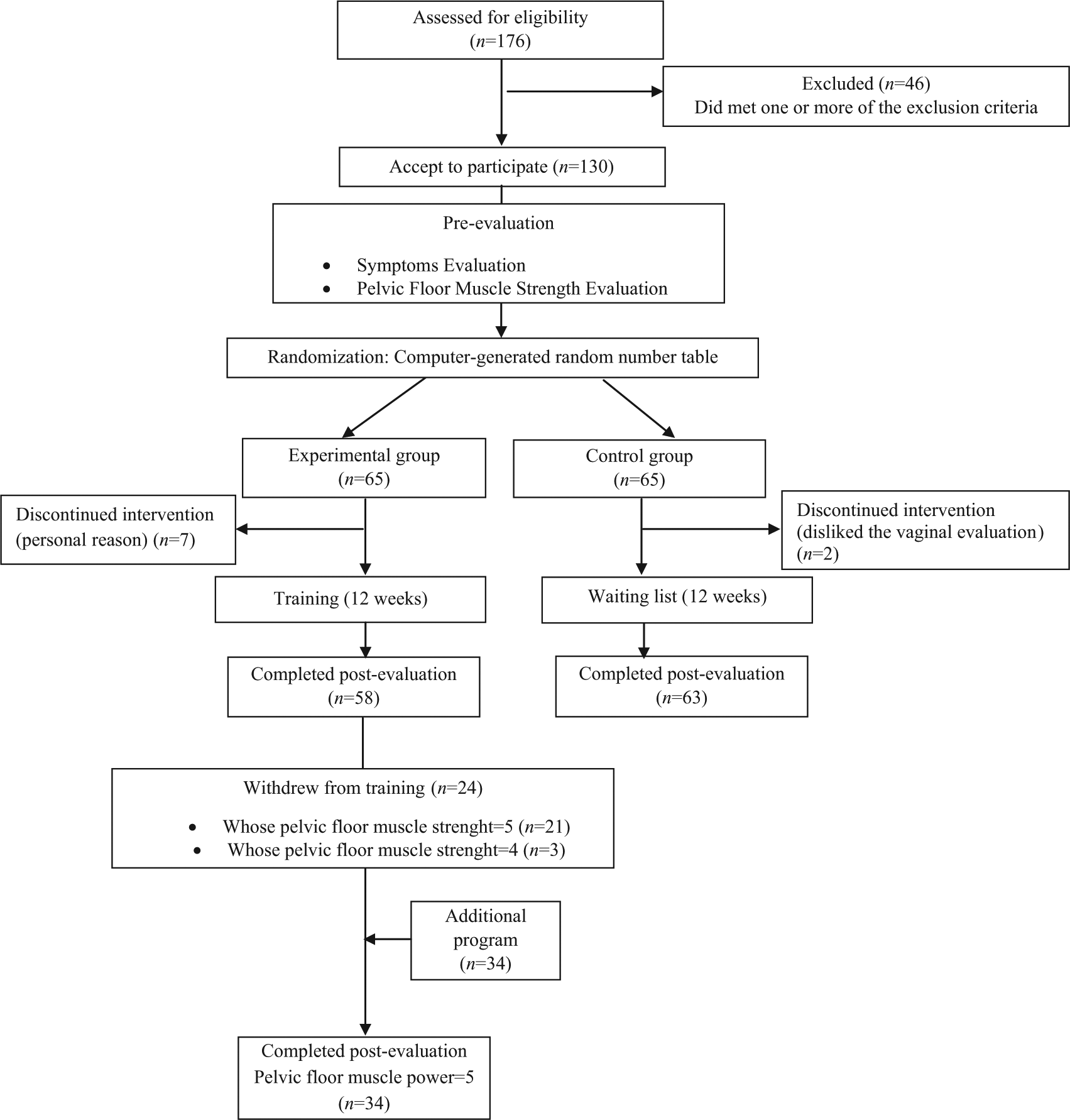
Design of the study (CONSORT flow diagram).
The baseline demographic and clinical characteristics of the patients are presented in Tables 1 and 2. Regarding the type of delivery, 81.3% of the patients had a vaginal delivery, 68.4% reported having an episiotomy, and 31.3% underwent a cesarean section. The analysis between the two groups indicated no significant differences in the demographic characteristics (Table 1). The comparison of the groups revealed no significant differences at baseline of clinical characteristics for Urogenital Distress Inventory-6, urgent urinary voiding, day time urinary frequency, urinary incontinence frequency, 1-hour pad test, stop test and pelvic floor muscle strength measurements (P>0.05). When compared with the control group, the women who underwent pelvic floor muscle training had lower Incontinence Impact Questionnaire-7 scores and higher nighttime urinary frequency before the intervention (Table 2).
Baseline values of pelvic floor muscle training and control groups.
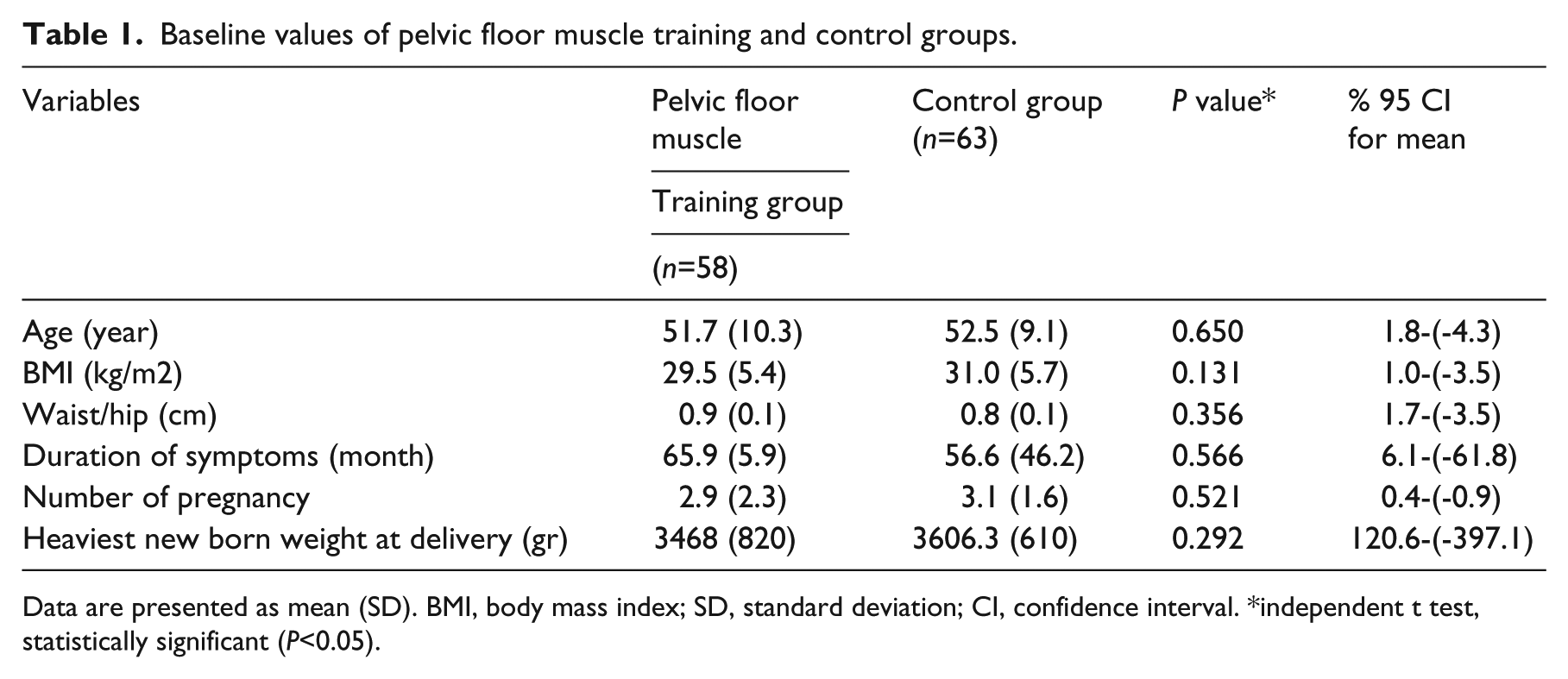
Data are presented as mean (SD). BMI, body mass index; SD, standard deviation; CI, confidence interval. *independent t test, statistically significant (P<0.05).
Comparisons of urinary incontinence symptoms and strength measurements of pelvic floor muscle before and after 12 weeks of treatment, between and within groups.
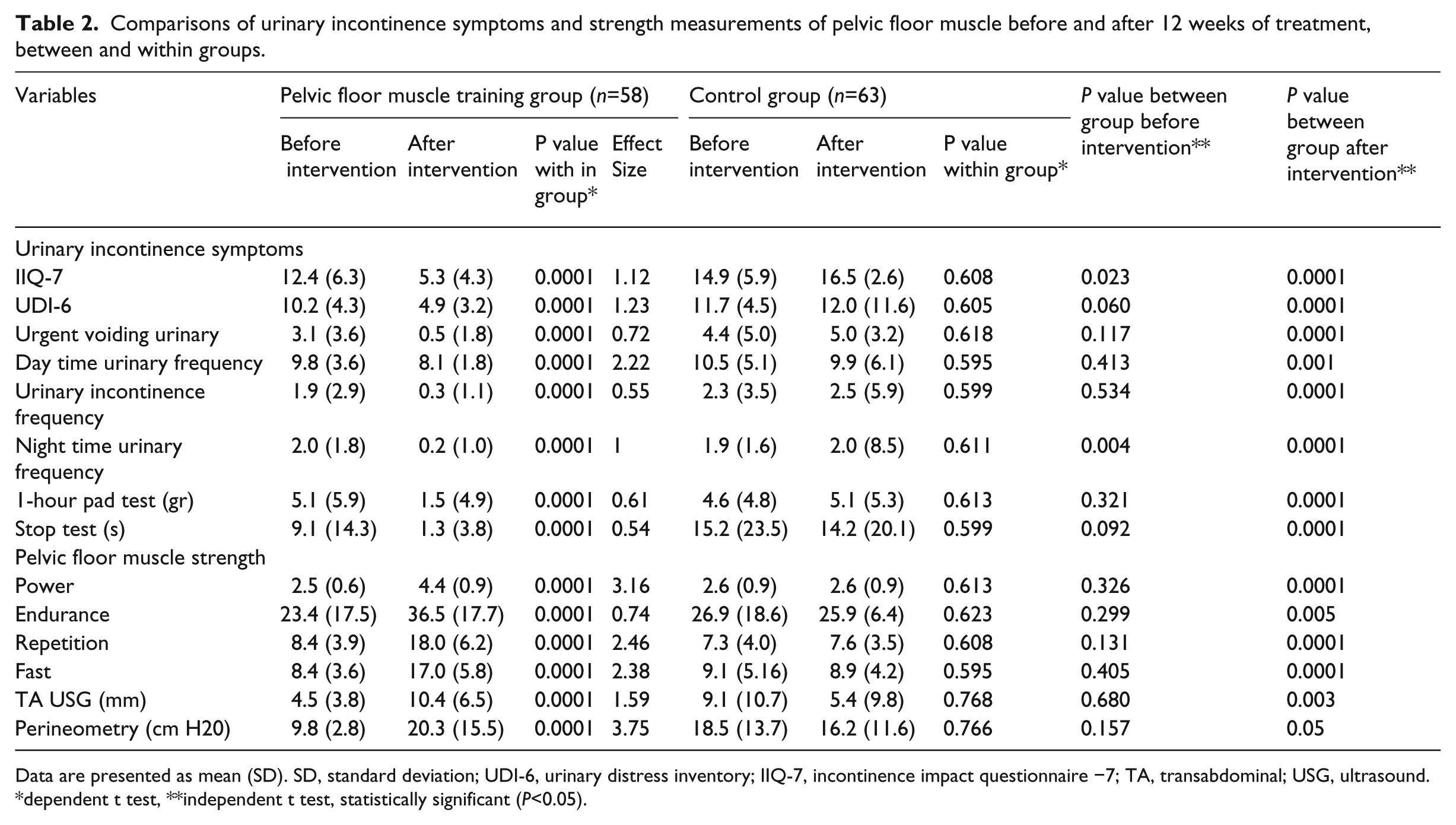
Data are presented as mean (SD). SD, standard deviation; UDI-6, urinary distress inventory; IIQ-7, incontinence impact questionnaire −7; TA, transabdominal; USG, ultrasound. *dependent t test, **independent t test, statistically significant (P<0.05).
Primary outcomes
The comparison of the results of all the urinary incontinence symptoms and the pelvic floor muscle strength between the groups is shown in Table 2. In the pelvic floor muscle training group, there was significant improvement in the symptoms of urinary incontinence and pelvic floor muscle strength after treatment compared to before treatment (Table 2). In the control group, there were no statistically significant differences before and after the intervention (Table 2). Improvements in all measurement parameters were significantly higher in the pelvic floor muscle training group than the control group after the 12-week treatment (P<.001) (Table 2).
Primary outcomes
After 12-weeks training of 58 patients, pelvic floor muscle strength increased to 5 in 21 patients (36.20%), to 4 in 33 patients (56.89%), and to 3 in 4 patients (6.8%). Pelvic floor muscle training was stopped in 21 patients whose pelvic floor muscle strength increased to 5. Three subjects (pelvic floor muscle strength was 4 for all) from pelvic floor muscle training group declined to continue to the study due to reasons such as ‘I am symptom free now’, ‘I will continue my exercises at home’ or ‘the distance between my home and clinic is so far’. Additional training program was supplied 34 (drop-out rate 8%) subjects in pelvic floor muscle training group (Figure 1). At the beginning of the additional training program, the strength grade of 29 patients was 4 and the strength grade of four patients was 3. Additional training program was carried on until the strength grade of the patients increased to 5. After 8-weeks of additional training, strength grade of two patients increased to 5 which was 3 at the beginning and after 12-weeks of additional training, strength grade of one patient increased to 5. The strength grade increased to 5 in six patients 8 weeks later and in 23 patients 4 weeks later, which was 4 at the beginning in all 29 patients.
Of the patients in the additional program who reached a pelvic floor muscle strength of grade 5, all except one of them achieved a score of zero during the ‘stop test’. After 12 weeks of treatment, a 1 gram urine loss measurement by the pad test was only found for four cases, and in other cases the scores were zero. While incontinence was eliminated according to the bladder logs of almost all patients, only two cases continued pelvic floor muscle training. Night time urination was eliminated in virtually all patients; only two people experienced a single night time urination. All the symptoms of urinary incontinence were significantly decreased in the patients that had reached pelvic floor muscle strength of grade 5 and continued the pelvic floor muscle training for an additional 12-week course (Table 3).
Improvement on symptoms of pelvic floor muscle training group after additional program.
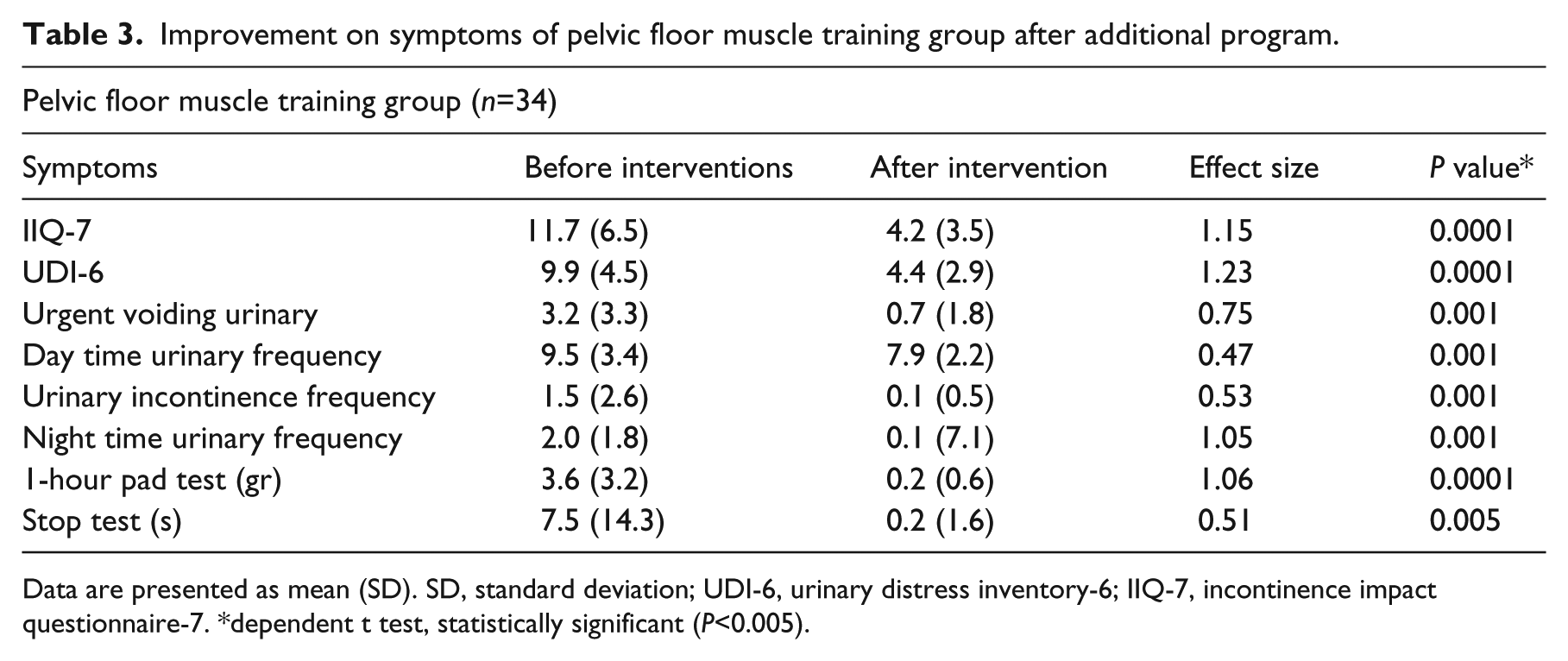
Data are presented as mean (SD). SD, standard deviation; UDI-6, urinary distress inventory-6; IIQ-7, incontinence impact questionnaire-7. *dependent t test, statistically significant (P<0.005).
Discussion
The present study demonstrated that, in patients with urinary incontinence, symptoms were reduced as the pelvic floor muscle training strengthened the pelvic floor muscles. Women in this study achieved a mean reduction in frequency of urinary incontinence of 83.1% and a mean reduction in urine loss by the 1-hour pad test of 71%. Additionally, 85.6% of women achieved the ability to stop urine flow midstream by the stop test, and there were improvements in the power measurements, Incontinence Impact Questionnaire-7, and Urogenital Distress Inventory-6 of 57%, 57%, and 74%, respectively.
The urinary incontinence symptoms almost completely disappeared in all but two patients when pelvic floor muscle strength of grade 5 (according to the Oxford system) was achieved. The symptoms were eliminated in 94.1% of the patients. The majority of the symptoms were greatly reduced when the pelvic floor muscle strength of grade 5 was achieved. However, the rate of reduction varied according to the parameters used to evaluate the symptoms.
Literature has been published describing investigations conducted to determine the impact of pelvic floor muscle training on pelvic floor muscle strength and the amount of urine loss. 3 In these studies, to measure pelvic floor muscle strength, quality of life and symptoms, different and similar methods to the current study were used. In addition to urinary incontinence in different populations, urinary incontinence in patients of different ages and the effect of various pelvic floor muscle training methods were analyzed. However, the aforementioned studies did not investigate whether symptoms of urinary incontinence decrease as pelvic floor muscle training is increased; they only examined the relative differences in pre-treatment and post-treatment pelvic floor muscle strength and contrasted that between different groups of patients and groups with differences in the training content. In general, these studies showed that pelvic floor muscle strength training caused a reduction in symptoms and an increase in the quality of life of patients with urinary incontinence, and we reached similar conclusions through our study.3,4,8–11,21–23
A valid and reproducible measurement is very difficult to obtain, although objective evaluations, such as perineometry and transperineal ultrasound, should help us understand the correlation between pelvic floor muscle strength and urine loss. The use of a scale based on the sensitivity of fingers introduced in the patient’s vagina during the contraction of the pelvic muscles (digital palpation) is a very common procedure in the diagnosis and analysis of urogynecological dysfunctions. Despite its subjective nature, the modified Oxford scale is a useful diagnostic tool; additionally, it is cheap and very simple to perform. However, it is strongly dependent on training and experience. 3 Madill et al., 6 in a study conducted on older women, found that as pelvic floor muscle training increased, symptoms of urinary incontinence decreased. In that study, pelvic floor muscle strength was evaluated by objective methods, such as electromyography, dynamometer and magnetic resonance imaging, and the study concentrated more on the effects of pelvic floor muscle training on muscle morphology. In our study, pelvic floor muscle strength was measured using perineometry, PERFECT and ultrasound.
The American College of Sports Medicine recently issued a special communication on evidence-based progression models for resistance training in healthy adults.18,24–26 These recommendations could be used to elaborate exercise regimen protocols aimed at improving timing and strength. The article sets out the basic principles, including progressive overload, specificity, and periodization, that need to be incorporated into any resistance-training program to achieve maximum results. Pelvic floor muscle training regimens should also adhere to these principals. For example, in relation to pelvic floor muscle training, progressive overload implies that the intensity of the exercises and the number of repetitions should be gradually increased throughout the exercise program, the speed or tempo of the repetitions with submaximal loads should be adjusted according to the desired goal (i.e., to train for either endurance or strength), the rest periods should be shortened for endurance-improvement training or lengthened for strength and power training, and, finally, the overall volume of the training should be increased gradually. 24 By providing our patients with a personal exercise schedule, we were able to benefit from the PERFECT system because the goal was to improve the functioning of the pelvic floor muscle. When patients 2, 4 and 8 came for their check-up, according to the data obtained from PERFECT, to apply the overload principle, adjustments to their personal exercise schedules were uploaded. The personal adjustments to the pelvic floor muscle training included differences in training supervision (amount, individual versus group), in approach (one versus another, the effect of an additional component) and in the exercise training (type of contraction, frequency of training). The existing evidence was insufficient to make any strong recommendations about the best approach for pelvic floor muscle training. Women are offered reasonably frequent appointments during the training period because the data that were obtained consistently showed that women receiving regular (e.g., weekly) supervision were more likely to report improvement than women performing pelvic floor muscle training with little or no supervision.24,25 For this reason, the control patients were invited for a check-up on a regular two-week basis. Our purpose was to avoid the risk of interfering with increases in strength, to adjust the exercise schedules on a regular basis and to provide motivation to the patients.
Evaluations of the patients’ symptoms were conducted during weeks 0 and 12 because the International Consultation on Incontinence Committee recommends that supervised pelvic floor muscle training for women with stress incontinence is maintained for 8–12 weeks before reassessment and that these patients should be considered for referral for further management if they have not improved sufficiently at the evaluation. 1 The National Institute of Clinical Excellence guideline on the management of urinary incontinence in women recommends pelvic floor muscle training for at least three months. The guideline states that pelvic floor exercises were found to be effective in the treatment of incontinence in female patients in more than 50% of cases. 2 In compliance with the recommended guidelines, patients were treated for 12 weeks and similar conclusions were reached. 4 We were able to effectively treat more than 50% of the patients for urinary incontinence.
In some cases, all of the symptoms experienced by the patients treated in our study whose pelvic floor muscle strength reached grade 5 did not disappear completely. The pelvic floor muscle is composed of two distinct muscle fiber types defined based on their contractile characteristics. Approximately one-third of the pelvic floor muscle fibers are fast twitch (type II) fibers and 67% are slow twitch (type I) fibers.6,7,24 They both provide support for the pelvic organs and contribute to urinary and fecal continence. 6 The Oxford grading system only evaluates slow twitch fiber strength, or muscular strength. It does not assess muscular endurance. During our study, muscular endurance was observed to be considerably increased after the treatment; however, muscular endurance may not be sufficient to reduce some urinary incontinence symptoms. Therefore, more studies need to be conducted to examine the importance of endurance for urinary continence. During the course of daily activities, due to increased intra-abdominal pressure, muscle endurance becomes more critical for urinary continence than having a pelvic floor muscle strength of grade 5. There is no literature that describes how to measure the force that occurs on the pelvic floor muscles during activities of daily living. We used the Oxford grading system to measure people as grade 5 while they were at rest. All these reasons could explain the elimination of urinary incontinence symptoms in these patients. More studies on this subject need to be conducted.
The use of pelvic floor muscle training in the treatment of urinary incontinence is suggested with A-level evidences. Certain limitations of pelvic floor training could not be determined. The evidences for the length of the rehabilitation program to minimize the symptoms of urinary incontinence or to relieve them are insufficient. 23 It was seen that the required time to increase the pelvic floor muscle strength to 5 in the patients, receiving additional training, differs. The strength grade increased to 5 in patients, whose grade was 2 at the beginning of our study, in a mean of 20-24 weeks, and in patients, whose grade was 3, in 16-20 weeks and in patients, whose grade was 4, in 12-16 weeks. The length of the program depended on the strength of their pelvic floor muscles. While those who had weak pelvic floor muscle strength needed to continue the exercise program for a longer time in order to achieve a grade of 5, those participants whose PFM strength was higher continued the exercise training program for a relatively shorter time. It was seen that it was necessary to provide pelvic floor muscle training for a longer time to decrease the symptoms as long as the pelvic floor muscle strength decreased. The duration of the pelvic floor strengthening can be affected by the factors as age and sex. It should be studied more how long strengthening exercises should be provided in which Oxford level. Further studies are needed for certain time periods.
To determine whether the symptoms of urinary incontinence were abolished completely, an additional pelvic floor muscle training program was applied to the patients who accepted. This training program was carried on until the pelvic floor muscle strength of the patients reached grade 5 by digital palpation. In conclusion, it was found that symptoms of urinary incontinence were decreased but not abolished completely when the pelvic floor muscle strength of patients reached grade 5 by digital palpation. In the literature, we did not come across training programs that were continued until a pelvic floor muscle strength of grade 5 was obtained. Therefore, we believe that our study contribute to the literature and lead to future studies.
Besides the depression, in 15% to 30% of the cases, urinary incontinance affects the social, occupational, physical and sexual life of the women of all ages. The psychosocial impact can be more devastating than the consequences on health, with multi and comprehensive effects that influence daily activities, social interaction and self-perception of health status. The amount of urinary loss may influence the quality of life of incontinent women. Psychosocial status and quality of life are affected negatively with the increment in the amount of leakage in urinary incontinance patients. 27 In a result of increments in pelvic floor muscles strength with pelvic muscle strengthening exercises, significant reductions in number of voidings per day and number of leakages per day are observed. The quality of life also increases with pelvic muscle strength.28,29 We obtained similar result in accordance with the literature. In our study when the pelvic muscle strength increased; urgent voiding urinary, urinary incontinence frequency, night time incontinence frequency, Incontinence Impact Questionnaire-7 and Urogenital Distress Inventory-6 was decreased.
The limitations of our study were that perineometer pressure changes may have been affected by an increase in abdominal pressure due to cocontraction of the abdominal muscles rather than contraction of the pelvic floor muscle; we could have evaluated intra-abdominal pressure that was not affected by a pelvic floor muscle strength-measuring method; our results were limited to follow-up outcomes of pelvic floor muscle training; and, finally, other factors that can affect increased muscle strength (parity, age at birth of last child, menopausal status) could have been observed.
In conclusion, this study demonstrated that pelvic floor muscle training is effective in reducing urinary incontinence symptoms and increasing pelvic floor muscle strength in women with stress and mixed urinary incontinence. Pelvic floor muscle training, by increasing the strength of the pelvic floor muscle, decreases the symptoms of urinary incontinence. The duration of the pelvic floor rehabilitation should be kept longer in patients with weaker pelvic floor muscle strength. In addition to, the duration of the training is shorter in patients who have relatively stronger pelvic floor muscles. However, more studies need to be conducted.
Clinical messages
Symptoms of urinary incontinence were decreased but not abolished completely when the pelvic floor muscle strength of patients reached grade 5 by digital palpation.
The duration of the pelvic floor rehabilitation should be kept longer in patients with weaker pelvic floor muscle strength.
Footnotes
Acknowledgements
The authors thank the physiotherapist Seher Ozyurek for her help.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.