
Abstract
Objective:
To conduct a systematic review of clinical trials that examined the effectiveness of interventions on balance self-efficacy among individuals with stroke.
Design:
Systematic review.
Summary of review:
Searches of the following databases were completed in December 2014: MEDLINE (1948–present), CINAHL (1982–present), EMBASE (1980–present) and PsycINFO (1987–present) for controlled clinical trials that measured balance self-efficacy in adults with stroke. Reference lists of selected articles were hand-searched to identify further relevant studies.
Review methods:
Two independent reviewers performed data extraction and assessed the methodological quality of the studies using the Physical Therapy Evidence Database Scale. Standardized mean differences (SMD) were calculated.
Results:
A total of 19 trials involving 729 participants used balance self-efficacy as a secondary outcome. Study quality ranged from poor (n = 3) to good (n = 8). In the meta-analysis of 15 trials that used intensive physical activity interventions, a moderate beneficial effect on balance self-efficacy was observed immediately following the programs (SMD 0.44, 95% CI 0.11–0.77, P = 0.009). In the studies that included follow-up assessments, there was no difference between groups across retention periods (eight studies, SMD 0.32, 95% CI −0.17–0.80, P = 0.20). In the four studies that used motor imagery interventions, there was no between-group difference in change in balance self-efficacy (fixed effects SMD 0.68, 95% CI −0.33–1.69, P = 0.18).
Conclusions:
Physical activity interventions appear to be effective in improving balance self-efficacy after stroke.
Introduction
Impairments in balance and mobility are common, such that the rate of falls after stroke is nearly two times higher relative to age and gender-matched counterparts. 1 Rehabilitation and recovery interventions typically focus on physical factors, such as balance and walking capacity, with gait training being one of most frequently addressed activities. 2 These interventions are effective in improving balance and mobility outcomes across the continuum of stroke care.3–5
Balance and mobility impairments are also associated with decreased balance confidence, 6 but the impact of stroke recovery interventions on psychological factors such as balance self-efficacy receives far less attention. Self-efficacy is defined as “an individual’s judgement of his or her ability to organize and execute given types of performances”. 7 It is a concept that originates from Social Cognitive Theory, which postulates that a person’s perceived level of ability better predicts behavior than their actual physical ability. 8 Within the context of balance and falls, self-efficacy may be related to either falls self-efficacy, defined as a person’s level of confidence in avoiding falling during daily activities, or balance self-efficacy, a person’s confidence in performing tasks without losing balance or becoming unsteady. 9 For the purposes of this review, falls self-efficacy and balance self-efficacy will be considered the same construct, and balance self-efficacy is the common term used hereafter.
Balance self-efficacy has been shown to be compromised in community dwelling individuals with stroke, 10 is a predictor of satisfaction with community reintegration, 11 a determinant of falls in chronic stroke survivors with low bone mineral density, 12 and is independently associated with post-stroke activity and participation. 13 Interventions that improve post-stroke mobility may also contribute to improved self-efficacy by influencing elements of Social Cognitive theory, such as mastery experience (offering opportunities for successful performance), verbal persuasion (positive feedback from instructors or therapists), change in physiological or affective states, or vicarious experience (observing others successes). Importantly, it is anticipated that strategies effective in improving balance self-efficacy are also associated with meaningful clinical endpoints, particularly reduced risk and rate of falling. To prevent a perpetuating cycle of fall incidents, deconditioning and functional decline, 14 it is important to establish effective interventions to improve balance self-efficacy after stroke.
To our knowledge, there has been no previous review of the effects of post-stroke interventions on balance self-efficacy. The objective of this review was to summarize the results of controlled clinical trials to determine the effectiveness of interventions on improving balance self-efficacy in people with stroke.
Methods
This review was written according to the guidelines of the Preferred Reporting Items for Systematic reviews and Meta-Analyses. 15
Studies were eligible for inclusion if they compared an intervention to a control group, involved adults with hemorrhagic or ischemic stroke, at any stage or severity along the post-stroke continuum, were conducted in any setting, reported an outcome measure (primary or secondary) related to balance self-efficacy and were published in English. Case studies, case series, pretest/posttest (non-controlled) studies, dissertations and conference proceedings were excluded, as well as studies that included participants with significant comorbidities affecting balance and mobility.
The following databases were searched up until 4 December 2014: MEDLINE (1946–present), Excerpta Medica database (EMBASE) (1974–present), PsycINFO (1987–present) and Cumula-tive Index to Nursing and Allied Health Literature (CINAHL) (1982–present). The specific MEDLINE, EMBASE and PsycINFO search strategies are outlined in the Appendix (available online), and an equivalent search was applied for the CINAHL database, with appropriate indexing and syntax modifications applied. Reference lists of selected articles were hand searched to identify further relevant studies. Studies were included for further screening even if balance self-efficacy related terms were not mentioned in the title and abstract, provided that all other eligibility criteria were met.
Two independent reviewers initially screened study titles and abstracts for eligibility, then screened and evaluated the full text of all relevant studies. If needed, disagreements were resolved through consultation with a third reviewer.
The following data were extracted: study type, details of participant characteristics, interventions, outcome measures, results and time of follow-up.
For the qualitative assessment, methodological quality of all studies was appraised using the Physical Therapy Evidence Database (PEDro) scale, 16 a scale that has been used beyond physical therapy interventions, such as pharmacological and non-pharmacological therapies. 17 Where available, scores were obtained from the PEDro website (www.pedro.org.au); otherwise, scores were determined independently by two reviewers with disagreements resolved by a third reviewer. Study quality was defined using PEDro scores as follows: “good” 6–8 points, “fair” 4–5 points and “poor” ⩽3 points. 18 Participants, interventions, comparisons, outcomes and occurrence of adverse events were described.
For the quantitative analysis, the end-point outcome measures used were continuous scales ofbalance self-efficacy or falls self-efficacy. Stand-ardized mean differences (SMD) were used to determine treatment effect sizes, along with 95% confidence intervals (CIs). For outcomes with opposite polarity, treatment effects were reversed so that higher scores always indicated better outcome. For all studies, mean change was calculated as the difference between baseline (pre-intervention) and the first postintervention time points. For studies that included long-term follow-up, mean change between the first and last postintervention time points was also determined. Effect sizes were defined as small 0.2–0.3, medium 0.5, large >0.8. 19 Fixed effect models were utilized if statistical heterogeneity was low (quantified using the I2 value, which represents the extent of inconsistency among the results that is owing to true variation rather than sampling error or chance 20 ). Random effect models were utilized in all other cases. The level of heterogeneity was defined as follows: I2 25% low, 50% moderate, 75% high heterogeneity. Forest plots were generated to illustrate the overall effect of interventions on balance self-efficacy, and funnel plots were used to determine whether publication bias was present. Sensitivity analysis was performed to compare random- and fixed-effect models, and by removing lower quality studies rated as poor or fair quality (PEDro score <6). Statistical analysis was performed using Review Manager software package (RevMan 5.0, Cochrane Collaboration).
Results
Figure 1 presents the study flow diagram. The initial search identified 459 citations, of which 181 were removed as duplicates. The titles and abstracts of the remaining 278 articles were screened, 246 were excluded, 32 full-text articles were further screened, of which 17 met all eligibility criteria. Two additional articles were identified through searching the reference lists of relevant articles. In total, 19 articles21–39 involving 729 participants, were included in the systematic review (Table 1, available online).
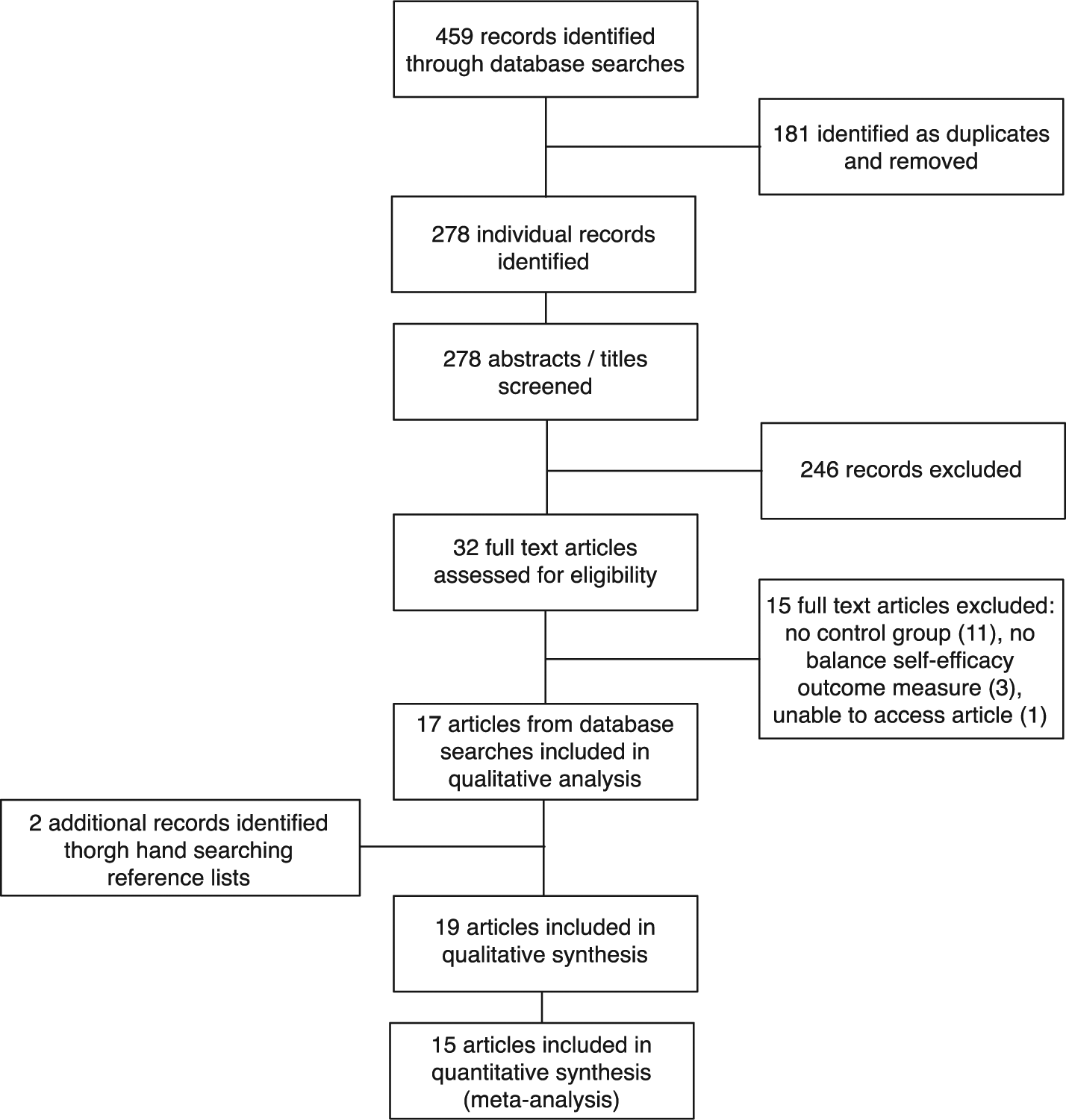
Study flow diagram.
Qualitative analysis
Of the studies included in the qualitative analysis, 15 were randomized controlled trials (RCTs).22–27,30–33,35–39 All but two37,38 were rated as “good” quality (Table 2, available online). Randomization was performed by an independent person or by a computer generated randomization program. The remaining three studies were controlled but not randomized trials, mostly rated “good” 34 and “fair”28,29 in quality, with the exception of one that was rated poor quality 21 (Table 2, available online). Eleven studies22–25,27,30–32,37–39 included assessments at follow-up time points to evaluate retention of benefits, ranging from two weeks to six months after the intervention ended. In five studies,24,26,31,37,39 loss to follow-up was greater than 15%.
Participants
Sample size ranged from 16 21 to 91. 36 Participants’ age ranged from 53 to 80 years, except in one study (<50 years). 29 All were ⩾3 months post-stroke, with 12 studies involving participants ⩾6 months post-stroke.22–26,29–33,35,39 Four studies set upper limits on time post-stroke (within 6,27,37 12, 36 or 24 24 months). Four studies were conducted in a rehabilitation setting, but participants were 1–5 years post-stroke.22,23,32,35. The remaining studies were conducted in the community or laboratory settings. Participants were independent with ambulation with or without assistive devices, except in one study where participants needed only to be able to stand with or without a device. 37 Participants with severe co-morbidities (such as neurological (other than stroke), orthopedic or cardiovascular problems, or any other conditions that precluded study participation) were excluded.
Interventions
Interventions were ⩽4 weeks,24,26,29,32,35,38,39 one to three months,21–23,25,27,28,30,31,36,37 or >5 months33,34 in duration. Intervention frequency ranged from one to five sessions per week.
A total of 14 studies involved physical exercise interventions: gait training alone30,34–36 or combined with virtual reality,26,39 exergaming, 22 combination of fitness, mobility and functional exercises,27,28,31–33 dynamic exercises combined with whole body vibration, 25 yoga 37 and functional movements combined with body awareness training. 23 Pool exercises, 28 home programs 27 and education sessions27,28 were also offered. In the four studies that did not use physical activity interventions, motor imagery training was used.21,23,24,29,38
Comparisons
All but four studies were RCTs. In the non-randomized studies, participants self-selected their intervention group based on location and accessibility constraints, 28 assigned based on order of study enrolment 21 or control participants were matched based on age, sex, lesion, time post-stroke or impairment level.29,34
In general, control interventions were comprised of less intensive or lower dose physical activity relative to the intervention groups. These included upper extremity physical33,36 or mental practice training, 21 weight shifting and stretching, 31 dynamic exercises without whole body vibration 25 or routine physical therapy.30,35 Otherwise, control interventions included stroke educational programming27,28,32,38 health-related documentary programs, which may have been supplemented with routine physical therapy,29,38 or treadmill training without an immersive virtual reality environment.26,39 In three studies,23,34,37 the control group continued with their usual activities but did not receive any intervention. In six studies,27,28,34,35,37, groups were not matched for equivalent minutes of attention. Only one study 22 was designed such that the control intervention was comparable with respect to time and content of training as the intervention group (weight shift training through exergaming vs. through conventional methods).
Outcomes
None of the trials used measures of balance self-efficacy as the primary outcome. Almost all studies used the Activities-specific Balance Confidence scale (ABC) (three25,34,39 used the Chinese version 40 ). The Falls Efficacy Scale-International (FES-I) 41 and Falls Efficacy Scale-Swedish version were also used.22,24,27 The ABC Scale and FES-I have both been shown to have good validity and reliability in community dwelling elderly individuals.9,41,42 The ABC scale has been validated for use in community dwelling individuals both within 43 and after one year post-stroke. 44 The standard error of measurement (SEM) among individuals with stroke is 6.81. 44 Eight25,26,28–30,35,36,39 of the 13 studies that used the original ABC scale reported improvement in the intervention group that exceeded the SEM.
Adverse events
Five studies21–23,25,30 reported that no serious adverse events occurred. Two studies reported on occurrence of falls among participants: 26 falls involving five people in the intervention group and six in the control group, 27 100 falls involving 16 intervention group participants and 11 in the control group. 31 Adverse events were not reported in the other studies.
Quantitative data analysis
A meta-analysis was performed with the 15 studies that compared more intensive physical exercise-based interventions to less intensive programs.22,23,25–28,30–37,39 Immediately following the programs, a medium effect was found favoring interventions over the control group to improve balance self-efficacy after stroke (627 participants, SMD 0.44, 95% CI 0.11–0.77, P = 0.009) (Figure 2(A)). When the non-randomized trials were removed from the analysis,28,34 the trend towards a beneficial effect of more intensive physical interventions remained (582 participants, SMD 0.43, 95% CI 0.07–0.80, P = 0.02). A large effect was found when only the 12 studies that used the ABC scale were included (545 participants, mean difference 3.17, 95% 0.45–5.89, P = 0.02). In the eight studies that included follow-up assessments,22,23,25,27,30–32,37 there was no difference between groups across retention periods (n = 347, SMD 0.32, 95% CI −0.17–0.80, P = 0.20) (Figure 2(B)).
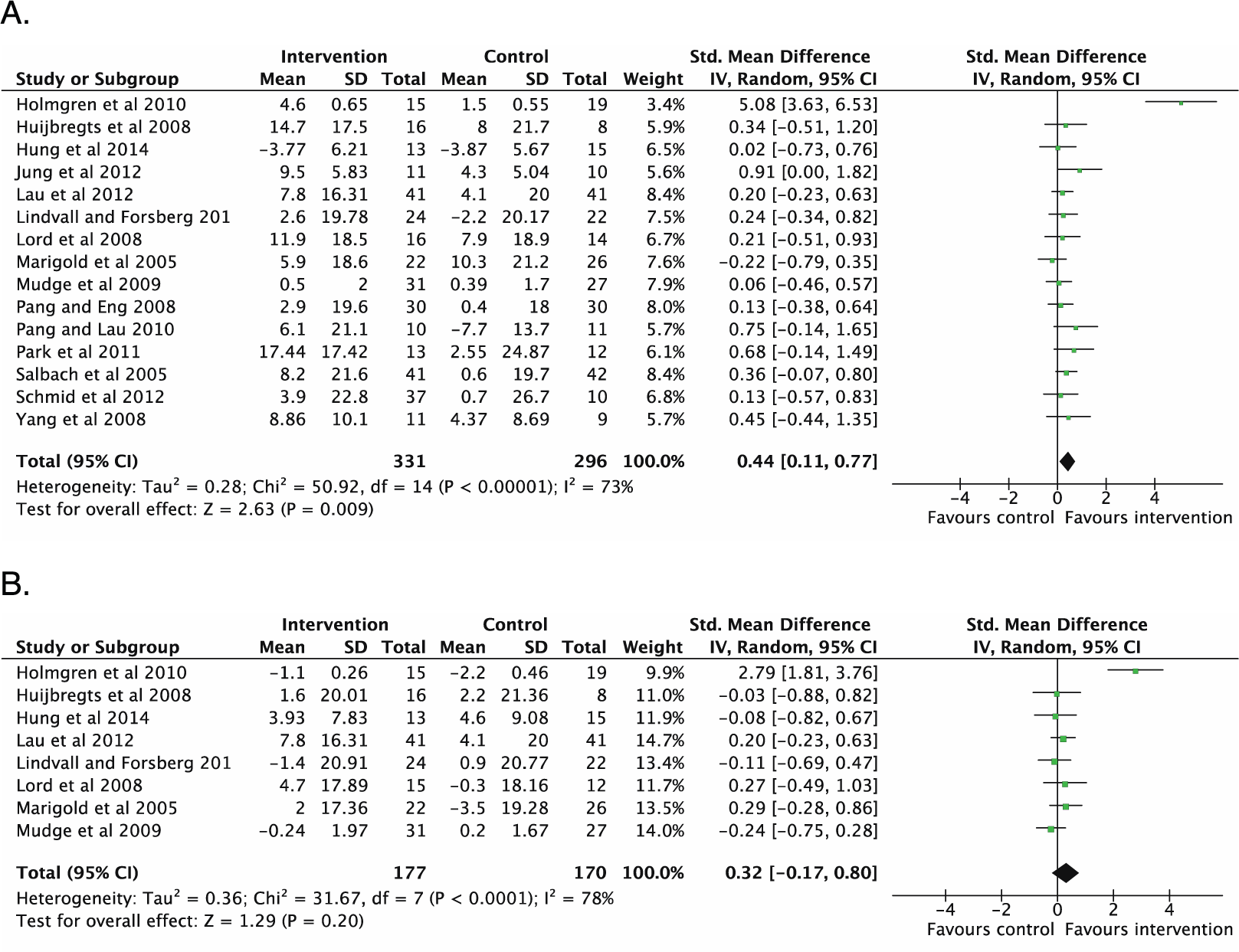
Meta-analyses of (A) 15 studies involving intensive physical activity interventions for training effects immediately after the programs ended, and (B) eight trials that included postprogram follow-up assessments.
In sensitivity analyses, all randomized trials were of “good” quality (PEDro score ⩾6) (Table 2, available online) and as such, no studies were removed based on quality. However, high heterogeneity was noted (I2 = 82%), and the funnel plot indicated possible publication bias with an outlier study 27 (Figure 3). With this study removed, the beneficial effect of intensive physical interventions on balance self-efficacy immediately following the programs remained among homogeneous studies (593 participants, fixed effects SMD 0.23, 95% CI 0.07–0.40, P = 0.006, I2 = 0%). In the studies that included follow-up assessments, no difference was observed between groups (313 participants, fixed effects SMD 0.05, 95% CI −0.17–0.28, P = 0.65, I2 = 0%).
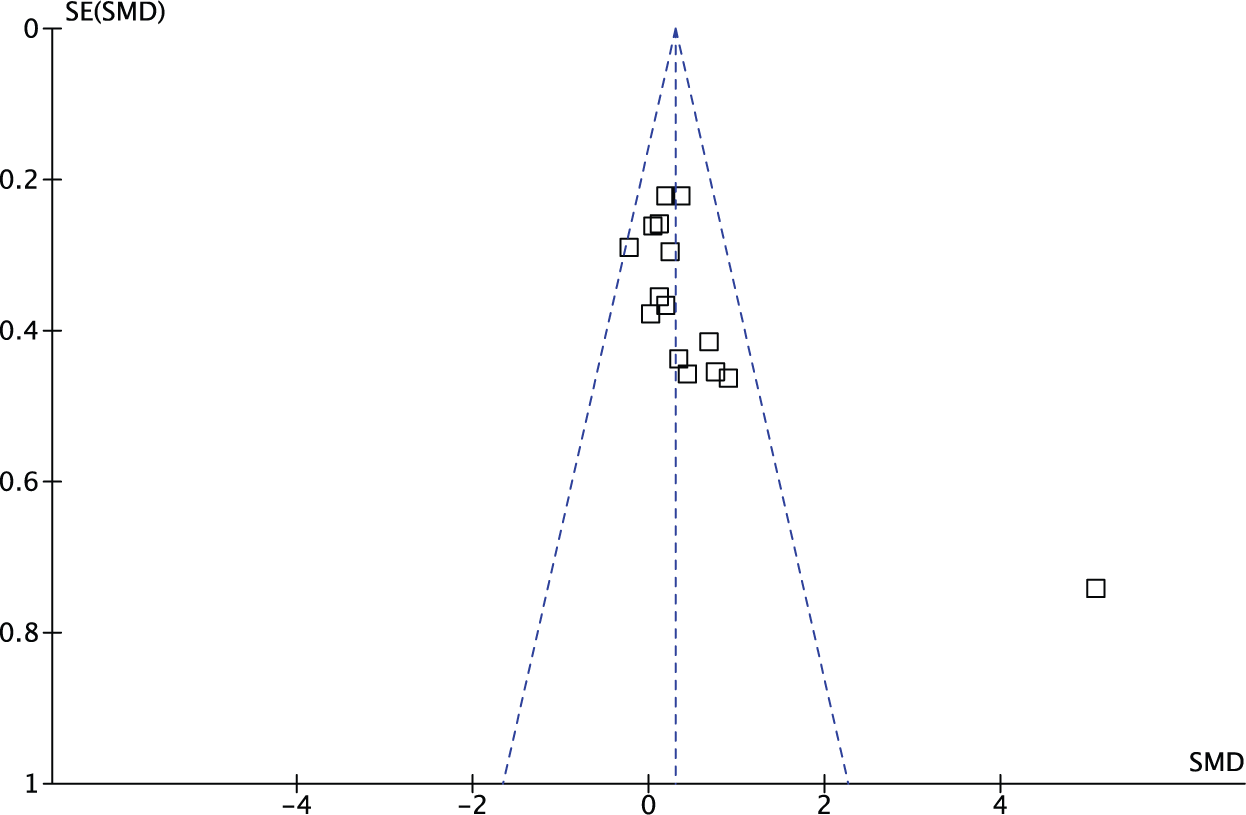
Funnel plot of 15 studies involving intensive physical activity interventions included in meta-analysis.
There were four studies21,24,29,38 that used motor imagery interventions. There was no difference in change in balance self-efficacy between groups (102 participants, fixed effects SMD 0.68, 95% CI −0.33–1.69, P = 0.18).
Discussion
Results from this systematic review suggest that intensive physical interventions, specifically those that involve strengthening, balance, endurance and functional exercises, are more effective than less intensive interventions for improving balance self-efficacy after stroke. There were no differences between groups in follow-up studies.
Post-stroke balance impairment is common and can contribute to mobility restriction and increased risk of falls, but balance self-efficacy is also an important predictor of fall risk, 11 activity, and participation. 13 It is important to establish interventions that not only address the physical factors that contribute to improved balance and walking after stroke, but also benefit psychological factors, such as balance self-efficacy. The interventions in these trials were not specifically targeted towards improving balance self-efficacy, as the measures selected were included as a secondary (not primary) outcome. Thus, the studies may not have been adequately powered to detect change in this outcome. Indeed, when individually considered, many of the studies reported non-significant effects of training on balance self-efficacy, but when study results were combined in the meta-analysis, we found that intensive physical interventions were effective in improving balance self-efficacy after stroke.
These programs may have offered the necessary elements of Social Cognitive Theory to influence balance self-efficacy, 8 which may account for the positive benefit observed. Indeed, Huijbregts and colleagues 28 designed the intervention arm of their study with enhancing self-efficacy in mind. In all other trials,27,30–37,39 physical activity interventions may have influenced self-efficacy through mastery experience by offering opportunities for successful performance of tasks and activities that challenge and improve balance. Further, verbal persuasion may have been incorporated through positive feedback from class instructors, and participants would also experience change in physiological or affective states during the interventions. In trials that offered group classes,28,31–33,37 vicarious experience may be gained from observing others successfully perform a task. Arguably, increasing self-efficacy after stroke is relevant only if it also leads to reduced occurrence of falls. Future research may focus on establishing the effectiveness of interventions on improving both balance self-efficacy after stroke and clinical end-points of risk and rate of falls.
In an earlier meta-analysis of the effectiveness of exercise interventions on balance self-efficacy among older adults without neurological conditions, Tai Chi was more effective than strengthening, functional or task-specific activities. 45 The authors postulated that the sensory-motor balance elements of Tai Chi, combined with cognitive and emotional stimuli of relaxation and awareness, contributed to greater improvements in balance self-efficacy compared with physical activity interventions alone. 45 For individuals with stroke, similar interventions that concurrently address physical and cognitive factors may yield greater benefit to balance self-efficacy than either form of intervention alone. To date, no studies have examined the effects of Tai Chi on balance self-efficacy after stroke, but one pilot study reported improvements in ABC score with post-stroke yoga. 37 The authors attribute these positive effects to the active mind–body connection and complex coordination of movement and breathing that is offered through yoga. 37 Future studies may also examine the effects of interventions that explicitly incorporate relevant components of Social Cognitive Theory foundations 8 to improve balance self-efficacy.
The heterogeneity of the included studies was quite high, such that one study 27 demonstrated the largest effect on balance self-efficacy and was identified as an outlier. When this study was removed from the meta-analysis, the trend towards improved balance self-efficacy was retained, although there was a reduction in the overall effect. Of the five trials where groups were not matched for attention,27,28,34,35,37 this study had the largest disparity (60 vs. 450 minutes/week for control and intervention groups, respectively 27 ). This difference in contact time may account for the greater between-group interaction effect.
There were no differences between groups in studies that included follow-up assessment time points. It is possible that intervention-related improvements in balance self-efficacy wane over time, or programs of longer duration are required for durability of benefits. This may also be a product of the smaller number of trials included in the analysis and thus, there was less sensitivity for detecting change.
The three studies that used motor imagery interventions had disparate findings. Hwang et al. 29 found a large treatment effect, but also enrolled younger participants (47 29 vs. 63 38 and 72 24 years) and provided the greatest total training time (five 30-minute sessions per week for four weeks (total 600 minutes) 29 vs. three 15-minute sessions per week for four weeks (180 minutes) 24 and three 50-minute sessions per week for two weeks (300 minutes) 38 ). Given the discrepancy in study results and differences in program design, further research focusing on imagery-related interventions is needed to establish its effectiveness on balance self-efficacy.
The major limitation to this systematic review is that none of the trials had the primary aim of examining the effectiveness of post-stroke interventions on balance self-efficacy as the primary outcome. RCTs designed and adequately powered to improve balance self-efficacy among individuals with stroke are warranted. There was also a range in methodological quality across the studies, and differences between control and intervention groups with respect to treatment type, delivery and attention time, which may have influenced the results. Moreover, owing to the small number of studies and participants, secondary analyses to compare participant subgroups or intervention types were not performed. As the body of evidence continues to develop, more in-depth analyses will be permitted that may examine the differential effects across stages of stroke recovery (early to late), across interventions (physical, cognitive, psychological, combination) or across levels of functional mobility (low to high). Further, more studies that include follow-up assessments to determine the long-term effects of post-stroke interventions on balance self-efficacy are warranted.
Clinical messages
Physical activity interventions involving strengthening, balance, endurance and functional exercises appear to be effective in improving balance self-efficacy after stroke.
Addressing psychological factors related to balance ability after stroke can be an important strategy for breaking the cycle of fall occurrence, activity restrictions and functional decline.
Footnotes
Acknowledgements
We would like to thank Charlotte Beck in assisting with our search strategy.
Conflict of interest
The authors declare no conflicts of interest.
Contributors
JJE designed the study. AT (Tang), AT (Tao), MS, CT, HT, JT conducted the research and drafted the manuscript. JJE revised the manuscript. All authors read and approved the final manuscript.
Funding
AT (Tang) is supported by personnel awards from the Heart and Stroke Foundation, Ontario Provincial Office [CS I 7468], the Canadian Institutes of Health Research [MFE-98550] and the Michael Smith Foundation for Health Research (MSFHR) [ST-PDF-03003(11-1)CLIN], and JJE was supported by the CIHR [MSH-63617].
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.