
Abstract
Objectives:
The three objectives of this scoping review were to (1) identify key conceptual/theoretical frameworks and the extent to which they are used to inform goal setting related to rehabilitation goal setting with children with motor disabilities, (2) describe research that has evaluated goal setting processes and outcomes, and (3) summarize the purposes of goal setting described in paediatric rehabilitation literature.
Methods:
The scoping review process described by Arksey and O’Malley was used to guide article selection and data extraction.
Results:
A total of 62 articles were included in the final review. While the concept of family-centered care was well represented, theoretical frameworks specific to goal setting (i.e. goal setting theory described by Locke and Latham, mastery motivation, social cognitive, personal construct, and self-determination theories) were rarely addressed. No articles reviewed addressed prominent behavior change theory. With the exception of the description of tools specifically designed for use with children, the role of the child in the goal setting process was generally absent or not well described. Few studies (n = 6) discussed the linkage between goals and intervention strategies explicitly. Only two studies in the review evaluated outcomes associated with goal setting. The primary purpose for goal setting identified in the literature was to develop goals that are meaningful to families (n = 49).
Conclusion:
The results highlight significant gaps in the literature explicating a sound theoretical basis for goal setting in paediatric rehabilitation and research evaluating the effects of goal qualities and goal setting processes on the achievement of meaningful outcomes.
Introduction
Goal setting is considered a critical component of the rehabilitation process. In paediatric rehabilitation, collaborative goal setting is emphasized because it aligns rehabilitation strategies with the individualized goals of children and families, enacting the tenets of family-centered care.1,2 The shift toward prioritizing participation outcomes in paediatric rehabilitation has also emphasized the importance of collaborative goal setting with parents and children since unique individual family life contexts and values shape the outcomes and rehabilitation activities that are meaningful to families. 3 While most clinicians would agree that goal setting is family-centered and a fundamental element of rehabilitation, there is evidence that formalized goal setting processes are inconsistently implemented in clinical practice4,5 and that parents and, in particular, children are not always optimally engaged in the process. 6 Implementation challenges highlight the need for a strong research foundation to support effective goal setting practices that engage children and families in identifying meaningful goals that inform therapy and improve outcomes.
While rationale for goal setting in rehabilitation is strong, it is largely based on pragmatic reasoning and less on a strong theoretical foundation, 7 particularly in paediatrics. 8 A theoretical framework has been developed for adult rehabilitation; 7 however, the increased engagement of families and developmental changes in child autonomy in paediatrics necessitates a theoretical framework specific to children and youth. Furthermore, research to support relationships between goal setting and improved child and parent engagement and outcomes is lacking. 1 With the exception of a review focussed on individualized goal setting tools, 9 no structured reviews on the theoretical basis and process aspects of goal setting in paediatric rehabilitation have been published.
A summary of current literature on goal setting in paediatric rehabilitation is needed to identify gaps in relation to goal setting in research and practice and to provide the basis for theory advancement to support goal setting process and evaluation. The overarching objectives of this scoping review were to (1) identify key conceptual/theoretical frameworks and the extent to which they are used to inform goal setting related to rehabilitation with children with motor disabilities, (2) describe research that has evaluated processes and outcomes related to goal setting, and (3) summarize the purposes of goal setting described in the paediatric rehabilitation literature.
Methods
The five steps outlined by Arksey and O’Malley 10 were used to conduct the review.
Article identification and selection
CINAHL, EMBASE, Medline, Scopus, Cochrane Database of Systematic Reviews, and Web of Science were searched for relevant records with the guidance of a medical librarian. The search strategy is provided in Supplementary Appendix 1. Records were not limited to any particular research methodology; all literature relevant to goal setting (i.e. research, review, and discussion articles) were included. Articles were included if they met the following inclusion criteria:
Addressed rehabilitation with children with motor disabilities;
Relevant to goal setting in a paediatric rehabilitation context;
Published in English;
Published in a peer reviewed journal between 1 January 1995 and 31 December 2017.
Studies were excluded if the authors used goal setting tools as outcome measures to evaluate effectiveness of interventions since our intent was to focus on the papers that directly addressed goal setting theory and practices. Articles were limited to those that discussed goal setting in paediatric rehabilitation generally or specifically discussed goal setting with children with physical or motor disabilities (e.g. cerebral palsy, Down syndrome, developmental coordination disorder, muscular dystrophy, and congenital limb deficiency). Articles that specifically discussed goal setting with children with neurobehavioral diagnoses such as autism were excluded because we anticipated that goal setting aims and strategies may differ.
The date range was selected because a preliminary search of the literature revealed no substantive articles related to goal setting prior to 1995.
L.P.-W. independently reviewed the titles and abstracts of the articles identified in the search and excluded duplicates and articles that were not relevant based on the eligibility criteria (see Figure 1 for a detailed flowchart of the selection and review process). The reviewers hand searched article reference lists for additional relevant articles, resulting in three additional articles for review. Full texts of selected articles were independently reviewed for relevance by L.P.-W. and a research assistant. The two reviewers met to discuss discrepancies and reach consensus on articles selected for inclusion. Discrepancies were resolved by a third rater (S.K.P.).
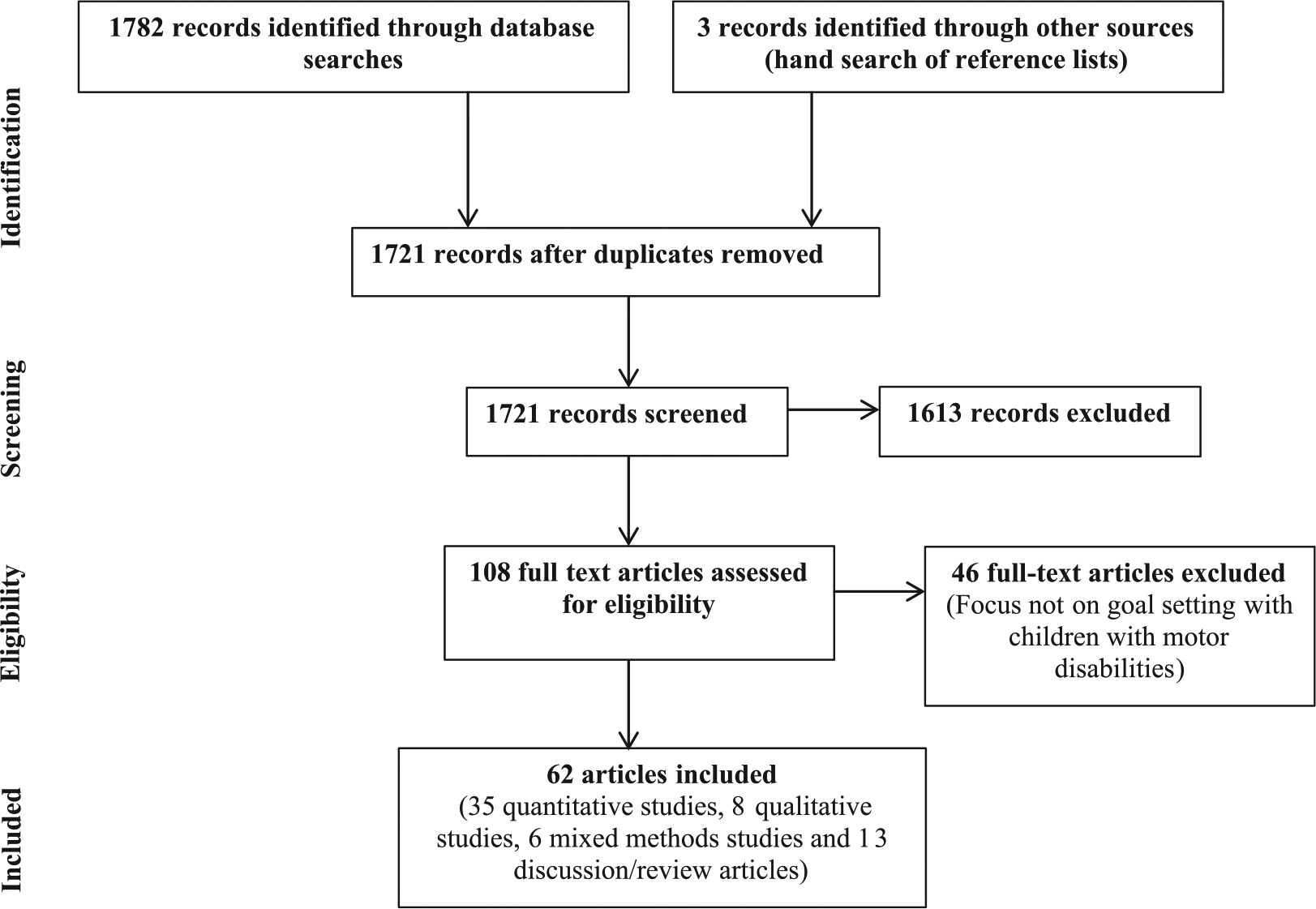
Scoping review flowchart.
Data extraction
The following data were extracted from each article: basic descriptive information (i.e. authors, title, year of publication, and journal), research objectives/questions, research design, theoretical/conceptual frameworks cited, extent to which theory was used, key processes related to goal setting, outcomes evaluated (and results), and the purpose of goal setting (either implicit or explicit). A scale was developed to categorize the extent theory related to goal setting was used throughout the article: 0 = no reference to theory relevant to goal setting, 1 = some use of theory (typically limited to the introduction/background), and 2 = theory described in depth and integrated throughout the article. Purposes for goal setting were classified using the four purposes of rehabilitation goal setting identified by Levack et al.: 11 (1) improving rehabilitation outcomes, (2) enhancing patient autonomy, (3) evaluating outcomes, and (4) responding to contractual, legislative, or professional requirements. Two additional categories were added to reflect the literature in paediatrics: (5) collaboration with families to ensure meaningful goals and (6) enhancing team collaboration.
Quantitative and mixed methods research articles were grouped and further reviewed for information on goal setting processes and outcomes if the effects of goal setting were specifically evaluated. Descriptions of the following aspects of goal setting process were extracted: (1) role of the child, (2) role of the parent, (3) role of the therapist, (4) goal setting tools used, (5) strategies to ensure linkages between goals and intervention strategies, and (6) if and how goals were revisited during the intervention process. Quantitative articles were excluded from this part of the analysis if the authors reported on aggregate data or chart reviews and therefore could not be expected to report on specific goal setting processes used by therapists and families. Qualitative and mixed methods research articles were reviewed for parent, child, and therapist perspectives on goal setting processes and outcomes.
L.P.-W. and a research assistant independently extracted data from the articles and compared and discussed ratings to reach consensus. Discrepancies were resolved by a third rater (S.K.P.). The team participated in regular meetings to discuss emergent insights and results.
Results
The 62 articles included in the final review are listed in Supplementary Appendix 2. The majority of the included articles were quantitative research articles (n = 35).4,5,12–44 Eight studies were qualitative6,45–51 and six used mixed methods.52–57 The remaining 13 included articles were discussion articles or reviews.8,9,58–68 The results of the review are presented according to the objectives of the review:
Which theoretical or conceptual frameworks are used to inform goal setting practices and to what extent are those frameworks used in the goal setting literature?
Six conceptual or theoretical frameworks were identified in the paediatric rehabilitation literature on goal setting: family-centered care, goal setting theory as described by Locke and Latham, 69 social cognitive theory (including self-efficacy theory and self-regulation theory), mastery motivation, personal construct theory, and self-determination theory. A summary of the conceptual and theoretical frameworks used is provided in Table 1. By far, the most prominent framework cited was family-centered care (n = 33). However, reference to the concepts of family-centered care was generally limited to brief reference to the principles; only nine of these articles demonstrated integration of family-centered concepts throughout the article.
Conceptual or theoretical frameworks cited.
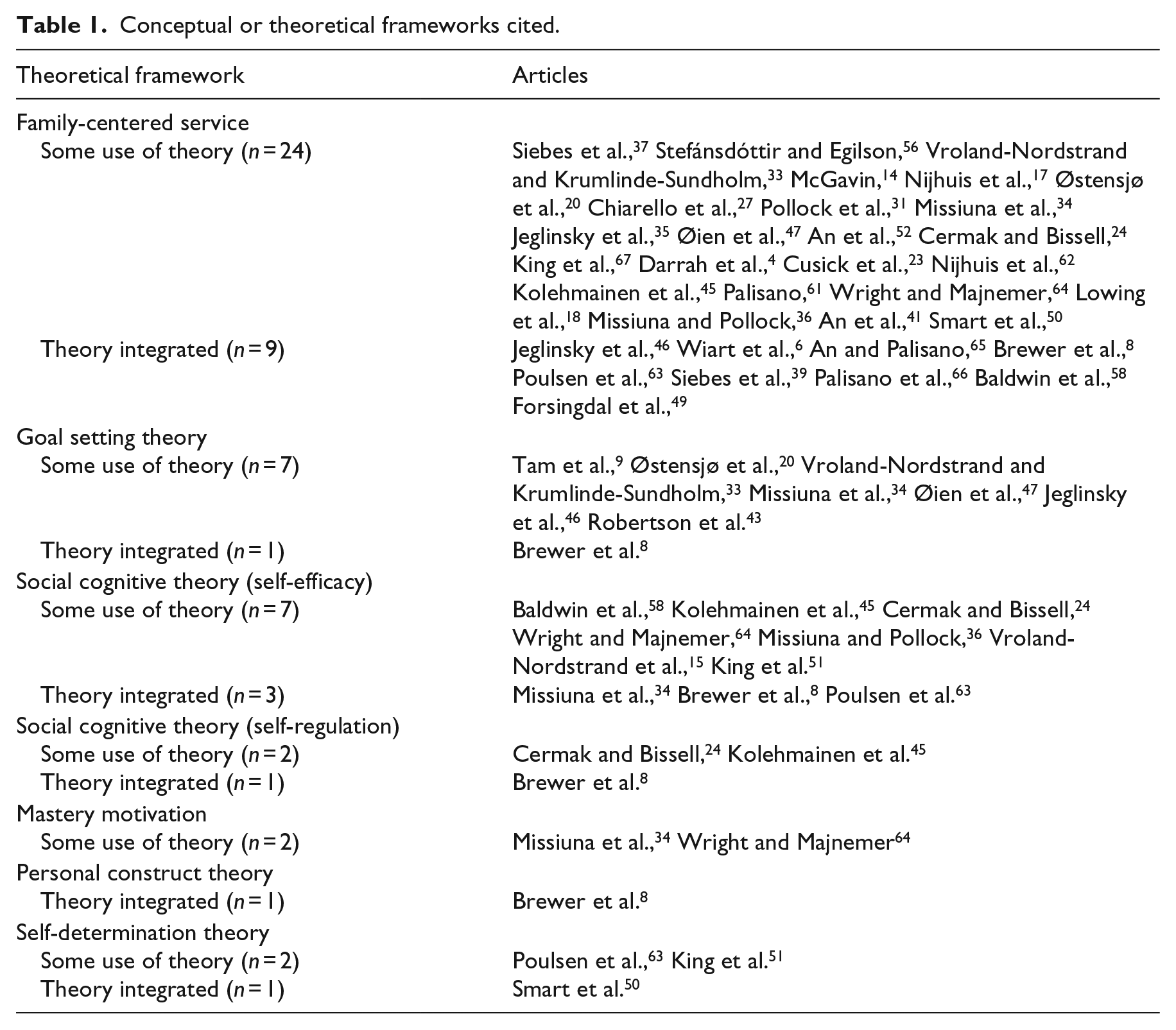
Social cognitive theory (n = 13) and Locke and Latham’s 69 goal setting theory (n = 8) have garnered some attention in regard to application to goal setting in paediatric rehabilitation. However, with three exceptions, 8,34,63 theoretical depth was lacking. Reference to mastery motivation (n = 2), personal construct theory (n = 1), and self-determination theory (n = 3) was limited to six articles.8,34,50,51,63,64 No articles addressed prominent theory related to behavior change such as the Health Action Process Approach. 70 Overall, the theoretical depth of this body of literature was weak. While family-centered care was fairly well represented, substantive conceptual or theoretical frameworks specific to goal setting were rarely mentioned in the literature and were not used to guide goal setting processes.
2. What is described in the literature about goal setting processes and outcomes?
12 of the 41 quantitative and mixed methods articles were excluded from this part of the analysis because the authors reported on aggregate data or chart reviews and therefore could not be expected to report on specific goal setting processes used by therapists and families. Therefore, 29 quantitative and mixed methods articles were reviewed for information related to goal setting processes. In addition, 14 articles (8 qualitative and 6 mixed methods studies) were reviewed for child, parent, or therapists’ perspectives on goal setting processes.
Role of the child, parent, and therapist
With the exception of brief descriptions of tools such as the Perceived Efficacy and Goal Setting System,15,16,34,36,57 the Canadian Occupational Performance Measure completed with parents and/or children,14,28 and the Here is How I Write Tool, 24 the role of the child was either unspecified or described using general statements such as “completed with families.” While some studies were not designed to include the child in goal setting (e.g. the purpose of the study was to identify therapist or parent goals), this review suggests that the role of children in setting their own rehabilitation goals is not well articulated in the paediatric rehabilitation literature.
The role of parents in the goal setting process is articulated to a greater extent than children, with their participation most often described as collaborating with therapists using individualized goal setting tools such as the Canadian Occupational Performance Measure,14,15,20,21,23,27,28,30,31,41,43,52,71 and Goal Attainment Scaling20,23,32,42 or the Canadian Occupational Performance Measure and Goal Attainment Scaling combined.20,23 Combined use of these tools generally involved use of the Canadian Occupational Performance Measure for identification of meaningful family goals followed by the use of Goal Attainment Scaling to operationalize more specific rehabilitation goals. The Canadian Occupational Performance Measure requires more involvement from the parent and/or child, and Goal Attainment Scaling is generally more therapist driven. 9 One paper 52 described a scaling process to facilitate Canadian Occupational Performance Measure performance ratings: Therapists discuss with parents how they would define ratings (i.e. scores of 1–10) in relation to their goals. This process was considered difficult to implement but potentially useful.
Two papers5,17 discussed the goal setting process implemented in the Netherlands, the Rehabilitation Activity Profile for Children. In this process, families identify their rehabilitation needs, the rehabilitation/education teams identify principal problems, and then families and service teams collaboratively formulate principal goals that drive rehabilitation interventions. With the exception of the use of formalized tools, for which processes are described in tool manuals, roles of parents are generally not well described or are unspecified. Therapist roles are also primarily characterized by the administration of formalized goal setting tools (i.e. Rehabilitation Activities Profile for Children, Canadian Occupational Performance Measure, Here’s How I Write Tool, Goal Attainment Scaling, and Perceived Efficacy and Goal Setting System).5,14,15,18,20,21,23,24,27,29,34,36,38,41–43,52,53,57,71
The qualitative studies provided insight into parent and therapist experiences with goal setting processes. In the qualitative component of a mixed methods case report with two mothers of children with cerebral palsy, 52 therapists perceived that goals grounded in meaningful conversations with mothers resulted in better goals compared to goals based on therapist-led perceptions of what was important for the child. The importance of a collaborative approach was identified; parents and therapists perceived cocreation of goals led to a shared understanding, enhanced parent/therapist collaboration, and better child outcomes. Furthermore, three qualitative studies that provided insight into the experiences of parents in the goal setting process6,47,49 reported that parents desired a flexible goal setting process, with some parents appreciating more therapist input into goals to capitalize on their clinical knowledge and experience. Notably, there were no qualitative studies that investigated the child’s perspective on goal setting processes or outcomes.
Linkage between goals and intervention strategies
About 10 of the 29 studies14,16,21,24,27,28,34,36,38,55 did not address the linkage between goals and interventions as this was beyond the scope of the research. Of the remaining 19 studies, only six18,29–32,52 explicitly addressed the direct link between identified goals and therapy activities. Four studies15,18,32,52 described processes for revisiting goals throughout therapy as a means to ensure focus and engagement in rehabilitation including ongoing reflection with parents on goal progress,15,52 regular communication strategies such as communication books and team meetings,18,32 using pictures so that the goals are more understandable for the child, 18 and discussion of goals during home visits. 32
Outcomes of goal setting
Only two studies included in this review evaluated outcomes associated with goal setting. Kolehmainen et al. 54 evaluated the implementation of a goal setting process in occupational therapy services in Scotland and reported that therapist uptake resulted in a shared rationale for decision-making among therapists, increased clarity in service provision (i.e. greater focus on goals), and improved interactions with schools and families. Length of treatment decreased by an average of two months following implementation, despite modest uptake of the process among therapists. Lowing et al. 18 compared the effects of goal-directed functional therapy and activity-focussed therapy with preschool children with cerebral palsy. Limited conclusions about the specific contributions of goal-directed therapy can be made from this study since there were other differences in therapeutic approaches between the groups, including a greater emphasis on parent education and engagement in the goal-directed therapy group.
3. What are the identified purposes of goal setting in the paediatric rehabilitation research and practice?
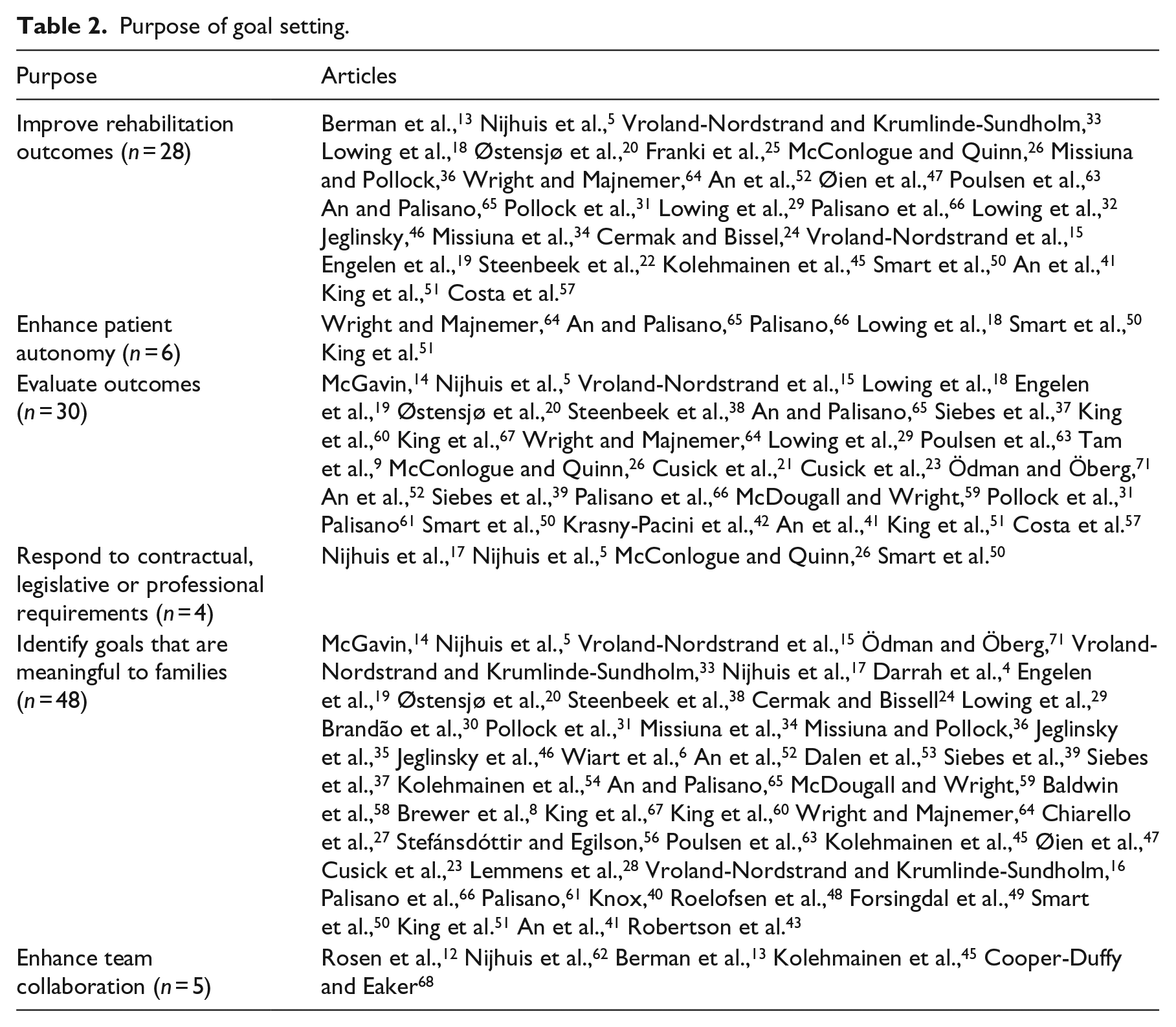
Purposes of goal setting either implied or explicitly stated in the 62 articles are presented in Table 2. Consistent with the theoretical emphasis on family-centered care, the primary purpose was identifying goals that are meaningful to families (n = 48), followed by evaluating outcomes (n = 30), and improving rehabilitation outcomes (n = 28). Responding to contractual or professional requirements (n = 4), enhancing patient autonomy (n = 6) and team collaboration (n = 5) were infrequently identified as purposes for goal setting.
Purpose of goal setting.
Discussion
The results of this study highlight a significant gap in the literature explicating a sound theoretical basis for goal setting in paediatric rehabilitation. While adherence to the principles of family-centered care is a crucial aspect of collaborative rehabilitation practice, family-centered care alone is an inadequate theoretical framework for goal setting. The principles of family-centered care provide the impetus for a goal-directed approach that is collaborative and based on goals that are important and meaningful to families. While this approach is crucial, it neither provides insight into the important personal and goal qualities that result in improved outcomes nor the psychological constructs associated with behavior change.
The absence of robust theoretical frameworks for goal setting in paediatric rehabilitation is conspicuous since behavior change lies at the core of most sustainable rehabilitation interventions. Theoretical frameworks specific to goal setting have been evaluated in other settings resulting in a significant body of literature and research with the potential to inform goal setting in paediatric rehabilitation. For example, Locke and Latham 69 evaluated relationships between goal qualities and outcomes in industrial and commercial settings. This theoretical framework has been used to support goal setting in adult rehabilitation. 72 Self-determination theory espouses that motivation to engage in effective goal pursuit depends on basic needs for autonomy, relatedness, and competence. 73 The Health Action Process Approach explains the three stages of behavior change—intention, planning, and action—and the relationships between psychological constructs at the three stages. 70 It is likely that a combination of theoretical frameworks is needed to adequately address goal setting in rehabilitation. 7 Implementation of these and other theoretical frameworks specific to goal setting is emerging in adult rehabilitation 7 and clearly has potential to inform goal setting theory and practice in paediatric. 8 Since research on the effects of goal setting is unlikely to develop in a systematic way and depart from the current focus on pragmatic application without explicit articulation of theory, a strong theoretical framework specific to paediatric is needed.
The development of substantive theory related to goal setting would also emphasize how and why goal setting is implemented in clinical practice. For example, self-determination theory purports that children who experience control and choice over their goals will be more engaged and focussed, thus highlighting the importance of maximizing child engagement in goal setting and therapy. 73 While an exclusive focus on family-centered principles will likely facilitate a collaborative approach to goal setting focussed on family priorities, it does not emphasize the importance of ensuring a consistent focus on therapy goals as a motivational strategy. Use of the Health Action Process Approach would encourage clinicians to use strategies that support families at various stages of change. The fact that less than half of the papers in this review stated or implied that goal setting was used to improve rehabilitation outcomes, suggests that a sound theoretical framework should address the potential for effective goal setting to increase motivation, engagement in rehabilitation and therapeutic outcomes. This lack of emphasis on the therapeutic benefits of goal setting is inconsistent with the larger body of goal setting literature that emphasizes improved performance as the most important reason for goal setting. 69
This review revealed a lack of research specifically focussed on the evaluation of the effects of collaborative goal setting with families. Studies frequently cited as providing evidence of effectiveness of goal setting for improving outcomes evaluated goal setting in conjunction with another treatment approach and compared the combined approach to a different intervention.19,74–76 There-fore, the distinct contribution of goal setting cannot be discerned. Research is needed to evaluate the proposed relationships between child and parent engagement in goal setting and the effects of autonomy, relatedness and competence on engagement in rehabilitation, and improved child outcomes. There is some evidence that strategies to increase child autonomy can contribute to increased performance and motor learning 77 and significantly increase child engagement in physical activity. 78 Since these two studies were conducted with typically developing children in non-rehabilitation settings, evaluation in the rehabilitation context is needed. Additional research is also needed to evaluate goal qualities and goal setting processes that optimize engagement in rehabilitation, outcomes that are meaningful to families and the effects at the service level. Kolehmainen et al. 54 provided some preliminary evidence that goal setting may decrease intervention duration due to a more streamlined approach to therapy focussed on family goals; however, additional evaluation of program level outcomes in different rehabilitation contexts is needed to make firm conclusions about the effects of goal setting on service level outcomes.
Children’s voices were largely absent from this body of literature. We did not find any qualitative studies exploring children’s experience with goal setting processes and descriptions of strategies to engage children in the goal setting process were lacking. Including children in joint administration of the Canadian Occupational Performance Measure, for example, may engage some children, but it does not ensure either optimal engagement of children or inclusion of their voices in setting their own rehabilitation goals. Older or more outspoken children may feel comfortable expressing their goals in a family interview with therapists, but many children will default to their parents. It is important to ensure the child’s voice is present in the goal setting process because they are capable of identifying achievable goals and they may not share the same goals as their parents. 15 They may place a greater emphasis on school and social activities, 15 for example. Exclusion of the child’s voice in goal-related discussions may lead to goals and related activities that are not motivating to the child, ultimately resulting in lower engagement in rehabilitation.
To date, implementation of formalized goal setting in clinical practice has been suboptimal.5,54,55 Pragmatic challenges to effective goal setting reported in the literature include a mismatch between clinician and patient perspectives on appropriate goals, 54 and organizational barriers such as lack of time, 38 inability to adequately coordinate service teams, 79 and poor documentation. 17 Therapists cite several barriers to goal setting including lack of time and concerns that families will not be able to identify reasonable goals.8,54 Efforts toward implementation of standardized goal setting processes have been time-consuming and have had limited uptake in paediatric clinical practice.5,54 Implementation challenges exist despite systematic efforts toward adoption as demonstrated by the implementation of the Rehabilitation Activities Profile for Children in the Netherlands 48 and the Good Goals 54 project in Scotland. Despite the multi-faceted and widespread implementation efforts associated with the Rehabilitation Activities Profile for Children, including a survey, national study group, local teams, extensive consultation of experts and potential users, a national conference, and evaluation of the tool, 48 approximately 24% of children in the Netherlands do not have documented rehabilitation goals 5 and 52% of identified goals are unrelated to parent-identified problems or needs. 17 While the outcomes of the Good Goals project related to increased service delivery efficiency were promising, therapist uptake was also less than optimal. 54
Increased patient autonomy was a rarely articulated purpose of goal setting. Currently, clinicians and researchers emphasize the importance of supporting children and families through transitional periods, such as a change in schools or transition to adulthood. We propose the current focus on “transitions” as finite events may detract from clinicians’ emphasis on facilitating autonomy development and engagement in healthcare decision-making over time. Consideration of the developmental trajectory of autonomy development 80 suggests that therapists should take a developmental approach to child and youth decision-making, encouraging increased engagement as the child’s capacity for decision-making increases. Strategies for engaging toddlers, for example, may include offering choices, acknowledging the child’s perspective, providing rationale for requests, and encouraging initiatives81,82 while engagement of adolescents will resemble adult shared decision-making.
Optimizing child engagement in goal setting should also be considered from a rights perspective consistent with the new era of children’s rights and new sociology of childhood.83–85 The United Nations Convention on the Rights of the Child 86 asserts that children’s voices should be heard and respected. The voices and agency that children have in the shaping of their own life worlds apply directly to the paediatric rehabilitation context. In response to emerging rights-based theoretical perspectives in childhood studies,85,87 ensuring the presence of children’s voices in decision-making in clinical practice and research becomes a priority. This shift involves engagement with theory that problematizes the power dynamics at play between clinician/researcher, parent, and child in order to envision processes that mitigate power imbalances and create space for children’s voices to be heard and valued. The prioritization of children’s perspectives on rehabilitation intervention goals, strategies, expectations, and outcomes in research is beginning to emerge.88–90
Limitations
Since we focussed on literature about goal setting, intervention studies that used individualized goal setting tools as outcome measures were excluded from this review. Therefore, this review did not represent the breadth of goal setting processes used in paediatric rehabilitation research. Similarly, since this review focussed on literature for children with motor disabilities from 1995 to 2017, the literature may not address specific implications for children with neurobehavioral diagnoses including autism spectrum disorder and any relevant literature prior to 1995.
Implications for practice
From an implementation perspective, it is important to consider that therapists’ perceptions of the reasons and benefits for goal setting may influence if and how they are willing to implement goal setting in their practice. 7 For example, if, consistent with our findings, therapists perceive that the primary purpose of goal setting is to be family-centered and identify goals that are meaningful to families, they may decide not to use a formalized goal setting process if they feel they are already family-centered in other areas of practice. If therapists view evaluation of outcomes as the primary purpose of goal setting tools, pre-post measures might be implemented with a lack of strategies to revisit goals throughout the intervention. Conversely, if goal setting is viewed as a tool to increase motivation and engagement, as goal setting theory research suggests, therapists may be more likely to implement strategies to ensure the child, parents, and others working directly with the child are consistently revisiting intervention goals.
While ensuring that goals are meaningful to families is undeniably important, the emphasis in the qualitative literature with parents about the importance of therapist input and the benefits of therapist/family coconstruction of goals6,47,49 suggests that a more tailored, collaborative, and flexible approach to goal setting is warranted. Families may prefer a collaborative approach with the therapists’ input and may not always want to be exclusively responsible for identifying goals. This finding emphasizes the importance of developing a relationship with families so that goal development and treatment planning is collaborative while grounded in the main concerns of families within their unique family contexts. The ability to cocreate short-term goals based on longer-term, family goals may also address the hesitancy of some therapists to engage in collaborative goal setting because of the concern that family goals may not always be attainable.
Clinical messages
While family-centered care provides strong rationale for collaborative goal setting, theory specifically related to goal setting has not been well articulated in paediatric rehabilitation.
Despite the commitment to family-centered care, the role of the child in the goal setting process is not well described.
Existing research on the evaluation of child, family, and service delivery outcomes associated with goal setting is limited.
Footnotes
Acknowledgements
The authors appreciate Barb Traill for her valuable insights on the concepts of autonomy and transition. Dr L.P.-W. led data collection and analysis and took the lead role in writing the manuscript. Dr S.K.P. resolved discrepancies in data extraction, participated in discussions about interpretation of analyses and completed a final edit of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr L.P.-W. was supported by the Canadian Child Health Clinician Scientist Training Program (CCHCSP), the Women and Children’s Health Research Institute (WCHRI) through the generous support of the Stollery Children’s Hospital Foundation, and Alberta Policy Wise for Children and Families.
Supplement material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.