
Abstract
Objective:
To explore the impacts of social participation and the environment on depression among people with stroke.
Design:
Cross-sectional survey.
Setting:
Structured interviews in the participants’ homes.
Subjects:
Community-dwelling persons with stroke in the rural areas of China (N = 639).
Interventions:
Not applicable.
Main measures:
Depression (Hamilton Rating Scale for Depression-6), activity and social participation (Chinese version of the World Health Organization’s Disability Assessment Schedule 2.0), environmental barriers (Craig Hospital Inventory of Environmental Factors), neurological function (Canadian Neurological Scale).
Results:
A total of 42% of the variance in depression was explained by the environmental barriers, neurological function, activity, and social participation factors studied. Social participation, services/assistance, and attitudes/support were directly related to depression; their standardized regression coefficients were 0.530, 0.162, and 0.092, respectively (p ⩽ 0.01). The physical environment, policies, and neurological function indirectly impacted depression. Depression influences social participation in turn, with a standardized regression coefficient of 0.29 (p ⩽ 0.01).
Conclusions:
Depression and social participation are inversely related. The physical environment, services/assistance, attitudes/support, and policies all impact post-stroke depression.
Keywords
Introduction
Depression is a frequent mental consequence of stroke, and it can contribute to poor quality of life, high mortality, and severe disability among persons with stroke.1,2 Despite this, post-stroke depression often remains unrecognized and poorly addressed. 3 The factors related to post-stroke depression have, however, been widely studied. The risk factors can be classified as socio-demographic characteristics (female, young, higher education level, living alone, lower income),4,5 stroke characteristics (stroke type, lesion location), 6 personal characteristics (low self-esteem, poor coping strategies, perceived stress),7,8 functional disability (dependence in activities of daily living (ADL), cognitive impairment, pre-stroke depression),2,4 and environmental factors (social support, living facilities).4,9
Compared with other factors, the impacts on depression of the environment (apart from social support) and social participation have been less frequently the focus of research, despite the fact that they have been emphasized in the International Classification of Functioning, Disability and Health (ICF). 10 A core concept of the ICF is that an individual’s functioning is determined by an interaction of health status with contextual factors (environmental and personal factors). 10
The ICF classifies health and the factors related to health into four components – body structure and function, activity and social participation, environmental factors, and individual factors – and assumes that the four components interact and are inter-related. 10 This is a powerful theoretical proposal that needs further testing. For persons with stroke, their functional disorders should, at least, involve cognitive, neurological, and mental dysfunction, along with activity limitation and social participation restriction.
Correlations between environmental barriers, activity, and social participation have been explored in the Chinese context, and the findings suggest that the physical environment and the services and assistance available are greater obstacles to social participation for persons with stroke in the rural areas of China than attitudes, support, or policies. 11 This study was therefore designed to explore the impacts of environmental barriers and social participation on depression among persons with stroke. To exclude the effects of confounding factors, neurological functions and activity that have been proved to be main factors impacting depression were included in the study. 2 The study tested the hypothesis that environmental factors – physical, social, and attitudinal – can directly or indirectly influence depression and social participation, and that the latter two variables interact.
Methods
This cross-sectional study was conducted between September 2013 and June 2014 in China’s Guangdong Province. Multistage cluster sampling was used. A stratified convenience sample of persons with stroke was drawn by first selecting six counties in the east, west, north, mountainous, and Pearl River delta areas of the province. In each county, five townships were selected randomly and convenience samples were drawn from 4–8 villages in each township based on the number of persons with stroke in each village. In total, six counties, 30 townships, and 202 administrative villages were sampled. All the persons with stroke in the sampled village were surveyed. The sampling method has been described in more detail in another article. 11
The inclusion criteria were as follows. (1) The subject had been told by a doctor that they had suffered a stroke more than three months previously. (2) They lived at home. (3) They were able to communicate at least with family members. And (4) their intellectual ability was within the normal range (Abbreviated Mental Test score ⩾6). 12
Ten trained postgraduate students in rehabilitation or nursing collected the data. All of the physicians working in the sampled villages were invited to participate in the research. They were familiar with the participants living in their villages and were responsible for screening persons with stroke and introducing the investigators. After obtaining consent, the investigators surveyed each participant at home. In case the investigator could not understand the participant’s dialect, a translator (a family member or the village physician) was involved. The interviews lasted 20–60 minutes depending on the participant’s condition. The average number surveyed per day was 30 by 10 investigators.
The study protocol was approved by the Ethics Committee of the School of Nursing of Sun Yat-sen University. Informed consent was obtained from all the participants. The literate participants signed their consent forms themselves, but the illiterate needed one of their family members to sign on their behalf. If no family member could sign, such as the participant living alone or having no family, the village physicians signed as a witness to the consent (this was one of the demands of the Ethics Committee).
Measures
Depression was evaluated using the Hamilton Rating Scale for Depression-6 (HRSD-6). 13 It covers depressed mood, guilt, work and activities, psychomotor retardation, psychic anxiety, and general somatic symptoms, which were sensitive to ‘core’ depression symptoms. The total score ranged from 0 to 22. A higher score denotes more serious depression. A structured interview guide proposed by Williams 14 and Potts et al. 15 was used in order to maintain consistency among the raters.
Activity and social participation were measured with the Chinese version of the World Health Organization’s Disability Assessment Schedule 2.0 (WHODAS 2.0). 16 It covers understanding and communicating (six items), getting around (five items), self-care (four items), getting along with others (five items), life activities (four items), and participation in society (eight items). Complex scoring was involved in calculating a composite DAS 2.0 score. 16 The values ranged from 0 to 100, with a lower score denoting better activity and social participation. Activity and social participation were analysed separately in this research, with the first three domains classified as activity and the latter three domains representing social participation. The reliability and validity of WHODAS 2.0 has been demonstrated in other studies. 17
Environmental barriers were measured using the Craig Hospital Inventory of Environmental Factors (CHIEF-15). 18 The CHIEF includes five domains, but only four of them were used in this study: Physical/structural barriers (four items), attitudinal/support barriers (three items), barriers to services/assistance (six items), and policy barriers (two items). The Chinese version of the CHIEF has been validated in Hong Kong. 19 The Cronbach’s α coefficient showing the internal consistency of the CHIEF was 0.889 and the test–retest reliability was from 0.515 (for work/learning) to 0.800 (for the total score). 19
Neurological function was evaluated using the Canadian Neurological Scale (CNS), 20 which was designed to assess neurological impairments after brain injury. The scale encompasses eight items assessing the level of consciousness (one item), orientation (one item), aphasia (one item), and motor strength (five items). The total score ranges from 0 to 11.5. A lower score denotes more serious impairment.
Data analyses
The statistical analyses were conducted using version 19.0 of the SPSS software suite (SPSS Inc., Chicago, IL) and Amos 17.0 for structural equation modelling. A structural equation model (SEM) could be defined as ‘a class of methodologies that seeks to represent hypotheses about summary statistics derived from empirical measurements in terms of a smaller number of structural parameters defined by a hypothesized underlying model’. 21 The first step building a SEM is to form a graphical depiction showing how the various concepts fit theoretically together. Then data were collected and variables were chosen that represent the theoretical constructs of interest. Finally, model parameters were estimated and tested, as was the overall fit of the model. The frequently used indices showing whether or not the theoretical model is fit to the data including the ratio of Chi-squared to the degrees of freedom (CMIN/DF), the adjusted goodness of fit index (AGFI), the comparative fit index (CFI), and the root of the mean squared error of approximation (RMSEA).
SEM represents a melding of factor analysis and path analysis into one comprehensive statistical methodology. 21 Modelling systems of structural relationships between a set of observed variables is often referred to as path analysis. Factor analysis is used to measure the underlying constructs. In the models of this report, activity and social participation were the underlying constructs that were measured by six indicators (Figure 1(a) and (b)).
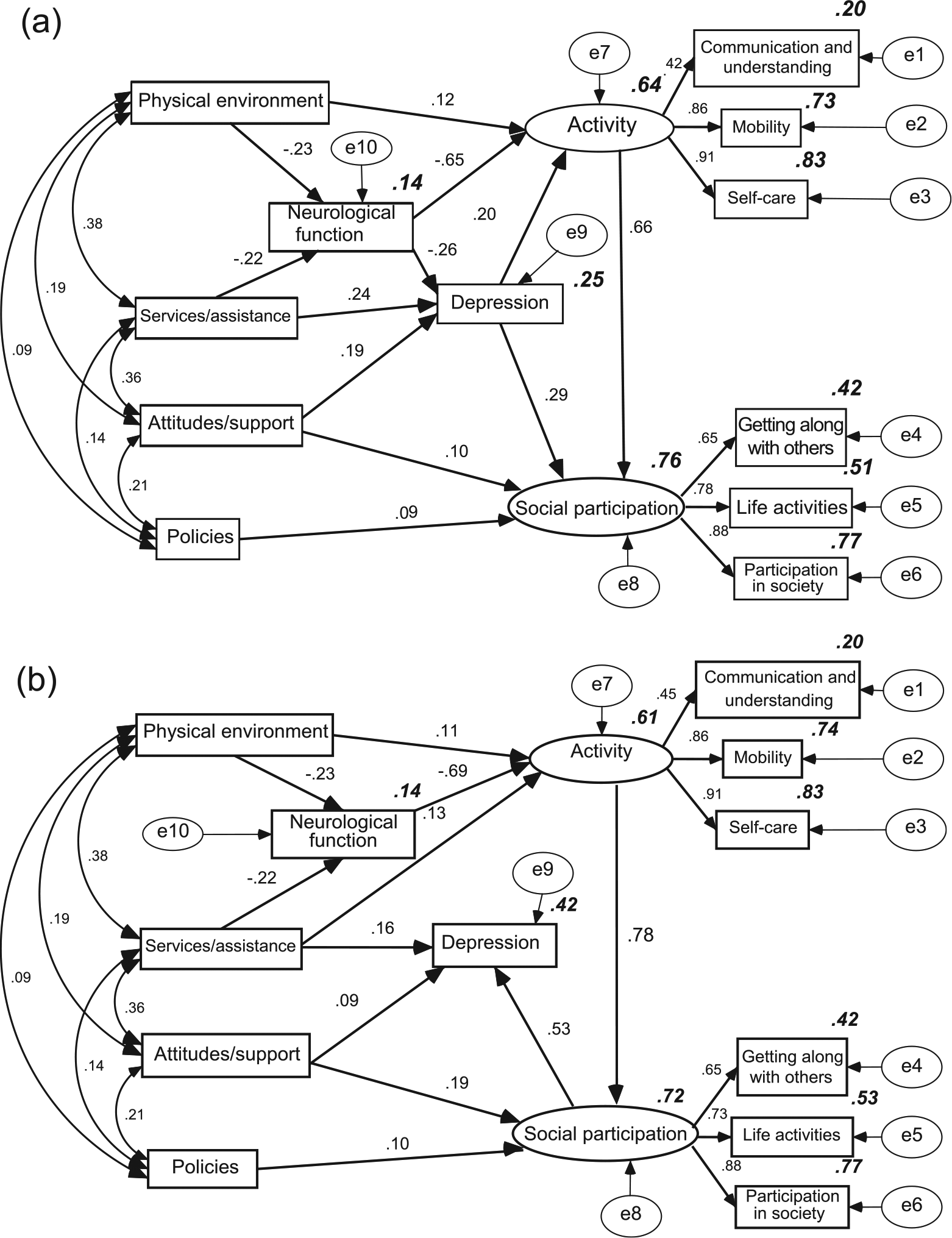
The SEM showing the associations of the main variables of this study. (a) SEM with social participation as the final dependent variable. (b) SEM with depression as the final dependent variable.
In this report, two SEMs were mapped. One had social participation as the final dependent variable; the other modelled depression. The estimation of the model parameters used maximum likelihood estimation. The standardized regression coefficients, determination coefficients (R squared), and total effects were estimated (Amos can calculate these parameters; we introduce them in detail in the legend of Figure 1).
Results
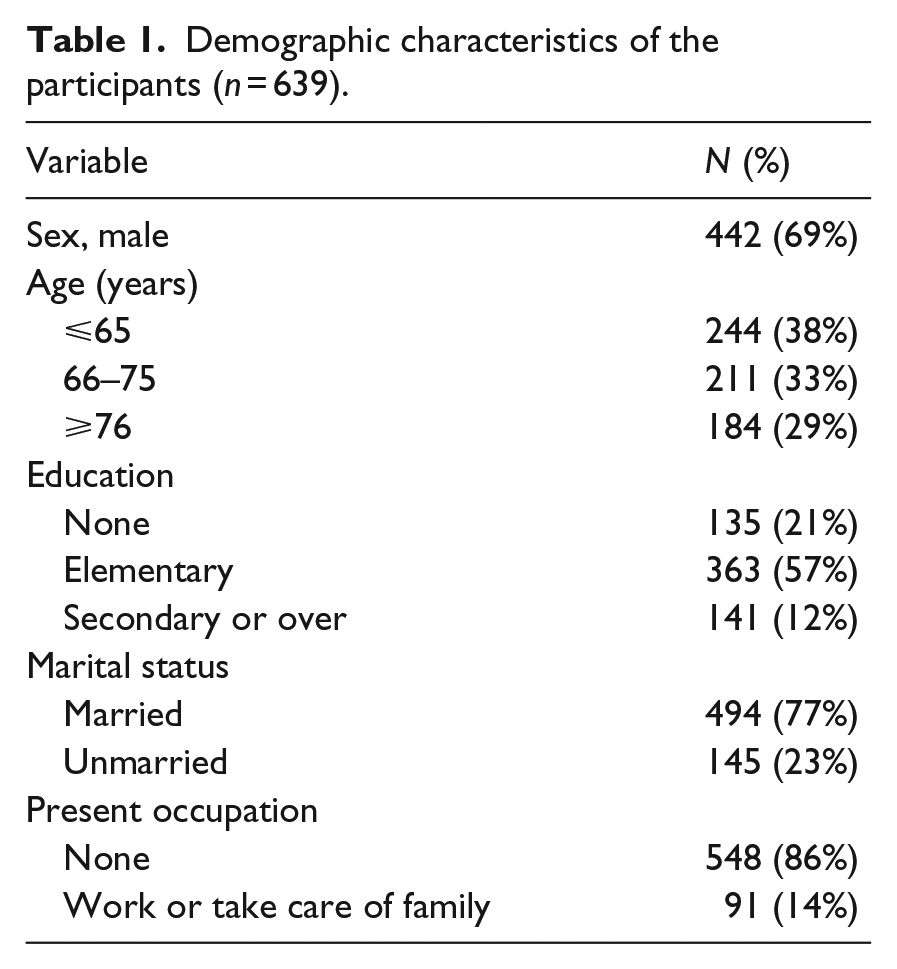
Altogether 656 participants were surveyed. The questionnaires of 17 participants were deemed invalid, so data for 639 participants were included in the analysis. The personal characteristics are shown in Table 1. A total of 81% of the participants (n = 515) were first-ever stroke survivors, 70% (n = 449) had suffered a stroke more than 2 years previously, 69% (n = 440) had suffered an ischemic stroke, and 74% (n = 472) displayed the comorbidity of hypertension.
Demographic characteristics of the participants (n = 639).
Each of the selected variables was found to be significantly directly or indirectly related to social participation (p ⩽ 0.01 in each case) (Figure 1(a)). Among them, depression (the standardized total effect of depression on social participation was 0.418) ranked as the third most influential factor behind activity (0.658) and neurological function (–0.538). Depression was a mediating variable, which was influenced by environmental factors and neurological function, and impacted activity and social participation (Figure 1(a)).
When social participation was treated as an independent variable predicting depression, 42% of variance in depression was explained by the factors directly related to depression, which involved social participation, services/assistance, and attitudes/support (Figure 1(b)). Their standardized regression coefficients were 0.092 for attitudes/support, 0.162 for services/assistance, and 0.530 for social participation (p ⩽ 0.01 in each case). According to the standardized total effects, the factors influencing depression were, in descending order, social participation, activity, neurological function, services/assistance, attitudes/support, the physical environment, and policies (Table 2).
The standardized total effects of each independent (column) variable on the dependent (row) ones.
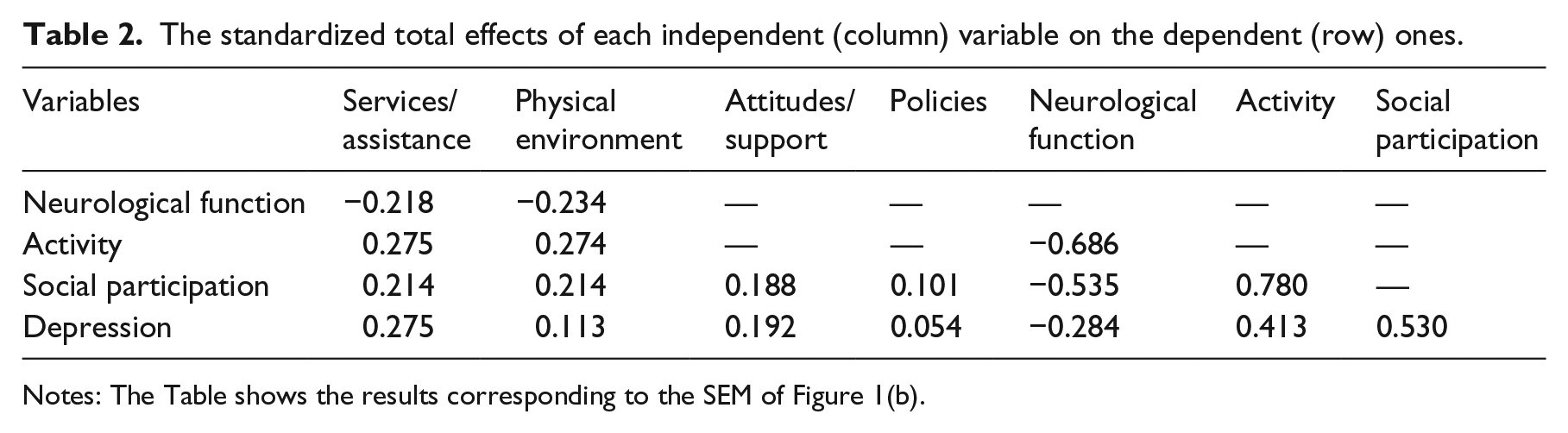
Notes: The Table shows the results corresponding to the SEM of Figure 1(b).
All four of the environment domains (services/assistance, attitudes/support, physical environment, and policies) were significantly related to depression or social participation, but their influence was weaker than that of neurological function, activity, social participation, or depression according to the standardized total effects (Table 2). Among the four domains, services/assistance and attitudes/support were, in general, more influential in determining depression than the physical environment or policies. And the four domains of the environment were interrelated; the correlation coefficients ranging from 0.09 to 0.38 (p ⩽ 0.05) (Figure 1(a) and (b)).
Discussion
This study was designed to explore the impacts of the environment and social participation on post-stroke depression. The findings show that depression can be a critical intermediate variable that connects environmental factors with activity and social participation. Depression was found to be a primary factor predicting restricted social participation. Social participation restriction was, in turn, a risk factor leading to depression; and all facets of the environmental barriers were related to depression as well.
That depression can impact social participation has been well documented. 22 Its effect on social participation surpasses even that of physical disability. 23 The reverse impacts of social participation on depression have been suggested by at least two published studies.1,24 Restricted social participation may lead persons with stroke to experience social isolation, which can further result in depression symptoms.25,26
Thus, social participation and depression interact. Each exacerbates or moderates the effects of the other. The same interaction is often observed between depression and physical illness, and then degraded health and increased risk of mortality.27,28 Depression is thus a key factor related to disability and the general health of persons living with stroke. It is imperative to routinely screen stroke survivors and identify early post-stroke depression, followed by early intervention if necessary.
The CHIEF scale used to measure environmental barriers was created according to the ICF’s classifications for the environment.10,19 The services/assistance and attitudes/support domains in the inventory are similar to ‘social support’ in concept. They explore whether family, the community, the healthcare system, transportation, etc., meet the subject’s needs, and the extent to which the subject is encountering problems in dealing with such environmental factors. 18
Many studies have shown that social support influences the emotions of persons with stroke.24,29 They perceive the support of family and friends as crucial to their recovery and a major influence on facets of their lives. 30 In rural China, families provide almost all the material and spiritual support for persons with stroke. 29 Among the nine items assessing services/assistance and attitudes/support, three relate directly to family support, and the other six (such as access to health services, transportation, and the attitudes of other persons apart from the family) are in fact indirectly related to family support in the China context as well. So the findings show that the two domains strongly influence depression.
The physical environment, including the home and community environment, has also received much attention from researchers. 30 But most attention has been paid to the association of the physical environment with activity and social participation after stroke. 31 It is undisputed that social participation can be improved to some extent through decreasing home and community barriers. 32 The present findings show similar relationships between the physical environment and depression. An accessible physical environment might delight and relax physically and psychologically, further increase activity, and moderate depression symptoms. A study has shown that indoor environmental barriers are associated with higher mortality among very old people. 33 Fall hazards are pervasive in older persons’ homes in China. 34 Specific investigations and targeted home and community environment interventions are needed in order to facilitate the social participation of persons with stroke and decrease depression symptoms.
Although the findings show that policies are the least influential of the factors studied, the World Health Organization argues that environmental barriers ‘… are interconnected—people with disabilities will not be able to benefit fully from improvements in one domain if the others remain inaccessible’. 35 The findings of this study reaffirm that view.
Neurological functioning and activity were included in the SEM analyses as well. Both showed strong relationships with social participation or depression. In the chronic phase of stroke, however, neurological function and activity (understanding and communication, mobility) are difficult to recover, 36 whereas eliminating or decreasing environmental barriers may yield prompt and positive effects on depression and social participation. Moreover, the environment could exert a subtle influence, which may help individuals deal with negative emotions, further decreasing depression symptoms.
This study protocol had limitations. In the first place, the participants spoke various Chinese dialects (Hakka, Cantonese, Chaozhou, and others) and few of them could not understand Mandarin well. Although the investigators had been trained in listening to or speaking in the dialects, questions or replies occasionally had to be translated by a family member or the village physician. This may have introduced inaccuracies or misunderstanding. Note too that the participants came from one southern part of mainland China; the findings may not automatically be generalized to other areas, as the environmental barriers could be very different.
Social participation among persons with stroke is inversely related to post-stroke depression. All facets of the environment (physical, services/assistance, attitudes/support, policies) influence depression. Interventions aimed at decreasing or eliminating environmental barriers may show positive effects on depression symptoms and social participation. Further studies are needed to provide stronger evidence of the relationships between environmental factors and post-stroke depression, and to explore the utility of specific environmental interventions.
Clinical messages
Depression and social participation interact, each exacerbating the other. Improving social participation may be effective to address depression.
All the facets of the environment can influence depression. Decreasing or eliminating environmental barriers may exert subtle positive influences on depression.
Footnotes
Acknowledgements
We thank the health workers and physicians in the township medical centres and village medical posts whose voluntary help made the survey successful. We also thank all the postgraduate students who collected data, and all the subjects who participated in the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Qixing Charity Fund for Stroke and Rehabilitation of the Guangdong Branch of the Red Cross Society of China [grant 20131217], the China Medical Board [grant 04-808], Science and Technology Plan Projects of Guangdong province [grant 2013B09100009].