
Abstract
Objective:
To assess single-session effects of three different types of stimuli known to increase cortical excitability when combined with functional task practice.
Design:
Randomized cross-over trial.
Participants:
A total of 24 participants with chronic cervical spinal cord injury.
Interventions:
One 30-minute session of each, applied concurrently with functional task practice: transcranial direct current stimulation, vibration, and transcutaneous electrical nerve stimulation.
Measurements:
Nine-hole Peg Test, pinch force, visuomotor tracking, and cortical excitability were collected at pretest, posttest and late posttest (30 minutes after). Early effects (posttest minus pretest) and short-term persistence (late posttest minus pretest) were assessed using a general linear mixed model. Magnitude of effect size was assessed using the Cohen’s d.
Results:
Transcutaneous electrical nerve stimulation was associated with moderate, significant early effects and short-term persistence on Nine-hole Peg Test performance (1.8 ±1.8, p = 0.003, d = 0.59; 2.0 ±2.5, p < 0.001, Cohen’s d = 0.65, respectively). Transcranial direct current stimulation (1.8 ±2.5, p = 0.003, Cohen’s d = 0.52) was also associated with significant short-term persistence of moderate size on Nine-hole Peg Test performance (1.8 ±2.5, p = 0.003, Cohen’s d = 0.52) and visuomotor tracking performance (p = 0.05, d = 0.51). Early effects on corticomotor excitability were significant for transcutaneous electrical nerve stimulation (p = 0.003), approached significance for transcranial direct current stimulation (p = 0.07), and only vibration was associated with significant short-term persistence (p = 0.006).
Conclusions:
Meaningful improvements in aspects of hand-related function that persisted at least 30 minutes after intervention were observed with transcutaneous electrical nerve stimulation and transcranial direct current stimulation, when combined with functional task practice.
Keywords
Introduction
Individuals with tetraplegia have varying degrees of upper extremity impairment, and restoration of hand/arm function is consistently cited as a priority in their rehabilitation goals.1,2 In addition to the damage to the ascending and descending tracts resulting from the primary injury, there is evidence of functional reorganization of the sensorimotor cortex that occurs postinjury. 3 It has been argued that this postinjury functional reorganization contributes to the impairment of function by limiting the ability of the cortex to drive efferent information down the spared spinal pathways. 4
Individuals with chronic incomplete tetraplegia who participated in intense functional task practice training (performed for two hours/day, five days a week for three weeks), in isolation or combined with somatosensory stimulation (i.e. low-amplitude, long pulse duration peripheral nerve stimulation) demonstrated significant changes in skilled hand use. 5 A follow-up study demonstrated that the combination of functional task practice and somatosensory stimulation led to greater gains in skilled hand function than when either approach was used in isolation, and the use of somatosensory stimulation in isolation is associated with significant improvements in pinch grip strength. 6 Taken together, these results suggest that stimulation can have a potent effect on motor control, and that stimulation may augment the effects of functional task practice.
In addition to somatosensory stimulation, other approaches have been used to deliver indirect cortical activation and have been associated with increased cortical excitability, such as vibratory stimulus 7 and transcutaneous electrical nerve stimulation, 8 but their effects on hand motor performance are not fully understood. In counterpart, transcranial direct current stimulation (i.e. the application of mild, monophasic currents to the scalp) has been shown to exert a neuromodulatory influence on the underlying neural tissue, thus providing a more direct approach to brain stimulation. Transcranial direct current stimulation has been associated with gains in hand motor performance, both in individuals with stroke 9 and neurologically healthy controls.10,11 In light of the decreased cortical excitability observed after tetraplegia, 12 and larger training effects observed when functional task practice is combined with somatosensory stimulation,5,6 we undertook an exploratory study to assess single-session outcomes of cortical excitability and hand function associated with a combined approach consisting of functional task practice with clinically accessible approaches for directly or indirectly increasing corticomotor excitability.
Methods
Participants with chronic tetraplegia owing to cervical spinal cord injury (SCI) were recruited from the research volunteer database of The Miami Project to Cure Paralysis. To be included, participants needed to be between 18–70 years of age with a history of an injury to the cervical spine at C7 or above at least one year prior to enrollment. Additionally, participants needed to have a preserved ability to voluntarily produce a visible twitch of the thenar muscles of at least one hand. Exclusion criteria were a history of head injury, family history of seizures or the presence of metal elements in the cranium (e.g. aneurysm clip), and any other neurologic, orthopedic, or cognitive condition that could affect the performance on the outcome measures. Following screening and informed consent to participate in the study, participants received instructions to maintain their usual level of activity and to not alter their medication regimen. This study was approved by the Human Subjects Research Office of the University of Miami Miller School of Medicine, Miami, FL.
We conducted a randomized crossover study consisting of one session of each stimulation condition (transcranial direct current stimulation, transcutaneous electrical nerve stimulation, and vibration) while participants engaged in functional task practice. Because our interest was in the comparative efficacy of the three different stimulation approaches, no control condition (i.e. sham stimulation) was included. Sample sizes were estimated based on another study 13 and increased to compensate for attrition. Prior to data collection, a member of the laboratory staff who was not otherwise involved with the study performed the randomization using a computer-based random number generator and prepared sealed envelopes. This investigator allocated participants to the intervention upon notification of completion of informed consent. Stimulation conditions were separated by one week to reduce the possibility of carryover effects.
Study procedures are illustrated in Figure 1. During each session, corticomotor and performance outcome measures were collected three times. The testing order was constant for all participants and conditions, and was as follows: pinch strength, motor evoked potential threshold and amplitude, Nine-hole Peg Test, and visuomotor tracking task. Participants began with the pretest measurements, which were followed by 30 minutes of functional task practice concurrently with stimulation. Training was supervised by a study investigator (JGO). Tasks were selected from previously published functional task practice training protocols4–6 (see Appendix for details, available online).
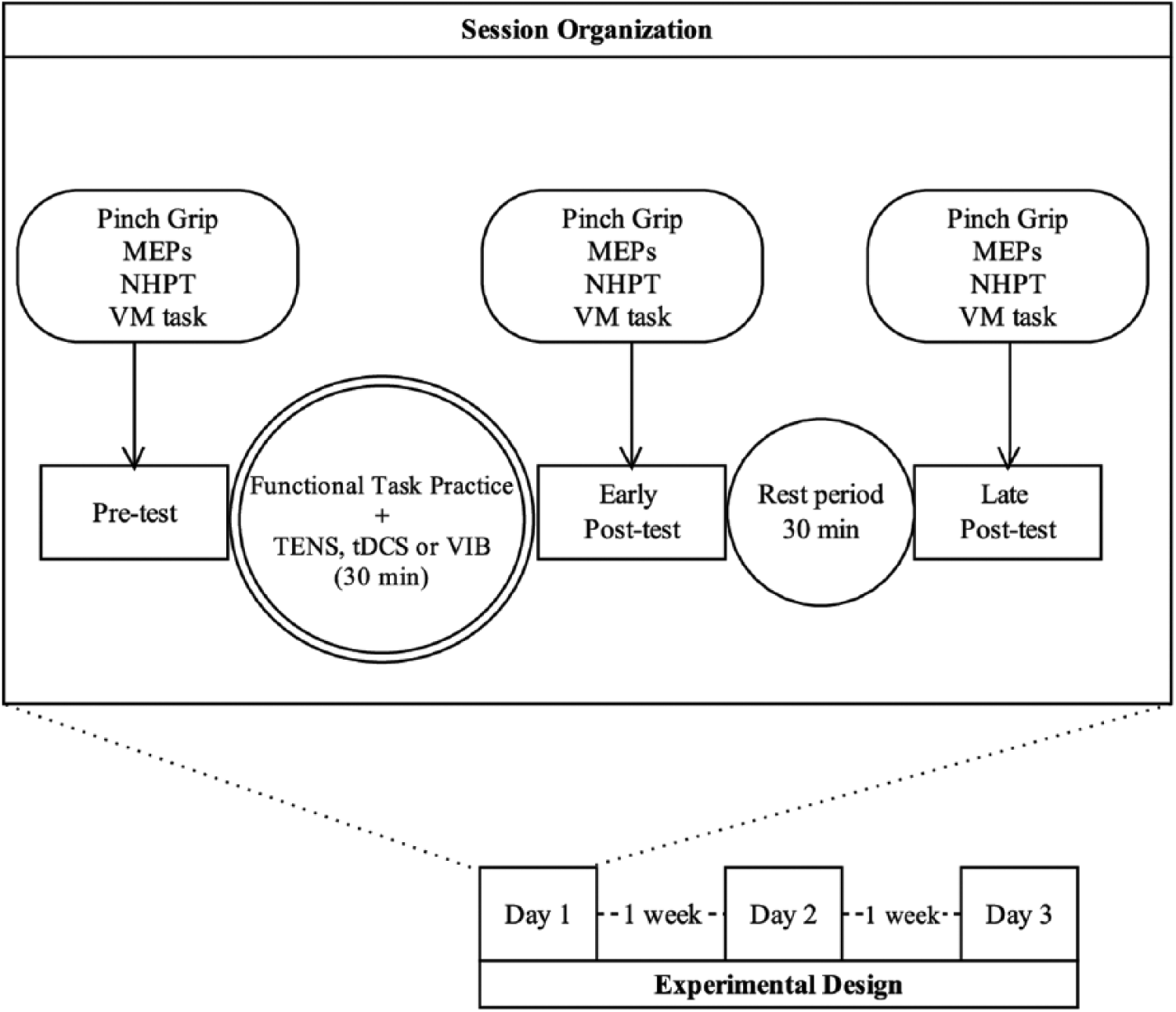
Experimental setup. Participants completed a total three of sessions, one week apart. Measurements of pinch force, cortical excitability (amplitude of motor evoked potential), fine motor performance (Nine-hole Peg Test), and visuomotor tracking at pretest, following 30 minutes of functional task practice with either transcutaneous electrical nerve stimulation, transcranial direct current stimulation, or vibration (early posttest) and after a 30 minute rest period (late posttest).
The investigator conducting the assessment was not blinded to the order of the interventions. Following this stimulation/practice period, participants performed the early posttest measurements, rested for 30 minutes, and then performed the late posttest measurements. Early effects were assessed through changes from pre-intervention (pretest) to postintervention (posttest), and short-term persistence were assessed through changes from pre-intervention to 30 minutes after the end the posttest (late posttest). Testing and training was targeted at the weaker hand, determined by self-report.
Transcutaneous electrical nerve stimulation was delivered to the volar aspect of the wrist overlying the median nerve utilizing a clinically available portable electrical stimulation unit (TENS 7000, Koalaty Products, Inc., USA) with the following parameters: biphasic symmetrical rectangular pulse wave at 100 Hz, 250 μs pulse width. The optimal site for activation of the median nerve was determined by moving the electrodes to identify the area wherein participants reported the stimulation was best perceived in digits I–III. Intensity was increased until the motor threshold was determined, and then set at a level where sensation was described verbally as “strong” and equivalent to at least 5–6/10 described using a verbal analogue scale in the absence of pain or muscle contractions assessed via visual inspection. 5
The optimal stimulation site for the corticomotor area controlling the weaker hand was identified using transcranial magnetic stimulation (Magstim200, Dyfed, Wales), detailed methods have been previously described elsewhere. 14 When it was not possible to obtain motor-evoked potentials from the thenar muscles, we used the 10–20 electroencephalographic system for electrode placement. Transcranial direct current stimulation was delivered by a direct current stimulator (Phoresor, Iomed Inc., Salt Lake City, UT) with intensity set at 1 mA, according to safety guidelines. 15 Two electrodes (Optima, Iomed Inc., Salt Lake City, UT) were used: the anode was a saline-soaked disposable iontophoresis electrode (with 28 cm2 area), and was placed on the scalp overlying the hotspot of the primary motor area (or alternatively on area C3 or C4), which correspond to the left or right primary motor areas, respectively; and the cathode was an adhesive electrode (with approximately 37 cm2 area), which was placed on the contralateral supraorbital area. The estimated current density was approximately 46 μA/cm2.
For the vibration condition, the vibration device (CEN, USA) was placed on the volar aspect of the distal wrist over the distal tendon of the flexor carpi radialis using elastic wrap and adhesive tape. We standardized the amplitude of vibration by attaching the device so that it made optimum contact without causing discomfort or altering wrist range of motion that could interfere with the repetitive task practice activities. Vibratory stimulus (80 Hz, continuous) was delivered on the first 10 minutes of the functional task practice training. 7
Changes in pinch strength for each phase were measured using a handheld dynamometer (Microfet4; Hoggan Health Industries, UT). Participants remained seated in their wheelchairs with the shoulder in a neutral position, elbow at 90° flexion, and the forearm rested on a table. The average force produced in three maximal voluntary contractions was recorded.
Change in the Nine-hole Peg Test was the primary outcome measure aimed at assessing fine motor control. For each session, a video record was made of the task performance, which included three trials of 30 seconds per phase. Participants were instructed to pick up pegs as quickly and accurately as possible and place them in the holes until filled, and without pausing, continue placing them back into the bowl using the weaker hand. 16 The scoring was performed based on the video recording, by an assistant not otherwise involved in the study, who timed each trial, counted the number of pegs successfully placed and removed, and calculated an average.
The main software interface of the visuomotor tracking task was a sinusoidal waveform that participants were encouraged to track as accurately as possible by controlling the force of their pinch grasp. The peak and valley of the target wave were calibrated to 10% and 20% of each individual’s maximum pinch force. Visual feedback of the desired trace and the actual trace were both available to the participants. Two familiarization trials were performed, and the following three trials (30 seconds each) were used for the analysis. The scoring was performed according to another study that utilized a visuomotor tracking task 17 (see Appendix, available online, for further details).
Corticomotor excitability was assessed with transcranial magnetic stimulation, delivered using a figure of eight coil (maximum field intensity 2 Tesla; Magstim Rapid 2, Magstim Co, UK) placed tangential to the scalp and in a postero-lateral direction in an angle of 45° with the mid-sagital line. Motor-evoked potentials were recorded via surface electromyography of the thenar muscle of the weaker hand while the subject maintained 10%–15% of their maximum voluntary contraction (active motor evoked potentials). 18 Two Ag Ag/Cl electrodes (3.2 × 2.2 cm2) were used: one electrode was placed at the distal one-third of the thenar eminence and the other electrode was placed 2 cm caudally; the ground electrode was placed on the styloid process of the ulna. The transcranial magnetic stimulation coil was placed on the hemisphere contralateral to the weaker hand with initial intensity set at 50% maximum stimulator output, and the site corresponding to the hand motor area was sought and recorded, as was reported in an earlier study. 11
Two computers were used during the data acquisition: One computer was used to store data for off-line analysis (Signal version 5.0, CED, UK), and another for biofeedback display (Spike, CED, UK). For the data acquisition, the electromyography signal was amplified (×1000), band-pass filtered (10–2 kHz; Grass model P511AC, Grass-Telefactor, USA), and converted from analogue to digital (CED model 1401; CED, UK) at a sampling rate of 2 kHz. Electromyography activity was captured 20 ms prior to and following the stimulation artifact (20 millisecond period in each case), in order to capture both baseline and poststimulus activity.
Motor threshold (MT) was defined as the stimulation intensity wherein it was possible to obtain 5–7/10 responses having a peak-to-peak amplitude greater than 50 µV above baseline during a minimal voluntary contraction. 18 Following motor threshold determination, ten responses were recorded with intensity set at 1.2 times the motor threshold (i.e. 20% higher than the motor threshold intensity). The amplitude of 10 averaged motor-evoked potentials at 1.2 times the motor threshold was used to assess corticomotor excitability. Motor-evoked potential amplitude data was normalized as a proportion of the participants’ maximum median nerve M-wave (i.e. maximum response evoked from the muscle with electrical stimulation). To assess M-wave amplitude, electrodes were placed in the cubital fossa with the cathode positioned caudal to the anode. Single pulses of 1000 μsec pulse duration were applied in increasing intensities until no further increases in amplitude of the response was observed.
Statistical testing was performed using SAS software (version 9.3, SAS Institute Inc., Cary, NC) and built-in functions in Excel 2010 (Microsoft Corporation, USA). Descriptive statistics including means, standard deviations, and 95% confidence intervals (CI) were calculated for the differences in pretest vs. early posttest and for pretest vs. late posttest for all measures. Preliminary analyses were carried out to assess order effects. 19 For this purpose, independent t-tests on the sum of group means for subjects who received all different combinations of orders involving the three conditions (transcranial direct current stimulation, vibration, and transcutaneous electrical nerve stimulation) were compared. No order effects were identified for the Nine-hole Peg Test, pinch force, or visuomotor tracking task (p > 0.05 for all comparisons), and therefore it was appropriate to treat conditions separately in the analysis.
Our hypothesis testing focused on within-condition comparisons of single-session functional task practice combined with stimulation. A general linear mixed model was used to analyze the data from this 3 × 3 within-subjects trial. The model included fixed effects for condition (three levels), time (three levels), and the interaction of condition and time. An unstructured covariance matrix was used to represent the correlated data structure. Planned comparisons were made among times within each condition. Analyses wherein p ≤ 0.05 were considered to have achieved statistical significance.
Owing to the small proportion of participants from whom it was possible obtain motor-evoked potential (MEP) measurements (transcutaneous electrical nerve stimulation = 11; vibration = 9, transcranial direct current stimulation = 7), we used paired t-tests to assess changes in corticomotor activity from pretest to posttest (early effects) and from pretest to late posttest (short-term persistence). These changes are of clinical interest, as they enable the assessment of early changes in cortical excitability and short-term retention of these changes. Because the hypotheses were prespecified, no adjustments were made to the p-values (Bonferroni correction), as reported per Perneger. 20
The magnitude of effect sizes was calculated for all outcome measures. The Cohen’s d21 were computed by dividing the change from pretest to early posttest (early effects) or from pretest to late posttest assessment (short-term persistence) by the standard deviation of the pretest values. Effect sizes were interpreted based on published values: <0.2 trivial effect, 0.2–0.5 small effect, 0.5–0.8 moderate effect, >0.8 large effect. 21
Results
A total of 24 participants completed the study (three females, mean age 43.7 ±10.8). Three subjects did not complete all sessions, and were lost to follow-up. One individual participated in the training, but was not able to perform any of the outcome measures; this participant was treated as an outlier and was excluded from the overall analysis. A total of 20 individuals completed all stimulation and assessment sessions and did not report adverse effects. Demographic information is given in Table 1.
Demographic characteristics of the participants included in the study.
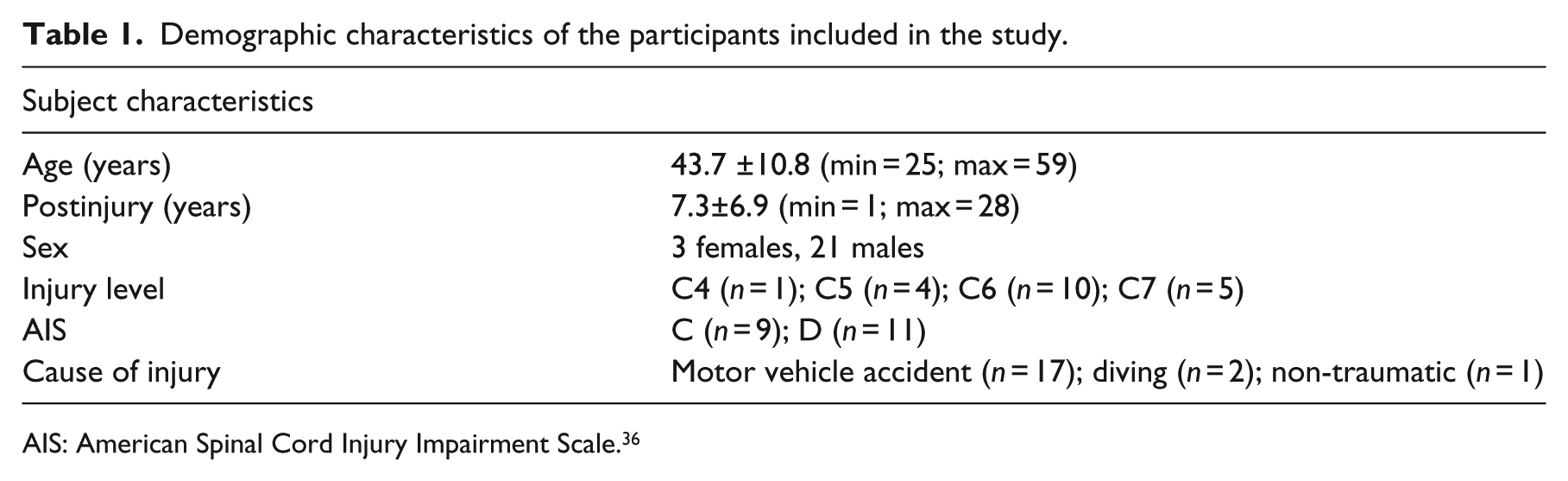
AIS: American Spinal Cord Injury Impairment Scale. 36
Scores for all performance measures at pretest are presented in Table 2. No differences were detected in baseline values for all outcome measures in the three conditions. Early effects (posttest vs. pretest) and short-term persistence (late posttest vs. pretest) for performance measures for all conditions are illustrated in Table 3.
Descriptive statistics of performance measures at pretest.
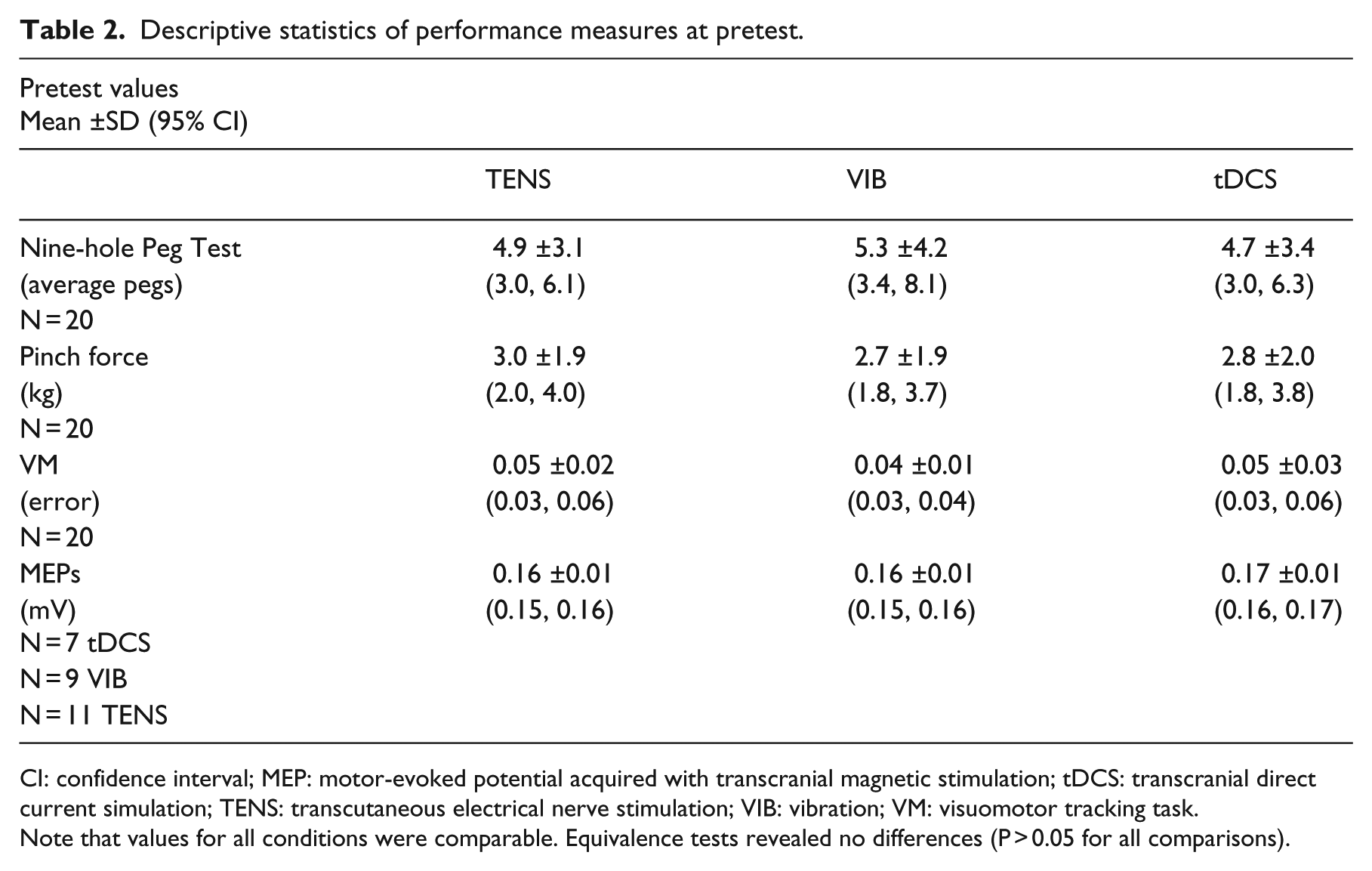
CI: confidence interval; MEP: motor-evoked potential acquired with transcranial magnetic stimulation; tDCS: transcranial direct current simulation; TENS: transcutaneous electrical nerve stimulation; VIB: vibration; VM: visuomotor tracking task.
Note that values for all conditions were comparable. Equivalence tests revealed no differences (P > 0.05 for all comparisons).
Descriptive statistics and results for analysis of variance for each performance.
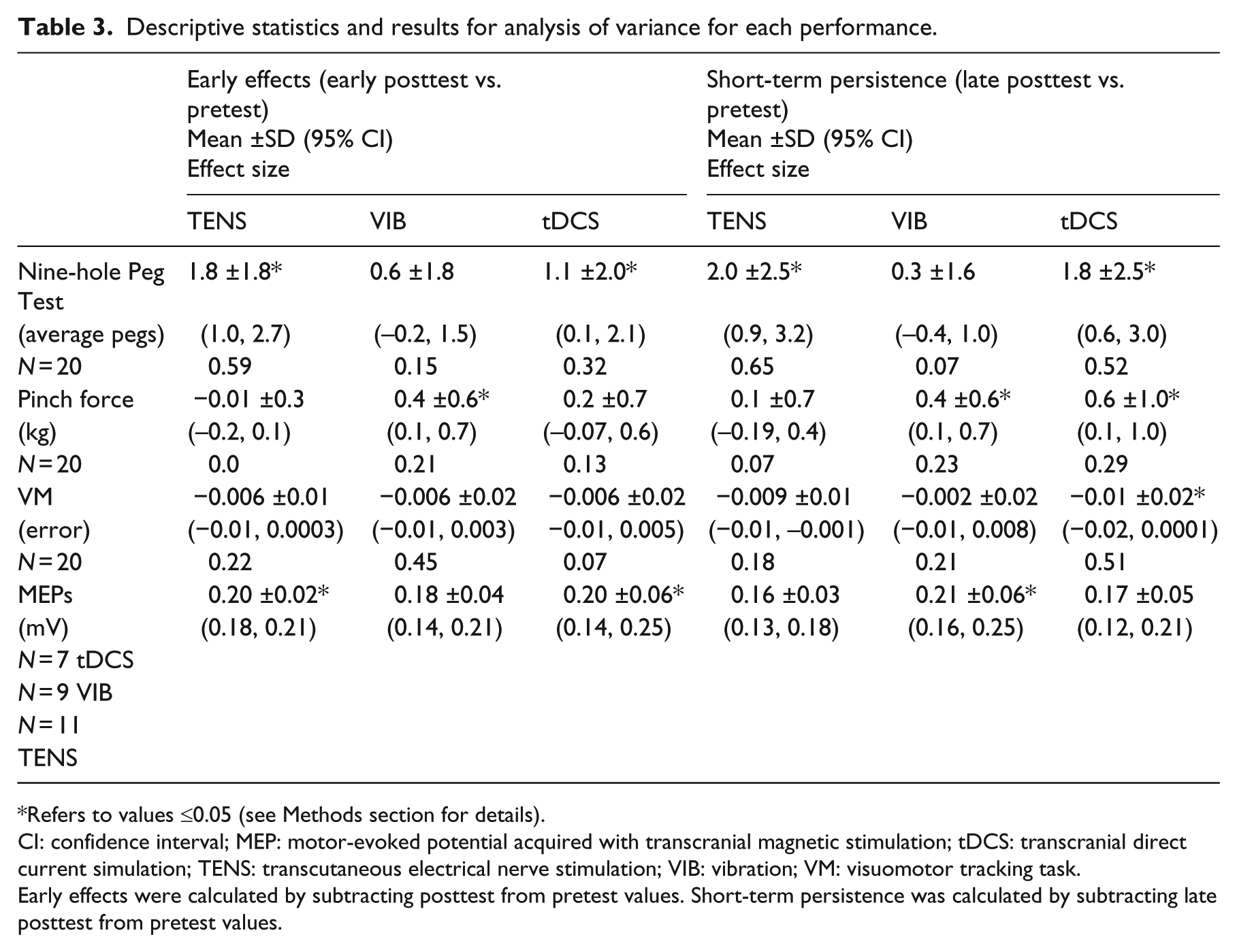
Refers to values ≤0.05 (see Methods section for details).
CI: confidence interval; MEP: motor-evoked potential acquired with transcranial magnetic stimulation; tDCS: transcranial direct current simulation; TENS: transcutaneous electrical nerve stimulation; VIB: vibration; VM: visuomotor tracking task.
Early effects were calculated by subtracting posttest from pretest values. Short-term persistence was calculated by subtracting late posttest from pretest values.
Early effects on the number of pegs transferred during the Nine-hole Peg Test were significant for transcutaneous electrical nerve stimulation with a moderate effect size (p = 0.003, d = 0.59). Transcranial direct current stimulation was also associated with significant early effects, but the effect size was small (p = 0.05, d = 0.32). There was no early effect on the Nine-hole Peg Test performance associated with vibration (p = 0.27). Short-term persistence followed a similar pattern, characterized by significant increases in the Nine-hole Peg Test performance for transcutaneous electrical nerve stimulation and transcranial direct current stimulation, with moderate effect sizes for both conditions (p < 0.001, d = 0.65 and p = 0.003, d = 0.52, respectively). Short-term persistence of vibration was not significant (p = 0.17).
Early effects of vibration were characterized by a significant improvement in pinch force, but the effect size was small (p = 0.03, d = 0.21). Neither transcutaneous electrical nerve stimulation nor transcranial direct current stimulation had a significant early effect on pinch force. Short-term persistence of transcranial direct current stimulation and vibration were associated with significant increases in pinch force, but effect sizes were small (p = 0.005, d = 0.29 and p = 0.03, d = 0.23, respectively). Transcutaneous electrical nerve stimulation was not associated with significant short-term persistence.
Early effects for visuomotor tracking were not significant for any of the stimulus types. Short-term persistence of transcranial direct current stimulation were associated with a significant improvement in visuomotor tracking that had a moderate effect size (p = 0.05, d = 0.51). Short-term persistence of transcutaneous electrical nerve stimulation and vibration were not significant.
Two participants could not tolerate the procedure for determining the maximum motor response (M-max), which was intended to normalize the MEP to differences in neuromuscular properties. In addition, we believe that by using electromyographic biofeedback and monitoring to ensure that pulses were given only when participants were at their “target” level (10%–15% maximum voluntary contraction) ensured a consistent level of baseline excitability. Therefore, we report the non-normalized MEP amplitudes, which were available for all participants (Table 3 and supplementary Figure 1, available in the Appendix online).
Changes in corticomotor excitability in the different stimulus conditions were characterized by different patterns (Table 3). Significant early effects on corticomotor excitability were observed after transcutaneous electrical nerve stimulation (p = 0.003), and early effects approached significance after transcranial direct current stimulation (p = 0.07). Vibration was not associated with an early modulation in corticomor excitability (p = 0.6). At the late posttest assessment, corticomotor excitability returned to pretest levels in the transcutaneous electrical nerve stimulation and transcranial direct current stimulation condition (p = 0.8 and p = 0.9, respectively), but was significantly increased in the vibration condition (p = 0.006).
Discussion
In this proof-of-concept study, we assessed the influence of three forms of clinically available stimulation (transcutaneous electrical nerve stimulation, transcranial direct current stimulation, and vibration) delivered in combination with functional task practice training in persons with chronic tetraplegia. We found that transcranial direct current stimulation was associated with beneficial effects on the ability to successfully manipulate small objects (Nine-hole Peg Test) and modulate pinch contraction forces (visuomotor task) that were of moderate size and persisted at least 30 minutes following the intervention (i.e. short-term persistence). Transcutaneous electrical nerve stimulation was also associated with short-term persistence of moderate size on the improvement in the Nine-hole Peg Test performance. The effects of vibration and transcranial direct current stimulation on the ability to generate pinch force were associated with a small effect size and thus, are of less clinical value. Because the main objective of the present study is to identify clinically meaningful, persistent effects that are relevant for future studies aimed at augmenting training effects with stimulation, this discussion will focus on those effects that persisted for at least 30 minutes following the intervention (i.e. short-term persistence) and had at least a moderate effect size.
In persons with tetraplegia, functional task practice combined with peripherally applied, electrical stimulation consisting of long pulse durations is associated with improvements in hand function and increased cortical excitability.4,6 Our results suggest that transcutaneous electrical nerve stimulation, an inexpensive stimulation approach that is easily available to most physical therapists and patients, may be also be of value to improve fine motor function. The similarity between the effects of transcutaneous electrical nerve stimulation (short pulse duration) and somatosensory electrical stimulation used in prior studies4,6 (long pulse duration) suggests that pulse duration of peripherally applied electrical stimulation may not be a critical variable when the goal is to promote cortical excitability with the objective of improving hand function. This argument is consistent with evidence supporting that these two approaches activate the same large diameter afferents22,23 that can in turn excite the primary motor cortex via cortico–cortico connections between the primary somatosensory cortex and the primary motor cortex. 24
The use of transcranial direct current stimulation aimed at improving arm and hand function after spinal cord injury has not been previously evaluated, but two systematic reviews25,26 in individuals with chronic stroke found the pooled effect sizes for the effect of transcranial direct current stimulation on fine motor performance to be in a similar range (standard mean difference; SMD: 0.4025 and 0.3926) as was found in the present study (d = 0.52). While the etiology of hand deficits after stroke and spinal cord injury are distinct, evidence suggests that these two clinical populations share similarities in that they exhibit reduced corticomotor excitability post-injury 3 and have been shown to exhibit a similar degree of improvement when participating in interventions consisting of motor training and stimulation. 11 The similarity between the effect sizes in previous studies in individuals with stroke and the effect size associated with the improvement in Nine-hole Peg Test performance found in the present study is evidence that transcranial direct current stimulation may be of value to augment the effects of training aimed at improving hand function in individuals with chronic tetraplegia. In addition, the similarity between the short-term persistence of transcutaneous electrical nerve stimulation (an approach for indirect cortical activation) and transcranial direct current stimulation (direct brain stimulation) on Nine-hole Peg Test performance in the present study seems to indicate that both direct and indirect approaches to increase corticomotor activation may be of value as adjuncts to functional task practice for the improvement of arm and hand function.
Transcranial direct current stimulation was the only form of stimulation that was associated with short-term persistence on the improvement in visuomotor tracking (Cohen’s d = 0.51). Improvements in the accuracy of visuomotor tracking following transcranial direct current stimulation have been previously demonstrated27,28 using a different task that that employs a joystick, but follows the same general goal of tracking the position of a changing visual stimulus on a computer screen in real time. Earlier studies have characterized the short-term persistence of transcranial direct current stimulation, showing that effects persist for up to one hour following 9–13 minutes of transcranial direct current stimulation,29–31 and are dependent on N-methyl-D-aspartate (NMDA) receptor activation as they can be abolished by administering dextromethorphane, a known NMDA receptor antagonist. 32 It is possible that transcranial direct current stimulation may be associated with a greater enhancement of NMDA receptor efficacy because it is a more direct approach to primary motor cortex activation, which would result in greater improvement on a task more specifically controlled by primary motor cortex (such as modulating small forces (10%–20% maximum voluntary contraction) using pinch grip).
While we had limited data for the cortical excitability measure, the time course of corticomotor activity appeared to be different between the three conditions. Transcutaneous electrical nerve stimulation and transcranial direct current stimulation were associated with early effects on corticomotor excitability in the absence of short-term persistence. Alternatively, vibration was associated with short-term persistence on corticomotor excitability in the absence of early effects. Given that the dose of vibration (10 minutes) was smaller than the transcutaneous electrical nerve stimulation and transcranial direct current stimulation (both administered for 30 minutes), it is likely that the lack of excitability increase at posttest could be owing to a difference in dose. Another possible explanation is that vibration of the distal tendon of the flexor carpi radialis could have been insufficient to stimulate the thenar muscles, which is consistent with the evidence, demonstrating that the increased corticomotor excitability following vibration is specific to the vibrated muscle. 33
This study has limitations. The lack of a control condition of functional task practice alone means that we are not able to assess the effects of functional task practice in the absence of stimulation. However, the finding that effects associated with vibration were minimal, despite being combined with 30 minutes of functional task practice, supports our conclusion that the outcomes with transcranial direct current stimulation and transcutaneous electrical nerve stimulation were not primarily owing to the functional task practice. While we realize that the vibration dose was lower than the other stimulation techniques and the vibration amplitude was not directly measured, our interest was to assess the most promising parameters that could be translated into direct clinical application. Our decision was based on data from our laboratory34,35 and others7,33 demonstrating that brief periods of vibration, ranging from 3 minutes to 15 minutes (continuously) can be associated with short-term persistence that can influence the nervous system. In addition, pilot data suggested limited application would be safer.
Clinical messages
Adding transcutaneous electrical nerve stimulation to functional task practice resulted in improved fine hand motor performance.
Adding transcranial direct current stimulation to functional task practice resulted in improved fine hand motor performance, pinch strength, and visuomotor tracking.
The addition of a single session of vibration to functional task practice did not influence arm and hand function.
Footnotes
Acknowledgements
The author(s) would like to thank Dr Jorge Bohorquez and Daniel Gonzalez for designing and building the visuomotor tracking task. In addition, the authors would like to thank Rachel Monahan for her assistance in the data collection and analysis.
Conflict of interest
The author(s) declare that there is no conflict of interest.
Funding
This work was funded by National Institutes of Health R01HD53854.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.