
Abstract
Objective:
To assess the feasibility of conducting a well-powered trial evaluating the neurological and functional effects of using an exoskeleton in individuals with chronic spinal cord injury.
Design:
A longitudinal, prospective, self-controlled feasibility study.
Setting:
Specialist Spinal Cord Injuries Centre, UK; 8 months during 2013–2014.
Subjects:
Individuals with chronic motor complete or incomplete spinal cord injury.
Interventions:
Enrolled subjects were assigned to 20 exoskeleton (ReWalk™, Argo Medical Technologies Ltd, Yokneam Ilit, Israel) training sessions over a 10-week training period.
Main measures:
Feasibility measures, clinical and mobility outcome measures and measures appraising subjects’ disability and attitude towards assistive technology were assessed before, during and after the study. Descriptive statistics were applied.
Results:
Out of 60 candidates, ten (17%) were enrolled and five (8%) completed the training programme. Primary reasons for not enrolling were ineligibility (n = 24, 40%) and limited interest to engage in a 10-week training programme (n = 16, 27%). Five out of ten enrolled subjects experienced grade I/II skin aberrations. While walking speeds were higher and walking distances were longer in all exoskeleton users when compared with non-use, the exoskeleton did generally not meet subjects’ high expectations in terms of perceived benefits.
Conclusions:
The conduct of a controlled trial evaluating the benefits of using exoskeletons that require a lengthy user-commitment to training of individuals with chronic motor complete or incomplete spinal cord injury comes with considerable feasibility challenges. Vigilance is required for preventing and detecting medical complications in spinal cord injury exoskeleton users.
Introduction
Two key goals of spinal cord injury (SCI) rehabilitation are to restore as well as reduce the impact of acquired physical impairments. Physical interventions that address activity limitations lead to increased participation and, ultimately, improve patients’ overall quality of life. 1 Among other rehabilitation targets, regaining independent ambulation has been demonstrated to be a high priority for recovery among patients with SCI. 2 However, recent data from a European multi-centre study demonstrated that only 4 out of 10 people who sustain a SCI will be able to walk independently again. 3
Over the last decade, researchers started to focus on the role of advanced assistive technologies for locomotor training in individuals with SCI. 4 Body-weight-supported treadmill training with robotic assistance is one such intervention. While both the quality and quantity of available evidence on these novel therapies is still limited, some ambulatory capacity and gait benefits have been demonstrated in patients with chronic SCI using these new approaches. 4 However, their effects on independent ambulation have not yet been established, and access to these assistive ambulatory technologies is limited to those attending specialist rehabilitation centres.
More recently, the safety and performance of powered exoskeletons have been investigated in various pilot studies.5–9 An exoskeleton is a wearable brace support suit featuring motors at the hip and knee joints, rechargeable batteries and a computer-based control system. One of the potential advantages of exoskeletons is that, in contrast to body-weight-supported treadmills, these wearable devices allow people to walk independently in the community. While other investigators have studied individuals with motor complete injuries only,5–9 our aim was to evaluate the neurological and functional effects, as well as changes in appraisals of disability in a broader group of individuals with chronic motor complete or incomplete SCI. Moreover, as previous studies reported on a highly selective group of exoskeleton users,5–9 we paid particular attention to the feasibility aspects of running a larger, well-powered study in an outpatient setting in the UK.
Material and methods
A longitudinal, prospective, self-controlled feasibility study was conducted at the National Spinal Injuries Centre (NSIC), Stoke Mandeville Hospital, Aylesbury, UK, between August 2013 and March 2014. National research ethics (reference: 13/EE/0048) and institutional approvals were obtained and study protocol details were publicised on ClinicalTrials.gov (NCT01943669) prior to commencement of the study.
Study population and recruitment
Adult individuals with an acquired SCI or dysfunction were invited and screened against the eligibility criteria presented in Table 1. A lay summary of the study proposal was presented on a webpage dedicated to the study as well as on the ClinicalTrials.gov webpage. In addition, advertisements inviting interested persons to participate were published in various magazines and newsletters that went out to the local and national SCI community. Outpatients visiting the hosting institution before and during the study were also informed about the opportunity to participate. In order to prescreen potential candidates, a ‘Volunteer Information and Questionnaire form’ was sent to those who expressed an interest to participate. The questionnaire covered the principal eligibility criteria as described in Table 1, which allowed interested persons to predetermine whether they would fit the inclusion criteria before approaching the study coordinator. Interested candidates who felt that they fitted the prescreening criteria were invited to attend a study screening appointment.
Study eligibility criteria.
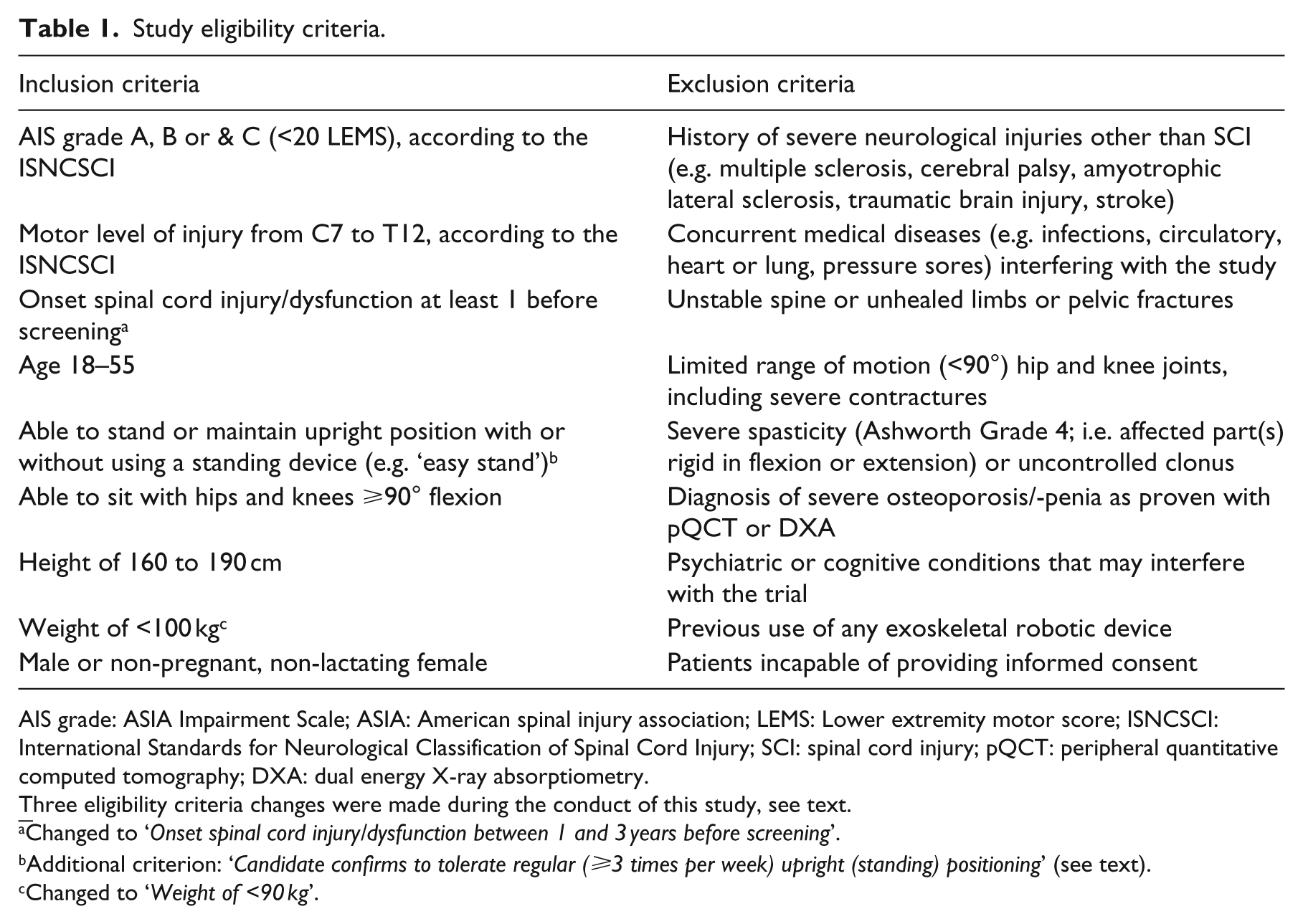
AIS grade: ASIA Impairment Scale; ASIA: American spinal injury association; LEMS: Lower extremity motor score; ISNCSCI: International Standards for Neurological Classification of Spinal Cord Injury; SCI: spinal cord injury; pQCT: peripheral quantitative computed tomography; DXA: dual energy X-ray absorptiometry.
Changed to ‘Onset spinal cord injury/dysfunction between 1 and 3 years before screening’.
Additional criterion: ‘Candidate confirms to tolerate regular (⩾3 times per week) upright (standing) positioning’ (see text).
Changed to ‘Weight of <90 kg’.
Device and training
For the current study, the ReWalk™ exoskeleton (Argo Medical Technologies Ltd, Yokneam Ilit, Israel) was used. This exoskeleton is an external, bipedal lower limb frame that is attached to a central pelvic bar and consists of inbuilt actuator motors located near the hip and knee joints. The user is strapped into the device using soft strapping and a rechargeable battery and computer unit are carried in a backpack. The exoskeleton is controlled by a wireless mode selector that is worn on the user’s wrist. A tilt sensor permits a predetermined hip and knee action that results in a step forward. A continuous gait pattern is reliant upon the user’s ability to tilt the device to the opposite side in order to allow the opposing hip and knee to step. This is done through altering the trunk position and therefore the centre of gravity with varying levels of trunk control and the use of elbow crutches. If no tilt or inadequate tilt is sensed, the exoskeleton takes this as a signal to stop, thus allowing the user to control ambulation without operating the remote. The exoskeleton also features a sit–stand–sit transfer mode that allows the user to stand up and sit down independently. The device is completely untethered and has the ability to ascend and descend stairs with set programs for each.
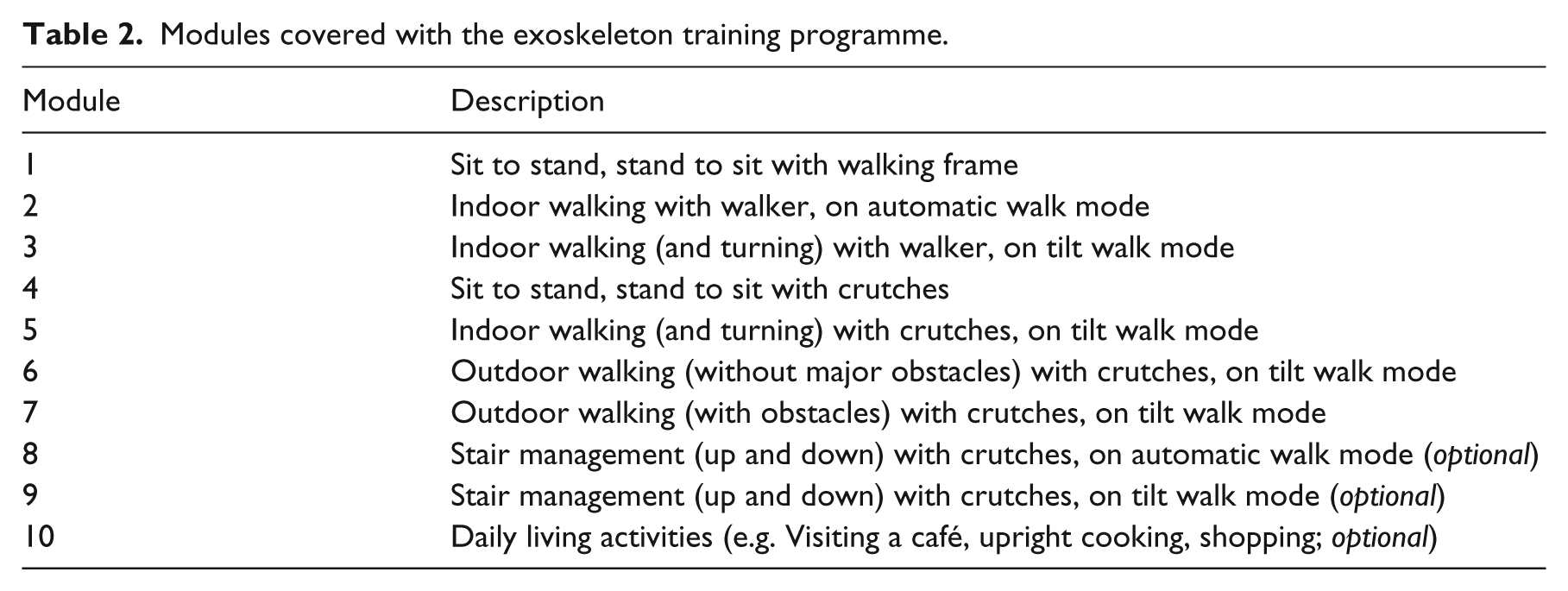
Individual measurements for the exoskeleton and strap lengths were taken. The pelvic width, femoral and tibial lengths were adjusted for each participant as required. Each training session lasted a total of two hours, which included one hour of exoskeleton training and time required for device set up and data collection. Training sessions took place twice weekly, and where possible, for an uninterrupted 10-week training period. A prespecified training programme consisting of progressive training modules was developed, see Table 2. Each training session was tailored to suit the individual’s progress and needs, and was performed by a chartered, registered and qualified physiotherapist trained in the use of the device.
Modules covered with the exoskeleton training programme.
Outcome measures and analysis
A number of feasibility indicators were documented in this study. First, the numbers of patients who showed an initial interest in participating, who were eligible and who successfully completed this feasibility study were recorded. Second, the number of training sessions each individual required before stair climbing was deemed safe and appropriate by the physiotherapist was documented. And third, the occurrences of and reasons for individual training interruptions were registered.
Subjects’ neurological status was assessed before and after the training programme using the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI). 10 Before and after each training session, a number of clinical measures, including heart rate, blood pressure and spasticity, were monitored. Levels of pain and fatigue were monitored using horizontal 10-cm visual analogue scales (VAS). Each session included a visual inspection of vulnerable areas of skin before, during and after exoskeleton use. Episodes of skin breakdown or damage were graded and documented according to the European Pressure Ulcer Advisory Panel classification system. 11
The 10-meter walk test (10MWT), 12 6-minute walk test (6MWT) 13 and the Timed Up and Go (TUG) Test 14 were measured before, during and after the study, with and (where possible) without use of the exoskeleton. A more detailed description of these mobility outcome measures is provided in Supplementary Text 1 (available online). Standardised training and assessment of ascending/descending stairs was performed over one flight of 11 steps, 17 cm in height. The total time required for ascending and descending was measured. A 23.5-meter obstacle course was constructed in an outdoor area and involved an inclination of 8°, a gravelled section, four 90° turns around objects and the option to ascend and descend a curb, depending upon the subject’s ability, see Supplementary Figure 1 (available online). The course was timed from start to finish, and any situations requiring assistance were noted.
The SCI-specific Appraisals of Disability: Primary and Secondary Scale (ADAPSS) questionnaire was taken to assess subjects’ appraisal of their individual coping strategy related to their disability. 15 This tool consists of 33 items covering six subscales: fearful despondency, overwhelming disbelief, determined resolve, growth and resilience, negative perceptions of disability and personal agency. Dean and Kennedy demonstrated adequate reliability of the ADAPSS in the SCI population. 15
Finally, the Assistive Technology Device Predisposition Assessment© (ATD-PA) questionnaire was taken to assess subjects’ perceived quality of life in relation to their attitude to assistive devices; 16 the exoskeleton in particular. It consists of two forms, the Person Form (54 items covering (a) functional abilities, (b) quality of life and (c) personal characteristics), and the Device Form which is a 12-item questionnaire covering subjects’ predisposition in using a particular assistive technology using a 5-point Likert scale. The ATD-PA was introduced by Scherer and colleagues who also demonstrated adequate test–retest reliability and internal consistency of the measurement tool. 16 For the current study, the pretraining questions of the ATD-PA Device Form focused on the participants’ expectations of the device. The study end-point questionnaire ATD-PA ‘Device Form’ assessed both the experiences of using the ReWalk™ device during the study, as well as the expectations for hypothetic use of the exoskeleton after discharge in the community.
Since this is a feasibility study, normal power calculations do not apply. A sample size of ten subjects was chosen pragmatically as we aimed to improve our understanding of the variability of effects in patients with various degrees of ambulatory impairment. Data were entered into spreadsheets in Excel (Office 2007; Microsoft) for descriptive analysis.
Results
Recruitment
During a six-month period, a total of 60 individuals contacted the study coordinator to participate in the study. A total of 24 patients (40%) did not meet the study criteria owing to the following reasons: sustained injury too long ago (n = 7), older than the upper age limit (n = 4), other neurological condition than SCI causing paralysis (n = 4), previous use of an exoskeleton (n = 4), higher level of SCI than the upper level limit (n = 4) and concurrent medical issues (n = 1, a fractured femur). While 36 subjects (60%) did meet the study eligibility criteria, 22 candidates (37%) did not consent to participate owing to the following reasons: not willing to commit to the 10-week programme owing to logistical, social and/or financial implications (n = 16), a belief that using the exoskeleton would not provide a long-term benefit (n = 4) and not interested (n = 2, not otherwise specified). Following the screening assessment, four further subjects were excluded owing to pre-existing pressure ulcers in key areas of contact of the exoskeleton device (n = 2), a fixed scoliosis that inhibited the ability to stand fully upright (n = 1) and having sustained the SCI longer than three years before screening (n = 1). A total of ten individuals were included and commenced exoskeleton training sessions.
The mean age of the 50 candidates not enrolled in the study was 37 years, with a range of 18 to 77 years. The most common levels of injury were T6 (n = 7), T10 (n = 5) and T12 (n = 5). A total of 37 (64%) had a motor complete lesion (AIS Grade A and B).
Baseline characteristics and feasibility outcomes
All ten included participants were male with ages ranging from 23 to 43 years, see Table 3. All participants had sustained a traumatic SCI. The levels of injury ranged from C8 to L1; seven participants had a motor and sensory complete SCI (AIS Grade A) and three had an incomplete SCI (AIS Grade C). The time between the onset spinal cord dysfunction and date of screening ranged from 15 months to 21 years.
Baseline characteristics.
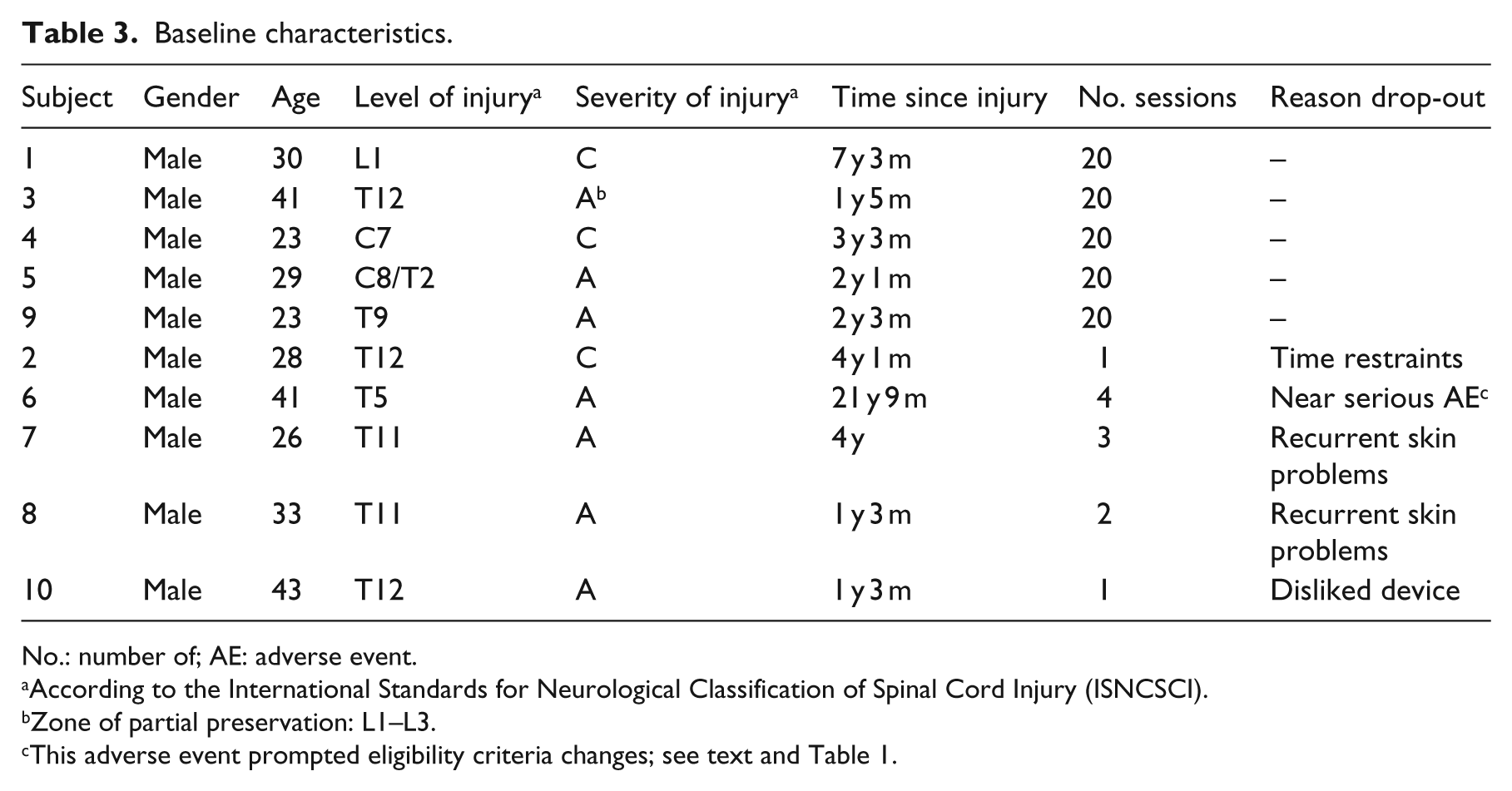
No.: number of; AE: adverse event.
According to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI).
Zone of partial preservation: L1–L3.
This adverse event prompted eligibility criteria changes; see text and Table 1.
Five participants completed the planned training schedule of 20 sessions. Two individuals decided not to continue with the exoskeleton training; one participant experienced time restraints and another participant disliked using the device. Three further participants were precluded from study completion for safety reasons; two participants experienced recurrent skin breakdown problems and another person sustained a near-serious device-related adverse event involving a fractured talus. Apart from a temporarily swollen ankle, which was noticed the morning following the fourth training session, and a hairline fracture of the talus seen on magnetic resonance imaging, no other signs and symptoms were noted. No treatment was necessary, yet a decision was taken to exclude this participant from further exoskeleton use and continuation in the study. This near-serious adverse event, which took place when the study had been underway for three months, prompted the investigators to narrow down the study selection criteria, see Table 1.
Throughout the study, a total of 44 interruptions (i.e. postponements of training session) were noted owing to logistical issues (n = 19), device-related skin aberrations: Grade I (n = 5; in three subjects) and II (n = 10; in five subjects), concurrent medical complications (i.e. urinary tract infections) (n = 5), non-device-related skin problems (n = 2), technical issues with the device (n = 2) and non-device-related – but exacerbated by exoskeleton use – musculoskeletal pain (n = 1). All 15 skin aberrations led to study interruptions; five subjects did not experience skin issues. For those five participants who completed the study, the mean number of weeks taken to achieve 20 sessions was 19 (range 10–31). The average number of completed training sessions before advancing to stairs training was deemed safe and appropriate was 6 (range 3–11).
Clinical observations
Clinical parameters measured before and after each training session are presented in Table 4 and Supplementary Table 1 (available online). For those who completed the training schedule, the average heart rate and systolic blood pressure were higher (+9 beats per minute (BPM) and +4 mm/hg, respectively) and fatigue was more severe (VAS: +1.6) following a training session. While two subjects with mild spasticity experienced a slight improvement after training sessions (Ashworth: –0.71), minimal changes were seen in terms of pain perception (VAS: +0.19), see Table 4. Comparing baseline and final follow-up examination outcomes, 3- and 2-point increases of the lower extremity motor score were noted in subject numbers 3 and 4, respectively. 10 No other neurological changes were noted.
Average individual outcomes and scores of clinical observations taken immediately before and after each training session.
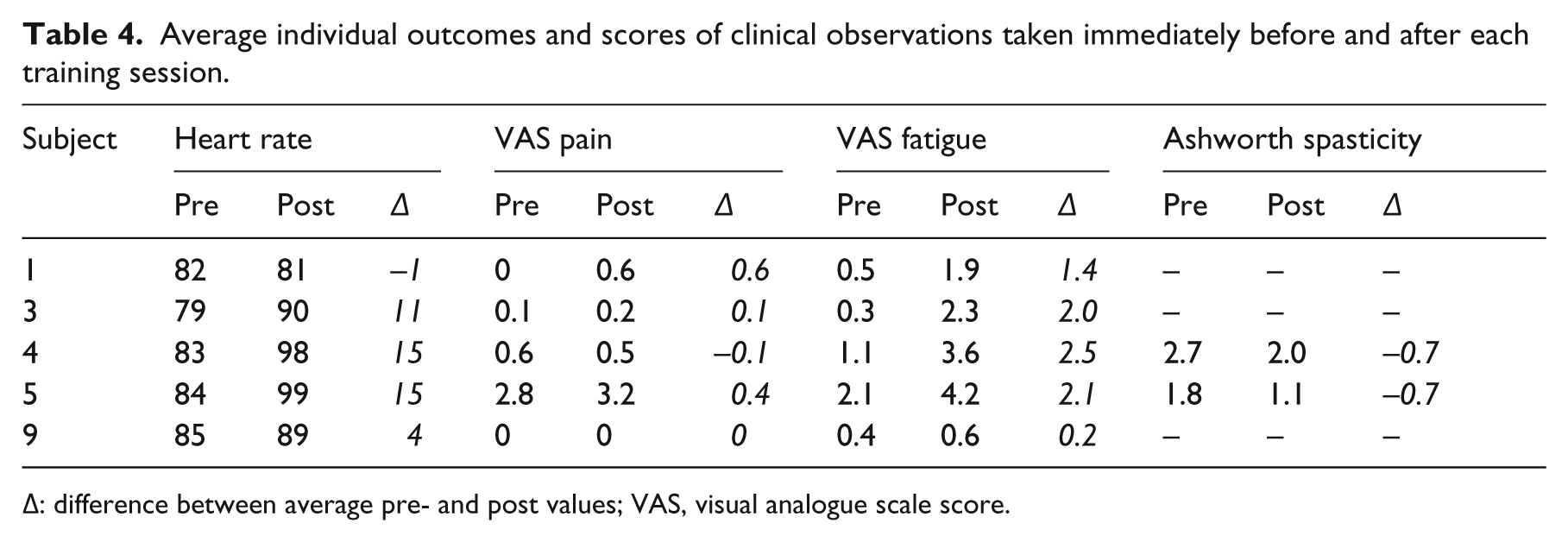
∆: difference between average pre- and post values; VAS, visual analogue scale score.
Mobility outcomes
The individual ambulation test outcomes with and without using the exoskeleton are presented in Tables 5 and Supplementary Tables 2a and 2b (available online). Table 5a demonstrates the progress of participants who completed the scheduled training sessions. Apart from one, all participants showed improved gait speed, were able to walk longer distances and were quicker in standing up, rotating and sitting down after the final training session. Four participants were able to ascend and descend stairs and also managed to complete the standardised obstacle course, see Supplementary Table 2a (available online).
Individual mobility outcomes with (a) and without (b) exoskeleton use. Mid-training and study end-point mobility outcomes were used for assessing differences in mobility outcomes with use of the exoskeleton, whereas pretraining and study end-point mobility outcomes were used for assessing mobility differences without use of the exoskeleton.
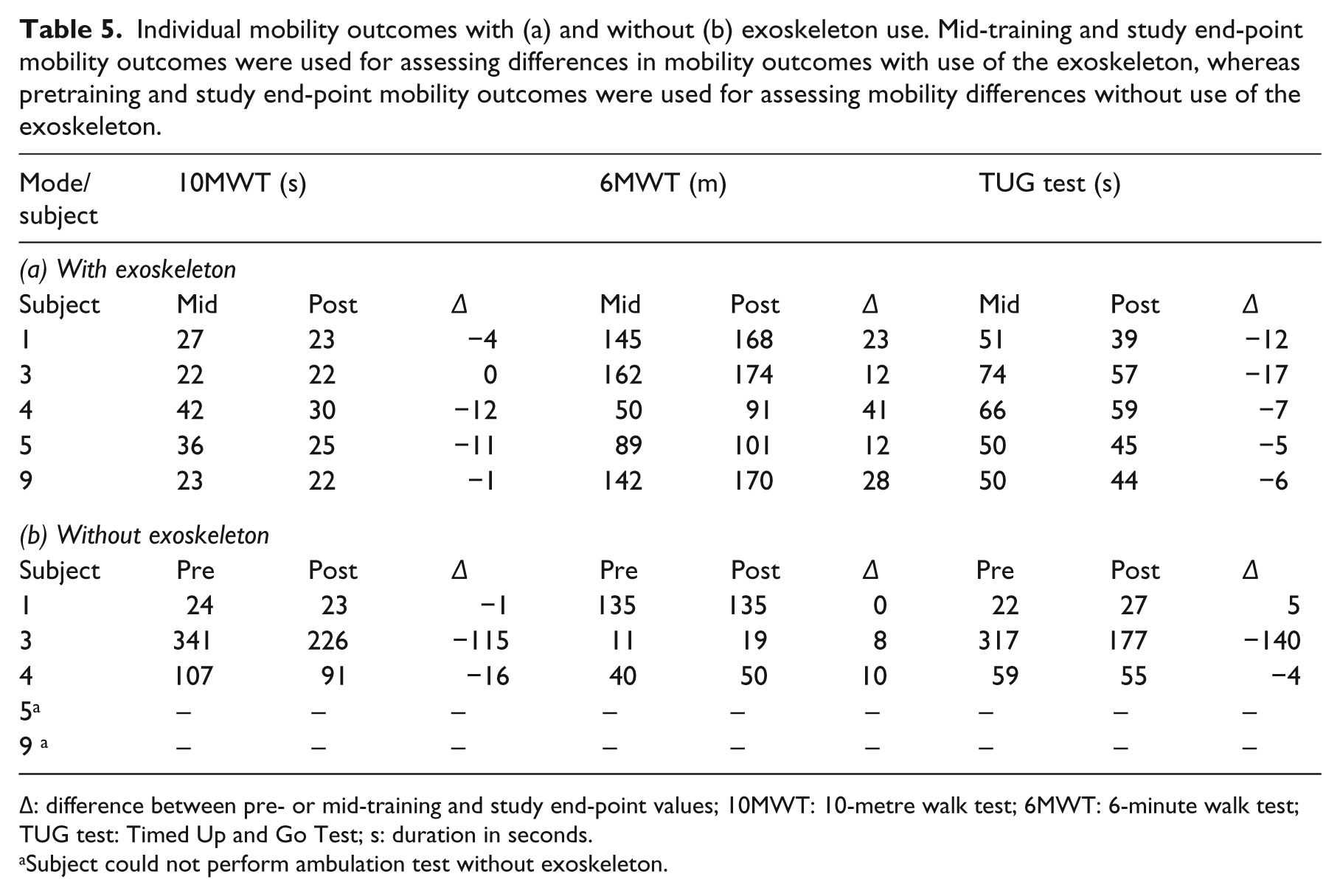
∆: difference between pre- or mid-training and study end-point values; 10MWT: 10-metre walk test; 6MWT: 6-minute walk test; TUG test: Timed Up and Go Test; s: duration in seconds.
Subject could not perform ambulation test without exoskeleton.
While the 10MWT and the TUG tests did not show a clear benefit of using the exoskeleton among the two participants with incomplete lesions, the exoskeleton did enable them to complete an additional 33 and 41 metres distance during the 6MWT, respectively. Two of the three subjects with a motor complete injury were not able to complete the ambulation tests without using the exoskeleton. The other participant (Subject 3) was able to walk without the exoskeleton and showed more pronounced benefits of using the exoskeleton for all mobility outcomes when compared with the two incomplete SCI subjects. All three participants who were able to walk without the exoskeleton also showed improved ambulation outcomes without using the exoskeleton, see Table 5b.
Appraisal of disability and assistive technology
The benchmark values and outcomes of the ADAPSS questionnaire are presented in Table 6 and Supplementary Table 3 (available online). The ADAPSS scores showed considerable differences in appraisal of disability between the participants at onset of the study, as well as a moderate range of higher and lower individual scores (–15 to 11) over time. No remarkable differences were found in the six subscales (data available upon request). No remarkable ADAPSS score differences were seen between those who completed the study and those who dropped out of the study.
Appraisal of disability scores of study participants who completed the exoskeleton training programme (n = 5).
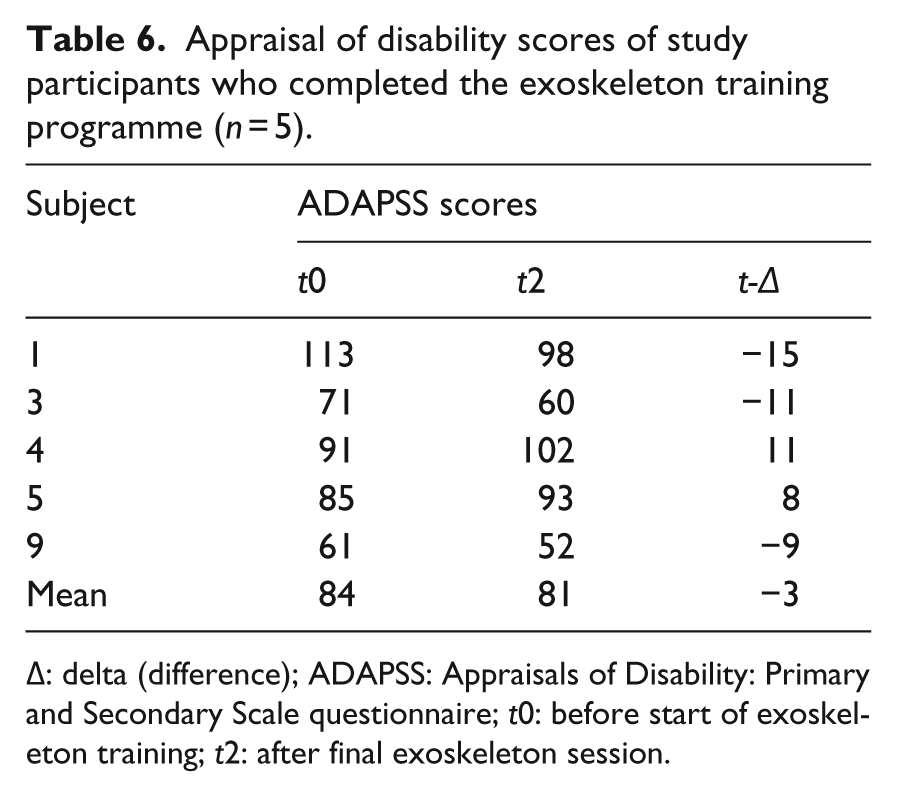
∆: delta (difference); ADAPSS: Appraisals of Disability: Primary and Secondary Scale questionnaire; t0: before start of exoskeleton training; t2: after final exoskeleton session.
The ATD-PA questionnaire outcomes are presented in Table 7 and Supplementary Table 4 (available online). No improvements of functional abilities or personal characteristics subscales were observed. A small mean improvement (+4 points; SD 4.2) was seen in the quality of life subscale. While the average device form score of 41 points indicate that participants initially had positive expectations of using the exoskeleton, not all of these expectations were met as the average study end-point score was 34. With an average device score of 35 points (range 26–56) predisposition scores for hypothetic use of exoskeletons after discharge in the community were equally moderate.
Assistive Technology Device Predisposition Assessment© (ATD-PA) questionnaire outcomes of study participants who completed the exoskeleton training programme (n = 5).
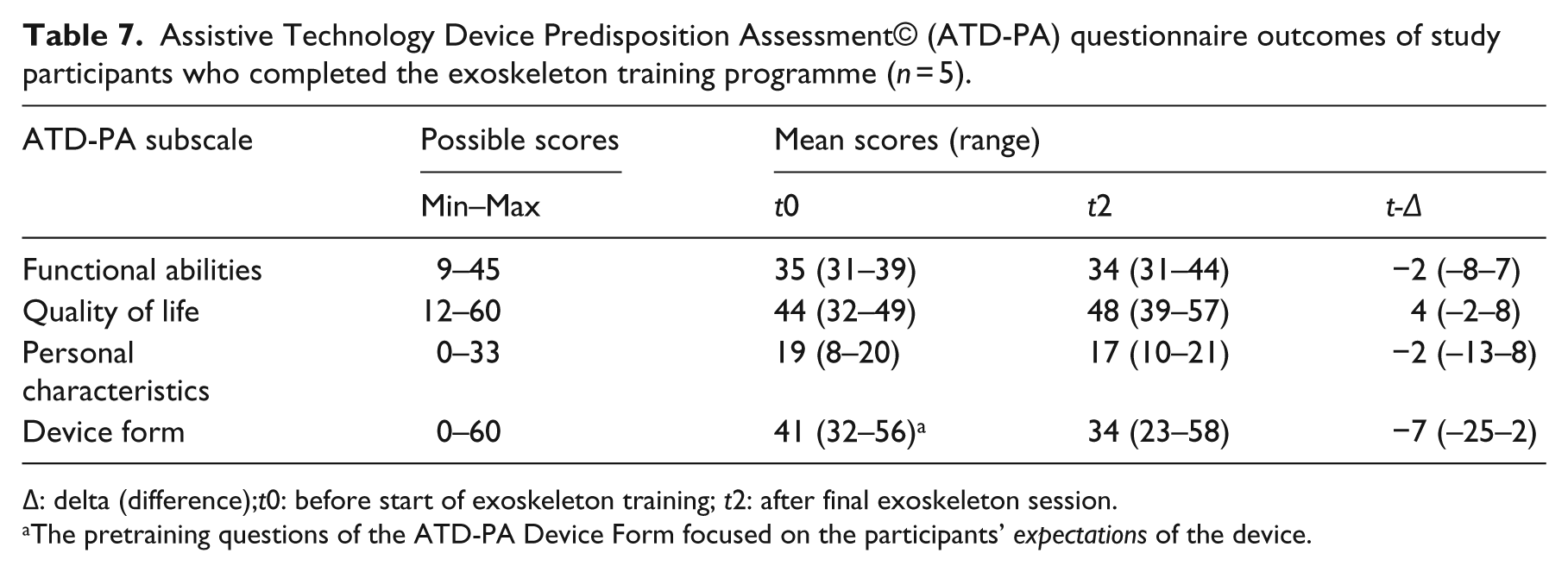
∆: delta (difference);t0: before start of exoskeleton training; t2: after final exoskeleton session.
The pretraining questions of the ATD-PA Device Form focused on the participants’ expectations of the device.
The average expectations of using the exoskeleton among those who did not complete the study (28 points) were lower than those who completed the study (41 points) and showed a strong average decline (–17 points) after reaching the end-point of the study, see Supplementary Table 4 (available online). Finally, equally poor expectations of using the exoskeleton after discharge in the community (average score 12; range 0–33) were documented among those who dropped out of the study.
Discussion
One in every six candidate participants was enrolled, and one in every 12 candidates did complete the training programme. For those who completed the study, we found profound ambulatory capacity improvements among exoskeleton users with complete SCI and subtle ambulatory performance improvements among incomplete SCI exoskeleton users. Nonetheless, the number of device-related skin aberrations was unexpectedly high and use of the exoskeleton generally did not meet subjects’ expectations in terms of perceived benefits and impact on quality of life. This feasibility study has provided some important information on the preliminary benefits and safety of using exoskeletons, which has not been presented in detail in previous studies.5 –9
We experienced great difficulties in recruiting the ten participants with chronic SCI required for this study. Although we acknowledge that our recruitment strategy was not as systematic as it could have been, e.g. we did not query our institutional database, during the design of this study we anticipated that there would have been more eligible study participants than required and that we had to enrol on a ‘first come, first served’ basis. Hence, we used advertisement materials in national ‘SCI niche’ magazines and newsletters, as well as in our outpatient department. A number of exclusion criteria, including further narrowing of selection criteria for safety reasons, and candidates’ prospect of committing to visit our centre twice a week for two-and-a-half months did have a negative impact on the actual recruitment rate.
For the current study, inclusion was restricted to those with chronic (i.e. ⩾12 month post-injury) SCI. The primary justification for this was that since little neurological recovery can be expected after the first 12 months, 17 a self-controlled trial would be a valid approach to assess the effects of using an exoskeleton. The majority of people who have sustained their injury more than a year ago have reintegrated into society. However, community-residing individuals may not be interested in a lengthy user commitment to training, which is required to learn how to use compensating, assistive technology that enables them to walk again. This means that a clear selection bias was observed, as those who are willing to dedicate ten weeks of exoskeleton training have demonstrated their motivation and determination in the first place. Recruiting from an inpatient rehabilitation setting may have led to a reduction, not elimination, of this selection bias and would most likely have resulted in better recruitment rates. However, as a varying degree of ‘natural’ recovery can be expected and a range of other concomitant treatments are being administered – something that has previously been referred to as the ‘black box’ of rehabilitation 18 – it becomes much more difficult to identify the true benefits of using exoskeletons during the early stages of rehabilitation.
All participants who completed the 20 training sessions experienced improved ambulation outcomes using the exoskeleton. As has been documented in previous studies,5,8,9 dramatic improvements in mobility outcomes were seen in subjects with complete SCI using the exoskeleton. It should be noted, however, that the 6MWT, a performance-focused ambulation capacity measure, showed that after the final training session, the walking speed with exoskeleton ranged from 0.25 to 0.48 m/second. Comparable velocities, 0.33 to 0.45 m/second, were found for the 10 MWT. These velocities do not even get close to 1.06 m/second, which is widely regarded as the required velocity to cross a road safely. 19 The authors believe that informing exoskeleton users about the potential, maximal walking speed will help adjusting their expectations and create a clear picture about the potential benefits of using the device. That said, and looking at how quickly ambulatory assistive technology has evolved over the last decade, it is expected that it will not take long until exoskeleton users will become functional and independent walkers. 19
In contrast to earlier reports,5,8,9,20 the current study found a high incidence of skin aberrations when using the ReWalk™ exoskeleton. Five participants experienced at least one mild skin aberration and two of them were withdrawn from the study owing to recurring skin breakdown problems. As individuals with SCI are at high risk of developing pressure ulcers, 21 exoskeleton users should be frequently checked for skin breakdown at every skin-device contact point. Despite applying tailored foam and padding modifications for each individual, the frequency of mild skin aberrations remained high. The current study stresses the importance of aiming to reduce shear forces and friction at skin–device interfaces during further development stages of exoskeletons.
Similarly, further research is required with regard to the use of exoskeletons in subjects with osteopenia or osteoporosis. One subject dropped out of the study as a result of a hairline fracture of the talus. Although this adverse event was not severe, this study highlights that besides the potential positive effects of physical activity on bone structure, risks of developing adverse musculoskeletal effects require careful consideration. Like the study published by Zeilig et al., 9 the current study did not apply bone mineral density (BMD) specific selection criteria. Esquenazi et al. 5 did measure prestudy BMD and excluded those who had a BMD t score of lower than −2; three of 17 subjects were excluded because of severe osteoporosis in the hip and spine. However, there are no consensus guidelines with regard to severity of osteoporosis and recommendations for physical activities in weight-bearing, upright posture. While there seems to be a strong relation between the BMD of epiphyseal trabecular bone and the risk of fractures, 22 others have stated that as forced manoeuvres and falls are the most frequent circumstances surrounding these fractures, a lack of awareness of the early and constant risk for fractures is a key behavioural risk factor. 23 In light of this, it should be realised that the low number of falls and fractures in clinical studies – where users have continuous expert supervision – may underestimate the real risk of adverse musculoskeletal events among exoskeleton users in the community.
The current feasibility study has provided some interesting insight around SCI patients’ priority for regaining their ability to walk. 2 The relatively low recruitment rate prompts further independent investigation into consumers’ perspectives on the use of novel exoskeletons. Such research would clarify at what costs and which anticipated benefits individuals decide whether or not to use new technology. Note that costs are not strictly confined to monetary costs. Physical costs, which include the number, duration and intensity of training and therapy sessions that are required for successful use of exoskeletons, 24 are perhaps even more important parameters to set out against expected risks and benefits of using these devices. Furthermore, more research is required to identify the optimal timing of using exoskeletons. In the current study we selected individuals with chronic SCI. The rationale behind this was to see whether new assistive technology has potential beneficial effects on mobility and quality of life outcomes for those who have been living with SCI for years. Evaluating the effects of using exoskeletons during early rehabilitation, where more attention is paid to detecting neurological and functional benefits, is another area requiring further investigation.
Strengths of our study include the publication and adherence to our study protocol, the detailed reporting of the recruitment process, the use of neurological, functional, as well as quality of life outcome measures and prospective data collection. Nonetheless, several potential limitations of our study exist. A total of 50% of included participants did not complete the training programme, which made clinical and mobility outcomes difficult to interpret. As mentioned, the recruitment strategy could have benefitted from a more structured and systematic approach. No posttraining follow-up assessments were scheduled; this could have provided further information about the longevity of reported mobility improvements of those who were able to walk without the exoskeleton.
In conclusion, primarily owing to endorsed eligibility criteria and the duration of the exoskeleton training programme, considerable recruitment difficulties were encountered during this study. This feasibility study shows that the effort and time study participants will need to commit – as well as the potential benefits of using exoskeletons – will need to be communicated clearly before enrolling in a definite trial. Both subjects with complete and incomplete SCI can benefit from using exoskeletons. Whereas complete SCI users will primarily benefit from the ability to stand up and walk, incomplete SCI users will benefit mostly from the ability to walking longer distances. These differences in walking performance and capacity benefits should be taken into consideration while designing future studies. As we found a relatively high number of device-related skin aberrations, more research is needed to minimise the shear forces and friction at skin-device interfaces of exoskeletons. This study highlights both the importance of careful selection of exoskeleton users and the vigilance required to prevent and detect medical complications in clinical trials and practice.
Clinical messages
This feasibility study reported more adverse events when compared with previous studies; the clinical implications of these complications warrant further investigation.
The effort and time commitment needed leads many patients to decline even being involved in using lower-limb exoskeletons. Informing candidate users about the efforts required and potential walking speed that can be reached will help managing their expectations.
Patients with complete injuries seem to benefit mostly from exoskeletons, although users with incomplete lesions may equally benefit from using exoskeletons for walking longer distances.
Footnotes
Acknowledgements
We thank Wen Li and Foteini Mavrommati for their assistance throughout the conduct of the research project.
Conflict of interest
No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript. The authors have no financial interest in the subject of this article.
Contributors
JJvM drafted the study protocol. IB, KH and DT contributed to the design of the study protocol. IB coordinated the conduct of the study. IB and JJvM analysed the results. IB drafted the manuscript. KH, DT and JJvM co-authored the writing of the manuscript. All the authors read and approved the final manuscript.
Funding
Charitable donations were received from the Stoke Mandeville Spinal Research for staffing costs required for the conduct of the study. Cyclone Technologies UK provided technical support throughout the study free of charge. Argo Medical Technologies Ltd, (Yokneam Ilit, Israel) provided an exoskeleton for the duration of the study free of charge.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.