
Abstract
Objective:
To assess the effectiveness of a six week cognitive–behavioural group intervention in patients with knee osteoarthritis pain.
Design:
Single-blinded randomized controlled trial.
Study setting:
Primary care providers in a medium-sized city in Finland.
Patients:
A total of 111 participants aged from 35 to 75 with clinical symptoms and radiographic grading (Kellgren-Lawrence 2–4) of knee osteoarthritis were included.
Interventions:
In the intervention group, 55 participants attended a cognitive–behavioural training programme for pain management with six weekly group sessions supervised by a psychologist and a physiotherapist. Concurrently, they and the 56 participants of the control group continued in ordinary GP care that was not altered by the study.
Main measures:
The primary outcome on three-month and 12-month follow-up was the Western Ontario and McMaster Universities (WOMAC) Osteoarthritis index pain subscale. Secondary outcome measures included self-reports of pain and physical function, health-related quality of life, and a comprehensive set of psychological questionnaires.
Results:
Mixed model results showed no significant differences between the intervention and control group for any measures of pain or function. A significant difference between the groups was found in the Pain Self-Efficacy Questionnaire (Pr = 0.022) in favour of the control group, and in the RAND-36 emotional well-being subscale in favour of the intervention group (Pr = 0.038). Conventional group comparisons of mean follow-up values showed no significant differences in any of the outcome variables.
Conclusion:
This trial could not confirm the hypothesized advantage of a cognitive–behavioural training programme over ordinary GP care in knee osteoarthritis pain patients.
Trial registration:
Current Controlled Trials ISRCTN64794760
Introduction
Knee osteoarthritis is a common chronic condition causing disabling symptoms, such as joint pain, physical and psychological dysfunction, and reduced quality of life.1,2 Psychological distress, including depression or depressed mood, or anxiety has been associated with higher levels of pain in osteoarthritis patients.3,4 Moreover, pain catastrophizing 5 and social isolation 4 have predicted higher levels of pain in osteoarthritis patients, and poor coping strategies 6 have predicted higher levels of both pain and dysfunction.
Since psychological factors play a role in the experience of osteoarthritis pain, interventions targeted at improving them should be studied. In degenerative musculoskeletal disorders, such as chronic low-back and neck pain, the effectiveness of behavioural and cognitive–behavioural treatment modalities has been somewhat modest.7,8 Different cognitive–behavioural models have been studied alone and in combination with other interventions in knee osteoarthritis patients. However, the number of randomized controlled trials (RCTs) so far conducted in this field is relatively small and the results have been somewhat contradictory. Calfas et al. conducted an RCT testing a 10-week group-based cognitive–behavioural programme for osteoarthritis patients. 9 They concluded that 12 months after the intervention, physical and psychological functioning did not differ between the cognitive–behavioural and the education control group. Keefe et al., using another cognitive–behavioural approach known as pain-coping skills training, reported that pain and physical function were improved in knee osteoarthritis patients in the short term (12 weeks), but the effect appeared to diminish over time. 10 Riddle et al. found that, in patients scheduled for knee arthroplasty, the pain-coping skills training programme resulted in significantly greater reductions in pain severity and catastrophizing, and greater improvements in function, when compared with the usual care cohort in the short term (two months). 11 Somers et al. reported the results of a four-arm RCT examining the effects of a pain-coping skills training programme, a behavioural weight management intervention, and their combination 12 in obese osteoarthritis patients. They concluded that participants randomized to receive both of these treatments showed improvements in pain, physical disability, psychological disability, and weight 12 months after the end of the intervention when compared with the other groups. Recently, Broderick et al. published the results of an RCT studying the effectiveness of a pain-coping skills training programme delivered by nurse practitioners compared with usual care in knee and hip osteoarthritis patients. 13 Their analyses indicated significant improvement for the intervention group compared with the control group for pain intensity, physical functioning, psychological distress, use of pain-coping strategies, and self-efficacy, as well as fatigue, satisfaction with health, and reduced use of pain medication. All outcomes, except for self-efficacy, were maintained through the 12-month follow-up.
The purpose of present study was to explore, in an RCT setting, the effectiveness a sole cognitive–behavioural intervention on knee osteoarthritis pain patients not scheduled for surgery. Our aim was to test an intervention that would be ready-to-use and not too laborious to put into practice for this wide group of patients mostly treated by health personnel in the primary care. For these reasons we chose the manualized six-session cognitive–behavioural group intervention described by Linton, 14 modified for patients with knee osteoarthritis. The model was originally developed for early identification and intervention in the prevention of persistent musculoskeletal pain.15,16 The model has previously been tested in RCT settings in patients with back and neck pain.15,16 In these studies, the cognitive–behavioural intervention led to less short- and long-term work absenteeism, fewer healthcare visits, decreased perceived risk and fear-avoidance beliefs, and a larger number of pain-free days. We hypothesized that participants with symptomatic knee osteoarthritis would benefit from this type of cognitive–behavioural rehabilitation programme. More specifically, we examined the effect of the intervention during a one-year follow-up in terms of self-reported pain and physical function, health-related quality of life, work abstinence, and the use of pain medication and healthcare services. We also measured the effect of the intervention on the psychological variables of resources and coping, fear and catastrophizing, and distress.
Patients and methods
We performed a prospective, randomized, single-blinded, primary healthcare trial among knee osteoarthritis patients with pain symptoms and no previous or planned arthroplasty. We compared the effectiveness of a six week cognitive–behavioural group intervention model presented by Linton 14 with a control group. Throughout the study, all participants received ordinary GP care that was not intervened in any way. The trial protocol has previously been published 17 (available at: http://www.biomedcentral.com/1471-2474/14/46), and the trial was registered with Current Controlled Trials (ISRCTN64794760).
Eligibility and randomization
Patients aged between 35 and 75 years with clinical symptoms and radiographic grading (Kellgren–Lawrence 2–4) 18 of knee osteoarthritis were eligible. All patients had experienced pain within the last year in or around the knee occurring on most days for at least a month. 19 One week prior to the study, their knee pain was rated as ≥40 on a 100-mm visual analogue scale in the pain subscale of the Western Ontario and McMaster Universities (WOMAC) Osteoarthritis index. 20 Exclusion criteria encompassed severe psychiatric or psychological disorders that had led to hospitalization or an inability to work, previous or planned lower extremity joint surgery, and other back or lower limb pain symptoms that had been more aggravating than the knee pain. Before inclusion, the participants also had to declare that they were able to attend six intervention sessions and presumably complete the study.
The patients were randomly assigned to either the GP care and intervention group or the GP care control group. Randomization was conducted in blocks of six, separately for men and women. A computer-generated code for randomization was constructed by a collaborator who did not meet the study patients, and it was administered via sequentially numbered sealed opaque envelopes. The study doctors responsible for enrolling the patients, distributing the envelopes for randomization, collecting the data, and performing the statistical analysis were blinded to the group assignment and were not involved in providing the interventions. The code for randomization was opened only after the statistical analyses had been performed after the 12-month follow-up point.
Intervention
Patients allocated to the cognitive–behavioural group intervention took part in six weekly sessions supervised by an experienced psychologist and a physiotherapist. The sessions took place in a group of 7−13 persons according to the model presented by Linton. 14 Each session lasted for two hours with a 15−20 minute break to enhance peer support and social bonding. The outline of the sessions included an introduction (15 minutes), lecture (knowledge and insight, max 15 minutes), problem solving (in pairs/teams, 15−20 minutes), skills training (15−20 minutes), homework assignments (15 minutes), and a résumé (feedback) of the session (15 minutes). A written example of a knee osteoarthritis pain patient’s life was used throughout the intervention as a basis for discussion and practice in problem solving. An outline of each session is presented elsewhere. 17 The psychologist was the principal leader of the cognitive–behavioural intervention. The physiotherapist’s tasks were to lead the relaxation exercises, provide the information on osteoarthritis pain mechanisms in the first session, offer advice about suitable exercises in the second session, and facilitate the group in general when needed. Both the intervention and the control group continued side by side with the usual GP care that patients might have received in primary care throughout the study.
Outcomes
The primary outcome measure of the study was the WOMAC self-reported pain subscale. We used the Finnish version of WOMAC that has been found valid and reliable. 20 The primary outcome score was measured at baseline, and at three- and 12-month follow-up points. We used postal questionnaires for collecting the outcome data at every assessment point. The study doctors responsible for the collection were blinded to the group assignment.
Secondary outcomes were assessed at baseline and at three- and 12-month follow-up points, apart from the global assessment of change, which was only assessed at the follow-up points. In the postal questionnaires we also inquired about smoking habits, alcohol consumption, exercising, the work situation, and major life events at every assessment point. Furthermore, at baseline, there were questions about demographic characteristics and the patients were asked to complete the Örebro Musculoskeletal Pain Questionnaire 21 to identify those at risk of persistent pain.
Secondary outcome measures included other measures of pain including numeric pain rating scales (0–10) of the worst and mean pain during the previous week and past three months. Physical functioning and stiffness were measured with corresponding subscales of the WOMAC. Health-related quality of life was measured with the RAND-36 22 and 15D. 23
The use of analgesics (paracetamol and opioids) and nonsteroidal anti-inflammatory drugs (NSAIDs), as well as topical pain medication (NSAID and others) for the treatment of knee osteoarthritis pain was assessed based on the patients’ reports. The participants were provided the following response alternatives: 0 = not using; 1 = using a couple of days a month or less; 2 = using a couple of days a week; 3 = using daily. Participants were also asked about intra-articular injections (cortisone and hyaluronate) to the knee in the six months before and during the study. The use of health services was asked about in the following way: the number of doctor appointments (1) related and (2) not related to knee osteoarthritis, and (3) the number of physiotherapist appointments related to knee osteoarthritis. Furthermore, the patients were asked about the number of sick leave days in the previous 3−6 months at each assessment point.
Secondary outcome measures also included questionnaires of life satisfaction, sense of coherence, pain self-efficacy, kinesiophobia, and pain catastrophizing. Life satisfaction was measured with a four-item Life Satisfaction scale that has been found strongly associated with self-rated health, as well as objectively assessed physical health. 23 Sense of Coherence was evaluated by the well-validated 13-item version of Sense of Coherence 24 scale. Pain self-efficacy was assessed by the Finnish version of the Pain Self-Efficacy Questionnaire 25 and kinesiophobia by the Finnish version of the Tampa scale of kinesiophobia. 26 Pain catastrophizing was evaluated by the Pain Catastrophizing Scale. 27 Although widely used in experimental and clinical studies, there are currently no published validation studies or reliability data on the Finnish Pain Catastrophizing Scale.
Depressive symptoms were assessed by the Finnish version of the 21-item Beck Depression Inventory that has been found valid and reliable. 28 The Beck Anxiety Inventory 29 was used to evaluate the severity of symptoms of anxiety. The Finnish version of the inventory has been used in some studies, but exact data on validity and reliability are scarce.
Global assessment of change was measured with the question ‘Compared with the beginning of the study, how have your knee osteoarthritis symptoms changed?’ The response was recorded using a 15-point Likert scale ranging from ‘worsened exceedingly’ (−7) to ‘no change’ (0) and ‘became exceedingly better’ (+7).
Sample size
The mean (±SD) knee joint pain score (WOMAC, visual analogue scale) was estimated by using the results of the knee joint pain scores in previous studies.30,31 Since the knee pain had to be ≥40 mm on a 100-mm visual analogue scale (WOMAC) in this study, we postulated that there would be a mean of at least 48 ±16.2 mm in the WOMAC pain subscale at baseline. In our study, a 20% reduction in the primary outcome (WOMAC pain) owing to the intervention was considered as being clinically relevant in accordance with the Outcome Measures in Rheumatology – The Osteoarthritis Research Society International (OMERACT-OARSI) set of responder criteria. 32 In the comparison of the mean pain scores between the groups, 54 patients per group were needed according to a power calculation with the two-tailed Student’s t-test, with a 5% significance level and 80% power, and assuming a 20% drop-out rate.
Statistical analysis
All statistical analyses were performed using SPSS (version 19.0, SPSS, Chicago, IL, USA).
Demographic characteristics and baseline data were summarized by descriptive statistics. Posttreatment (follow-up) average values were calculated for each outcome. Differences between groups were analysed for continuous variables with the two-tailed Student’s t-test and for non-parametric variables with the Mann–Whitney U-test. Standard diagnostic plots were used to check model assumptions.
All analyses adhered to the intent-to-treat principle. The primary analysis was carried out using the linear mixed model, and separate models were estimated for each outcome. The mixed model has the advantage of using all available data in the analysis, irrespective of whether some data points are missing for a given participant. The follow-up measurement (measures of the outcome from the three-month to the 12-month measurement point) was the response variable and is referred to as the posttreatment level. Modelling both posttreatment measurement occasions in this manner allowed us to understand the course of the outcomes over the entire year of follow-up and enabled the mixed model to preserve the cases that had one or more missing data points during the follow-up.
We decided to perform the mixed model analysis according to the statistical analysis of an RCT by Somers et al., 12 who assessed the impact of a pain coping skills training and behavioural weight management in obese osteoarthritis patients. In the model, the predictor side included the baseline level of the corresponding outcome variable, treatment group, age, gender, disease severity, time, and the treatment-by-time interaction. It has been recommended that covariates should be chosen based on their substantive basis and not on a test of differences. 33 Thus age, gender, and disease severity were included in all models based on their associations with the study outcomes in prior research.5,34 In comparison to the study by Somers et al., race was not included in our model, since all our study patients were of Caucasian origin. The inclusion of covariates in a randomized trial improves the precision of the treatment estimates and improves the power of the tests of the treatment effect. 33 Thus, a model was fitted of the form:
In addition to improving the precision of the treatment effect estimates, using the baseline level of the outcome as an adjustment covariate also has important implications for which model terms are of most interest. In the case of a conventional repeated measures analysis of variance, where the baseline measure is included on the response side of the model, the effect of primary interest is the time-by-treatment interaction term. In contrast, the term of primary interest in the present model was the main effect of treatment, which was interpreted as the effect of treatment averaged over the posttreatment period from three to 12 months.
Of secondary interest was the time-by-treatment interaction, which addressed the question of whether the groups differed in the change between the second and third measurement points. A non-significant time-by-treatment interaction suggests that the changes over the posttreatment follow-up period cannot be distinguished from sampling error. If interaction terms were not statistically significant, they were removed from the model and the model was re-estimated with only the main effects terms. Since all but one of the outcomes showed non-significant differences between the groups, even when the time-by-treatment interaction was removed, we decided to report mixed model results according to the model showing the smallest Pr value.
Results
Between August 2011 and September 2012, 111 patients with knee osteoarthritis pain were included in the study. Patients were recruited from primary care providers in the Kuopio (105,000 inhabitants) area of eastern Finland. The majority of participants (77%, n = 86) were enrolled in the study after replying to a recruitment letter sent to those who had had Kellgren–Lawrence grade ≥2 osteoarthritis changes in knee X-rays taken at most 5 years prior the study in primary healthcare. The rest of the participants (23%, n = 25) had contacted the study doctors by phone as instructed in study advertisements placed in the facilities of local primary care providers, as well as the outpatient clinics of the Departments of Orthopaedics, and Physical and Rehabilitation Medicine at Kuopio University Hospital. The flow of patients is presented in detail in Figure 1.
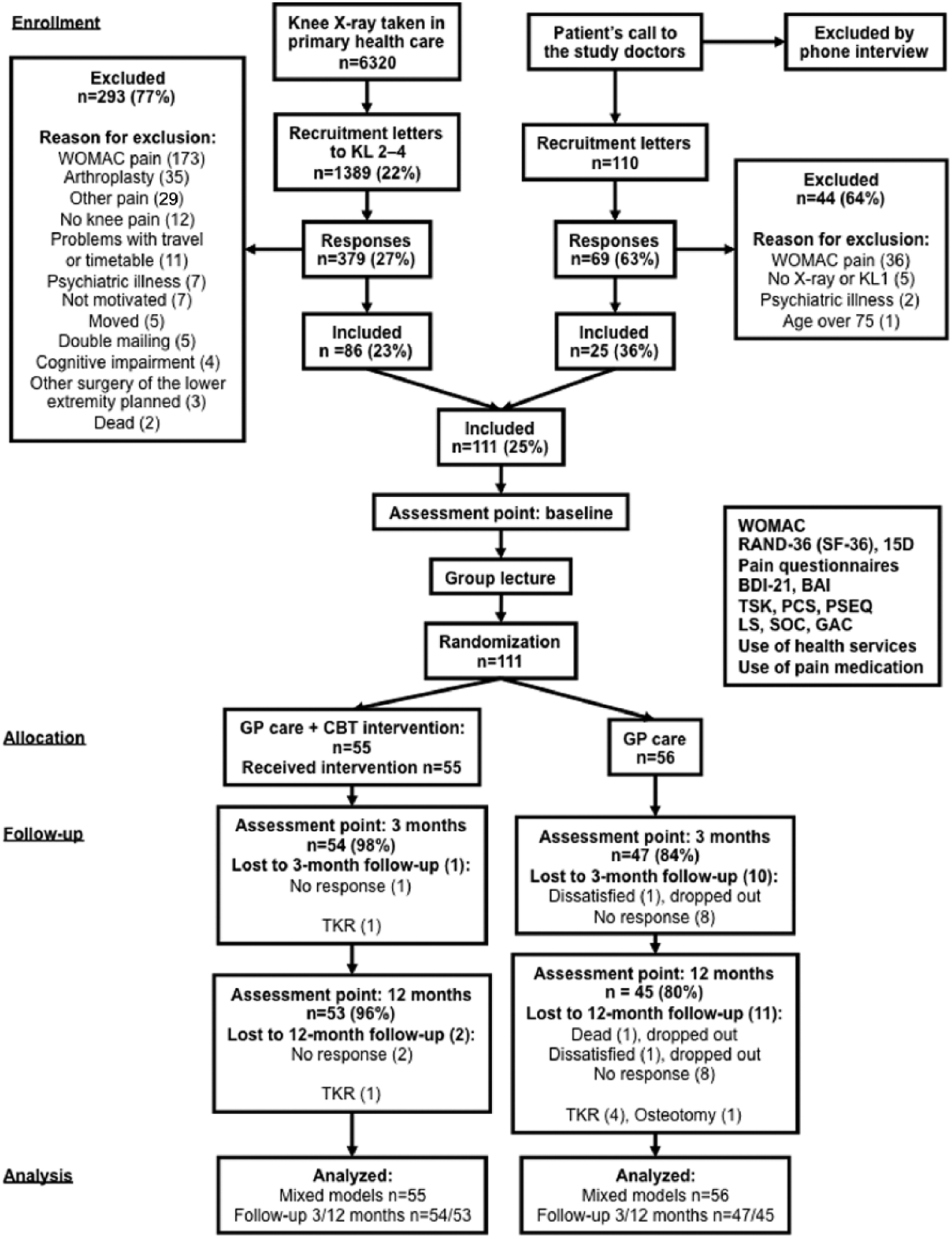
Flow of study patients.
The patients entered the study in groups of 14−28 (about 20), with the first group starting in September 2011 and the last in October 2012 (follow-up period ending correspondingly from September 2012 to October 2013). After participating in a lecture about the conservative treatment of knee osteoarthritis held by the study doctors, the participants were randomly assigned to intervention (GP care + intervention, n =55) and control (GP care, n = 56) group. The mean number of attended intervention sessions was 5.1 (SD ±1.6) out of 6. No statistical differences were noted in the baseline characteristics between the two groups (Table 1). No adverse events were recorded in either of the study groups.
Baseline characteristics of the 111 study patients, n (%).
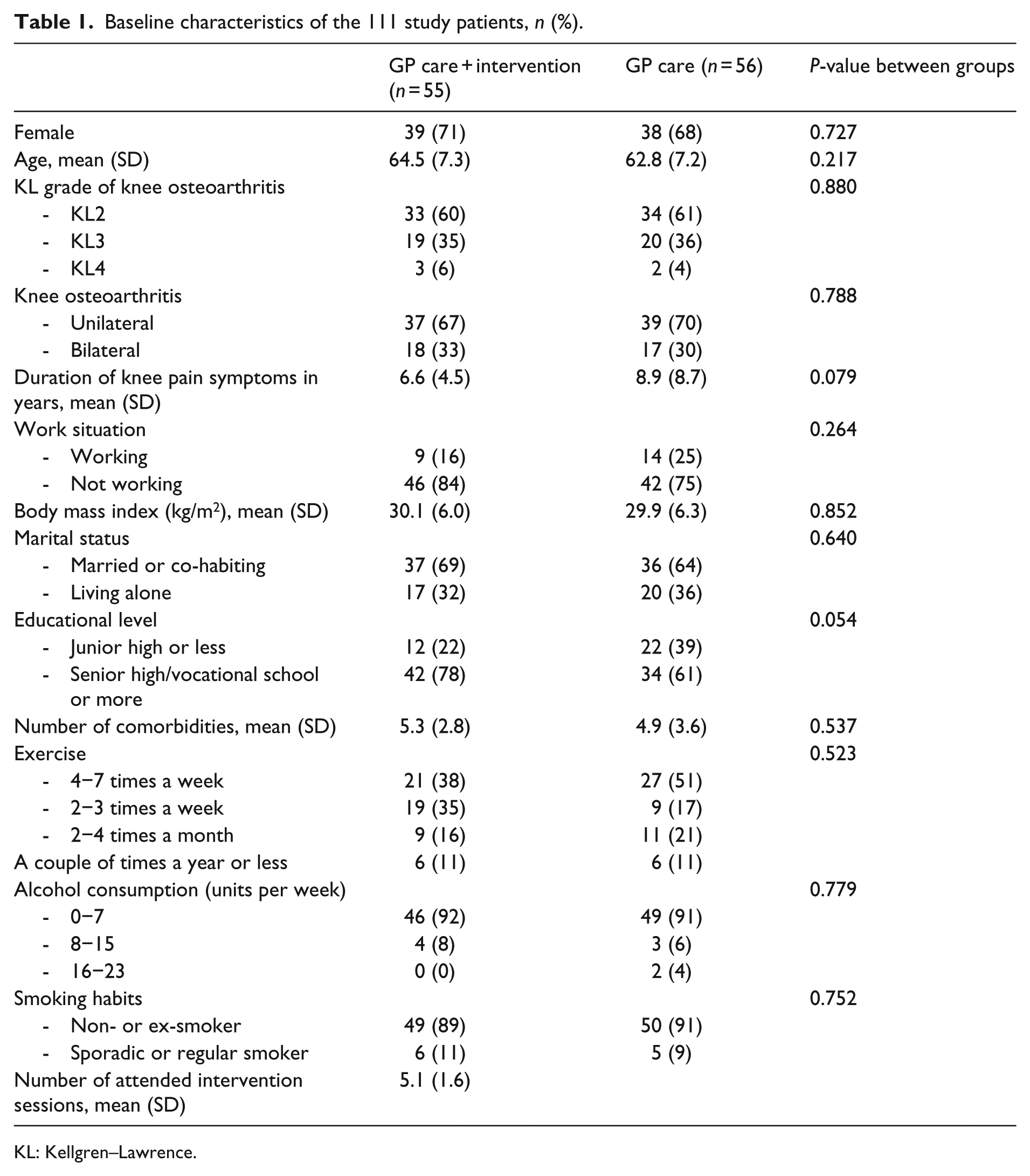
KL: Kellgren–Lawrence.
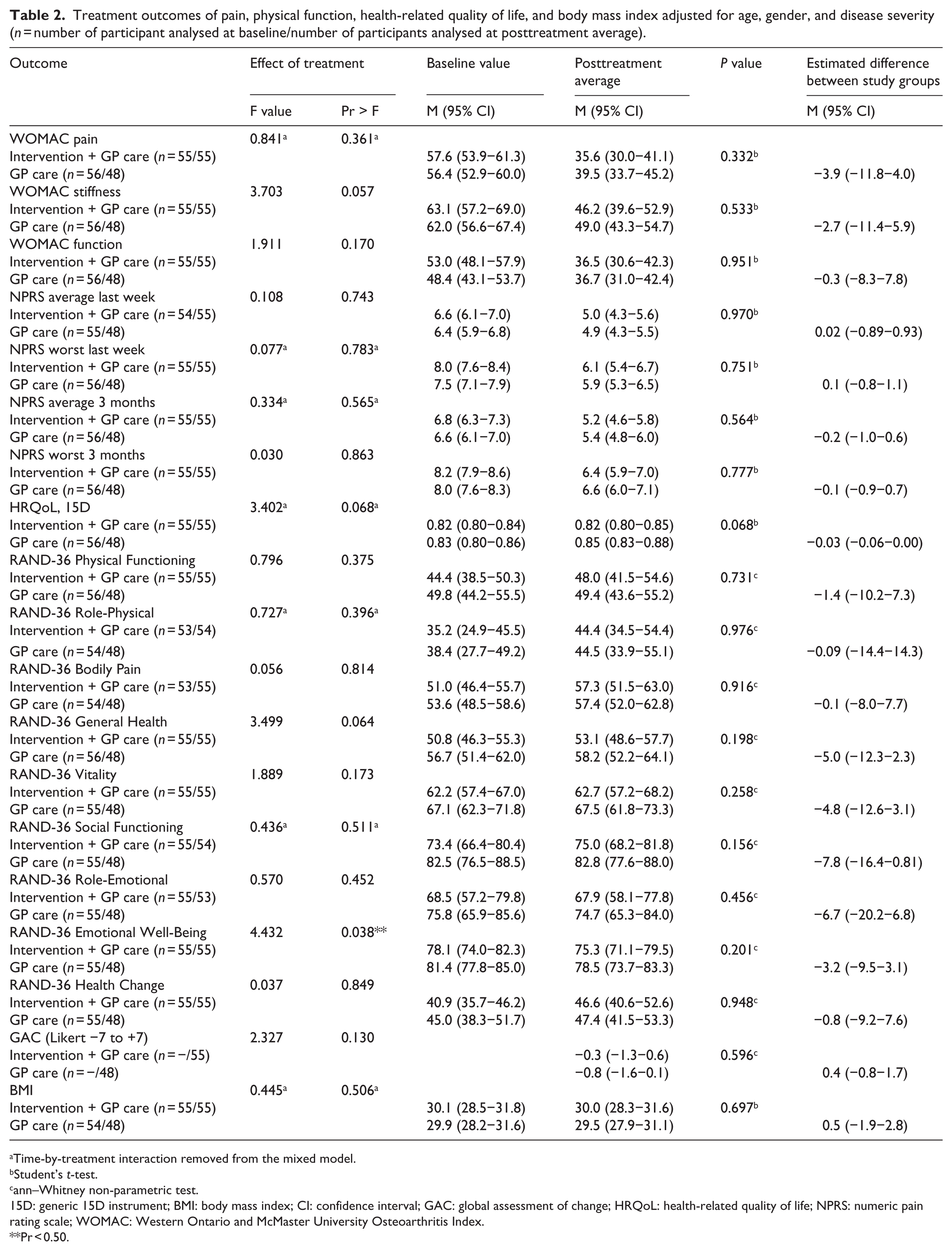
Mixed model results showed no significant difference between intervention and control group for any outcome measures of pain or function (Table 2). Among health-related quality of life instruments, no significant differences were found between the study groups in the 15D. In the RAND-36 a significant difference was detected in the emotional well-being multi-item subscale in favour of the intervention group (Pr = 0.038) (Table 2). The trend in the subscale, however, was descending in both of the groups so the mixed model detected a smaller decline for those who had participated in the intervention. Among psychological variables, a significant difference between groups was found in the Pain Self-Efficacy Questionnaire (Pr = 0.022) in favour of the control group (Table 3). Conventional group comparisons (Student’s t-test, Mann–Whitney U-test) of mean follow-up values revealed no significant differences between the groups in any of the outcome variables (Table 2 and 3). The WOMAC pain subscale was slightly lower in the intervention group at both follow-up points and the WOMAC function subscale at the short-term follow-up point (Figure 2), but no statistically significant differences were detected at these time points. Furthermore, there were no significant differences between the groups at any assessment point in the use of pain medication, the number of doctor appointments, physiotherapist appointments, or sick-leave days owing to osteoarthritis.
Treatment outcomes of pain, physical function, health-related quality of life, and body mass index adjusted for age, gender, and disease severity (n = number of participant analysed at baseline/number of participants analysed at posttreatment average).
Time-by-treatment interaction removed from the mixed model.
Student’s t-test.
ann–Whitney non-parametric test.
15D: generic 15D instrument; BMI: body mass index; CI: confidence interval; GAC: global assessment of change; HRQoL: health-related quality of life; NPRS: numeric pain rating scale; WOMAC: Western Ontario and McMaster University Osteoarthritis Index.
Pr < 0.50.
Treatment outcomes of psychological variables adjusted for age, gender, and disease severity (n = number of participant analysed at baseline/number of participants analysed at posttreatment average).
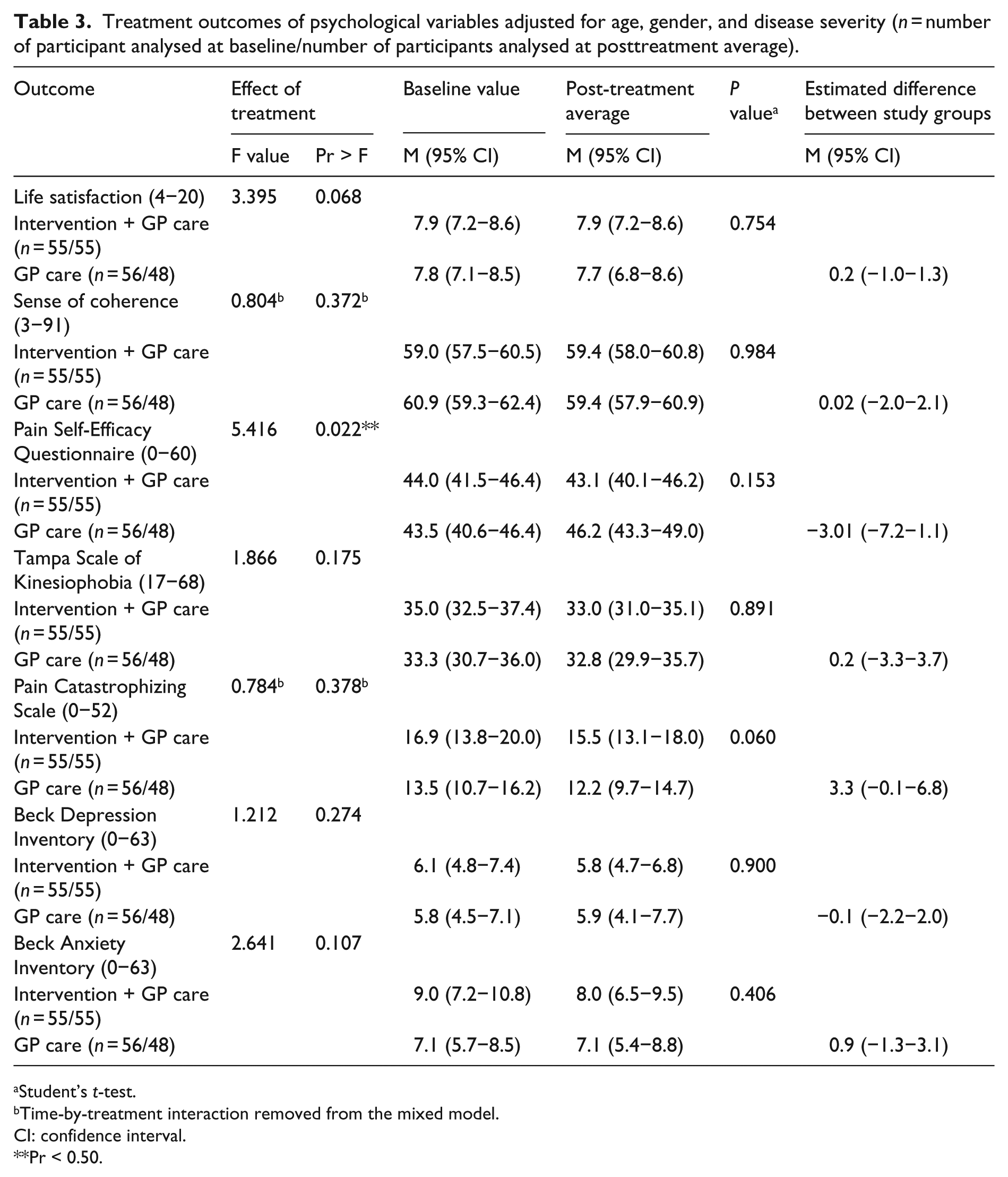
Student’s t-test.
Time-by-treatment interaction removed from the mixed model.
CI: confidence interval.
Pr < 0.50.
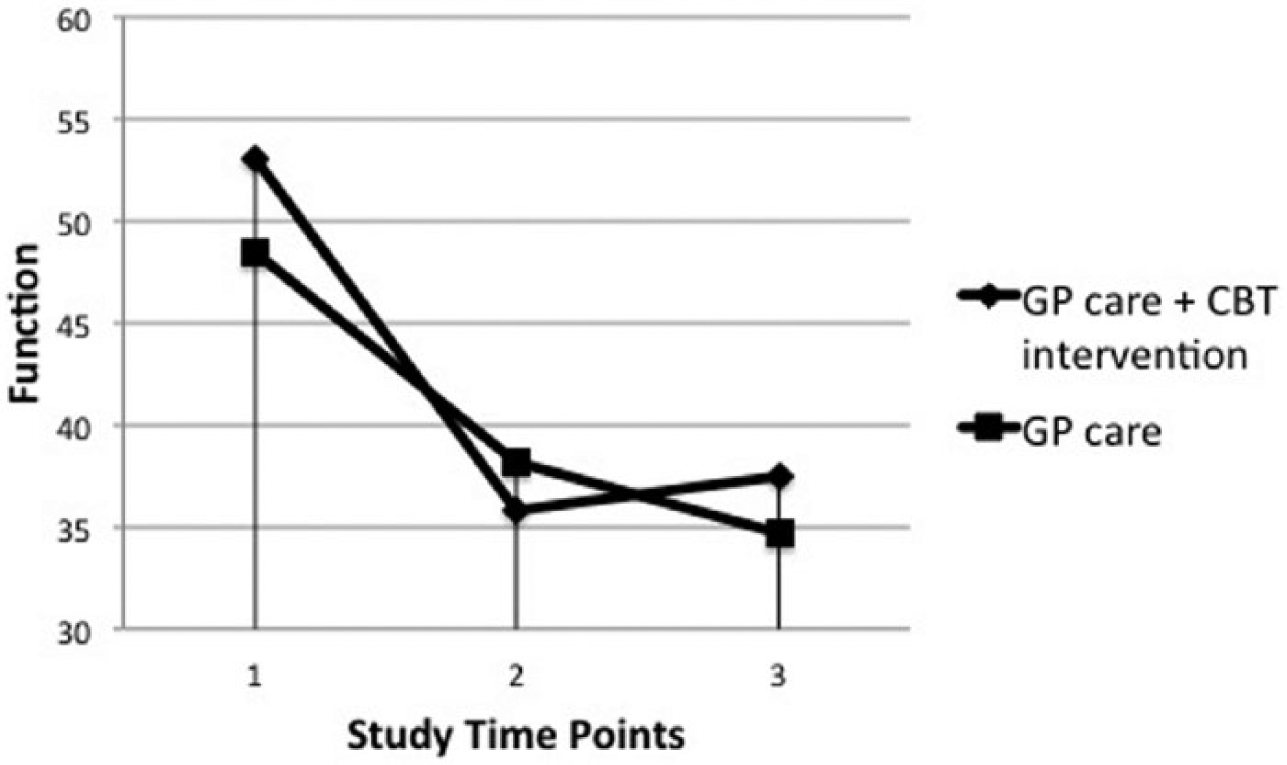
WOMAC function scores at baseline, three-months follow-up, and 12-months follow-up by randomization condition.
Discussion
This single-blinded RCT could not confirm the hypothesized advantage of a group-based cognitive–behavioural training programme over ordinary GP care in knee osteoarthritis pain patients. On the contrary, our findings indicated a negative impact of the intervention on pain self-efficacy in knee osteoarthritis patients. However, there seems to be a smaller decline in the emotional well-being for those who participated in the cognitive–behavioural training programme.
This study adds to the limited number of single-blinded RCTs evaluating the sole impact of a cognitive–behavioural intervention on knee osteoarthritis pain. To our knowledge, it is the only RCT applying Linton’s cognitive–behavioural model to treat knee osteoarthritis patients. The main reason for using Linton’s model was that we wanted a standardized and easily accessible model for further use. 14 However, Linton’s model does not include any assessments of adherence to the cognitive–behavioural practices of pain management after the programme. In hindsight, such measurements would have given us valuable information when interpreting the study results and evaluating the impact of the intervention. The strengths of this study include the repeated examination of a number of osteoarthritis related outcomes, the use of radiographic X-ray to confirm the osteoarthritis diagnosis, and the use of intent-to-treat. Furthermore, we considered that we recruited a representative sample of ordinary community-dwelling knee osteoarthritis patients, as most of the participants (77%, n = 86) were enrolled in the study as a result of a previous referral to a knee X-ray by their GPs.
The finding of the possible negative impact of cognitive–behavioural training on pain self-efficacy in knee osteoarthritis patients deserves attention. One explanation for this may be found in the characteristics of our study population: According to Nicholas, 35 high Pain Self-Efficacy Questionnaire scores following pain management programmes are commonly strongly associated with clinically significant gains, and they can thus be regarded as a useful gauge for evaluating intervention outcomes. However, it has been noted that high Pain Self-Efficacy Questionnaire scores (over 40) at the initial assessment would appear somewhat incongruent with someone needing a pain management programme. 35 When examining the initial scores of our intervention and control groups, it becomes evident that both of these groups reported strong confidence in performing activities while in pain (e.g. pain self-efficacy), even before any treatment or care: the initial Pain Self-Efficacy Questionnaire scores were 44.0 (intervention group) and 43.5 (control group). Although the respective posttreatment scores were 43.1 and 46.2, the clinical significance of these changes remains unclear. One interpretation of this unexpected result could be that cognitive–behavioural training may cause the patients to become more conscious of their pain and pain-related behaviour, and thus more clearly recognize the negative impact of knee osteoarthritis on their lives.
In a similar vein, one may question the applicability of Linton’s cognitive–behavioural treatment model 36 for our study population. Originally, the intervention of Linton et al. was designed to enhance coping behaviours in order to prevent long-term disability among patients with spinal pain. This intervention was therefore targeted at patients of working age having only a small number of sick leave days during the past six months. 37 In the original intervention study, 37 the mean age of the cognitive–behavioural treatment participants was 44 years. In contrast, the mean age of our study population in the cognitive–behavioural treatment group was 63 years, with the majority of the subjects not working and having had knee pain symptoms for over six years. In hindsight, the majority of our knee osteoarthritis patients had probably found their own ways of coping with knee osteoarthritis-related disability and recurrent pain.
Finally, as has previously been suggested, a predisposition to treating all chronic pain patients with the same set of methods may lead to incorrect conclusions regarding treatment efficacy.36,38 Instead, the tailoring of interventions according to patient subgroups has been investigated with promising results.36,38,39 It has been proposed that variables, such as the point of time for intervention, the duration of symptoms, psychological stress, low levels of physical activity, and reduced self-rated health, may be essential to the outcome in low back pain. 40
On a more general level, cognitive–behavioural treatment methods have been found useful in the management of chronic pain, with some evidence of positive effects being found at six months. 41 Clearly, more studies are needed to elaborate the significance of tailoring the interventions according to patient characteristics/subgroups at different time points of pain-causing disease.
Clinical messages
A group-based cognitive–behavioural training programme did not have a significant effect on knee osteoarthritis pain or function.
Footnotes
Acknowledgements
We thank the physicians who helped with patient recruitment at Kuopio Health Centre and Kuopio University Hospital; the data manager, Pauli Kuosmanen, of Kuopio Health Centre for technical support; the statistician, Tuomas Selander, of Kuopio University Hospital for advice in statistical matters; and professor, Olli-Pekka Ryynänen, of Kuopio University Hospital Primary Health Care Unit for creating the code for randomization. Finally, we thank the study patients for making this trial possible.
Conflict of interest
The authors declare that there is no conflict of interest.
Contributors
The authors contributed to the manuscript in the following way: EE Helminen, JPA Arokoski, and SH Sinikallio designed the trial protocol. EE Helminen and JPA Arokoski were responsible for patient recruitment. SH Sinikallio, RH Väisänen-Rouvali, EE Helminen, and JPA Arokoski adjusted the intervention programme to suit osteoarthritis patients. SH Sinikallio and RH Väisänen-Rouvali held the intervention sessions for the participants. EE Helminen, JPA Arokoski, and SH Sinikallio drafted the manuscript. AL Valjakka translated the session manual for therapists. JPA Arokoski and EE Helminen applied for the project funding. All authors have read and approved the final manuscript.
Ethical approval
The Research Ethics Committee of Hospital District of Northern Savo approved the protocol (reference number 14/2011). Written informed consent was obtained from all patients.
Funding
This study has been supported by an EVO and a VTR grant from Kuopio University Hospital.