
Abstract
Objectives:
To investigate the acceptability and potential efficacy of two commercial video games for improving upper extremity function after stroke in order to inform future sample size and study design.
Design:
A controlled clinical trial design using sequential allocation into groups.
Setting:
A clinical occupational therapy department.
Subjects:
Twenty-four first-stroke patients.
Interventions:
Patients were assigned to one of three groups: conventional group, Wii group, and XaviX group. In addition to regular one-hour conventional rehabilitation, each group received an additional half-hour of upper extremity exercises via conventional devices, Wii games, or XaviX games, for eight weeks.
Main measures:
The Fugl-Meyer Assessment of motor function, Box and Block Test of Manual Dexterity, Functional Independence Measure, and upper extremity range of motion were used at baseline and postintervention. Also, a questionnaire was used to assess motivation and enjoyment.
Results:
The effect size of differences in change scores between the Wii and conventional groups ranged from 0.71 (SD 0.59) to 0.28 (SD 0.58), on the Fugl-Meyer Assessment of motor function (d = 0.74) was larger than that between the XaviX and conventional groups, ranged from 0.44 (SD 0.49) to 0.28 (SD 0.58) (d = 0.30). Patient enjoyment was significantly greater in the video game groups (Wii mean 4.25, SD 0.89; XaviX mean 4.38, SD 0.52) than in the conventional group (mean 2.25, SD 0.89, F = 18.55, p < 0.001), but motivation was not significantly different across groups.
Conclusion:
Patients were positive to using video games in rehabilitation. A sample size of 72 patients (24 per group) would be appropriate for a full study.
Introduction
Upper limb motor deficit is one of the main symptoms of stroke patients. Up to 85% of stroke patients experience hemiparesis immediately after stroke. 1 Between 55% and 75% of survivors continue to experience motor deficits associated with diminished quality of life. 1 Many daily living tasks are performed with the upper limbs; therefore, rehabilitation treatment of the upper limbs is very important for stroke patients. The most fundamental principle in motor learning is that the degree of performance improvement is dependent on the amount of practice. 2 Practice at its simplest, which is just performing the same movement repeatedly,2,3 may be the most effective way to improve performance during the training session itself. 2 However, most existing clinical upper extremity rehabilitation equipment provides no feedback to the patients. Patients may find repeating the same activity to be boring and monotonous and thus develop a negative attitude toward the therapy process.4,5 In order to increase the mental satisfaction and effectiveness of rehabilitation therapy, some therapists have been using alternative digital applications in rehabilitation,6,7 such as off-the-shelf video game systems. 1
Many studies have focused on the use of video game systems, such as the Nintendo Wii,1,4,8,9 the Playstation EyeToy, 10 Kinect, 5 and virtual reality devices in rehabilitation for stroke patients.11 –14 In terms of treatment effectiveness, some studies have found effective treatment outcomes on the Fugl-Meyer Assessment of motor function (FMA),4,13 –15 the Functional Independence Measure (FIM),14,15 the Box and Block Test of Manual Dexterity, 12 the Wolf Motor Function Test,1,12 and upper extremity range-of-motion measurements. However, other studies have found no significant effective treatment outcomes on the FMA. 12 Based on the above results, it is still debatable whether treatment with video gaming systems can effectively facilitate upper extremity functions, and this area still needs more research.1,16 –18 The acceptability of video games in stroke rehabilitation is also an area requiring further exploration.
Clinical studies have shown the importance of using objects to develop motor skills.19,20 Therefore, this study applied the control devices of active video game (exergame) systems, i.e. the Nintendo Wiimote and XaviX®Port gloves, in rehabilitation. The Nintendo Wii, the most well-known system, is the system that is most widely used in rehabilitation facilities.21,22 XaviX®Port has been supported by researchers in the fields of sports science and medicine, with the goal of preventing declines in motor and brain function in the elderly. 23 However, knowledge of the effectiveness and feasibility of using the XaviX®Port in rehabilitation is still limited.
Therefore, a pilot study was designed with two goals. The first was to investigate the acceptability and potential efficacy of two commercial video games to improve upper limb function after stroke in order to inform future sample size and study design, and the second goal was to compare the acceptability and potential efficacy of two treatment modalities.
Methods
Stroke patients were recruited from an outpatient occupational therapy department of Chung Shan Medical University Hospital in Taiwan. Inclusion criteria were as follows: (a) hemiparesis with upper extremity dysfunction following a single unilateral stroke; (b) a history of first-time stroke (3–24 months post-stroke); (c) a need for upper extremity rehabilitation to convalescent levels of Brunnstrom stages III to V; (d) ability to communicate, and to understand and follow instructions; and e) ability to maintain sitting and standing balance unsupported for two minutes under supervision (score ≧ 3 on the Berg Balance Scale). Exclusion criteria were as follows: (a) engagement in any other rehabilitation studies during the study; and (b) serious aphasia or cognitive impairment. Each patient gave informed consent. This study was approved by the Human Research Ethics Board of a local hospital.
This study was a single-blind clinical trial and used a pretest–posttest control group design. First, clinical therapists reviewed their patients with the inclusion criteria and asked about their willingness to participate in this trial. Subjects who accepted were asked to sign an informed consent form. The two assessors were blinded to the group assignment. All subjects were sequentially allocated into three groups (the XaviX®Port group, the Nintendo Wii group, or conventional group) by the researcher according to the order of recruitment (i.e. patient one goes into group A, patient two into group B, patient three into group C, patient four into group A, and so on). The functional ability of each subject’s affected upper extremity was assessed by one of the assessors in two stages: (1) prior to the interventions, and (2) immediately after completing all the training sessions. All subjects were asked to complete a total of 20 training sessions over eight weeks, scheduled at three 30-minute sessions per week (excluding set-up time). In addition to the training sessions in this study, all subjects also received at least one hour of occupational therapy and physical therapy, respectively. After the post-training assessment, each patient also completed the motivation and enjoyment questionnaire.
This study included three groups for treatment intervention: (1) the conventional group, (2) the Nintendo Wii group, and (3) the XaviX®Port group (Appendix, available online). In addition to the regular treatment, each group was assigned to use two specific games or devices in the additional treatment sessions. Specifically, the conventional group used two traditional devices, the Curamotion exerciser and the climbing board and bar; the Nintendo Wii group played bowling and boxing games; and the XaviX®Port group played bowling and ladder climbing games. The games and devices for the groups were selected by three occupational therapists, and their upper extremity movement requirements were evaluated similarly.
The FMA, 24 Box and Block Test of Manual Dexterity (BBT), 25 FIM, 26 and Range of Motion Measurement of the Upper Extremity (ROM) 27 was used at baseline and postintervention. ROM was used to assess the ranges of active joint motion of the shoulder, elbow, forearm, and wrist joints.
An interviewer-administered questionnaire was designed to evaluate the motivation and enjoyment associated with using traditional devices or video game devices. After completing all 20 sessions, each patient answered two questions. For motivation, the patients were asked, “Did the conventional/Wii/XaviX treatment increase your motivation?” For enjoyment, the patients were asked, “Do you feel that the conventional/Wii/XaviX treatment was interesting?” The motivation and enjoyment items were scored on a 5-point Likert-type scale, with 1 signifying “strongly disagree” and 5 being “strongly agree”. For motivation, we assessed whether each device increased the treatment motivation of patients who used the Nintendo Wii or XaviX®Port system for treatment. To assess enjoyment, we looked at how enjoyable patients found using the Nintendo Wii or XaviX®Port system for treatment to be.
Data analyses
All data were analyzed with SPSS for Windows version 13.0. The characteristics of the three groups were analyzed with descriptive statistics. The Wilcoxon signed ranks analysis was used for within-group analyses, and the Kruskal–Wallis test, for between-group analyses. Differences were considered significant when p < 0.05. The effect size d was calculated for each measurement to indicate the magnitude of group differences in performance. 28 The mean and standard deviation were calculated for each question on the questionnaire. G*Power 3.1 power analysis software was used to compute the sample size required to detect significant differences for the FMA baseline means between groups.
Results
A total of 28 post-stroke patients were recruited from the Occupational Therapy Department of Chung Shan Medical University Hospital from November 2011 to February 2013. The characteristics of the patients in the three study groups are shown in Table 1. There were no statistically significant differences among the three groups with regard to age and time since stroke onset. However, for the between-group differences at baseline, one-way analysis of variance (ANOVA) showed that ROM of the distal joints was significantly higher in the Nintendo Wii group than in the conventional and XaviX®Port groups (χ2 = 11.862, p = 0.003 < 0.01). A total of 24 consecutively screened stroke patients completed all the training sessions (see Figure 1 for the flowchart diagram of this study). 29 Of the four who did not finish, one of them was transferred out of the hospital owing to complications, one was discharged, and the other two failed to continue treatment. The two patients who failed to continue treatment missed their Occupational Therapy/Physical Therapy (OT/PT) and treatment sessions in this study more than three times, and the authors were unable to contact them.
Characteristics of stroke patients.
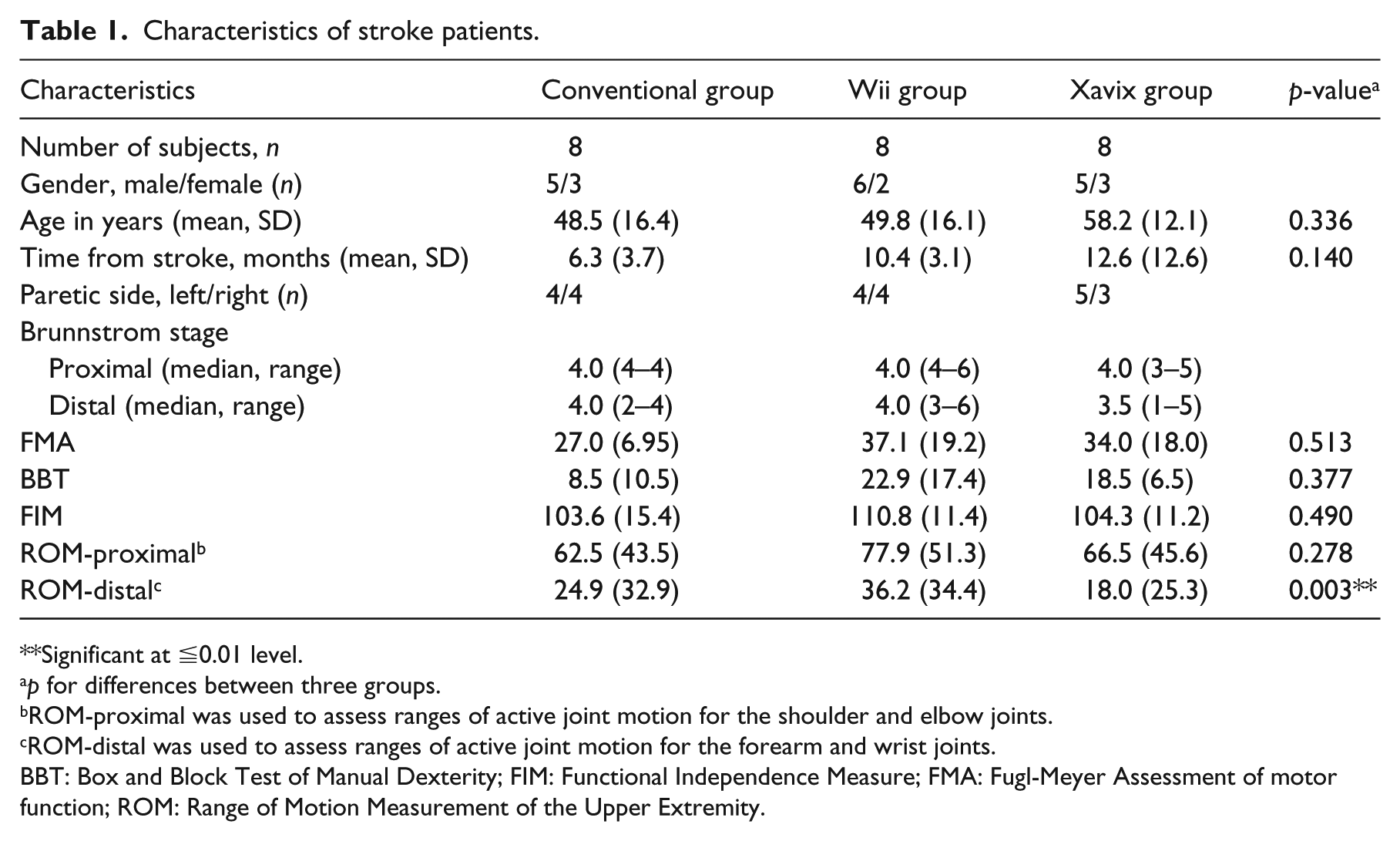
Significant at ≦0.01 level.
p for differences between three groups.
ROM-proximal was used to assess ranges of active joint motion for the shoulder and elbow joints.
ROM-distal was used to assess ranges of active joint motion for the forearm and wrist joints.
BBT: Box and Block Test of Manual Dexterity; FIM: Functional Independence Measure; FMA: Fugl-Meyer Assessment of motor function; ROM: Range of Motion Measurement of the Upper Extremity.
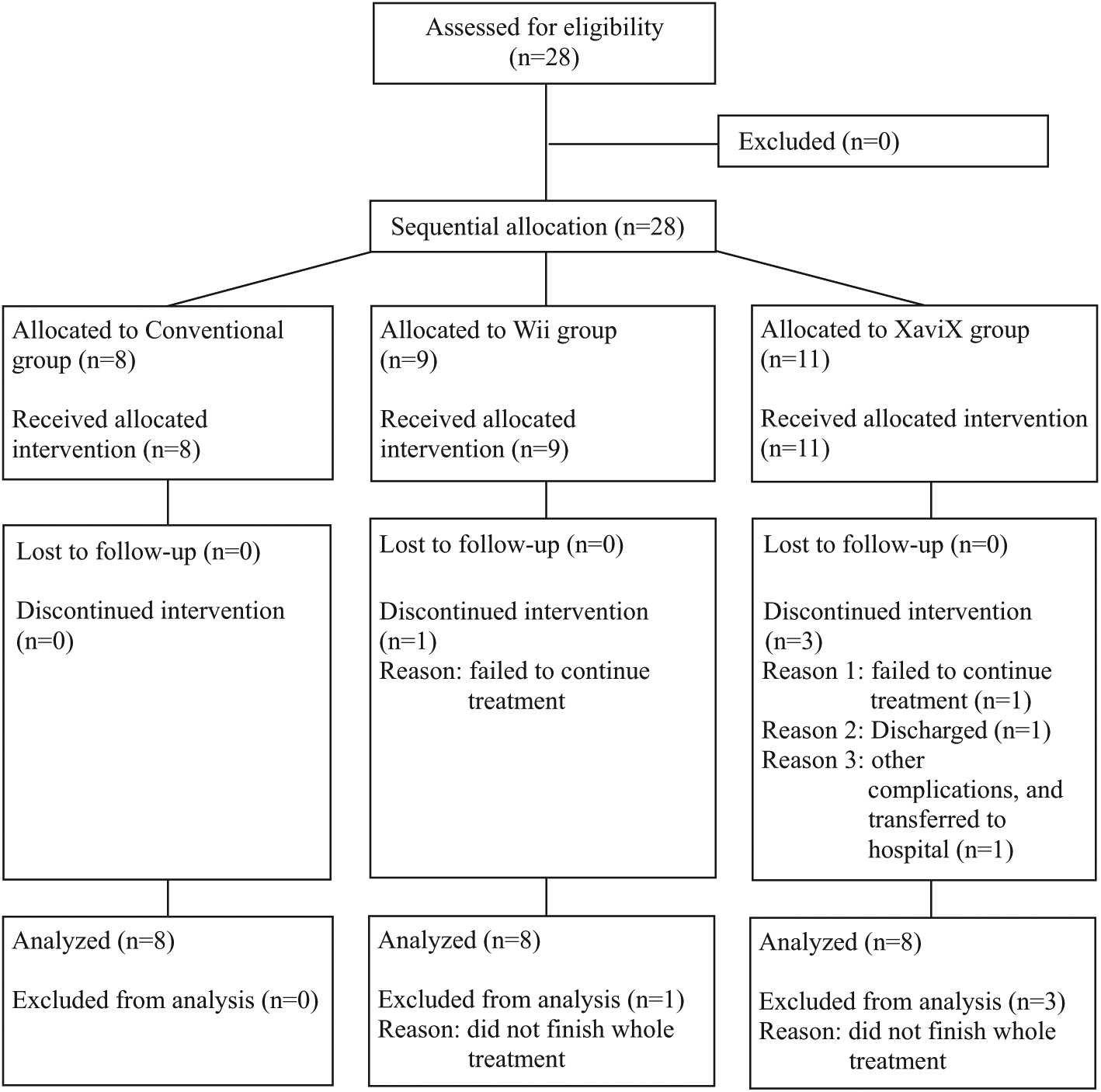
Flow diagram of the progress through the phases of sequential allocation trials in this study.
Regarding within-group changes, the groups showed significant improvements in upper extremity function (Table 2). The XaviX®Port group had significant differences on all four assessments (FMA, BBT, FIM, and ROM), while the conventional group and the Nintendo Wii group had significant differences on three of the four assessments (FMA, FIM, and ROM).
Comparison of the three groups for functional outcome measures.
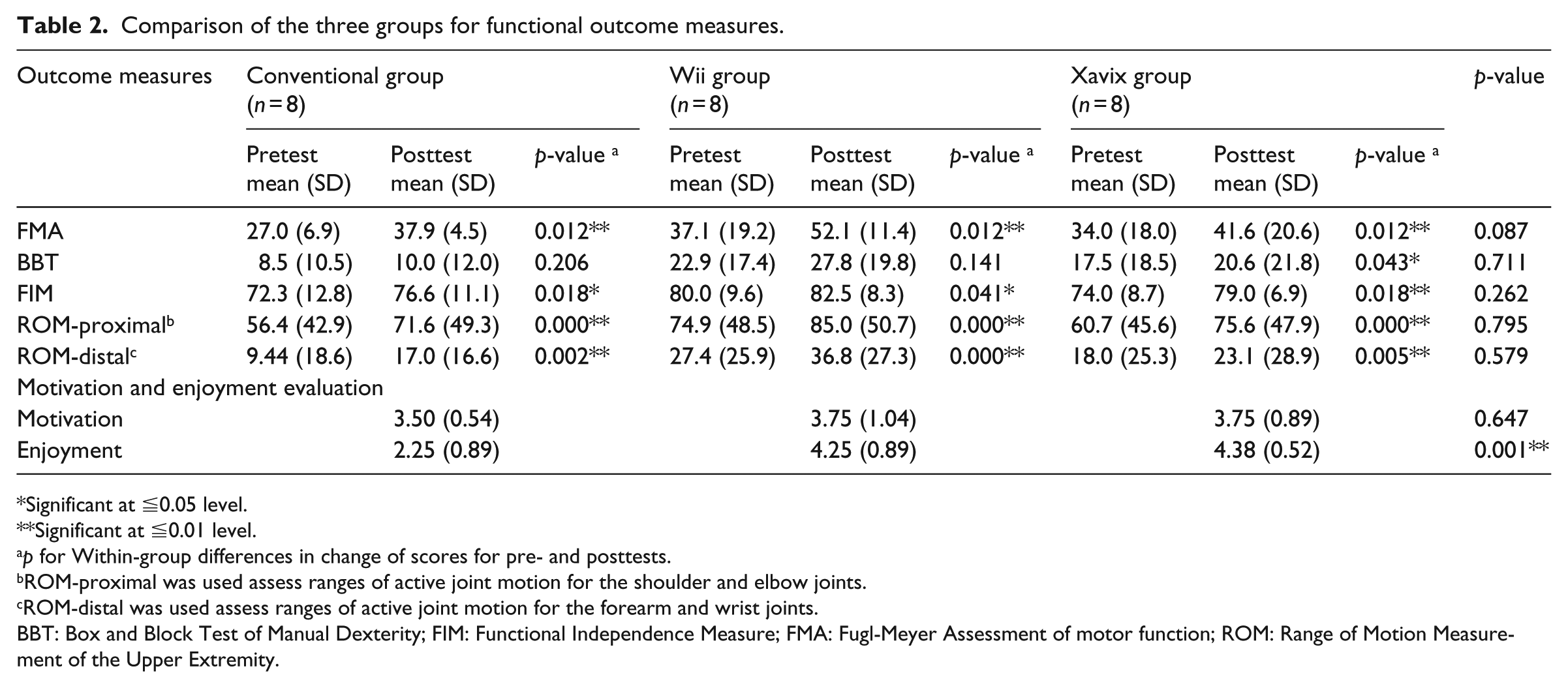
Significant at ≦0.05 level.
Significant at ≦0.01 level.
p for Within-group differences in change of scores for pre- and posttests.
ROM-proximal was used assess ranges of active joint motion for the shoulder and elbow joints.
ROM-distal was used assess ranges of active joint motion for the forearm and wrist joints.
BBT: Box and Block Test of Manual Dexterity; FIM: Functional Independence Measure; FMA: Fugl-Meyer Assessment of motor function; ROM: Range of Motion Measurement of the Upper Extremity.
For the between-group differences, the Kruskal–Wallis one-way ANOVA ranks test showed no significant between-group differences on all four outcome measurements (Table 2). The effect sizes of differences in the change scores between the Nintendo Wii and conventional groups ranged from 0.71 (SD 0.59) to 0.28 (SD 0.58), with the largest effect seen on the FMA (d = 0.74), and also between the XaviX®Port and conventional groups ranged from 0.71 (SD 0.59) to 0.28 (SD 0.58) on the BBT (d = 0.67). The effect sizes of differences in the change scores between the Nintendo Wii and conventional groups ranged from 0.04 (SD 0.07) to 0.01 (SD 0.03), with a moderate effect on the BBT (d = 0.56) and also between the Nintendo Wii and XaviX®Port (d = 0.50). The effect sizes of differences in the change scores between the XaviX®Port and conventional groups ranged from 0.44 (SD 0.49) to 0.28 (SD 0.58), with the smallest effect seen on the FMA (d = 0.30).
Regarding motivation and enjoyment, patients in the Nintendo Wii and XaviX®Port groups reported that using video games in treatment increased their treatment motivation. In the Nintendo Wii group, 38% (n = 3) of the people gave ratings of 4, and 25% (n = 2) of the people gave ratings of 5; in the XaviX®Port group, 63% (n = 5) of the people gave ratings of 4, and 13% (n = 1) of the people gave ratings of 5; in the conventional group, only 50% (n = 4) of the people gave ratings of 4 and 50% (n = 4) of the people gave ratings of 3. However, there were no significant between-group differences in motivation among the three groups (F2, 21 = 0.23, p > 0.05). Enjoyment was significantly greater in the Nintendo Wii and XaviX®Port groups than in the conventional group (F2, 21 = 18.55, p < 0.001). In the XaviX®Port group, 63% (n = 5) of the people gave ratings of 4, and 38% (n = 3) of the people gave ratings of 5; in the Nintendo Wii group, 25% (n = 2) of the people gave ratings of 4, and 50% (n = 4) of the people gave ratings of 5. In contrast, in the conventional group, none of the people gave ratings of 4 or 5.
The current data were also used to compute the number of patients required to detect significant between-group differences for the FMA baseline means. Using an estimated effect size f of 0.40, alpha of 0.05, and power 85%, it was determined that a total of 72 patients (24 patients in each group) would be needed for a full study.
Discussion
These results are consistent with those of other studies12,16 reporting that Nintendo Wii games improve upper extremity function on the FMA. For the Nintendo Wii, the effect size was large on the FMA. This result can be explained as follows: (1) device-specific factors, such as the precision and sensitivity of the sensors and/or differences in surface texture; and (2) the greater challenges presented by the Nintendo Wii Remote than by the XaviX®Port system. In order to successfully complete the action, patients had to use their distal upper extremity to press the buttons. This action in the Nintendo Wii group could induce the fingers to execute motor skills and further increase the effectiveness of the therapy.
In terms of the performance outcomes, we identified the potential efficacy of the two commercial video game systems to improve upper extremity function after stroke. We found significant improvements on the FMA, FIM, and ROM in each group, and a significant improvement on the BBT in the XaviX®Port group, from the pretest to the posttest. Although the effectiveness of the between-group differences did not reach significant differences, the results suggest that training with commercial video games may improve upper extremity function.
The results of this study show that the motivation of patients was slightly better in the video game groups than in the conventional group. This finding is consistent with those of other studies indicating that video games increase motivation for rehabilitation. 5 The increased motivation with the use of video games could result from the following: (1) video games serve as motivators 30 because the games make patients focus on playing the game, distracting their attention from the fact that they are in rehabilitation, and (2) the high motivation in the video game groups results from the high interest level of the games, and patients play them happily and voluntarily. This increase in motivation is important because active participation in rehabilitation programs increases the benefits and effectiveness. 31 In contrast, motivation was lower in the conventional group than in the video game groups, and the individuals in the conventional group indicated that they had no choice but to participate in the therapy if they wanted to improve.
Enjoyment was higher in the video game groups than in the conventional group. One potential advantage of the use of these games for rehabilitation is the psychological effects. These games may facilitate motor learning 30 while increasing enjoyment and interest in rehabilitation by promoting motivation through the built-in commentary, prizes, and visual and verbal cues, all of which tap into patients’ innate competitive natures and into their desire for interaction.1,16 These advantages may increase the effectiveness of the patients’ rehabilitation therapy. Therefore, the researchers suggest that video games be incorporated into the design of digital rehabilitation devices or the redesign of traditional rehabilitation devices. 31
Based on these preliminary results on a small number of patients, it is difficult to definitively advocate video game intervention therapy over conventional therapy for rehabilitation of the upper extremities. For comprehensive understanding of the effects of the video game intervention therapy, we suggest that a full study would require at least 24 patients in each group, in order to have the power to demonstrate statistically significant differences in effectiveness between the three groups. In addition, five suggestions are proposed for future studies: (1) appropriate functional measures for the upper extremities must be selected; (2) the intensity of the intervention therapy times 4 should be increased based on the motor learning concept;2,3 (3) the individual differences of patients must be considered, possibly using a repeated measures design, for such differences may affect the significant differences in effectiveness between groups; (4) block-randomization considering time since stroke could be designed into a larger study to ensure uniformity; and (5) participants should be recruited from more than one hospital.
Three limitations of this trial are noteworthy. First, because of the difficulty in finding eligible patients who met all the inclusion criteria of this study in just one hospital, we had a relatively small sample size. Second, the time since stroke onset (3–24 months) may have been too long, and this factor may have influenced the recovery potential. Third, considering the rules of research ethics and the interests of patients, their regular treatment was not discontinued; therefore, we had difficulty determining the intensity of the therapeutic effectiveness in the Nintendo Wii or XaviX®Port gaming system groups. Thus, further research is needed to examine the long-term effects and intensity of using video games in rehabilitation. Fourth, this study is not a randomly allocated study. This may increase the risk of bias.
In conclusion, a controlled pilot trial of two commercial video games for rehabilitation of arm function after stroke has shown that video games may improve upper extremity function while also increasing motivation and enjoyment in stroke patients, but the increases in effectiveness and motivation found in this study were not significant. Based on the results of the pilot study, the authors provide suggestions (i.e. using appropriate functional measures and methods, increasing the intensity of the intervention therapy times, including block-randomization, and recruiting from more sources) for a larger study to develop further support for the increases in effectiveness and motivation.
Clinical messages
Patients reported greater enjoyment with video games, which are feasible to use in rehabilitation.
A larger sample size with at least 72 participants (24 per group) would be needed to reach an inferred conclusion of efficacy for rehabilitation of upper limb function.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This study was partly supported by the Ministry of Science and Technology with grant No. NSC 100-2221-E-040-009-MY2.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.