
Abstract
Objective:
To evaluate the effect of very early mobilisation on functional status following acute stroke.
Design:
Single blind, randomized controlled trial.
Setting:
University hospital.
Subjects:
Eighty-six patients with acute stroke (42 men and 38 women) aged 30-80 years were randomized to an Intervention group and a Standard care group.
Interventions:
All participants received 45 minutes standard care once a day for seven days. In addition, the intervention group (n=43) performed very early mobilisation consisting of early and frequent out of bed activities which started within 24 hours of stroke onset for 5 to 30 minutes at least twice a day, for seven days.
Outcome measures:
Functional status was measured with Barthel ADL Index on admission, discharge and three months follow up.
Results:
Intervention group showed a significant improvement in Barthel Index change scores (discharge - admission) (median=35, IQR=30-38.75 versus median=17.50, IQR=10-30) than the standard care group. Intervention group showed a significant improvement in Barthel Index change scores (three month follow up - admission) (median=42.50, IQR=35-55) versus (median=30, IQR=20-35) than the standard care group. The Intervention group reported statistically significant improvement in functional status at discharge (P<0.001) and at three months follow up (P<0.001) compared with the Standard care group.
Conclusions:
The results indicate that very early mobilisation in addition to the standard care may be effective in improving the functional status following acute stroke.
Keywords
Introduction
Early and intensive rehabilitation is one of the important components of acute stroke care units, which may be associated with better and quicker improvement of the activities of daily living performance.1,2
Very Early Mobilisation is defined as an intensive out of bed activity of daily living (ADL) within the first 24 hours of symptom onset. 3 Initial results from the ongoing AVERT (A Very Early Rehabilitation Trial) reveal that, a very early and frequent mobilisation reduces medical complications (i.e. pneumonia, contracture formation, deep vein thrombosis, bedsore and constipation) and physical disability.4,5,6 A recent Cochrane review has reported that there is no adequate evidence whether mobilisation within 48 hours after stroke is effective or harmful? 3
Two randomized controlled trials indicate that very early mobilisation appears safe, feasible, easy to deliver and reduces the length of stay in the hospital. Furthermore, it is potentially deliverable to 85% of the acute stroke population.7,8 However, very early mobilisation had had a nonsignificant summary effect size (SES) on independence in the activities of daily living at three months, following an acute phase of stroke. Furthermore there are ambiguities over the timing of initiation of mobilisation, intensity, frequency, cost, benefits and harms.9,10
The objective of this single-blind, randomized control trial was to evaluate the effect of very early mobilisation in addition to standard care on the functional status following an acute stroke.
Methods
The study was a single blinded, randomized controlled trial with a blinded assessment at the end of the follow up. This study was conducted at the stroke unit of the Department of Neurology and Medicine of the University Teaching Hospital in Mangalore, India. The stroke unit was staffed by a neurologist, general physician, nursing staff, physiotherapist team, a speech therapist and a dietician.
The patients included were above 18 years. Acute stroke patients were admitted within 24 hours of the symptom onset in the stroke unit. They were able to react to verbal commands, both the sex, systolic blood pressure between 120 and 180 mm Hg, an oxygen saturation >92% (with or without supplementation), a heart rate between 40 and 100 beats per minute, with temperature <38.5○C. The patients were recruited after obtaining physician permission to mobilisation within 24 hours of stroke.
Patients were excluded if the condition deteriorated within the first hour of admission to the hospital (National Institutes of Health Stroke Scale 11 (NIHSS)). Pre morbid modified Rankin Scale 12 (mRS) Score>3, transient ischemic attacks, concurrent progressive neurological disorder, unstable coronary condition (e.g. acute myocardial infarction) or other medical condition that would impose hazard to the patient, or if their physiological variables (blood pressure, oxygen, heart rate, temperature) go beyond set safety limits, severe heart failure, lower limb fracture preventing mobilisation, as well as those patients having terminal cancer.
Stroke patients were randomly allocated equally to either the Intervention group (Very Early Mobilization out of bed within 24 hours of stroke onset) or the Standard care group by the computer generated, randomization procedures using a concealed opaque envelop method. This randomization list was held by a university researcher who was not related to any part of the study.
The Intervention group received the Very Early Mobilisation and the Standard Care treatment, the mobilisation was started (upright and out of bed activities) as soon as practical after the recruitment, which aiming to have first mobilisation within 24 hours of the onset of the symptoms. The time spent on early and frequently out of bed activities was determined by the patient’s tolerance (5-30 minutes), and they received mobilisation minimum two times per day for seven days or until the discharge whichever was sooner. (We adopted the ‘A Very Early Rehabilitation Trial’(AVERT) Protocol). 4,5,7,8
The Intervention group received the following activities: Sitting supported in bed, sitting unsupported out of bed, transfer along with assistance, roll and sit up, sitting without support, transfer feet on the floor, standing activities, walk- early gait, and advanced gait activities.
Patients in the Standard care group, received routine stroke unit care, including the passive and active (if possible) mobilisation, correct positioning in bed, mobilisation in bed, sitting balance activities, facilitation of limb and trunk control activities, education of patient and caregiver. Both groups received standard care treatment, for 45 minutes a day, for seven days or until discharge.
Patient baseline characteristics were collected at the beginning included age, sex, and stroke (side, type, severity as per the National Institutes of Health Stroke Scale) 11 risk factors (Hypertension, Diabetes mellitus, Cardiovascular disease, Smoking, Alcoholics); pre morbid disability 12 (as per mRS);Outcome measures (length of hospital stay and time to first mobilisation after symptom onset).
Outcome measures
Barthel index measurement was used to assess functional status.13,14 The measurements were taken at the admission as a baseline, at the end of seven days or at discharge (whichever was earlier). The follow up was carried out at the end of three months following the onset of stroke. The outcome measurements at three months follow up were taken directly by the blinded assessor when the patients visited the hospital for a routine medical check-up.
Ethics
The study was approved by the Central Ethical Committee of the Nitte University (Ref: NU/CEC/Ph.D-52/2012). Informed consent was obtained from all patients, or their representatives at the beginning of the study. No adverse events associated with participation in the study were observed.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Science (SPSS), version 16.0 (SPSS Inc., Chicago, IL, USA). 15 Significance level was set at P <0.05.
Descriptive statistics were used to analyze all demographic and clinical characteristics. Continuous data were presented as mean (standard deviation) and categorical data were presented as number and percentage. Since ordinal measurements (Barthel Index) were used, data were presented here as median and inter quartile range (IQR). Non-parametric analysis of the intra group scores comparison on admission, at discharge, and at the end of 3 month follow up for Barthel Index measurements, were analysed by the Wilcoxon signed rank test and the Mann-Whitney U test was used to identify any significant differences in the Barthel Index measurements between the two groups.
Sample size
A pilot randomized control study was conducted among 20 subjects. The pooled mean (38.7) and standard deviation (11.2293) of Barthel Index were obtained. The sample size was calculated along with these estimates for the effect of interest and the variability. A total of 43 patients were needed for each group with a two sided significance of 0.05 (alpha 5%) and a power of 0.8 (80%). 16
Results
Recruitment and participant flow chart is represented in Figure 1. A total of 140 stroke patients were screened for eligibility during the period of March 2012 to September 2014. The Table 1 summarizes the demographic and clinical characteristics and outcome measures, which were equivalent in the two groups except two outcome measures, time to first mobilization after the symptom onset was median 18 hours (IQR 16.62 to 19.75) in the Intervention group and a median 30.5 hours (IQR 29.0 to 35) in the Standard Care group (P<0.001). And the length of the hospital stay was median of 8 days (IQR 7 to 9) in the Intervention group and a median of 10 days (IQR 8 to 12.75) in the Standard care group (P<0.001).
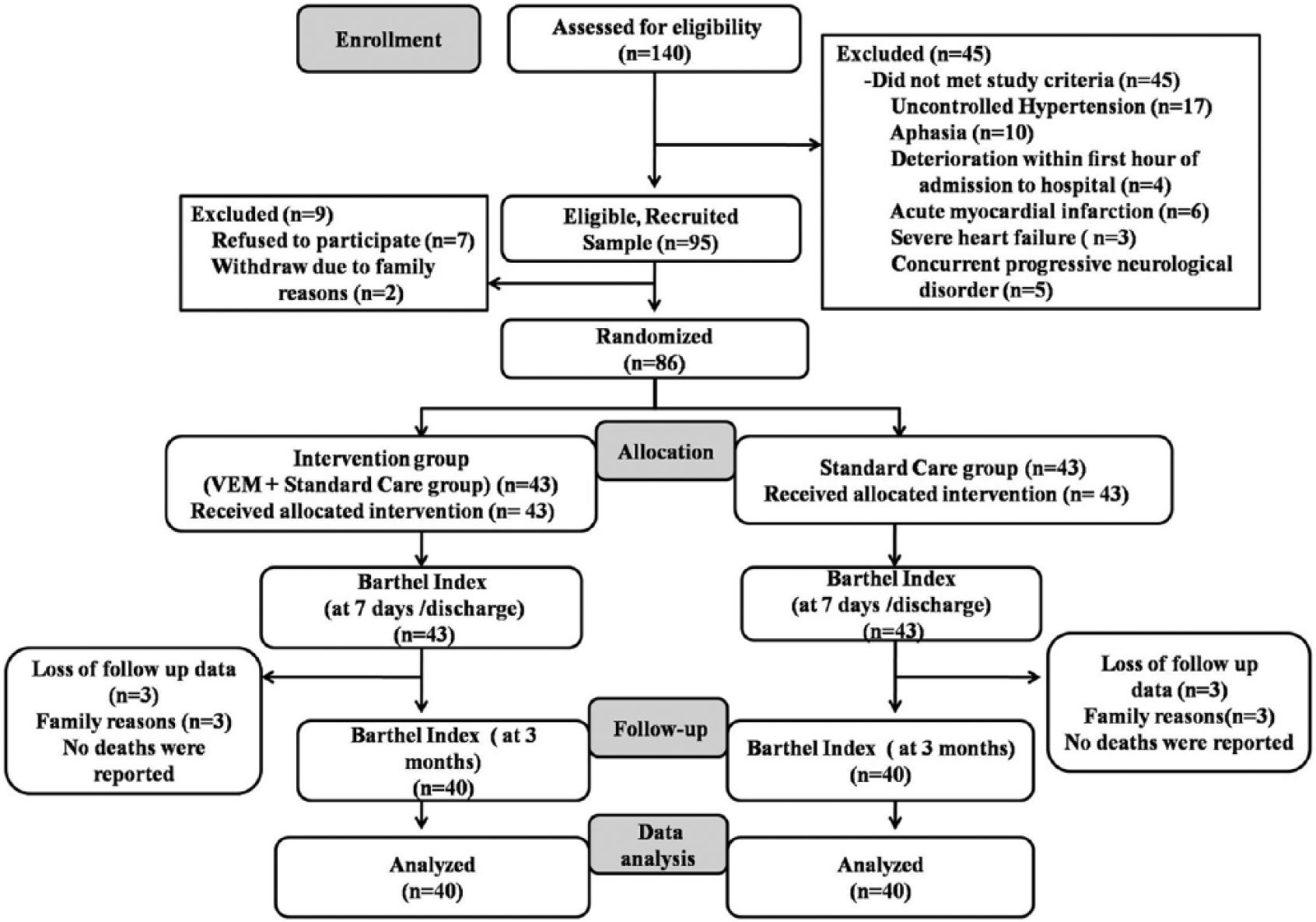
Participants flow chart.
Demographic, clinical characteristics, and outcome measures of recruited patients.
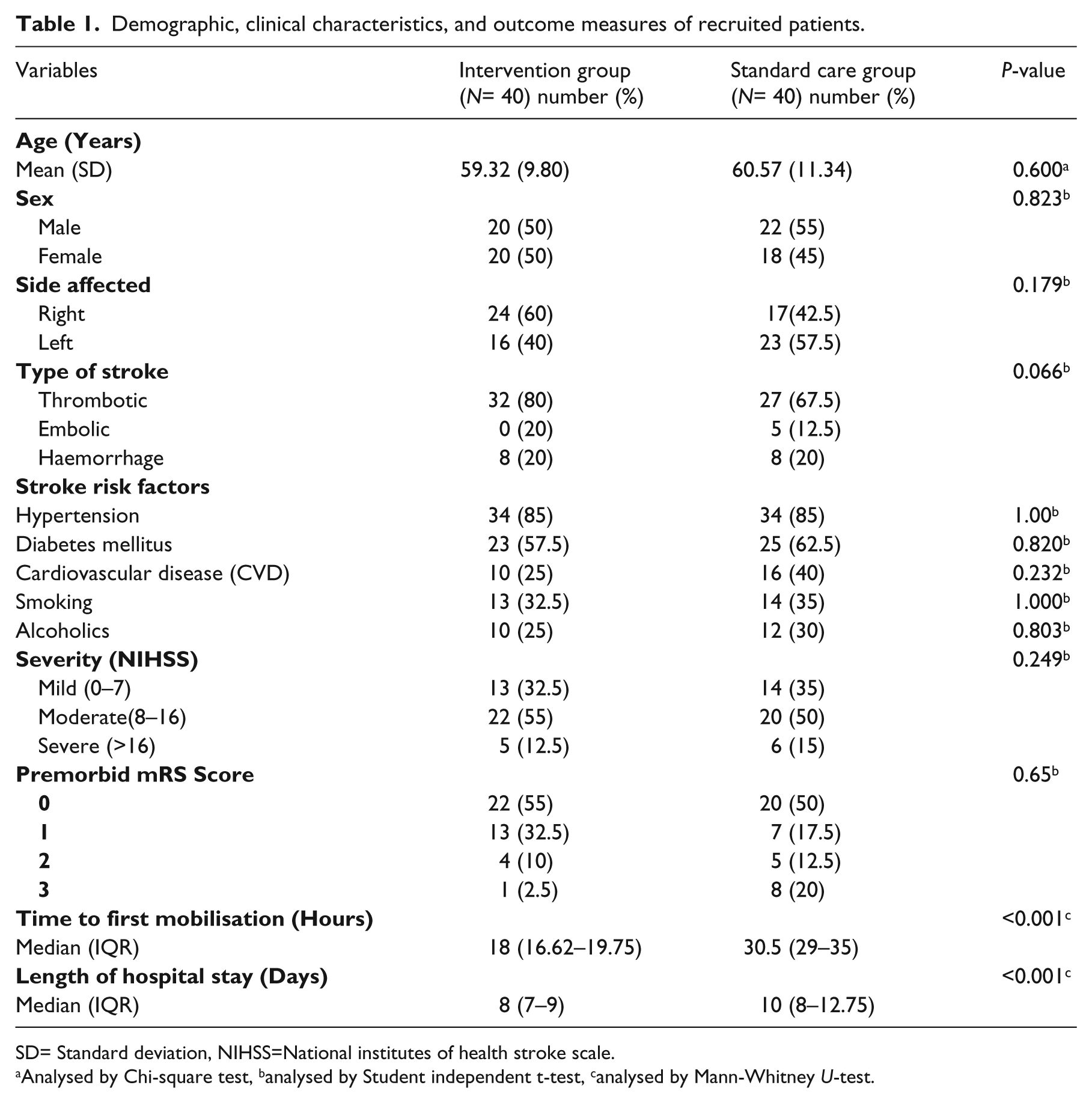
SD= Standard deviation, NIHSS=National institutes of health stroke scale.
Analysed by Chi-square test, banalysed by Student independent t-test, canalysed by Mann-Whitney U-test.
Eighty-six patients (mean age = 59.95 years, SD = 10.55, range = 30–80 years) were randomized into two groups with equal number (43) in each group. There were six dropouts three in each group due to family reasons at the end of 3 months follow up and they were excluded in the final analysis (Figure 1) and no deaths were reported.
Table 2 shows descriptive and inferential statistics of Barthel Index scores on admission, at discharge and at three months follow up for intervention group and standard care group. Difference (at discharge - at admission) in Barthel Index scores were found high for the Intervention group (median=35, IQR=30-38.75) than the Standard care group (median=17.50, IQR=10-30) and difference (three month follow up - at admission) in Barthel Index scores were found high in the Intervention group (median=42.50, IQR=35–55) than the Standard care group (median=30, IQR=20–35). The Intervention group reported statistically significant improvement in functional status at discharge (P<0.001) and at three months follow up (P<0.001) compared with the Standard care group.
Comparison of Barthel Index Score measurements (changes scores of within- group and between- group comparisons).
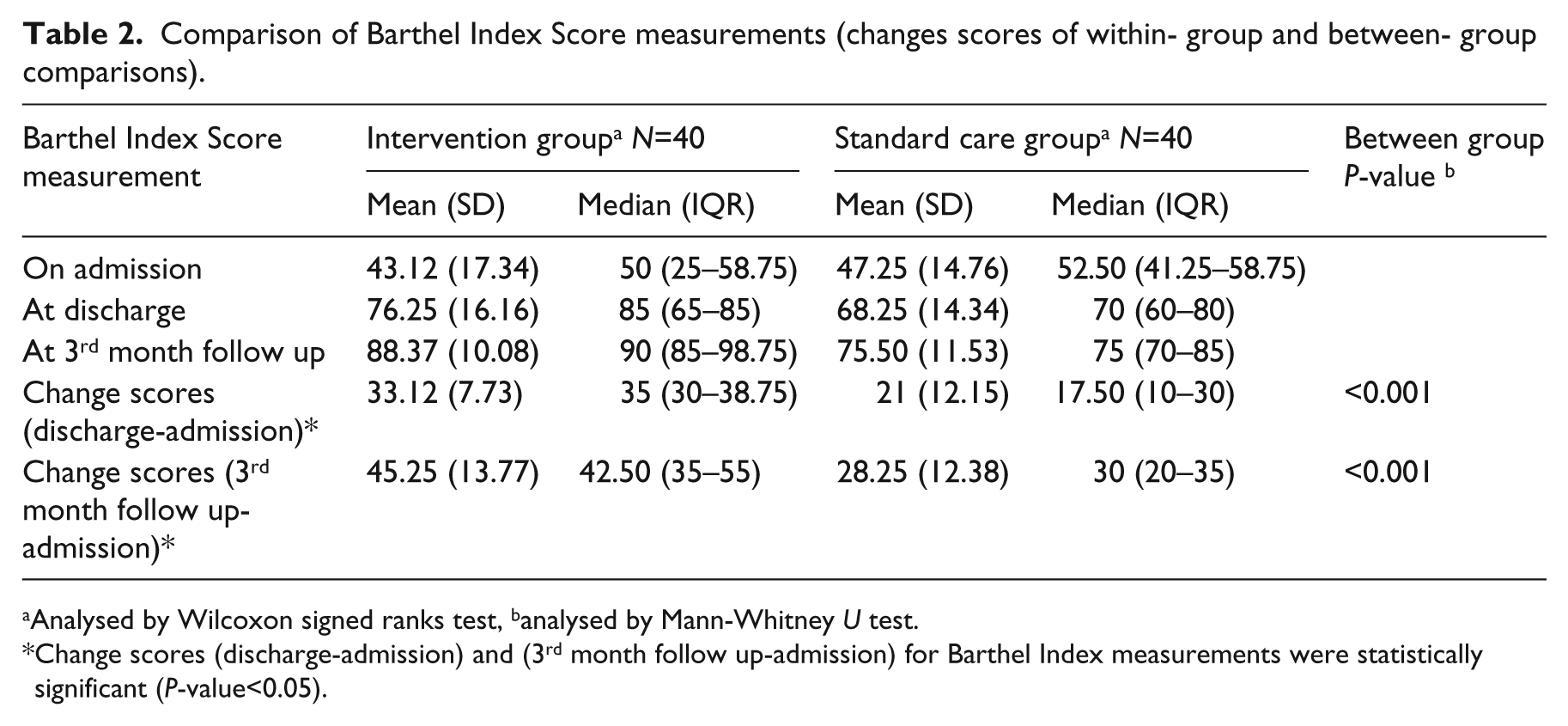
Analysed by Wilcoxon signed ranks test, banalysed by Mann-Whitney U test.
Change scores (discharge-admission) and (3rd month follow up-admission) for Barthel Index measurements were statistically significant (P-value<0.05).
Based on Barthel Index scores at discharge, 70% (28 of 40) of the patients in the Intervention group were independent in activities of daily living compared to 32.5% (13 of 40) of the Standard care group (P <0.01). At 3 months follow up 85% (34 of 40) patients of the Intervention group were independent in activities of daily living compared to 45% (18 of 40) patients in the Standard care group (P <0.01).
Discussion
The results of this single-blind, randomized controlled trial showed that very early and frequent mobilisation accelerated the return of the activities of daily living following acute stroke.
The findings of the present study go along with the study conducted by Cumming et al., 5 who did a randomized controlled trial study and found that the very early mobilisation group, 47% (17 of 36) of patients had a better effect on the functional ability measured in the Barthel Index at the end of 3 months compared to 28% (9/32) of Standard Care patients (P=0.136).
The findings of the present study contrast with studies conducted by Bernhardt et al., 7 Langhorne et al., 8 where they found that very early mobilisation had a nonsignificant summary effect size (SES) on independence in activities of daily living at three months, following an acute phase of the stroke.
The current randomized control trial is different from AVERT protocol, which is a multi center, large sample size, with stratified randomization and the study duration is fourteen days. 4 Current study was a single centered study, where a simple randomization method was used to allocate the recruited participants. The total duration of study was seven days or until discharge, whichever was earlier. The follow up was made up to three months of post stroke and data was analyzed by a person blinded to randomization and intervention.
The strength of the current study is its randomized, controlled design with a single blinded assessment at the end of follow up, notwithstanding the small sample size of the present study. Statistically significant and clinically applicable results were observed during the study.
The limitations of this study are that the patients recruited were not representatives of the whole stroke population (patients with severe aphasia were excluded). Low power and longer follow up were not undertaken. Upcoming studies may also benefit from larger sample sizes which would increase the generalizability of the results. Further, it emphasizes the need for multi center, larger randomized controlled trials that would address the effect of early mobilisation within 24 hours, such as the ongoing AVERT Phase III.
The results of the current randomized clinical trial suggest that very early mobilisation along with standard care may improve the functional status following acute stroke.
Clinical messages
Very early mobilisation in addition to the Standard care started within the first 24 hours after stroke is associated with a better level of function in activities of daily living at three months follow up.
Footnotes
Acknowledgements
We would like to appreciate all of the stroke survivors and their family members who participated in this study. The authors would like to acknowledge the support of the clinical staff at the KS Hegde Charitable Hospital, Mangalore, Nitte University, Darsana N for assistance in data collection, Ancy for assistance in manuscript review. We would like to thank and appreciate Professor Derick Wade, for his support and valuable guidance on manuscript revision. We also would also like to thank Dr. Sanal, PhD. for statistical analysis.
Conflict of interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.