
Abstract
Objective:
Structural analysis of the German translation of the “Client-Centered Rehabilitation Questionnaire” (CCRQ).
Design:
Cross-sectional multicenter study.
Setting:
Ten inpatient rehabilitation centers in Germany.
Subjects:
The CCRQ was completed by patients in the ten rehabilitation centers.
Main measures:
The psychometric analysis of the CCRQ was conducted using exploratory and confirmatory factor analysis.
Results:
The CCRQ was completed by 496 patients (average age: 59 years; 59.7% women). The CCRQ’s 7-factor structure could not be confirmed. Factor analysis showed that the three latent constructs “decision-making/communication”, “self-management/empowerment”, and “psychosocial well-being” (60.73% variance explained) adequately represent patient-centeredness in medical rehabilitation assessed by the CCRQ. The scales possess good reliability (Cronbach’s α = .83 to .87) and convergent criterion validity (r = 0.48 to 0.68). The three-factorial model exhibited good local and global data fit (RMSEA: 0.063, CFI 0.962, TLI 0.954) and proved to have a better data fit than concurring models (e.g. a model assuming an underlying factor).
Conclusions:
A validated short form of the Client-Centered Rehabilitation Questionnaire, CCRQ-15, could be identified. Three scales based on 15 items allow assessing the key aspects of patient-centeredness in German medical rehabilitation.
Introduction
Patient-centeredness is considered an important principle in all areas of medicine and health care.1,2 According to the Institute of Medicine, 3 patient-centered care is defined as “providing care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions.” Patient-centeredness is not only considered a normative imperative4,5 but also an important quality criterion.6–8 The theoretical foundations of patient-centeredness differ in the extent of integrated concepts.8–15 Some take into account only the patient and physician and their interaction,12–14 while other, broader concepts consider structural and organizational aspects such as access to care, coordination, interprofessional teamwork, etc.10,16,17,15 Accordingly, a systematic review and concept analysis by Scholl et al. 18 identified an integrative model of patient-centeredness (comprising 15 dimensions).
As a result of the differing theories, assessment instruments assess different dimensions of patient-centeredness. 18 Systematic consideration of the demanded patient-centeredness criterion in patient care requires appropriate and psychometrically proven measurement instruments. In English-speaking countries, the Client-Centered Rehabilitation Questionnaire by Cott et al. 11 is commonly applied. Another comprehensive instrument is the Patient Assessment of Chronic Illness Care. 19 A systematic literature search in the Medline database (PubMed) showed that no psychometrically sound German-language instrument currently exists for measuring patient-centeredness. Hence, the Client-Centered Rehabilitation Questionnaire (CCRQ), which has already been psychometrically analyzed in Canada, 11 was translated into German. The aim of this study is to test the structure of the Client-Centered Rehabilitation Questionnaire (theoretically suggested by Cott et al.) 11 in a large sample of German rehabilitation patients. The unique characteristics of the medical rehabilitation setting in Germany involve treatment of the chronically ill patient (oncological, cardiologic, orthopedic, rheumatologic, neurological, and psychosomatic diseases) by an interdisciplinary rehabilitation team (physicians, nurses, physiotherapists, etc) in an inpatient rehabilitation center.
Methods
Data collection
Ten inpatient rehabilitation centers (two oncological, two neurological, and six orthopedic) in southwest Germany participated in the study. Each center assigned one contact person to be responsible for study activities; this person distributed the questionnaires to patients, collected the completed questionnaires, and returned them directly to the research team. The questionnaires were completed by the patients at the end of their stay. The following inclusion criteria were used: (1) participation in a rehabilitation program at one of the participating centers; (2) age 18-65 years; (3) adequate knowledge of the German language; and (4) no cognitive deficits. The study was reviewed and approved by the ethics committee of the University of Freiburg, which has given a favorable opinion.
Instrument
The original CCRQ 11 measures the construct of ‘patient-centeredness’ using seven scales. Thirty-three items are included. The individual scales cover the sub-dimensions “Participation in decision-making and goal-setting (6 items)”, “Client-centered education (8 items)”, “Evaluation of outcomes from client’s perspective (4 items)”, “Family involvement (5 items)”, “Emotional support (4 items)”, “Physical comfort (4 items)”, and “Co-ordination and continuity” (2 items). The items are answered on a five-point Likert scale (1 = strongly disagree; 2 = disagree; 3 = neither agree nor disagree; 4 = agree; 5 = strongly agree). The response option “Does not apply” (= 0) is also available. High item scores (and high subscale scores) correspond to higher perceived patient-centeredness. The seven scales have not been verified through factor analysis. Internal consistencies lie between 0.72 (Scale 2, “Client-centered education”) and 0.89 (Scale 4, “Family involvement”).
For the present study, the English CCRQ was translated into the German language with the forward-backward method by an English teacher and an English native speaker. No notable deviations from the original version were identified. In addition, two global items were generated and added to check convergent validity, specifically Global Item A (Item 34): “I was involved in decisions regarding my treatment” and Global Item B (Item 35): “The center focuses on patients and their needs.”
“Patient satisfaction” was used for criterion validation because of its relation to patient-centered communication. 20 It was assessed with the established and validated Questionnaire on Patient Satisfaction, 21 which was developed on the basis of the American ‘‘Client Satisfaction Questionnaire CSQ-8”. 22 Using eight items, the questionnaire measures general patient satisfaction with the received treatment. Based on eight 4-point Likert-scaled items, the questionnaire assesses general patient satisfaction. High scale values (total scores) correspond to high patient satisfaction. The internal consistency of the total score is high, with Cronbach’s alpha between .87 and .93. 23
Data analysis
A structural analysis of the CCRQ was planned. Factor analyses were used to identify a model of the CCRQ structure that is valid for this population. The quality of the model was tested by applying measures of global and local fit. Model improvement steps were applied using modification indices. Then, the validity of the new CCRQ structure was evaluated.
The CCRQ contains five items on family involvement (Items 4, 12, 17, 23, and 27). As this content is only meaningful for a subsample (only 58.8% acceptance in the study sample), these items were excluded from the subsequent analyses.
Classic exploratory factor analysis (EFA) was conducted for structural analysis of the CCRQ using principal component analysis and VARIMAX rotation to achieve a simple structure. The identified structure was then reanalyzed using confirmatory factor analysis (CFA). CFA tests the validity of the presumed structure according to the rigorous assumptions of classic test theory.11,24,25
The CFA model assumes (a) correlated constructs and (b) each item to be a distinct, linear indicator of one of these constructs. Items with factor loadings of 0.5 or above are considered acceptable, and those with 0.7 or above are considered good. 11 Goodness-of-fit indices were calculated to check global model fit. 24 Fit testing was conducted on the basis of the Root Mean Square Error of Approximation (RMSEA) as a measure of unexplained variations on the variance-covariance level as well as the Tucker-Lewis Index (TLI) and the Comparative Fit Index (CFI) as indicators of approximate model fit.24,25,11 In case of inadequate model fit, model optimization steps (elimination of unreliable items and definition of alternative item-construct associations) were tested by analyzing indicator reliabilities and residual correlations in accordance with Kline’s recommendations. 24
To test local model quality, 11 indicator reliability, factor reliability, and average variance extracted (AVE) were calculated. Discriminant validity was tested using the strict Fornell-Larcker criterion, which demands for each individual construct to be more strongly correlated with its respective indicators than with other constructs. 26 The relationship of each scale with “patient satisfaction” was additionally calculated to check convergent validity.
All cases with more than ten missing CCRQ responses (>30%) were excluded from analysis. For the remaining sample, missing values were imputed using the expectation maximization algorithm (NORM program).27,28 The software package IBM SPSS 19.0 was used for the statistical analysis and complemented by AMOS 19.0 for differentiated structural analysis.
Results
Sample characteristics and item acceptance
A total of n=1085 questionnaires were sent out, and n=539 completed questionnaires were returned (response rate: 49.7%). The questionnaires from 43 people (8.1%) had to be excluded because of an excessive number of missing items. The characteristics of n=496 remaining respondents are shown in Table 1. Their average age was about 59 years, and more than half of the participants were women (59.7%). The patients primarily received rheumatology or orthopedic care (62.3%), and 40.3% of them had a low educational level. Almost one-fifth (19.8%) of patients had suffered from the respective disease for more than six years.
Characteristics of the sample (n = 496 inpatients).
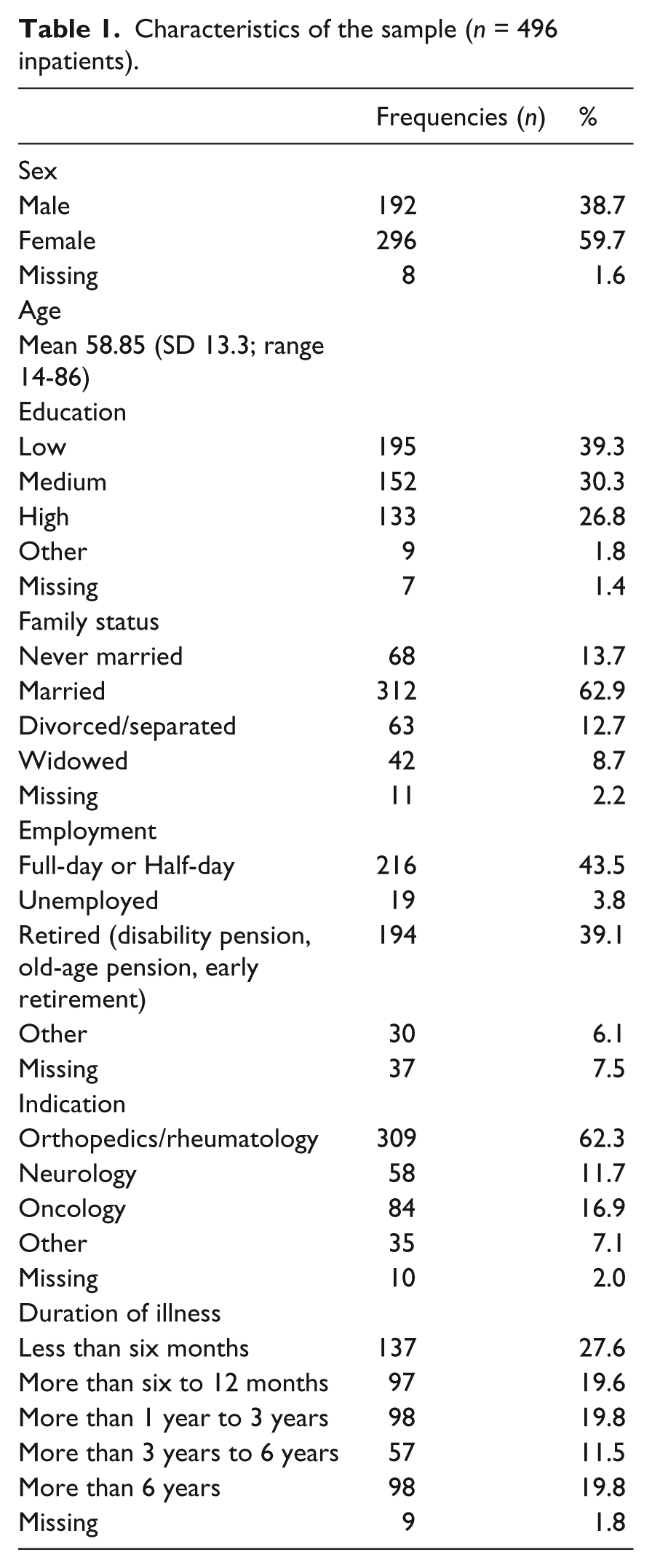
A comparison of patient characteristics with the statistics of the German statutory pension insurance 29 shows a noticeably higher average age of rehabilitation patients (average age of 50.4 years in Germany versus 58.85 in the study). In addition, the percentage of female patients is 10.1% higher (women make up 49.6% of the population in Germany versus 59.7% in the study). 29 Acceptance of the individual items was between 75.1% % (Item 10 “I was given adequate information about support services in the community” original scale “Client-centered education” scale) and 97.6% (Item 19, “Physical comfort” scale).
Exploratory factor analysis (EFA)
The EFA performed with the 28 items yielded a five-factor structure (eigenvalues > 1) according to the eigenvalue criterion (explained variance: 60.73%). The three negatively worded items, namely Items 2, 7, and 33, exhibited insufficient loadings (of a maximum of 0.55.) 30 Reanalyzing the remaining 25 items led to a four-factor solution (explained variance: 61.25%) with some considerable violations of selection criteria on the item level. After eliminating Items 8 (physical pain), 11 (meeting expectations), 18 (contact person), 20 (encouragement for shared decision making) and 32 (perceived teamwork) because of insufficient factor loadings or ambiguous factor assignments, a three-factor simple structure proved to be fit the data. This 20-item solution proved to be content valid and to meet the Kaiser criterion and the scree-plot criterion (explained variance: 60.73%; eigenvalues = 9.559/ 1.410/ 1.176/ 0.907/ 0.739).
The seven items of the first factor (1, 5, 6, 9, 13, 15, and 16) can be summarized as reflecting “decision-making/communication”. The second factor comprises items on the topic of “self-management/empowerment” (also seven items: 3, 10, 22, 24, 25, 26, and 29). The third scale is defined by six items (14, 19, 21, 28, 30, and 31) that are indicative of “psychosocial well-being.”
Confirmatory factor analysis (CFA)
CFA was conducted to test construct validity according to the assumptions of classical test theory for the three-dimensional structure of this 20-item version of the CCRQ. The measures of global model fit failed to meet the threshold levels recommended in the literature 11 for acceptable model fit (see Supplementary Table 1, “three-factor model” line (20-item-version)).
Items 6 (accommodation of needs), 13 (respectful treatment), 14 (acknowledgement of reported pain), 19 (time for rest) and 29 (preparation for returning home) had to be eliminated due to insufficient loadings (indicator reliability <0.4) or high residual correlations. The resulting CFA model of the CCRQ exhibits an appropriate model fit (TLI =.954, CFI = .952, RMSEA = 0.63).
Table 2 shows the discrimination values as well as the scale values. Internal consistency was measured as Cronbach’s α of .85 for Scale 1, .87 for Scale 2, and .83 for Scale 3. Item difficulty varies between 3.67 (Item 10) and 4.45 (Item 5). All items and the created subscales show a left-skewed response distribution, but only values of |2| and above are considered problematic. 31
Overview of the scales and items of the new Client-Centered Rehabilitation Questionnaire 15 (CCRQ-15).
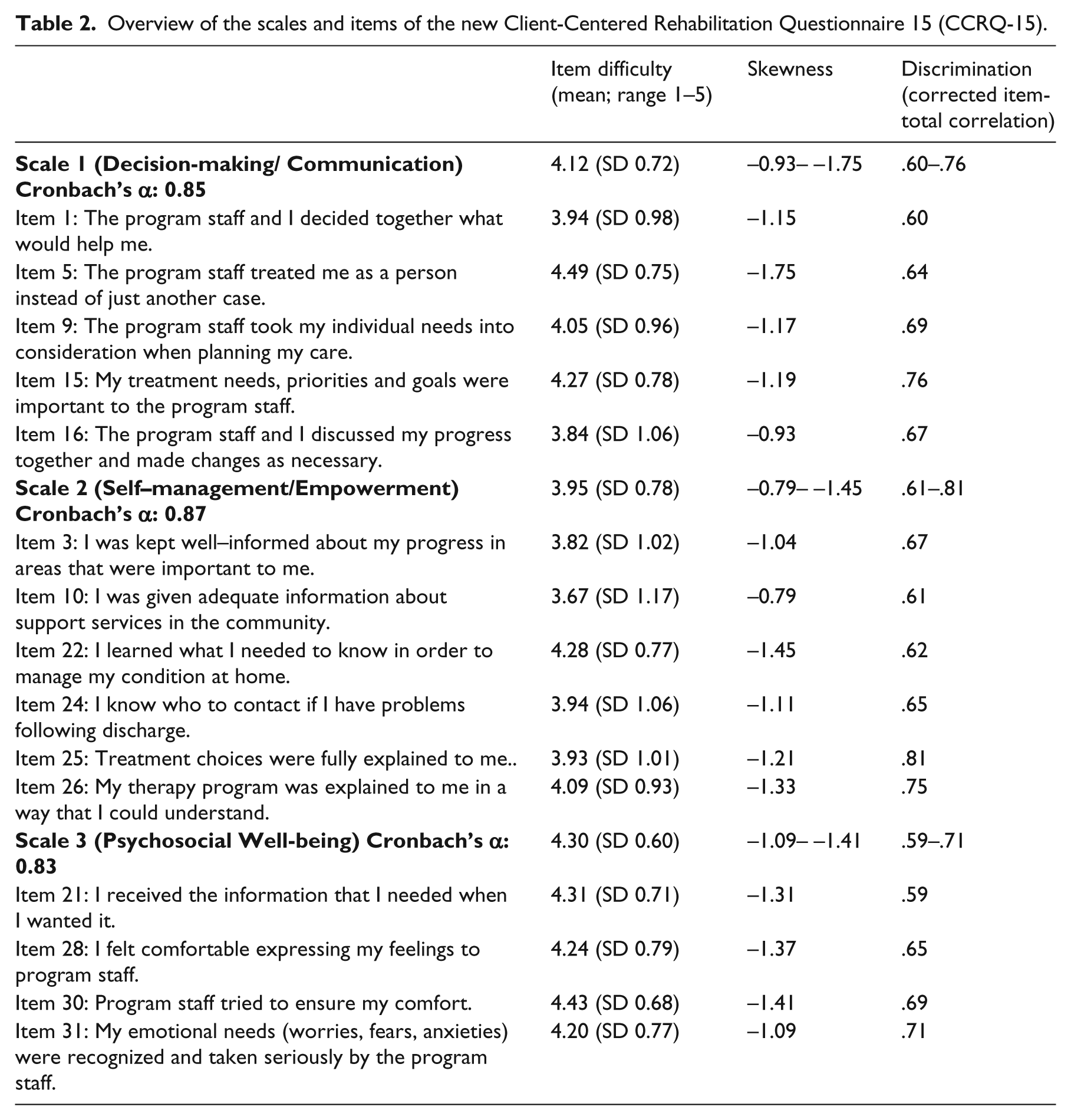
The measures of local fit are shown in Supplementary Table 2. All items are significantly associated with the respective latent constructs, and all items except Item 1 possess an indicator reliability greater than 0.40. 32 Factor reliability and average variance extracted (AVE) confirmed reliable construct measurement. According to the discriminant construct validity, reliable discrimination between the three scales could not be proven using the Fornell-Larcker criterion. 26 The intercorrelations between the constructs (r= .82 - .90) are considerably higher than the root of the AVE of the individual constructs (sqrt(AVE) = .73 - .74).
Hence, two additional models of the theoretical structure were defined, which assumed the existence of a second-order factor representing “patient-centeredness” and a unidimensional model, respectively. Compared to the CFA model, all global measures of fit substantiate a considerably poorer fit for these alternative models. Especially BIC, which is decisive for comparing models with different degrees of freedom, documents the advantageous properties of the CFA model. Hence, despite the high construct associations in the alternatives to the CFA model, assuming first-order or second-order homogeneity of the CCRQ contents does not constitute a reasonable alternative to the three-dimensional structure.
Figure 1 illustrates the final structure of the questionnaire CCRQ-15. It depicts the allocation of the items to the three scales and their factor loadings. Additionally, the correlations between the constructs are presented. All steps of the EFA and CFA that resulted in the CCRQ-15 are shown in a table in the appendix.
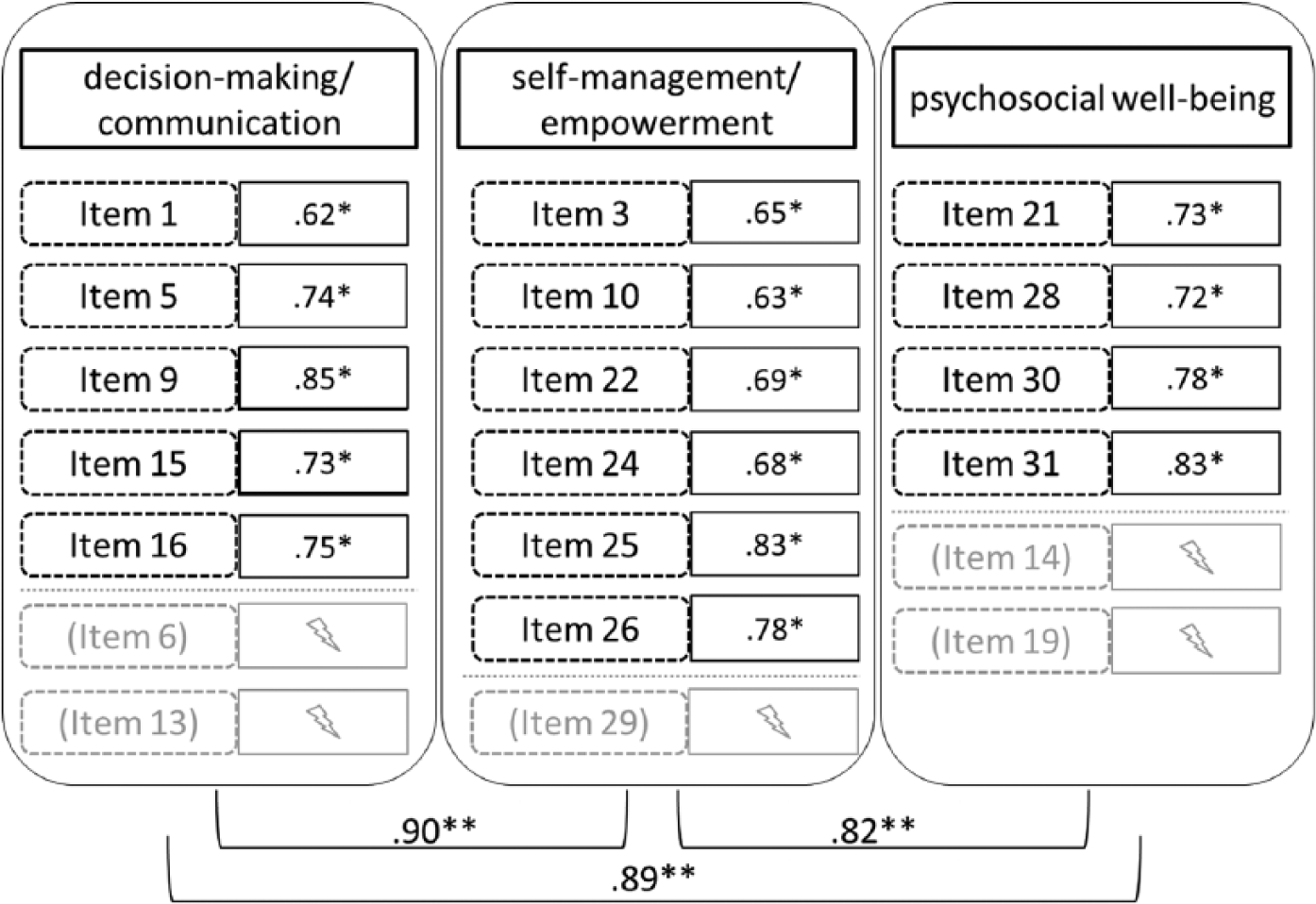
Structure of the CCRQ-15 (including factor loadings of the items = *, correlations between the constructs = **).
Criterion validity
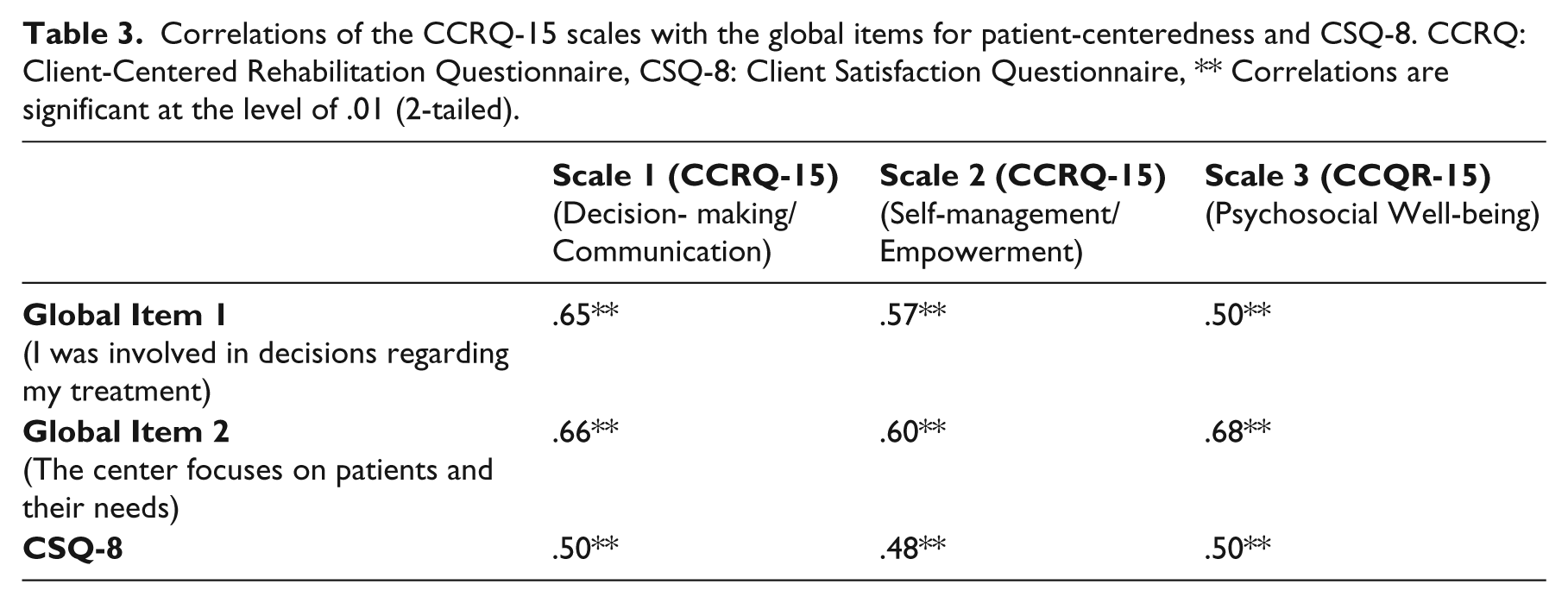
To test criterion validity in the form of concurrent validity, 24 the relationships between the three constructs (“decision-making/communication”, “self-management/empowerment”, and “psychosocial well-being”) and the global assessment of patient-centeredness were determined (see methods/instrument for Global Items A and B). All three scales were found to be moderately, significantly positively correlated (0.48 to 0.68) with the total value of the Questionnaire on Patient Satisfaction as well as with both global items (see Table 3).
Correlations of the CCRQ-15 scales with the global items for patient-centeredness and CSQ-8. CCRQ: Client-Centered Rehabilitation Questionnaire, CSQ-8: Client Satisfaction Questionnaire, ** Correlations are significant at the level of .01 (2-tailed).
Discussion
The seven scales of the CCRQ suggested by Cott et al. 11 could not be replicated in the factor analysis in the large sample of German medical rehabilitation patients. Three alternative scales were identified, namely “Decision-making/communication”, “Self-management/empowerment”, and “Psychosocial well-being”. This structure was successfully verified in confirmatory analysis. It revealed convincing goodness-of-fit indices. Furthermore, the scales demonstrated good reliability as well as validity. Therefore, this questionnaire structure with 15 items representing three scales is defined as the CCRQ-15 (Client-Centered Rehabilitation Questionnaire 15). It adequately measures important aspects of patient-centeredness in the German rehabilitation setting. The CCRQ-aspect of “family involvement” was not included in our analysis, as the associated items had a low acceptance rate and therefore were only meaningful for a subsample of our study population.
The resulting 15 of the original 33 items could be assigned to the three scales as follows: The “Decision-making/communication” scale contains two items on shared decision-making (Items 1 and 16) as well as three items on individuality in decision-making (Items 5, 9, and 15). This means that decision-making is considered in the context of individuality and patients’ particular needs.
The “Self-management/empowerment” scale focuses on establishing the prerequisites for shared decision-making (Items 3, 25, and 26) as well as on enabling patients to engage in health-promoting behaviors after they are discharged (Items 10, 22, and 24). Emotional coping is a key component of managing chronic diseases. 34 It is an important element of the empowerment concept, 35 but it cannot be measured with the CCRQ-15 short version. Developing and testing appropriate items could be a valuable advancement of the CCRQ-15. The three negatively worded items (Item 2, Item 7, and Item 33), which measure the quality aspects of conveying information, were already eliminated in the original version 11 due to low test-retest reliability.
The “Psychosocial well-being” scale measures both general well-being (Item 30) and aspects of mental-cognitive well-being (Item 21). Items 28 and 31 additionally measure emotional well-being and the consideration of affect and emotion in the context of the provider-patient relationship. This is in line with the results reported by Farin 36 in his review of provider-patient communication in chronically ill people. He concludes that affective and emotionally supportive communication is particularly important for patients. Based on the fact that the scale does not measure physical well-being, an adequate psychometric basis for measuring patient-centeredness in line with the biopsychosocial perspective needs to be developed. However, the patient-centeredness theories of Mead and Bower 37 as well as Stewart 38 do not explicitly mention this factor either. Unlike these theories, Scholl et al. 18 consider the biopsychosocial perspective. Furthermore the perception of patients as unique individuals is a fundamental principle of their integrative model of patient-centeredness. Patient involvement in treatment and patient empowerment as aspects of patient-centred activities are also included in the integrative model of patient-centeredness. However, higher-level factors conducive to patient-centeredness, such as teamwork, continuity, and coordination of care as well as access to care, cannot be measured using the three new scales.
The high correlations of the sub-dimensions are also in accordance with the theory of patient-centeredness. Scholl et al. 18 describe these individual dimensions of patient-centeredness as interrelated as well. Shared decision-making as well as self-management/empowerment and the concept of holism or the biopsychosocial perspective promote viewing patients as unique individuals.1,34,37 Leplege et al.39 write that patient-centeredness emphasizes the person as a whole. Hence, all three scales include aspects of holistic approaches such as the consideration of special, individual circumstances; defining goals or preparing the patient for the time following rehabilitation are also related to that. Shared decision-making and self-management/empowerment are regarded as complementary concepts with shared elements, such as shared responsibility 34 and the development of a trustful, respectful partnership. 35 Shared decision-making is often considered a prerequisite of self-management/empowerment,34,40 but simultaneously, empowerment can enable patients to actively participate in decision-making processes as equals and hence can be considered a prerequisite of shared decision-making.40 Nevertheless, the existence of a second-order construct proved not to be a reasonable alternative model in the study sample.
The following methodological limitations must be considered when interpreting the analysis results: First, participation was voluntary. Only motivated patients were likely to complete the questionnaire, which is likely to lead to selection effects. The second limitation is related: No information is available on the people who did not complete and return the questionnaire. Hence, there is no control of non-responders. In addition to the voluntary nature of participation, this means that data may be distorted. Third, the population of study participants had a higher average age and a greater percentage of women compared to members of the German statutory pension fund; 29 this difference reduces the generalizability of results. Fourth, the high correlations or rather the poor discriminability of the scales has to be considered. However, it should be noted in summary that the three scales do measure the essential aspects of patient-centeredness in rehabilitation settings. Besides, the evaluation of questionnaires using factor analysis is a useful method.
The development of a validated short questionnaire (named CCRQ-15) for measuring patient-centeredness can be viewed as an important contribution to research and practice on the topic of “patient-centeredness in rehabilitation.” There has been a demand for appropriate measurement instruments. The German CCRQ-15 can be an improvement upon the original 33-item version as it contains only 15 items. This questionnaire is therefore a practical instrument that can be recommended for use in practice. To verify the stability and generalizability of findings, the suggested factorial structure of the CCRQ-15 should be cross-validated on a large sample of rehabilitation patients in the future.
Clinical messages
The seven original CCRQ scales could not be replicated in the German rehabilitation patient sample.
Three newly determined scales were identified, namely “Decision-making/communication”, “Self-management/empowerment”, and “Psychosocial well-being”, resulting in a validated German short scale, named CCRQ-15.
The CCRQ-15 allows for a reliable, valid assessment of patient-centeredness in German medical rehabilitation.
Footnotes
Acknowledgements
We would like to thank the following rehabilitation facilities: ACURA Fachklinik Waldbronn; ACURA Waldklinik Dobel; Asklepios Klinik Triberg; Földiklinik Hinterzarten; Kliniken Dr. Vötisch; Mooswaldklinik Freiburg; Parkklinikum Bad Krozingen; Rehaklinik Siegmund Weil Bad Schönborn; Reha-Zentrum Schömberg; Theresienklinik Bad Krozingen.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was done in the context of the project “PATENT – Patient-centered team development in rehabilitation clinics”, which is funded by the German Federal Ministry of Education and Research and the German Pension Fund.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.