
Abstract
Objective:
To empirically test the hypothesis that the 10 roles on the Revised Role Checklist are represented in the International Classification of Functioning, Disability and Health participation areas.
Design:
Cross-sectional survey.
Subjects:
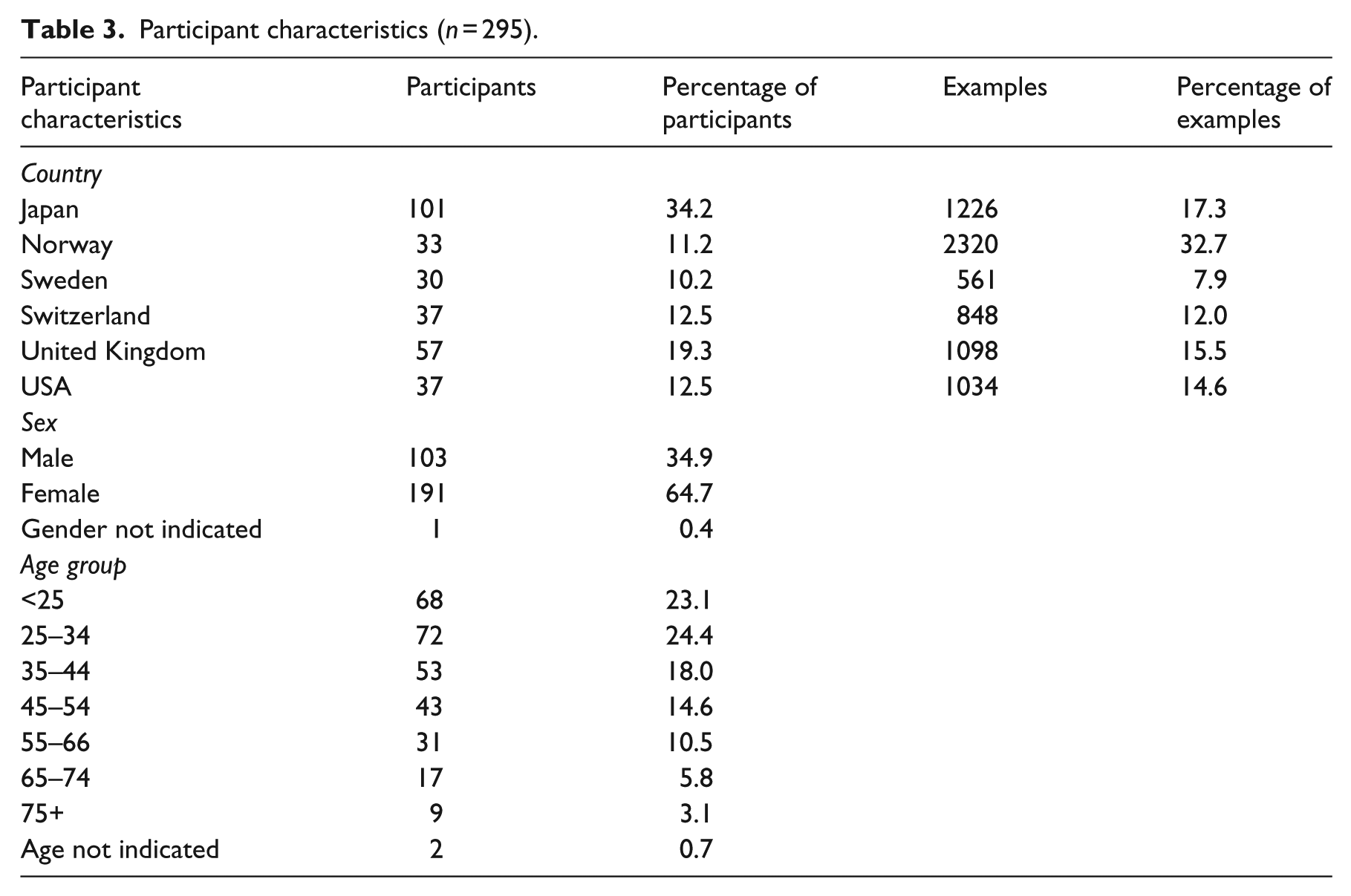
Investigators from Japan, Norway, Sweden, Switzerland, the United Kingdom and the United States recruited a total of 295 adults from the general population. There were 103 (34.9%) male and 191 (64.7%) female participants with one participant not indicating gender. The age distribution of participants was from <25 (n = 68) to 75+ with a mode of 25–34 years.
Main measure:
The Revised Role Checklist Part 1 was used to assess perceived incumbency in 10 roles. In addition, subjects were asked to provide role examples.
Results:
Of the 7087 examples provided by participants, 6578 (92.8%) fit the original hypothesis that the roles in the Revised Role Checklist were covered in participation areas. Fit was determined when the role example was either named in the associated International Classification of Functioning, Disability and Health participation area or when the criteria of: “does this example conceivably fit in the respective area as ‘a person’s involvement in life situations’ fit relative to each role.” Slight modification of the scope of three roles of the original hypothesis resulted in a 97.6% match.
Conclusion:
The roles in the Revised Role Checklist are well represented in the International Classification of Functioning, Disability and Health categories of participation.
Introduction
Participation in society, for persons who are aged or with disabilities, is of global concern; 1 however, there is a lack of instruments that can report on participation outcomes across disability groups. The International Classification of Functioning, Disability and Health (ICF) 1 aspires, in a large part, to establish common definitions for health outcomes and for practitioners and researchers to gather data and report outcomes using terminology consistent across cultures and languages. It therefore provides the appropriate framework to guide measurement standards. Can the Revised Role Checklist 2 serve as a measure of participation consistent with the ICF? Roles reflect participation.3,4 This is important as patients face complex physical and mental challenges during prolonged illness or disability. These challenges include disruption of the ability to perform valued roles, such as worker or homemaker and interfere with ways of participating in usual activities. 2 Rehabilitation involves assisting people to return to participation in society.
In occupational therapy, participation is frequently measured with the Role Checklist or the recent revision. The Revised Role Checklist is based on the original Role Checklist 5 and comprises role participation in 10 common roles in life: student, worker, volunteer, caregiver, home maintainer, friend, family member, religious participant, hobbyist, and participant in organizations in the present or the desired future. It is a short and easy-to-understand questionnaire in which results are immediately visible. It is used to assure client-centered practice by identifying desired client outcomes. The instruments are theoretically based in the Model of Human Occupation (MOHO) 6 which has been found to be consistent with the ICF. 7 The MOHO supports that roles enable individuals to participate in society. 3 It is consistent with the World Health Organization’s (WHO) definition of participation as “involvement in a life situation”. 1
In 2014, Scott 4 hypothesized that these 10 roles are associated with sections of ICF Activity and Participation Chapters 6–9: major life areas, domestic, interpersonal, and social community and civic domains (Table 1). The Revised Role Checklist is a balanced measure of participation. Balanced refers to the combination of the outsider and the insider view, both required as stated by participation literature.8–11 In accordance with the ICF, the outsider view reflects the objective data suitable for information about groups and subgroups of people—with and without disabilities. The insider view, however, goes beyond the objectivity of the ICF. This view is present when the instrument captures the individual’s own valuation of their performance: that is, not only whether they participate, but also how they feel about their performance or non-performance.
Roles described in the Revised Role Checklist and hypothesized categories of the International Classification of Functioning, Disability and Health (ICF).
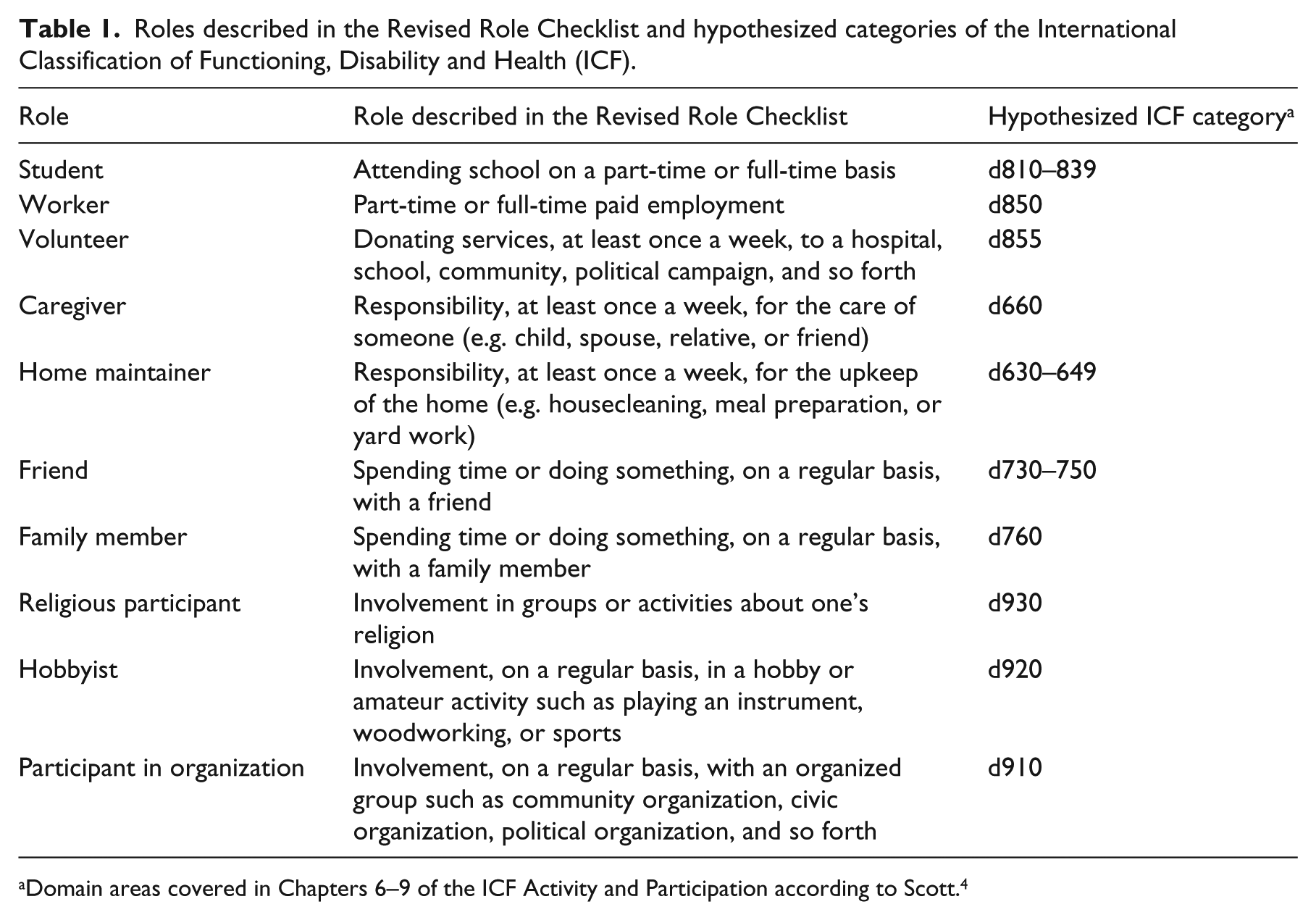
Domain areas covered in Chapters 6–9 of the ICF Activity and Participation according to Scott. 4
Participation is differentiated from activities in the ICF by the qualifier of “involvement with others.” Furthermore, in the Annex 4, four ways are provided to specify the difference: One way allows theory to dictate the distinction. In the present case, the MOHO is the theoretical basis with roles reflecting participation. Roles comprised a set of activities, performed automatically, in a routine and contextual manner. 6 For example, a working mother of three children may consider meal preparation as part of the caregiver role and later may develop an interest in cooking as a hobby. In this way, life events, skills, and interests assist in natural transitions of roles related to expected life changes such as marriage, retirement and normal aging. Roles are therefore changing and activities can be associated with different roles when performed in different contexts.
Measurement of participation and the ICF are seen as problematic in the literature outside of occupational therapy in the “what and how” participation can be measured. The issue has two intertwined elements: content and scope. Content refers to the items included in a measure. Rehabilitation therapists treating persons with differing diseases or disabilities are interested in the inclusion of activities required for role participation. Consequently, most of the psychometrically sound participation measurement tools are tailored to specific populations and include activity-related limitations. This is well documented elsewhere is the literature.11–13
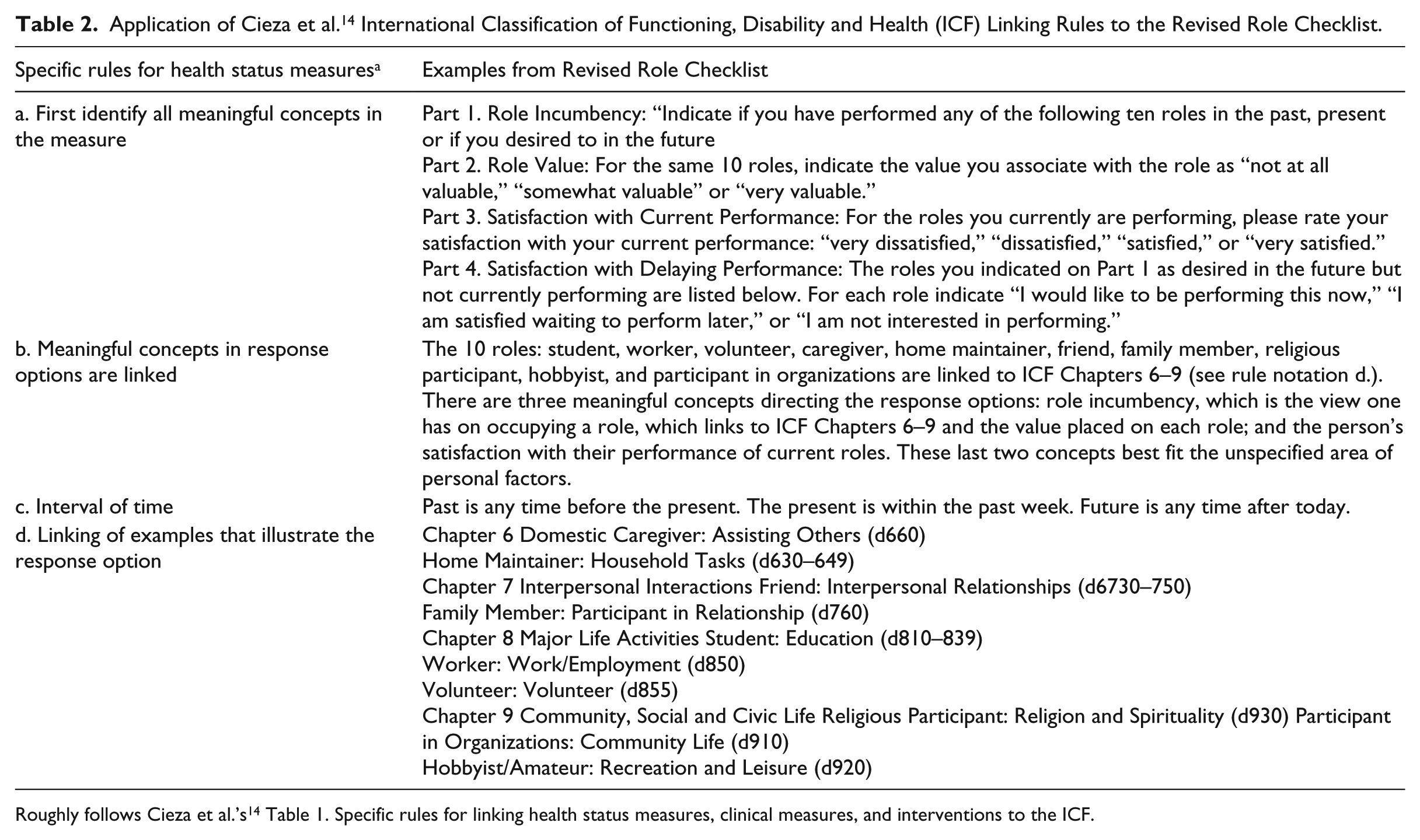
In terms of the scope of participation measures, and partly as a way to standardize information published about available measures, Cieza et al. 14 specified four rules to link measures to the ICF. These rules aim to direct researchers to the most appropriate tool for measuring desired outcomes (Table 2). According to Cieza et al.’s 14 specifications, the Revised Role Checklist is a health status measure, specifically a Patient-Reported Outcome Measure. They are personal assessments of functional performance with expression of personal value, which in the current case is satisfaction. Table 2 details the application of these linking rules to the Revised Role Checklist.
Application of Cieza et al. 14 International Classification of Functioning, Disability and Health (ICF) Linking Rules to the Revised Role Checklist.
This study aimed to empirically test Scott’s 4 theoretically derived hypothesis that the 10 roles on the Revised Role Checklist reflect participation areas present in the ICF. 1
Methods
To test Scott’s 4 hypothesis, our intention was to collect examples for activities individuals performed in the 10 roles of the Revised Role Checklist and link these examples to the ICF 1 Chapters 6–9.
Translation procedure
For the translation of the Revised Role Checklist, the working group, following international standards, established guidelines for translation. The instrument was then translated from English into German, Japanese, Norwegian, and Swedish following these guidelines. The version for the United Kingdom and the United States were kept identical. For all translations, a back-translation process was performed. Then, the back-translated versions were checked against the original. Differences between the original and the translations were discussed among the translators and the study principals to find an adequate solution. Slight modifications were made in the translated versions to reflect cultural difference within the constructs of role as specified in the MOHO.
Participants and recruiting
Participants were recruited from the general population in each of the participating countries (Japan, Norway, Sweden, Switzerland, the United Kingdom, and the United States). The aim was to make the sample as diverse as possible and thereby to represent a blend of gender, age groups, education levels, and work status. A convenience sample was collected by participating researchers through selected distribution of questionnaires among and through acquaintances, colleges, friends, and family. Participants had to be 18 years old or older and understand the respective language used in the questionnaire. No other limitations for participation were given and no specific group of disabled people was chosen since the goal at this step was to analyze the linkage of the instrument to the ICF through typical responses to role examples.
Data collection
Data were collected in winter 2014/2015. All participants were given Part 1 of the Revised Role Checklist. Part 1 asks for 10 roles—the self-reported role incumbency at present, past, and desired future. In the United States and United Kingdom, the data were collected with a combination of paper and pencil and an on-line questionnaire. In Sweden, Norway, Switzerland, and Japan, data were collected by paper questionnaire only. According to the findings of equivalence between paper and pencil and electronic administration, 15 we felt confident using both versions. Respondents in the English-speaking countries were asked to give an example for each role, whereas the instructions inadvertently differentiated slightly in the Swedish, German, Norwegian, and Japanese versions: “… provide an example of an activity that you either participated in the past, are currently performing, or plan to participate in the future for each role …” After data collection, examples in Japanese, German, Norwegian, and Swedish were translated into English by the researcher from the respective country. All provided examples were used.
Data linkage
For the linkage of the examples to the ICF, the rules proposed by Cieza et al. 14 (see Table 2) were followed. In a first step, each example was evaluated and had to be a “meaningful concept”; therefore, a set of words with one meaning identified. Examples with no “meaningful concept” were excluded from further analysis. In a second step, for every provided example, the corresponding three- or four-digit code(s) from section “d” of the ICF was sought out and linked as hypothesized by Scott 4 (Table 1). If the meaning of the example did not fit with any of the ICF-defined areas, it was classified as “not defined.” Those examples were excluded from further analysis. The linkage was performed by two independent raters: examples were first considered within countries by the individual researcher from that country who were all familiar with the ICF and the Revised Role Checklist. Second, the linkage was done by a second rater assuring consistency between countries with that researcher going through all examples. If differences occurred, a third researcher was consulted to identify the relevant code. The first and last authors (U.M. and P.J.S.) performed the classification process in collaboration. When in doubt, our reference was “Does this example conceivably fit in the respective area as ‘a person’s involvement in life situations’ (WHO 1 ) relative to each role,” and whether situations were consistent with our theoretical conceptualization of role with the WHO’s definition of participation 1 ). The same data were used to determine the degree to which the role examples support the Revised Role Checklist as a measure of the MOHO constructs of occupational performance and occupational participation. 16
Data analysis
Descriptive statistics was used to characterize the sample and frequency of role incumbency with SPSS 22 Windows version. Windows Excel was used to calculate the percentage of example that fit to the ICF categories of participation according to Scott’s hypothesis. Overall proportion of examples that fell into each ICF classification across countries was calculated. The linked identifiers were then compared to the hypothesized categories of the ICF for the respective role. The first and last authors (U.M. and P.J.S.) then subjected the original hypothesis to empirical testing. According to this analysis, the hypothesized categories were amended if indicated and in line with the construct of roles according to the MOHO. 16 The final step was to recalculate the overall percentage of role examples that fell into each classification.
Ethics
Ethical approval and/or approvals from the data protection agencies were obtained for each country as required by the country’s legislation. All respondents volunteered to take part and provided informed consent prior to data collection.
Results
An overview of the sociodemographic characteristics of the sample is provided in Table 3. A total of 295 adults participated providing 7250 examples of roles. Of these examples, 163 (2.5%) were considered “not defined” as they were ambiguous in meaning or could not be matched to the ICF. They consisted of temporal indications of role participation like “in the past” or frequencies like “seldom” or “daily” but also words like “yes.” They were excluded from further analysis. The linking of the 7087 remaining examples according to Scott’s 4 hypothesis showed a match of 92.8% (n = 6578) to the ICF (Table 4).
Participant characteristics (n = 295).
Preliminary results of the linkage of role examples with the International Classification of Functioning, Disability and Health (ICF) according to the hypothesis of Scott. 4
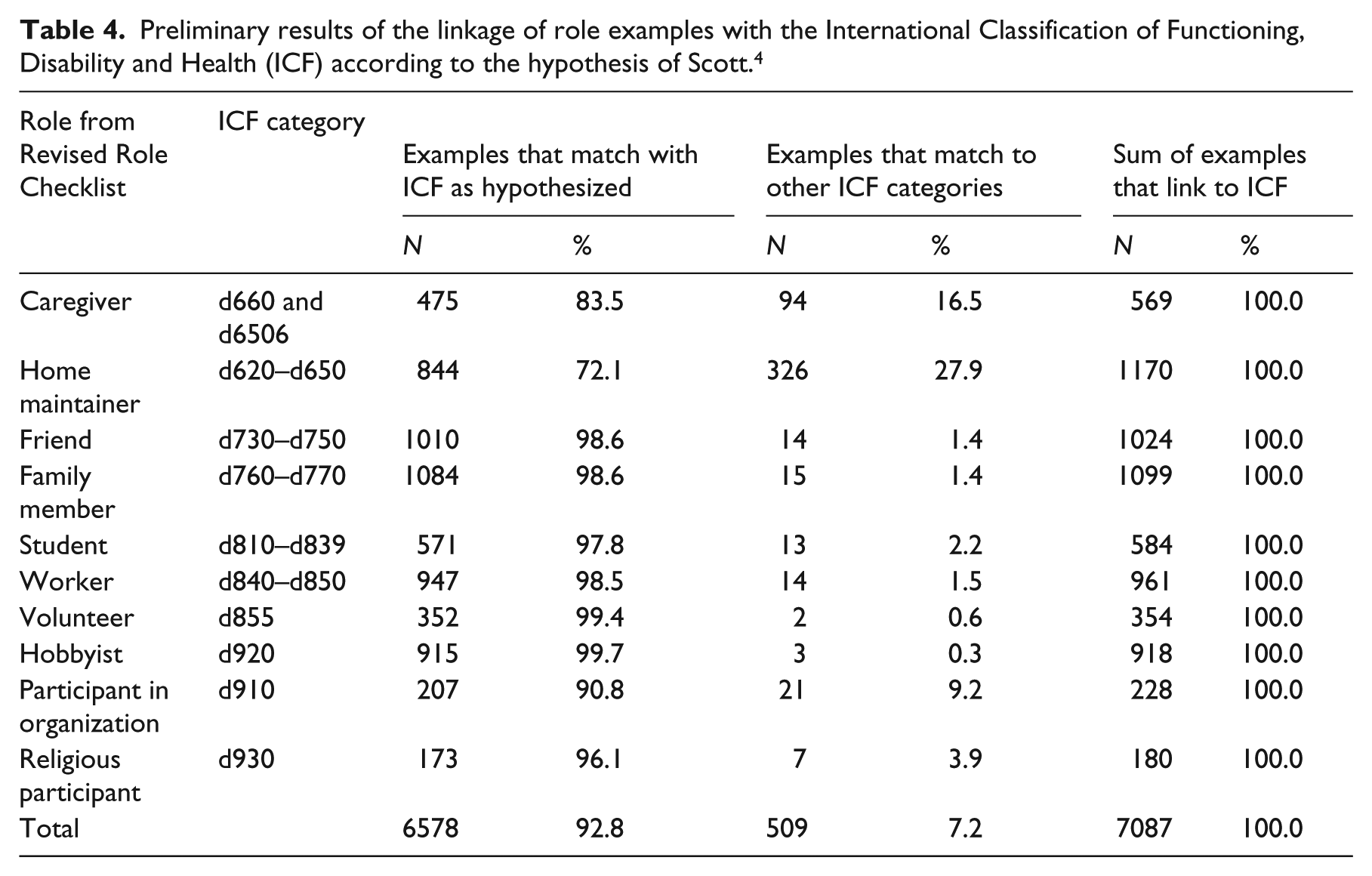
The comparison between the hypothesized ICF categories 4 and the linked data showed a variation from 72.1% (for role of “Home Maintainer”) to 99.7% (for the role of “Hobbyist”) with an average of 92.8% fit. The lowest fits were found for the roles of “Home Maintainer” with 72.1%, “Participant in an organization” with 90.8% and “Caregiver” with 83.5%. Analysis showed that many examples for those three roles were linkable to the ICF; however, they were outside of the hypothesized categories of d630–649 for “Home Maintainer” and d910 for “Participant in an Organization” and d660 for “Caregiver.”
For the role “Home Maintainer,” the analysis showed that most examples were associated well with ICF categories of “Household Tasks” (d630–d649) as initially hypothesized by Scott. 4 However, we found that the definition was too narrow as n = 99 examples (27.9%) were fitting into the category of “Caring for household objects” (d650) and “Acquisition of goods and services” (d620). Those two categories also should be considered as activities that an individual considerers part of the role performed by a home maintainer. The original hypothesis, therefore, was amended to comprise the categories of d620–d6505 and d6508–d6509. Applied to our data, this leads to a fit of 96.2% for “Home Maintainer.”
The category of “Assisting others” (d660) includes tasks such as assisting others with self-care, movement, communication, nutrition and health maintenance. Although for the role of “Caregiver,” we found n = 475 (83.5%) examples fit in this category, such as caring for my grandkids. However, n = 16 (2.8%) items could conceivably fit under “Household tasks,” such as preparing meals for my children, cooking for … which concern the International Classification of Functioning, Disability and Health section of “Preparing meals” (d630) and n = 25 (4.4%) examples that concern the section of “Doing housework” (d640), such as cleaning or washing clothes. There were also n = 5 (0.9%) examples from the section “Caring for household objects” (d650): maintenance of the house and repairing things around the house. Therefore, each of these are activities a person could ostensibly consider as caregiving if it is a responsibility they have as caregiver. Furthermore, the category “taking care of animals” (d6506) was also considered to be a task performed under the role of “Caregiver.”
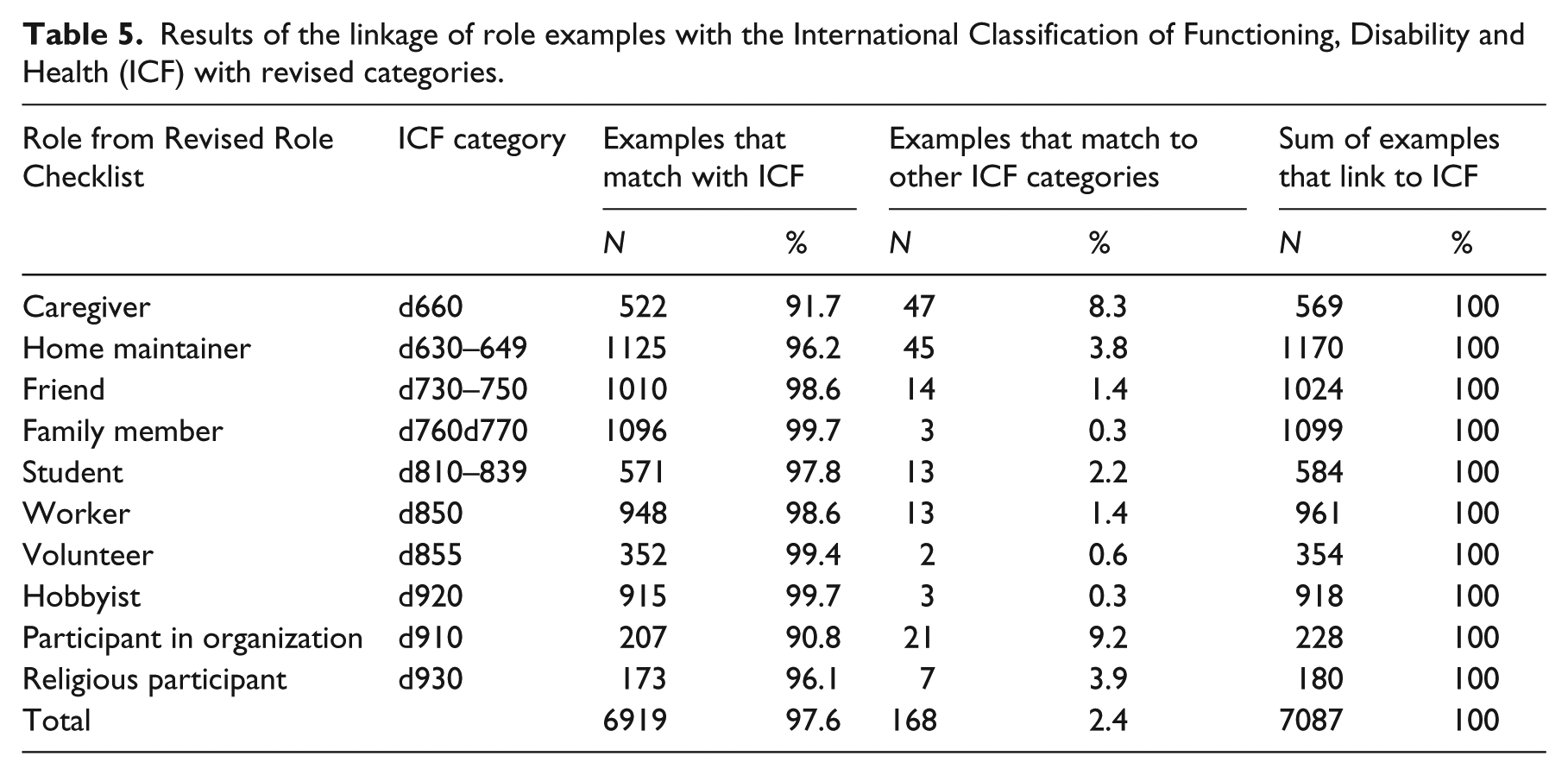
While linking the examples for the role of “Family Member,” we again found n = 12 (1.1%) examples which indicated that the initial definition with d760 was too narrow and should include also activities with spouse (d770). Table 5 shows all results.
Results of the linkage of role examples with the International Classification of Functioning, Disability and Health (ICF) with revised categories.
Discussion
In this study, we sought empirical support for the argument that the Revised Role Checklist is a valid assessment of the ICF construct of participation. Therefore, 7087 examples of activities from the 10 roles included on the Revised Role Checklist were linked to the ICF. The data showed that the 10 roles described in the Revised Role Checklist were well represented in the ICF categories of participation with 97.6% of the role examples fit in the categories of participation after modification of the original hypothesis. The remaining 2.4% fit to other categories of the ICF such as Body Functions and Structures as they described content such as “I am blind,” “depression,” or lacked relevance such as “I used to.”
We found that the criterion for classifying examples does this example conceivably fit in the respective area as ‘a person’s involvement in life situations’, relative to each role, was important to capture the example given for participation in a specific role. The rationale for this criterion is consistent with the ICF 1 and the MOHO. 3 In many cases, we found that the same examples for activities could be found for different roles; for example, the activity of using the phone. When done with a colleague at work, it is coded as “informal social relationships” (d750). If one calls to promote a political candidate, it is coded as “political life and citizenship” (d950), and if it is made to arrange medical assistance for a family member, the code is “assisting others” (d660). Each of these phone calls are contextualized in the role; however, the activity itself, using a telephone, fits with Chapter 3 of Activities and Participation—Communication, specifically “conversation” and “using communication devices and techniques” (d350–d369). Activities therefore are in most cases not role specific. Rather, performance of activities may be required for adequate participation in a role or the performance of an activity may simply be part of the daily routine of an individual.
Future studies are needed to investigate the distribution of roles in diverse clinical groups and cultures, as well as outcomes related to abandoning valued roles. For example, Scott 17 showed that liver transplant recipients displayed a pattern of disengagement with previously enacted roles. Dickerson and Oakley 18 found a pattern of more current roles among non-disabled community-living individuals compared with individuals who had physical or psychosocial disabilities, and a recent study found that elderly participants (>65 years) performed significantly fewer roles compared to the younger participants. 19 Assuming that role participation is related to important outcomes, research is needed to identify populations at risk, and what measures may be effective in remediating disrupted role patterns.
However, in our judgment, the process of ticking one of the roles listed in the Revised Role Checklist is unlikely to differ between the general population and specific disability groups or between cultural groups. This perspective is theoretically grounded in Oakley’s original concept of role incumbency. Role incumbency means that a person’s role identity is internally held. The listed roles are generically described and are therefore likely to be conceptualized in much the same way across groups. Activities that are tied to roles may differ between groups—for example, stroke survivors with hemiplegia may not engage in playing tennis, while their notion of the generic role of hobbyist is the same. Furthermore, as seen from the initial analysis of our data, the roles were stable across six culturally diverse countries. The numerous examples of the 10 listed roles matched the hypothesized ICF category in more than 92.8% of the cases (Table 4). Though replicating studies may be warranted, we consider it likely that examples of roles will link to the ICF categories in a similar manner as shown in this study.
Study strengths and limitations
A strength of this study is the broad range of countries participating to cover the concepts of roles described in the Revised Role Checklist from different cultures. Also, the vast amount of different examples that were linked is a strength of this study. One limitation of this study lies in the modest size of the sample. Taking into account the proportionally large subsample of young people from Japan (representing a third of the total number of participants) and the large amount of examples provided by the Norwegian participants, the distribution of participants and the examples they provided may limit the generalizability of the findings. In other words, the large number of young Japanese participants and the large number of examples from the Norwegian participants may have skewed the results for the sample as a whole. While the Revised Role Checklist was subjected to an appropriate and pre-established translation procedure in Japan, Switzerland, Sweden, and Norway, only the project representative in each of these countries translated the specific role examples into English. Thus, the procedure for translating the examples is a potential source of bias. The recruitment approach of collecting a convenience sample may also have influenced the results.
The slight differences in the wording of the instructions for participants to provide examples lead to differences in responses by country. In the United Kingdom and United States, participants were simply asked to give an example for each role. In Sweden, Norway, Switzerland, and Japan, respondents were instructed to “… provide an example of an activity for each role …” This difference in phrasing may have elicited different types of responses. The researchers assume the wording “provide an example of caregiver present” prompted responses such as “mother,” whereas the wording “give an example of what you do as a caregiver” prompted responses such as “caring for my child.”12,16 They discovered in retrospect that different translations of the question would elicit different types of responses. In the Norwegian translation, for example, respondents were guided toward giving performance-related responses, whereas the original English language version was neutral in this respect. This discrepancy was also apparent in a similar study where Bonsaksen et al. 16 linked these examples to the constructs of occupational participation and occupational performance.
Another effect the different phrasing of the questions in the questionnaire was that in some countries, the respondents were explicitly asked to provide one example, whereas respondents in other countries felt invited to state several examples.
Conclusion
Previously, there has been disagreement on the scope of items which belong on a participation measure. The findings of this study illustrate how roles can be an effective way to capture participation. It is clear, in this study, to recognize the impact of the wording of the question and how it can provoke different associations: as a series of activities or as a function: shopping for food, doing dishes and cleaning up, or providing meals for my family, valid responses to the caregiver role.
This study has provided evidence that a large number of specific role examples provided by a cross-cultural general population sample are almost perfectly consistent with the ICF categories of participation. The instrument therefore may be used to measure and document participation with the unique value to yield valid cross-cultural comparisons of participation.
Clinical messages
Implications for rehabilitation:
The study has shown that the Revised Role Checklist is a valid instrument that can report on an individual’s participation in society consistent with the International Classification of Functioning, Disability and Health.
As a population or aggregate measure, the Revised Role Checklist can measure participation patterns across all disability groups by various professions.
The Revised Role Checklist allows for cross-cultural comparisons of participation.
Footnotes
Acknowledgements
The authors would like to thank all who participated in the study and provided role examples. The authors acknowledge the work invested by those who collected the data in the involved countries not represented in the list of authors: Lena Haglund (Sweden), Kirsty Forsyth and Susan Prior (United Kingdom), Takashi Yamada (Japan), as well as Deana Schuman (USA) for her support provided with the linkage of the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.