
Abstract
Objective:
To identify the extent to which exercise intervention studies in multiple sclerosis rehabilitation are addressing comorbidities and if researchers consider comorbidities as possible moderators or mediators of exercise outcomes.
Methods:
Five databases were searched from inception to January 8, 2016, for exercise-related terms in combination with multiple sclerosis. Studies were screened and limited to randomized control trials, full text, and English language. We assessed whether comorbidities were excluded or included, how they were reported and described, and if they were examined as possible moderators or mediators of exercise outcomes.
Results:
We reviewed 99 articles that included various exercise interventions, where the most common were general multi-faceted exercise training (n=34), cardiovascular training (n=18), progressive-resistance training (n=12), and balance and gait training (n=12). In total, 77 of 99 studies reported one or more comorbidities as an exclusion criterion. The most commonly excluded comorbidities were cardiovascular diseases, cognitive impairments or psychiatric disorders, and unspecified conditions or contraindications. Only nine studies reported details on excluded participants with comorbidities. Across studies that reported comorbidities of included participants (n=8), none examined comorbidities as possible moderators or mediators of exercise outcomes.
Conclusion:
Although a variety of exercise interventions have positive outcomes, there is limited evidence that these interventions are generalizable to people with multiple sclerosis who have comorbid conditions.
Introduction
Physical inactivity and deconditioning are common in people with multiple sclerosis 1 which can lead to mobility disability and worsening of disease-related impairments2,3 and reduced quality of life. 4 Physical inactivity increases the risk of other diseases such as cardiovascular disease in people with multiple sclerosis, 5 and consequently accentuates disability progression. 6 Thus, exercise plays a major role in multiple sclerosis rehabilitation for symptom management, slowing disability progression and increasing quality of life. Aerobic and progressive-resistance training are the most common exercise interventions studied and have been shown to be effective for improving muscle function,7, 8 aerobic function, 8 mobility,7–9 balance, 10 fatigue,11, 12 depression 13 and quality of life. 14 Based on a systematic review of available evidence, Latimer-Cheung et al. 15 developed physical activity guidelines for people with multiple sclerosis recommending engagement in aerobic training (30-60min) and resistance training 2-3 times per week at moderate intensity.
Exercise interventions for people with multiple sclerosis are increasing in complexity, sometimes integrating technologies to find more efficient ways to improve physical conditioning and reduce disease-related symptoms. However, physical inactivity and deconditioning could also be consequential to physical or mental conditions unrelated to multiple sclerosis, that is, comorbidities. 16 Comorbidity refers to one or more other diseases among people with an index-disease, 17 in this case, multiple sclerosis. Prevalence studies estimate that up to 50% of people with multiple sclerosis have one or more comorbidities. 18 The most prevalent comorbidities in people with multiple sclerosis are depression, anxiety, hypertension, hyperlipidemia and chronic lung disease. 6 As exercise can have a direct and positive impact on these common comorbidities,19–22 it is important to determine if comorbidities moderate or mediate exercise outcomes in multiple sclerosis rehabilitation interventions.
As the awareness of the burden of comorbidities in people with multiple sclerosis is increasing, we performed a comprehensive study aimed at documenting the impact of comorbidities on outcomes in rehabilitation intervention studies, including exercise interventions, neurorehabilitation interventions, 23 self-management and behavioural interventions, and cognitive training interventions. This paper focuses exclusively on the systematic scoping review of exercise interventions, which aimed to 1) identify the extent to which exercise intervention studies in multiple sclerosis rehabilitation are addressing comorbidities and 2) determine if they considered comorbidity as a possible of exercise outcomes.
Methods
Search strategy, article selection process and data extraction
The search strategy, article selection process and data extraction of the large comprehensive study have been previously described. 23 In brief, five major databases (EMBASE, Medline, PubMed Central, CINAHL, and Web of Science) were searched to locate articles of rehabilitation interventions (last search on January 8, 2016). An extensive list of search terms and keywords was used to capture the focus or content of a wide range of rehabilitation interventions and these were combined with the search term “multiple sclerosis” (for example, see the search strategy used for EMBASE in supplementary materials). Specific terms to capture exercise interventions were: exercise, physical activity, motor activity, and fitness. Search results were then limited to randomized controlled trials, full text articles, and English language. Studies were excluded if the results from people with multiple sclerosis were not reported separately from other populations (e.g., stroke) or the intervention was primarily medical (e.g., surgery or pharmaceutical) where rehabilitation was secondary or adjunctive.
Data extracted included general study information (research questions/objectives, intervention description, as well as sample size, age, percent of females, and level of disability of the sample), and information about comorbidities (if they were excluded or included, how were they reported and described, and whether their impact on the outcomes was tested).
Based on the intervention description in the articles, two experienced rehabilitation clinicians who have delivered rehabilitation services to people with multiple sclerosis (AF, MF) categorized all articles by type of intervention according to the mechanism of the intervention. Supplementary Material Table 1 outlines the definitions used to identify and group the different exercise interventions, which is the focus of this paper. To be considered an exercise intervention, the study intervention had to involve a form of physical activity that was planned, structured and repetitive over an extended period of time, with the intention of improving fitness, performance or health.22, 24 , 25 Several other intervention categories were identified (e.g. cognitive training, self-management program, neurorehabilitation) 23 but are not the focus of this paper, thus will not be discussed further.
Results
From the 250 articles selected during the larger comprehensive study (see PRISMA chart in Fakolade et al.), 23 99 exercise intervention studies were identified and categorized into different exercise intervention groups based on our definitions (see Supplementary Material Table 1), and thus reviewed for this study (see list of included articles in the Supplementary Materials).
Study characteristics
A summary of study characteristics by exercise intervention groups is shown in Table 1. General multi-faceted exercise training had substantially larger sample sizes compared to all exercise intervention groups. The mean age per group was very similar across all exercise intervention groups and consistent with most multiple sclerosis studies, participants were predominantly female. However, there were a few studies with predominantly male participants.26–28 The disability level of participants included was widely diverse in each exercise intervention group based on scores from the Kurtzke Expanded Disability Status Scale 29 or from the Patient-Determined Disease Steps. 30
Summary characteristics of included studies.
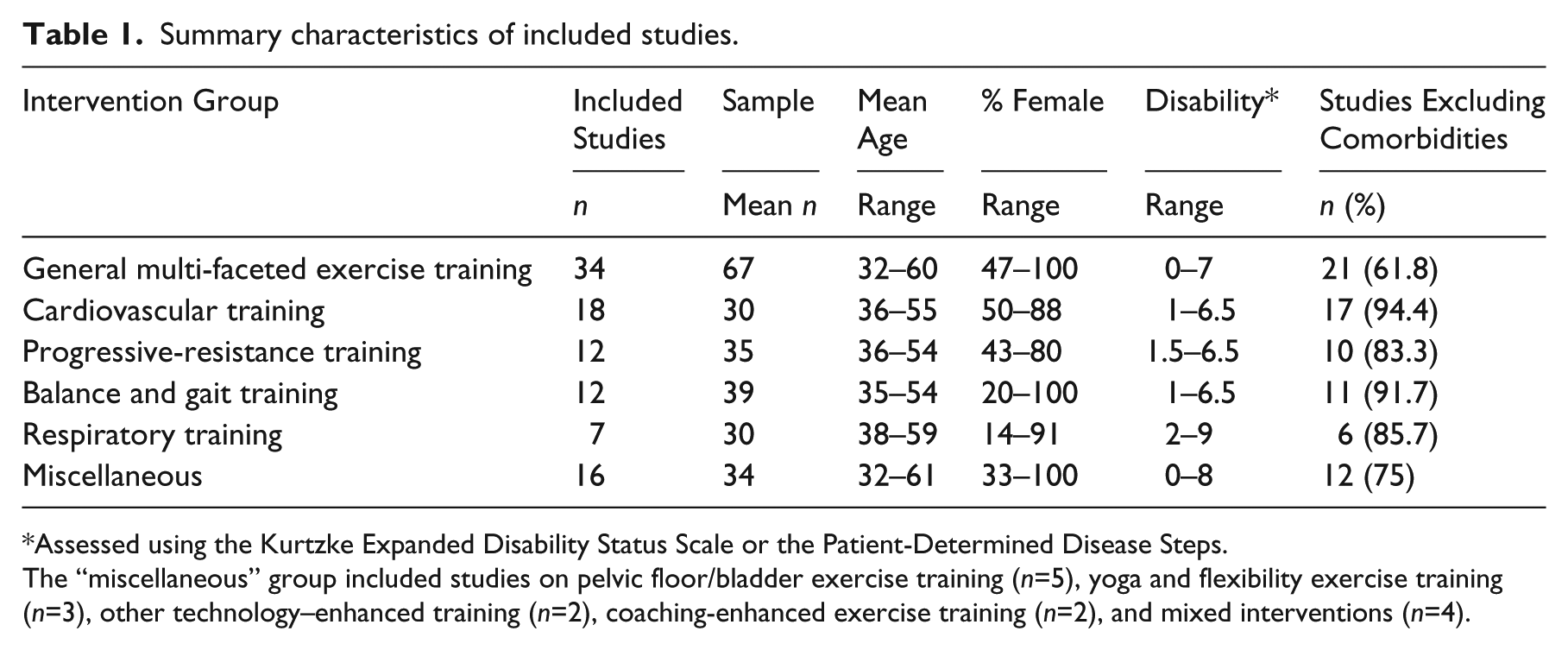
Assessed using the Kurtzke Expanded Disability Status Scale or the Patient-Determined Disease Steps.
The “miscellaneous” group included studies on pelvic floor/bladder exercise training (n=5), yoga and flexibility exercise training (n=3), other technology–enhanced training (n=2), coaching-enhanced exercise training (n=2), and mixed interventions (n=4).
Excluded comorbidities
In total, 77 of 99 studies reported one or more comorbidities as an exclusion criterion. More specifically, the majority of studies on cardiovascular training (17; 94.4%), progressive-resistance training (10; 83.3%), balance and gait training (11; 91.7%), and respiratory training (6; 85.7%) excluded people with one or more comorbidities. Nearly two-thirds of the studies on general multi-faceted exercise training (21; 61.8%) and three-quarters of those from the “miscellaneous” group (12; 75%) excluded people with one or more comorbidities.
Of the 77 studies that excluded participants with comorbidities, only nine studies (12%) reported on the number of participants excluded due to a specific comorbidity: six studies on general multi-faceted exercise training,31–36 one study on cardiovascular training, 37 one study on respiratory training 26 and one study in the miscellaneous group. 38 Thus, 68 studies had some comorbidities as exclusion criteria without reporting who and how many were actually excluded from the study.
The most commonly excluded comorbidities were grouped in three main categories: i) unspecified conditions or contraindications, ii) cardiovascular diseases, and iii) cognitive impairments or psychiatric disorders. The distribution of papers that excluded one or more comorbidities in each category is shown in Supplementary Material Figure 1. At least 50% of the studies in each exercise intervention group reported unspecified conditions or any contraindications, except for respiratory training (43%), making it unclear the specific comorbidities that were excluded. This problem was most evident in progressive-resistance training studies (75%), cardiovascular training (67%), and balance and gait training (58%).
Forty-two percent of all studies excluded people with one or more cardiovascular diseases. For the exercise intervention groups requiring the most physical effort (i.e. cardiovascular training, progressive-resistance training and respiratory training), 61%, 57%, and 50% of the studies, respectively, excluded people with cardiovascular diseases.
Forty-one percent of all studies excluded people with one or more cognitive impairments or psychiatric disorders. When cognitive skills were needed to perform the exercise, for example, in the balance and gait training group or the miscellaneous group, 67% and 63% of the studies, respectively, excluded people with cognitive impairments or psychiatric disorders.
Included comorbidities
Twenty-two studies (22%) did not report any comorbidities as exclusion criteria; thus, we assume that all people with comorbidities were included. From these papers, only Castro-Sanchez et al. 39 provided some information on the comorbidities of included participants. Based on reported Beck Depression Inventory II 40 scores at baseline (control group = 15±8.7, intervention group = 14±7.7) and known cut-offs for depression (14), 40 people with depression were included in the 20-week Tai-Chi aquatic exercise training intervention. Although the results demonstrated a 52% decrease in levels of depression in people with multiple sclerosis in the intervention group, the authors did not examine depression as a moderator or mediator on the primary outcomes (pain and disability).
From the studies that excluded individuals with comorbidities, seven reported on comorbidities of included participants.31,41–44 From these studies, one used general multi-faceted exercise training, 31 three cardiovascular training42–44 and one progressive-resistance training. 41 The main comorbidity reported was depression (n=5), however only one study had participants with scores on the Beck Depression Inventory II high enough to suggest clinical levels of depression. 41 Cakıt et al. 41 showed improvement in depression after cycling resistance training in combination with balance exercises. However, they did not look at the impact of depression or a change in depression on the other outcomes such as walking speed, balance, and fatigue. Petajan and colleagues 42 also reported reduced scores for depression (measured with the Profile of Mood States) for those who completed the cardiovascular training. However, according to their scores on the Profile of Mood States, the participants were not depressed at baseline, thus examining the impact of depression on the exercise outcome may not have clinical value. Hence, from all 99 articles reviewed, none examined comorbidity as a possible moderator or mediator on the exercise outcomes of these rehabilitation interventions.
Discussion
Based on the review of 99 exercise intervention studies, we found that the majority had one or more comorbidities as an exclusion criteria. The most common comorbidities excluded were cardiovascular diseases, cognitive impairments or psychiatric disorders, and unspecified conditions or contraindications. Only 8 reported information about included participants with comorbidities and none examined comorbidities as a possible moderator or mediator on the exercise outcomes of these interventions.
Exclusivity in exercise intervention studies
Most studies that excluded participants with comorbidities were exclusive in their selection of participants, which is methodologically strong in terms of maximizing internal validity. Yet, the consequence is that external validity is compromised, since up to 50% of people with multiple sclerosis have one or more comorbidities. 18 Thus, this review suggests that many of the trials included in this review may be unable to generalize their findings to a large segment of the multiple sclerosis population.
Excluding people with cardiovascular diseases
The most commonly excluded comorbidities reported were related to cardiovascular diseases which, ironically, are the most prevalent comorbidities in people with multiple sclerosis. 18 Among participants in the North American Research Committee on Multiple Sclerosis registry (over 8000), more than a third (37%) reported having at least one physical comorbidity with the most common ones being hypercholesterolemia (37%) and hypertension (30%). 45 Using administrative health data from Manitoba Canada, Marrie and colleagues found that, in people with multiple sclerosis, the prevalence of hypertension (20.8%), 46 and hyperlipidemia (13.8%) 46 were similar to the general population, and higher for ischemic heart disease (6.8%). 47
One of the primary goals of exercise therapy in multiple sclerosis rehabilitation is to stop, reduce or reverse deconditioning experienced by people with multiple sclerosis in order to support symptom management and to reduce the risks or burden of comorbidities such as cardiovascular diseases. 21 It follows that individuals with cardiovascular diseases would be included in studies in order to determine if their burden can actually be reduced by exercise interventions. However, 50% of studies on cardiovascular training and 40% of studies on progressive-resistance training excluded people with cardiovascular diseases. Thus, we do not have evidence from the reviewed papers that exercise interventions are appropriate or effective for people with multiple sclerosis with cardiovascular diseases.
Most exercise interventions excluded people with cardiovascular diseases for safety reasons, however, there is evidence suggesting that exercise is safe and beneficial for this specific population.19, 48 There is a need to develop new designs to minimize tension between internal and external validity and confidently and vigorously test tailored exercise interventions for people with multiple sclerosis with different comorbidities.
Excluding people with cognitive impairments or psychiatric disorders
Exercise therapy can also be beneficial for people experiencing cognitive impairments or psychiatric disorders. 22 Exercise has been shown to increase self-efficacy, regulate mood, distract from stressors and negative thoughts and activate postive and rewarding behavior. 49 Altough cognitive impairments and psychiatric disorders are some of the most prevalent comorbidities in people with multiple sclerosis, 6 only depression was reported in a few studies (n=5). Considering that the prevalence of anxiety and depression in people with multiple sclerosis was estimated at 23.7%, 50 and that all but one exercise intervention for people with multiple sclerosis included this sub-group, 41 there is lack of evidence on the beneficial effects of exercise in people with multiple sclerosis who have cognitive impairments or psychiatric disorders.
Lack of specificity in reporting comorbidities
Most of the studies reviewed did not provide adequate specificity in their reporting of exclusion criteria regarding comorbidities making it difficult to know which conditions were excluded. In fact, more than half (57.5%) of the studies excluded participants with “any condition that precludes safe exercise” which could include a variety of comorbidities such as stroke, cancer, hypertension, hyperlipidemia and chronic lung disease. 6 In addition, most studies excluding people with cognitive impairments or psychiatric disorders did not specify which conditions, thus assumptions are made that all conditions were excluded. Since the nature and potential cause of some impairments were unknown (e.g., cognitive), it is also unclear in these papers if they are reporting on a comorbidity or a multiple sclerosis symptom.
The rationale for exercise intervention trials to be so exclusive in their participant selection is most likely to ensure homogeneity (i.e., maximize internal validity) or for safety reasons. However, the extent to which the findings can be applied in clinical settings to prescribe a proper exercise program then becomes limited. The lack of details about the excluded comorbidities or the exclusion of all comorbidities creates a situation where clinicians may be applying “evidence” in ways that cannot be fully supported due to safety, adherence, and treatment effects. Also, clinicians and other readers cannot achieve a full and clear understanding about who can safely participate or to whom the treatment can be generalized.
Impact of comorbidities on exercise intervention outcomes is unknown
Despite a growing interest in comorbidities among people with MS, the knowledge about the impact of comorbidities on exercise intervention is very limited. From the few papers that included people with comorbidities (n=8), none of them examined the extent to which comorbidities may be influencing exercise outcomes. Thus, besides better reporting on excluded participants, future researchers should start developing multi-site pragmatic trials including participants with comorbidities. 51 These types of trials, although more complex, would provide the greater sample size required to perform sub-group analyses within the multiple sclerosis population (e.g., people with multiple sclerosis and diabetes, multiple sclerosis and depression) and determine if any comorbidities have moderating or mediating effects on outcomes. This knowledge would provide clinicians with evidence that better fits their practice context, therefore enabling clinicians to prescribe exercise programs to people with multiple sclerosis based on the totality of their health status. Thus, until more inclusive exercise interventions are determined to be effective and appropriate for people with multiple sclerosis with comorbidities, some degree of caution may be warranted when prescribing exercise based on the physical activity guidelines for people with multiple sclerosis. 15
Limitations
This review has some limitations that need to be acknowledged. The search strategy was limited to electronic databases and peer-reviewed articles. We also limited our search strategy to randomized controlled trials, excluding all other intervention designs (e.g., pre-post test, quasi-experimental designs). This narrow search strategy is not common for a scoping review but was chosen because randomized controlled trials are the gold standard in reporting detailed protocols, thus, comorbidities were more likely to be reported.
In conclusion, despite the beneficial evidence for exercise interventions in multiple sclerosis rehabilitation, there is little to no evidence that these interventions are suitable for people with multiple sclerosis with comorbidities, which accounts for half of this population. The reporting of comorbidities in multiple sclerosis exercise studies is limited to the exclusion of these persons, making it very difficult to generalize the findings. This gap of knowledge can be addressed with larger, multi-site trials with tailored exercise interventions where it would be possible to determine which, if any, comorbidities influence exercise outcomes. This knowledge is key for clinicians to decide on the best exercise therapy for the specific needs of each patient.
Clinical messages
The reporting of comorbidities in multiple sclerosis exercise studies is limited to the exclusion of people with comorbid conditions.
There is little to no evidence that exercise therapy interventions can be generalized to people with multiple sclerosis with comorbidities, which is half of the multiple sclerosis population.
There is little to no evidence about how comorbidities in people with multiple sclerosis may be influencing exercise outcomes.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Bisson’s work on this project was supported by the National Multiple Sclerosis Society (Mentor-based Post-doctoral Fellowship in Rehabilitation Research; MB0028); Ms Fakolade’s work was supported by a Multiple Sclerosis Society of Canada Doctoral Studentship (EGID-2022).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.